1. Introduction
Snacks are a simple and quick way to satisfy so-called first hunger. They are commonly considered the most convenient alternative to regular food when you do not have time to eat or as a supplement between regular meals. There are many definitions of a snack. Generally, a snack is a small portion of food eaten between regular meals. Snacks can be sweet, savory, or healthy, and they serve various purposes, such as satisfying hunger, providing energy, or indulging in a treat [
1]. According to a Nielsen IQ report, from April 2023 to March 2024, the snack market in Poland reached PLN 27.1 billion (6.77 trillion USD), with sweet snacks dominating. Among sweet snacks, Poles most often bought pre-packaged cakes and cookies (3.9–0.97 billion USD), pralines (2.9 billion USD), and chocolate bars (2.8 billion USD); among salty snacks, chips and crisps dominated (5 billion USD) [
2].
In Poland, sweets are a regular part of the diet for most consumers (91%) [
3]. In 2024, the European market for confectionery (this segment includes chocolate products, confectionery, and preserved pastry products) and snacks was valued at approximately 256.20 billion USD, with a projected annual growth rate (CAGR) of 5.18% between 2024 and 2029 [
3]. On average, Poles consume between 5.7 and 5.9 kg of chocolate per person per year [
4], which is less than in leading European countries. In contrast, several other European countries have higher per capita chocolate consumption [
5,
6], such as Switzerland: 8.8 kg, Austria: 8.1 kg, and Germany: 7.9 kg.
Sweet and salty snacks mainly provide simple sugars and fats. In European Union (EU) legislation, fat is defined as total fat, including phospholipids. The basis for this definition is how total fat is extracted from food products. In this context, the term “fat” refers to all lipid fractions, both free and bound, in plant and animal tissues, extracted together from a food sample using generally accepted analytical methods [
7].
Dietary fats play a key role in health by providing energy, promoting cell growth, developing during early life, and aiding in the absorption of fat-soluble vitamins (A, D, E, and K). They also contribute to hormone production (steroid hormones, prostaglandins) and brain function—omega-3 and omega-6 fatty acids are crucial for cognitive function, mood regulation, and neuroprotection [
8]. However, not all fats are created equal in terms of health effects [
9]. Types of dietary fats include monounsaturated fats (MUFA), polyunsaturated fats (PUFA), saturated fats (SFAs), and trans fats (TFAs) [
10]. Metabolic and epidemiological studies have shown that consumption of saturated and trans fats accelerates cell apoptosis, elevates inflammatory markers (such as C-reactive protein, fibrinogen, interleukin 6, ICAM-1, VCAM-1, PGE, TNF alpha), promotes insulin resistance, promotes weight gain, contributes to visceral fat accumulation, and contributes to liver dysfunction. This results in an increased risk of various chronic diseases, including cardiovascular disease (CVD), cancer (especially breast, prostate, and colon), obesity, type 2 diabetes, and non-alcoholic fatty liver disease [
11,
12,
13,
14,
15,
16]. Childhood obesity is also linked to increased risk of depression and anxiety, lower self-esteem, and poorer academic performance.
There is a correlation between saturated fat intake and elevated levels of triglycerides, low-density lipoprotein (LDL) cholesterol (as well as reduced levels of high-density lipoprotein cholesterol (HDL-C) [
17]. A Cochrane review found that reducing saturated fat intake for at least two years led to a reduction in cardiovascular events, although it had no significant effect on total mortality or cardiovascular mortality [
18].
Trans isomers of fatty acids (so-called trans fats) are classified according to the two main sources from which they are derived: natural so-called r-TFAs (ruminant trans fatty acids) and industrially produced so-called i-TFAs (industrially produced trans fatty acids). i-TFAs are primarily formed by partial hydrogenation of vegetable or fish oils as an unfavorable side effect of industrial hardening processes [
7]. Trans fats raise inflammatory markers and low-density lipoprotein cholesterol, while lowering high-density lipoprotein (HDL) cholesterol, leading to an unfavorable lipid profile. For example, a meta-analysis showed that a 2% increase in energy intake from trans fats is associated with a 23% increase in cardiovascular risk [
19]. A 30% increase in the risk of developing CHD and an 18% increase in the risk of death were reported for high intake of i-TFAs alone.
The TFAs have negative effects on fertility in both men and women. In women, elevated intake of TFAs has been linked to the most negative effects on ovulation, pregnancy length, fetal malformations, and increased risk of fetal loss [
20,
21]. In men, higher TFA intake is inversely associated with sperm concentration and total sperm count. In addition, there is a positive correlation between trans fatty acid intake and asthenospermia [
21].
The lack of adequate research on TFA intake in children may be due to the fact that most epidemiological studies on TFA intake have evaluated cardiovascular effects, which typically do not occur until later in life [
22].
Saturated fatty acids and trans fatty acids are a constant ingredient in processed snacks, as they affect their taste, texture, and shelf life. Although trans fats are increasingly being eliminated due to international and national regulations, they can still be present in some products. The 2023 National Nutrition Test of Poles indicates that sweets—such as candies, cakes, cookies, candy bars, yeast cakes, and waffles—are chosen by 44% of respondents [
23]. According to the same survey, young adults (18–24 years old) were the most likely to consume sweet snacks (63%) as well as yogurt, cheese, and dairy desserts (42%).
The World Health Organization (WHO) recommends that in individuals aged 2 years and older, saturated fatty acids should constitute no more than 10% of total daily energy intake (EI), while trans fatty acids should contribute less than 1% of total daily EI [
24]. According to the Nutrition Standards for the Polish Population, the intake levels of saturated fatty acids and trans fatty acid isomers across all age groups should be minimized as much as possible while ensuring the nutritional adequacy of the diet. Moreover, the total fat intake for children and adolescents aged 3–18 years should provide 30–40% of total energy intake [
7].
The aim of this study was to assess the snack consumption behaviors of Polish adolescents aged 10–15 years, and to estimate their intake of total fat, saturated fatty acids (SFAs), and trans fatty acid isomers (TFAs) from sweet and salty snacks.
3. Results
The study included 362 school pupils: 192 girls (53.0%) and 170 boys (47.0%). The age distribution was as follows: 50 pupils aged 10 and 12 years (13.8%), 49 aged 11 years (13.5%), 47 aged 13 years (13.0%), 82 aged 14 years (22.7%), and 84 aged 15 years (23.2%).
Based on BMI-for-age percentile charts, 253 participants (69.9%) had normal weight, 43 (11.9%) were classified as underweight, 56 (15.5%) as overweight, and 10 (2.7%) as obese (
Table 3).
When stratified by sex, girls more frequently had a normal weight compared to boys (82.3% vs. 55.9%). Conversely, underweight was considerably more common among boys (24.1%) than girls (1.1%). Overweight was slightly more prevalent among boys (17.6%) than girls (13.5%), while obesity affected 3.1% of girls and 2.4% of boys (
Table 4 and
Table 5).
Age-specific patterns also varied between sexes. Among girls, all cases of obesity occurred exclusively in the 15-year-old group. In contrast, boys with obesity were mostly observed in the youngest group (10 years). Overweight was most prevalent in 15-year-old girls (57.7%) and 12-year-old boys (30.0%)—
Table 4 and
Table 5. Interestingly, underweight boys were present in nearly every age group, with the highest percentages noted among those aged 13–15 years.
3.1. Estimation of Fat Intake
The mean daily fat intake from confectionery and salty snacks among the entire study group was 34.5 g/day, representing 46.8% of the recommended daily fat intake. The values ranged widely, from as little as 0.76 g/day to as much as 117.6 g/day. Girls consumed slightly more fat than boys on average (36.5 g/day vs. 32.2 g/day), corresponding to 52.6% and 41.0% of their respective dietary fat requirements. However, this difference was not statistically significant (
Table 6).
A significant age-related effect on fat intake was observed (
p < 0.05). The highest intake was recorded among 10-year-olds (41.4 g/day, 65.3% of the reference intake), with a noticeable drop in the 11- and 12-year-old groups (25.0 and 29.7 g/day, respectively). In older adolescents (13–15 years), fat intake stabilized between 33.3 and 38.7 g/day. Among girls, fat intake was highest in 14-year-olds (46.3 g/day, covering 63.8% of the recommended intake) and lowest in the 13-year-olds (29.4 g/day, 41.8%). Among boys, the greatest intake was noted in the 10-year-olds (42.5 g/day), with markedly lower values observed in 11-year-olds (21.7 g/day) and a gradual increase thereafter (
Table 7 and
Table 8).
With regard to nutritional status, there was a trend of increasing fat intake with increasing BMI category. Underweight participants consumed an average of 30.3 g/day, compared to 38.5 g/day among those who were overweight and 41.6 g/day among those with obesity. While the overall effect of BMI on fat intake was not statistically significant, selected subgroups showed marked differences. For instance, boys with overweight or obesity at age 10 consumed substantially more fat (73.1 g/day and 50.7 g/day, respectively) than their normal-weight peers (30.6 g/day). Similar patterns were observed at age 13, where boys with overweight reported the highest relative fat intake (118.5% of the recommendation).
Among girls, the highest intake relative to dietary requirements was observed in 11-year-olds with overweight (51.3 g/day, 80.4% of recommendation), while the lowest was in 13-year-olds with underweight (18.8 g/day, 26.7%). Notably, no data were available for underweight or obese girls in most age categories, likely due to low group numbers.
3.2. SFAs Intake Estimation
The average intake of saturated fatty acids (SFAs) from confectionery and salty snacks among the study participants was 15.3 g/day, which corresponds to 59.1% of the recommended daily maximum. Girls consumed more SFAs than boys (16.1 g vs. 14.4 g/day), covering 66.0% and 52.2% of their respective daily limits. However, the differences between sexes were not statistically significant (
Table 9).
Statistically significant differences in SFA intake were observed across age groups (p < 0.05). The highest average intake was recorded among 10-year-olds (18.9 g/day, 84.8% of the recommendation), whereas the lowest was found in 11-year-olds (10.8 g/day, 46.6%). From age 12 onwards, intake levels increased gradually, ranging from 12.7 g to 17.2 g/day, corresponding to 51–63% of the allowable daily intake.
With regard to nutritional status, overweight and obese students had the highest SFA consumption (18.0 g and 18.3 g/day, respectively), corresponding to 70.6% and 73.8% of the maximum daily limit. In contrast, underweight individuals consumed the least (13.8 g/day; 48.6% of the daily limit) and those with normal weight averaged 14.8 g/day (58.0%). This trend was observed in both sexes.
Among girls, the highest SFA intake was noted in 10-year-olds with normal weight (19.7 g/day; 92.5% of the limit), and in 11-year-olds with overweight (20.4 g/day; 91.1%)—
Table 10.
In boys, the highest values were observed in 10-year-olds with overweight (36.2 g/day; 157.4% of the limit) and in 13-year-olds with overweight (40.6 g/day; 145.5%). Notably, some boys with overweight or obesity in younger age groups substantially exceeded the recommended maximum intake (
Table 11).
Overweight and obese individuals had the highest intake of saturated fatty acids. The average intake of SFA in these individuals ranged from 18.0 to 18.3 g, which was more than 70% of the daily intake limit for this dietary component. Normal-weight students averaged an intake of 14.8 g of SFA (58% of the daily intake limit).
Although not statistically significant for BMI overall, these subgroup differences suggest that higher fat mass may be associated with excessive consumption of SFAs from snacks. Furthermore, wide interindividual variation within BMI and age categories highlights the heterogeneity of dietary habits in this population.
3.3. TFAs Intake Estimation
The mean daily intake of trans fatty acid isomers among the surveyed students was 2.5 g/day, corresponding to 96.2% of the recommended daily limit. Girls showed a slightly higher intake than boys (2.5 g/day vs. 2.4 g/day), resulting in 104.2% and 85.7% of their respective dietary limits. However, these differences were not statistically significant (
Table 12).
Statistically significant differences were observed across age groups (
p < 0.05). The highest average TFA intake was recorded among 10-year-olds (3.6 g/day, 163.6% of the recommended intake), far exceeding the suggested maximum. The lowest intake was observed in 11- and 12-year-olds (1.5 g/day and 1.8 g/day, respectively), while adolescents aged 13–15 consumed approximately 2.2–2.8 g/day, close to or slightly exceeding the allowable limit (
Table 11).
Age significantly affected TFA intake (
p < 0.05). The highest average intake was recorded among 10-year-olds (3.6 g/day; 163.6% of the recommendation). Girls in this age group consumed particularly high amounts, with 10-year-old girls with overweight recording an average intake of 3.9 g/day—185.7% of the recommended maximum—
Table 13.
In contrast, the lowest intake was observed among 11- and 12-year-olds (1.5 and 1.8 g/day, respectively), both in girls and boys—
Table 14.
Among girls, TFA intake exceeded recommendations in several age and BMI subgroups. For example, 14- and 15-year-old girls exceeded the threshold on average (108.0% and 107.7%, respectively), with overweight girls aged 15 showing a particularly high intake of 3.7 g/day (142.0%). Interestingly, in most age groups, girls with overweight consumed more TFAs than their normal-weight peers.
Among boys, extremely high TFA intake was noted in certain individuals. Overweight boys aged 13 consumed an average of 12.8 g/day (457.1% of the limit), while obese 10-year-old boys reached 3.9 g/day (169.5%). Nevertheless, not all boys exceeded the intake limit: boys aged 11 and 12 had average intakes below 2 g/day—
Table 14.
In total, 115 students (31.8%) exceeded the recommended TFA intake. The proportion was similar between girls (30.7%) and boys (32.9%). However, breakdown by age showed that excessiveness was most common among 10-year-olds (64.0%), followed by overweight (42.8%) and obese (40.0%) participants.
These findings highlight that both girls and boys, particularly those with excess body weight and aged 10–15, are at elevated risk of excessive TFA intake.
Across the entire study population, 12.2% of participants exceeded the recommended daily intake of total fat from confectionery and salty snacks. In contrast, exceedance was more common for saturated fatty acids (SFAs) and trans fatty acid isomers (TFAs), reported in 19.9% and 31.8% of students, respectively (
Table 15).
Girls were more likely to exceed the recommendations for total fat and SFAs than boys (14.6% vs. 9.4% for total fat; 23.4% vs. 15.9% for SFAs). In contrast, boys slightly more frequently exceeded TFA limits (32.9% vs. 30.7%).
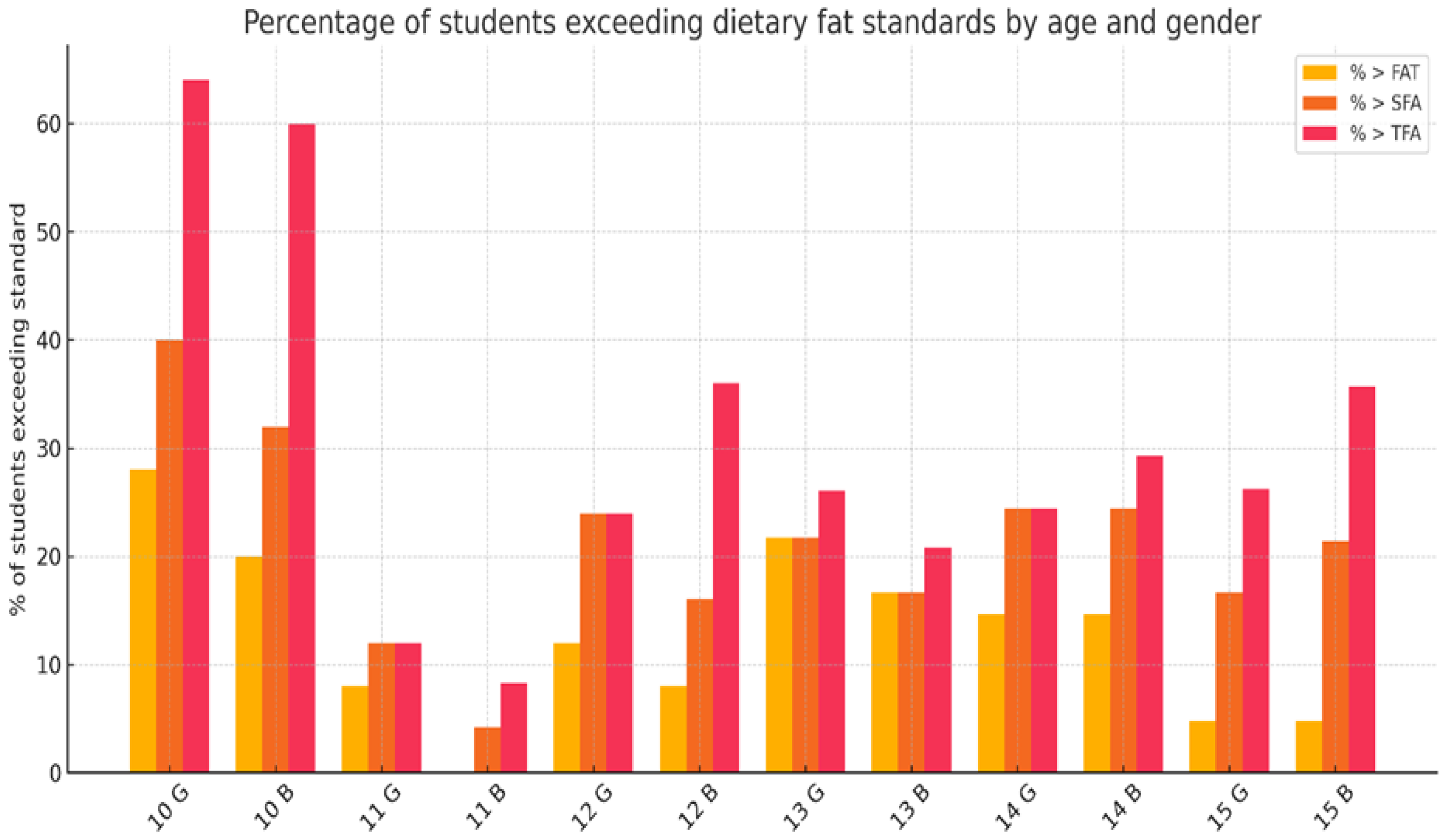
Age was a major determinant of dietary fat excess. Among 10-year-olds, nearly two-thirds (64.0%) surpassed the TFA intake recommendation, while 26.0% exceeded SFA limits and 24.0% exceeded total fat intake. The lowest proportions of exceedance were observed among 11-year-olds (4.1% for total fat; 8.2% for SFAs; 14.3% for TFAs)—
Figure 1.
When stratified by nutritional status, overweight students most frequently exceeded recommendations: 21.4% for total fat, 30.4% for SFAs, and 42.8% for TFAs. Obese students also showed high rates of excess (40.0% for TFAs), although their numbers were small. In contrast, underweight and normal-weight students were less likely to exceed intake thresholds across all types of fat.
Figure 1 illustrates the proportion of students exceeding dietary recommendations for total fat, SFAs, and TFAs intake, disaggregated by age and gender. The highest exceedance rates were recorded among 10-year-olds, particularly for TFAs, where more than 60% of both girls and boys surpassed the recommended limits. Among older students, the percentage of exceedance was generally lower but remained notable, especially in 14- and 15-year-olds. Girls tended to exceed the fat and SFA recommendations more often in early adolescence, while boys exceeded TFA limits more frequently, particularly at ages 10 and 15.
4. Discussion
The body’s fat requirements under homeostatic conditions depend on various factors such as age, sex, type of physical activity, and physiological status (e.g., pregnancy, lactation, menopause, and andropause) [
7]. According to the latest World Health Organization dietary recommendations for the prevention of unhealthy weight gain, fat intake should be limited to 30% of total energy intake [
30]. In the prevention of diet-related diseases—as well as for proper development and the maintenance of health—the quality of fat consumed is more important than the total amount. In particular, efforts should be made to eliminate industrially produced trans fats and animal fats rich in saturated fatty acids [
31].
Given the widespread availability and marketing of high-fat, ultra-processed snacks targeted at children and adolescents, it is important to evaluate the nutritional quality of these products [
32,
33,
34]. Based on earlier reports indicating the popularity of sweet and salty snacks among Polish youth, a photographic food album with 20 snack items was used. From this list, five of the most frequently selected categories—including chocolate bars, wafers, crisps, and cookies—were chosen in collaboration with study participants to reflect their real-life preferences. Nutritional data for these snacks are presented in
Table 1 and serve as the basis for estimating daily fat intake.
Our findings are consistent with broader trends reported by Beltrá et al. [
32], who analyzed 3209 food products from the BADALI Food Database in Spain. Among all products intended for children or adolescents, 61.5% were high in fat, 58.5% in free sugars, 45.4% in saturated fat, and 45% in sodium. Snacks contribute approximately 25.0% of adolescents’ daily total fat intake and 25.4% of their saturated fat intake [
33]. In the study by Larson et al. [
34], adolescents consumed an average of 2.2 daily servings of energy-dense snacks and 4.3 snacks per day, with many consumed outside the home. Findings from the study by Kotowska et al. [
35] indicate that 13.4% of young Polish individuals consumed sweets between main meals on a daily basis, 37.7% did so several times per week, and 16.2% once per week. Chips, crackers, and puffed snacks were also reported as frequent snacks, with daily consumption observed in 2.1% of respondents, several times per week in 13.4%, and once per week in 21.4%.
This is particularly concerning given the growing body of evidence suggesting that dietary habits are established early in life, tend to persist from childhood, and have long-term consequences for future health outcomes [
36,
37,
38,
39].
More than 12% of participants exceeded the recommended fat intake based on snack consumption alone, particularly among girls, 10-year-olds, and individuals with overweight. Girls exhibited a slightly higher fat intake than boys (~4 g/day). This may reflect gender-based differences in snacking behavior, emotional eating, or early body image awareness, particularly among preadolescent girls. While sex differences were not statistically significant, a visible trend was observed, consistent with earlier reports [
39]. This partially aligns with the study by Hoy et al. [
40], which found that snack consumption is higher among children aged 6–11 years compared to adolescents aged 12–19 years. Younger children may rely more on habitual household snacking patterns, while older youth may be more influenced by peer norms, diet culture, or body image concerns [
41,
42].
The mean saturated fatty acid (SFA) intake from snacks was 15.3 g/day, covering 59% of the maximum recommended daily intake. Girls consumed slightly more SFAs (16.1 g/day) than boys (14.4 g/day). The highest intake was observed among 10-year-olds (18.9 g/day), significantly higher than that of 11-year-olds (10.8 g/day; p < 0.05). This suggests a steep drop in SFA intake with age.
One methodological consideration is that nutrient intake estimations in our study were based on chronological age and sex categories. However, 10-year-old children represent a highly heterogeneous group in terms of biological development—some may already be entering puberty, while others remain in early childhood stages. This variability can influence both physiological needs and food preferences. Therefore, interpreting the unexpectedly high intake of saturated and trans fats in this group requires caution. Future research should consider using continuous variables such as BMI-for-age z-scores or biological maturation indicators to better reflect individual differences in growth and metabolic demands.
Notably, children with overweight or obesity showed the highest mean SFA intakes (18.0–18.3 g/day), exceeding the recommendations. This pattern reinforces the link between excess body weight and increased intake of energy-dense snacks, suggesting that BMI may be a more informative marker than age alone in dietary risk assessment. Trends in total fat intake and changes in fatty acid intake among Polish youths aged 11–15 years over a 24-year period were analyzed by Charzewska et al. [
42]. The lowest percentage of energy from fat (EF%) was observed in 1999/2000—34.4% in boys and 32.7% in girls. However, in the most recent study period (2005/2006), an increase was noted—up to 35.1% in boys and 33.7% in girls.
Similar trends were observed in the Korea National Health and Nutrition Examination Survey (KNHANES VI-1-2013) [
43]. Based on 24 h recall data collected from 6406 adolescents between 2007 and 2017, total fat intake increased from 54.3 g (21.7% of energy) to 61.8 g (25.2% of energy). Intakes of saturated fatty acids (SFAs) and monounsaturated fatty acids (MUFAs) also rose—from 17.8 g (7.1% of energy) and 17.2 g (6.8% of energy) to 20.6 g (8.4%) and 20.7 g (8.4%), respectively. The proportion of Korean adolescents consuming more than 30% of total energy from fat increased significantly from 13.7% to 27.5%, with all gender and age groups showing upward trends. Additionally, the percentage of individuals obtaining more than 8% of energy from SFAs rose from 36.0% in 2007–2009 to 49.7% in 2016–2017 [
44].
In contrast, results from the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study showed that cholesterol and total fat intakes among 1590 European adolescents aged 12.5–17.5 years were generally in line with recommendations in both sexes; however, SFA intake exceeded the recommendations by approximately 40% [
45]. Similarly, among adolescents aged 15–18 years living in Gdynia (Poland), SFA intake was within the recommended range of 45.5% of respondents, moderately high in 12%, and very high in 5.8% [
46]. Importantly, high SFA intake in youth has been associated with greater adiposity and increased cardiometabolic risk [
36,
37,
38].
Trans fatty acid (TFA) intake averaged 2.4 g/day, corresponding to more than 90% of the WHO-recommended limit of <1% of total daily energy intake. The highest values were observed in 10-year-olds (3.6 g/day) and in participants with overweight or obesity (2.9–3.2 g/day). These amounts exceed the acceptable intake level of 2.6 g/day and highlight the continued dietary relevance of TFAs despite national efforts to eliminate them. In 2018, the World Health Organization launched the REPLACE initiative to eliminate industrial TFAs. Poland was among the first countries to receive WHO certification for trans fat elimination. However, our findings show that ultra-processed snacks remain a dietary source of TFAs for school-aged children [
47].
It is important to note that our estimates reflect only fat intake from selected snacks and do not capture other dietary sources, which may lead to underestimation of total fat and fatty acid consumption.
Overall, children with overweight or obesity had the highest intakes of total fat, SFAs, and TFAs, which may contribute to excess body weight and long-term metabolic risk. While sex and BMI did not reach statistical significance, visible trends indicate that these groups are more likely to exceed intake recommendations. These results support earlier research linking snack consumption with adiposity in youth [
47] and emphasize the importance of early dietary interventions.
Taken together, our findings underscore the need for targeted nutrition education for children and parents to promote healthier snacking habits early in life. Regulatory efforts to limit the marketing and availability of high-fat snacks, particularly those high in SFAs and TFAs, remain crucial. Interventions should begin before adolescence to prevent excessive intake patterns and reduce the risk of obesity and related chronic diseases.
Limitations of the Study
This study has several limitations that should be considered. First, respondents were recruited from schools located in a single region of Poland, which may limit the generalizability of the results to the broader population of Polish children and adolescents. Second, although the sample size of 362 students was adequate for exploratory purposes, it may not fully capture the heterogeneity of dietary behaviors and socioeconomic backgrounds.
Importantly, data on socioeconomic status, parental education, type of school (public vs. private), and physical activity levels were not collected. These factors may influence food choices and energy requirements, and their absence restricts the depth of interpretation.
Additionally, information on pubertal development was not collected, and no clinical assessment of maturation status was performed. As a result, chronological age was used as a proxy for biological development, which may not accurately reflect individual variability in growth patterns, physiological needs, or dietary preferences, especially in early adolescence. These biological and clinical indicators will be included in our next studies.
Their absence limits the ability to fully contextualize the results and to explore potential interactions between clinical, environmental, behavioral, and nutritional determinants. Future studies should incorporate these variables to provide a more comprehensive understanding of snack-related fat intake among school-aged populations.



 ,
, 

{kind=link}