

The Role of Vitamin D Supplementation in Enhancing Muscle Strength Post-Surgery: A Systemic Review
 , ,
, ,
Abstract
1. Introduction
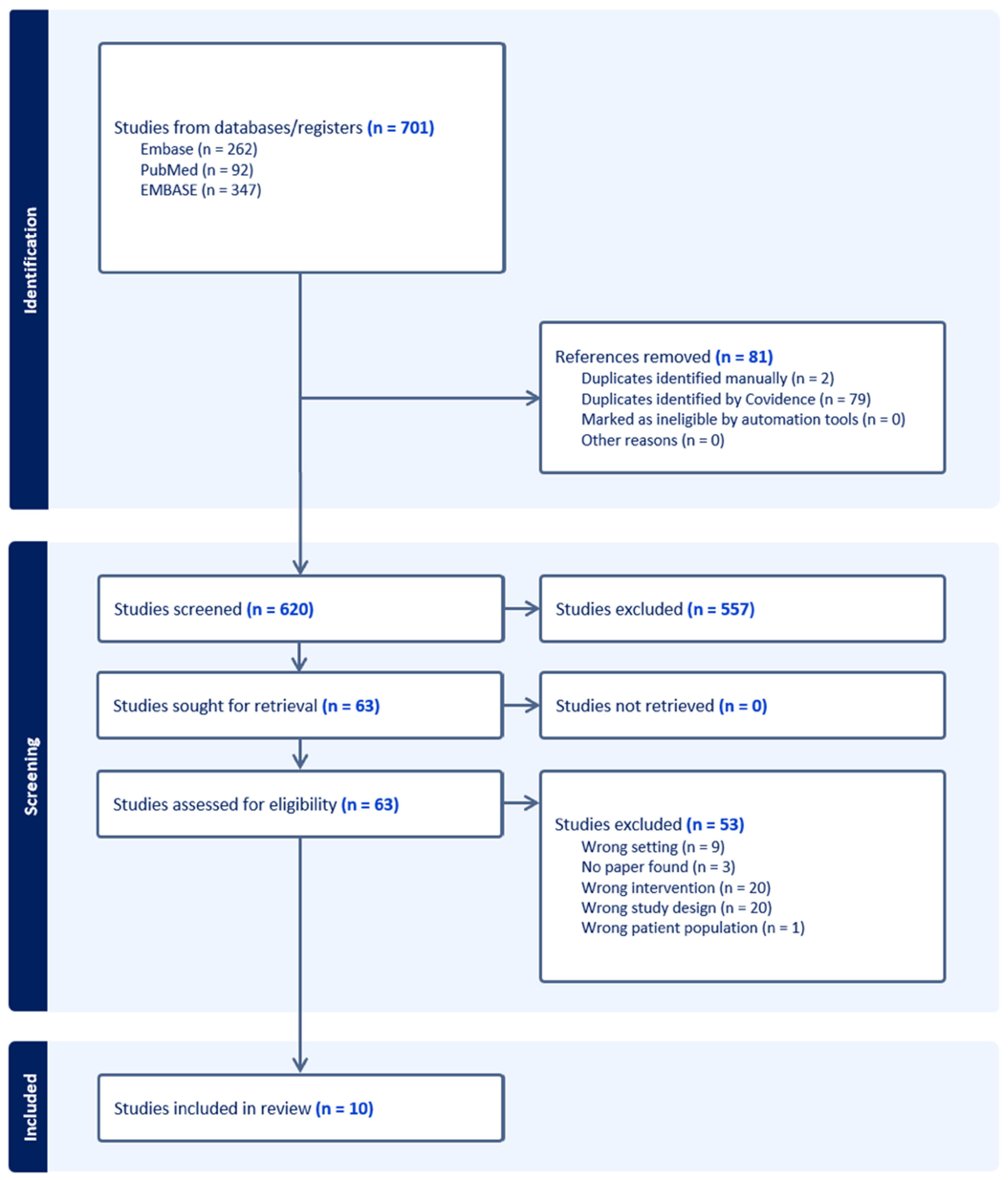
2. Methods
2.1. Information Source and Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Analysis
3. Results
3.1. Role of Preoperative Vitamin D Levels
3.2. Dosage and Timing of Supplementation
3.3. Differential Effects by Type of Surgery
4. Discussion
4.1. Mechanisms Linking Vitamin D to Muscle Strength
4.2. Considerations of Obesity and Vitamin D Bioavailability
4.3. Interplay Between Vitamin D and Other Rehabilitation Factors
4.4. Vitamin D Status in Included Populations
4.5. Clinical Implications
4.6. Research Implications
4.7. Knowledge Gaps
4.8. Strengths and Limitations
5. Conclusions
Supplementary Materials
Funding
Acknowledgments
Conflicts of Interest
References
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, molecular mechanism of action, and pleiotropic effects. Physiol. Rev. 2015, 96, 365–408. [Google Scholar] [CrossRef]
- Girgis, C.M.; Clifton-Bligh, R.J.; Hamrick, M.W.; Holick, M.F.; Gunton, J.E. The Roles of Vitamin D in Skeletal Muscle: Form, Function, and Metabolism. Endocr. Rev. 2012, 34, 33–83. [Google Scholar] [CrossRef] [PubMed]
- Bass, J.J.; Kazi, A.A.; Deane, C.S.; Nakhuda, A.; Ashcroft, S.P.; Brook, M.S.; Wilkinson, D.J.; Phillips, B.E.; Philp, A.; Tarum, J.; et al. The mechanisms of skeletal muscle atrophy in response to transient knockdown of the vitamin D receptor in vivo. J. Physiol. 2020, 599, 963–979. [Google Scholar] [CrossRef]
- Beaudart, C.; Buckinx, F.; Rabenda, V.; Gillain, S.; Cavalier, E.; Slomian, J.; Petermans, J.; Reginster, J.; Bruyère, O. The Effects of Vitamin D on Skeletal Muscle Strength, Muscle Mass, and Muscle Power: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Endocrinol. Metab. 2014, 99, 4336–4345. [Google Scholar] [CrossRef] [PubMed]
- Meara, J.G.; Leather, A.J.; Hagander, L.; Alkire, B.C.; Alonso, N.; Ameh, E.A.; Bickler, S.W.; Conteh, L.; Dare, A.J.; Davies, J.; et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Int. J. Obstet. Anesth. 2015, 25, 75–78. [Google Scholar] [CrossRef]
- Javed, H.; Olanrewaju, O.A.; Owusu, F.A.; Saleem, A.; Pavani, P.; Tariq, H.; Ortiz, B.S.V.; Ram, R.; Varrassi, G. Challenges and Solutions in Postoperative Complications: A narrative review in General surgery. Cureus 2023, 15, e509420. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Gust, C.; Baser, O.; Dimick, J.B.; Sutherland, J.M.; Skinner, J.S. Medicare Payments for common Inpatient Procedures: Implications for Episode-Based Payment Bundling. Health Serv. Res. 2010, 45, 1783–1795. [Google Scholar] [CrossRef]
- Goretti, G.; Marinari, G.M.; Vanni, E.; Ferrari, C. Value-Based healthcare and enhanced recovery after surgery implementation in a High-Volume Bariatric Center in Italy. Obes. Surg. 2020, 30, 2519–2527. [Google Scholar] [CrossRef]
- Lim, C.; Roh, Y.H.; Kim, S.; Nam, K.W. Preoperative Vitamin D Deficiency is Associated with Postoperative Functional Recovery and Complications after Hip Fracture Surgery. J. Bone Metab. 2021, 28, 333–338. [Google Scholar] [CrossRef]
- Argilés, J.M.; Campos, N.; Lopez-Pedrosa, J.M.; Rueda, R.; Rodriguez-Mañas, L. Skeletal muscle regulates metabolism via interorgan Crosstalk: Roles in health and disease. J. Am. Med. Dir. Assoc. 2016, 17, 789–796. [Google Scholar] [CrossRef]
- Finnerty, C.C.; Mabvuure, N.T.; Ali, A.; Kozar, R.A.; Herndon, D.N. The surgically induced stress response. J. Parenter. Enter. Nutr. 2013, 37, 21S–29S. [Google Scholar] [CrossRef]
- Koh, F.H.; Chua, J.M.; Tan, J.L.; Foo, F.; Tan, W.J.; Sivarajah, S.S.; Ho, L.M.L.; Teh, B.; Chew, M. Paradigm shift in gastrointestinal surgery − combating sarcopenia with prehabilitation: Multimodal review of clinical and scientific data. World J. Gastrointest. Surg. 2021, 13, 734–755. [Google Scholar] [CrossRef]
- Demling, R.H. Nutrition, anabolism, and the wound healing process: An overview. Eplasty 2009, 9, e9. [Google Scholar]
- Toh, E.Q.; Wong, H.P.N.; Wang, J.D.J.; Liau, M.Y.Q.; Tan, Y.F.; Shelat, V.G. Prehabilitation programs in liver resection: A narrative review. Chin. Clin. Oncol. 2024, 13, 9. [Google Scholar] [CrossRef] [PubMed]
- Hogenbirk, R.N.M.; Van Der Plas, W.Y.; Hentzen, J.E.K.R.; Van Wijk, L.; Wijma, A.G.; Buis, C.I.; Viddeleer, A.R.; De Bock, G.H.; Van Der Schans, C.P.; Van Dam, G.M.; et al. Postoperative muscle loss, protein intake, physical activity and outcome associations. Br. J. Surg. 2022, 110, 183–192. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Bernabei, R.; Onder, G.; Marzetti, E. Sarcopenia as the Biological Substrate of Physical Frailty. Clin. Geriatr. Med. 2015, 31, 367–374. [Google Scholar] [CrossRef]
- Agoncillo, M.; Yu, J.; Gunton, J.E. The role of Vitamin D in skeletal muscle repair and regeneration in animal models and Humans: A systematic review. Nutrients 2023, 15, 4377. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, O.; Yanık, S.; Bebitoğlu, B.T.; Akyüz, E.Y.; Dokuyucu, A.; Erdem, Ş. Effect of Calcium β-Hydroxy-β-Methylbutyrate (CaHMB), Vitamin D, and Protein Supplementation on Postoperative Immobilization in Malnourished Older Adult Patients With Hip Fracture. Nutr. Clin. Pract. 2016, 31, 829–835. [Google Scholar] [CrossRef]
- Moon, A.S.; Boudreau, S.; Mussell, E.; He, J.K.; Brabston, E.W.; Ponce, B.A.; Momaya, A.M. Current concepts in vitamin D and orthopaedic surgery. Orthop. Traumatol. Surg. Res. 2019, 105, 375–382. [Google Scholar] [CrossRef]
- Patel, A.; Caruana, E.J.; Hodson, J.; Morrison, R.; Khor, B.; Gysling, S.; Trevis, J.; Mangel, T.; Benson, R.; Zakeri, R.; et al. Role of vitamin D supplementation in modifying outcomes after surgery: A systematic review of randomised controlled trials. BMJ Open 2024, 14, e073431. [Google Scholar] [CrossRef]
- Hedström, M.; Sjöberg, K.; Brosjö, E.; Åström, K.; Sjöberg, H.; Dalén, N. Positive effects of anabolic steroids, vitamin D and calcium on muscle mass, bone mineral density and clinical function after a hip fracture: A randomised study of 63 women. J. Bone Jt. Surg. -Br. Vol. 2002, 84, 497–503. [Google Scholar] [CrossRef]
- Stoker, G.E.; Buchowski, J.M.; Bridwell, K.H.; Lenke, L.G.; Riew, K.D.; Zebala, L.P. Preoperative vitamin D status of adults undergoing surgical spinal fusion. Spine 2012, 38, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Flodin, L.; Cederholm, T.; Sääf, M.; Samnegård, E.; Ekström, W.; Al-Ani, A.N.; Hedström, M. Effects of protein-rich nutritional supplementation and bisphosphonates on body composition, handgrip strength and health-related quality of life after hip fracture: A 12-month randomized controlled study. BMC Geriatr. 2015, 15, 149. [Google Scholar] [CrossRef]
- Maniar, R.N.; Patil, A.M.; Maniar, A.R.; Gangaraju, B.; Singh, J. Effect of Preoperative Vitamin D Levels on Functional Performance after Total Knee Arthroplasty. Clin. Orthop. Surg. 2016, 8, 153. [Google Scholar] [CrossRef]
- Fischer, K.; Trombik, M.; Freystätter, G.; Egli, A.; Theiler, R.; Bischoff-Ferrari, H. Timeline of functional recovery after hip fracture in seniors aged 65 and older: A prospective observational analysis. Osteoporos. Int. 2019, 30, 1371–1381. [Google Scholar] [CrossRef]
- Lee, M.H.; Gong, H.S.; Lee, M.H.; Cho, K.J.; Kim, J.; Baek, G.H. The effect of vitamin D deficiency correction on the outcomes in women after Carpal Tunnel release. J. Hand Surg. 2019, 44, 649–654. [Google Scholar] [CrossRef]
- Smelt, H.J.M.; Pouwels, S.; Celik, A.; Gupta, A.; Smulders, J.F. Assessment of Physical Fitness after Bariatric Surgery and Its Association with Protein Intake and Type of Cholecalciferol Supplementation. Medicina 2019, 55, 281. [Google Scholar] [CrossRef] [PubMed]
- Stemmle, J.; Marzel, A.; Chocano-Bedoya, P.O.; Orav, E.J.; Dawson-Hughes, B.; Freystaetter, G.; Egli, A.; Theiler, R.; Staehelin, H.B.; Bischoff-Ferrari, H.A. Effect of 800 IU versus 2000 IU vitamin D3 with or without a simple home exercise program on functional recovery after hip fracture: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2018, 20, 530–536.e1. [Google Scholar] [CrossRef]
- Schiavo, L.; Santella, B.; Paolini, B.; Rahimi, F.; Giglio, E.; Martinelli, B.; Boschetti, S.; Bertolani, L.; Gennai, K.; Arolfo, S.; et al. Adding Branched-Chain Amino Acids and Vitamin D to Whey Protein Is More Effective than Protein Alone in Preserving Fat Free Mass and Muscle Strength in the First Month after Sleeve Gastrectomy. Nutrients 2024, 16, 1448. [Google Scholar] [CrossRef]
- Birinci, M.; Hakyemez, Ö.S.; Geçkalan, M.A.; Mutlu, M.; Yildiz, F.; Bilgen, Ö.F.; Azboy, İ. Effect of vitamin D deficiency on periprosthetic joint infection and complications after primary total joint arthroplasty. J. Arthroplast. 2024, 39, S151–S157. [Google Scholar] [CrossRef]
- Iglar, P.J.; Hogan, K.J. Vitamin D status and surgical outcomes: A systematic review. Patient Saf. Surg. 2015, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Poon, C.C.; Wong, M.; Li, W.; Guo, Y.; Zhang, Y. Vitamin D supplementation Improves handgrip Strength in Postmenopausal Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Endocrinol. 2022, 13, 863448. [Google Scholar] [CrossRef] [PubMed]
- Gatt, T.; Grech, A.; Arshad, H. The effect of vitamin D supplementation for bone healing in fracture patients: A systematic review. Adv. Orthop. 2023, 2023, 6236045. [Google Scholar] [CrossRef] [PubMed]
- Latham, C.M.; Brightwell, C.R.; Keeble, A.R.; Munson, B.D.; Thomas, N.T.; Zagzoog, A.M.; Fry, C.S.; Fry, J.L. Vitamin D Promotes Skeletal Muscle Regeneration and Mitochondrial Health. Front. Physiol. 2021, 12, 660498. [Google Scholar] [CrossRef]
- Salles, J.; Chanet, A.; Guillet, C.; Vaes, A.M.; Brouwer-Brolsma, E.M.; Rocher, C.; Giraudet, C.; Patrac, V.; Meugnier, E.; Montaurier, C.; et al. Vitamin D status modulates mitochondrial oxidative capacities in skeletal muscle: Role in sarcopenia. Commun. Biol. 2022, 5, 1288. [Google Scholar] [CrossRef]
- Uchitomi, R.; Oyabu, M.; Kamei, Y. Vitamin D and Sarcopenia: Potential of Vitamin D Supplementation in Sarcopenia Prevention and Treatment. Nutrients 2020, 12, 3189. [Google Scholar] [CrossRef]
- Dzik, K.P.; Kaczor, J.J. Mechanisms of vitamin D on skeletal muscle function: Oxidative stress, energy metabolism and anabolic state. Eur. J. Appl. Physiol. 2019, 119, 825–839. [Google Scholar] [CrossRef]
- Widajanti, N.; Hadi, U.; Soelistijo, N.S.A.; Syakdiyah, N.N.H.; Rosaudyn, N.R.; Putra, N.H.B.P. The Effect of Vitamin D Supplementation to Parameter of Sarcopenia in Elderly People: A Systematic Review and Meta-Analysis. Can. Geriatr. J. 2024, 27, 63–75. [Google Scholar] [CrossRef]
- Park, C.Y.; Han, S.N. The role of vitamin D in adipose tissue biology: Adipocyte differentiation, energy metabolism, and inflammation. J. Lipid Atheroscler. 2021, 10, 130. [Google Scholar] [CrossRef]
- Carrelli, A.; Bucovsky, M.; Horst, R.; Cremers, S.; Zhang, C.; Bessler, M.; Schrope, B.; Evanko, J.; Blanco, J.; Silverberg, S.J.; et al. Vitamin D storage in adipose tissue of obese and normal weight women. J. Bone Miner. Res. 2016, 32, 237–242. [Google Scholar] [CrossRef]
- Wei, S.; Nguyen, T.T.; Zhang, Y.; Ryu, D.; Gariani, K. Sarcopenic obesity: Epidemiology, pathophysiology, cardiovascular disease, mortality, and management. Front. Endocrinol. 2023, 14, 1185221. [Google Scholar] [CrossRef] [PubMed]
- Abidin, N.Z.; Mitra, S.R. Total vs. Bioavailable: Determining a Better 25(OH)D Index in Association with Bone Density and Muscle Mass in Postmenopausal Women. Metabolites 2020, 11, 23. [Google Scholar] [CrossRef]
- Holmes, C.J.; Racette, S.B. The Utility of body composition assessment in nutrition and Clinical Practice: An Overview of Current Methodology. Nutrients 2021, 13, 2493. [Google Scholar] [CrossRef] [PubMed]
- Sadat-Ali, M.; AlTabash, K.W.; Al-Turki, H.A.; AlMousa, S.A.; AlSayed, H.N. Time out: Should vitamin D dosing be based on patient’s body mass index (BMI): A prospective controlled study. J. Nutr. Sci. 2021, 10, e106. [Google Scholar] [CrossRef]
- Chakhtoura, M.T.; Nakhoul, N.; Akl, E.A.; Mantzoros, C.S.; Fuleihan, G.A.E.H. Guidelines on vitamin D replacement in bariatric surgery: Identification and systematic appraisal. Metabolism 2016, 65, 586–597. [Google Scholar] [CrossRef]
- James, W.J.D.; Shaik, A.A.F.; Matthew, T.Y.; Yin, L.Y.; Voi, T.K. A Systematic Review and Meta-Analysis on the impact of preserving the hepatic branch of the vagus nerve in upper gastrointestinal surgeries. Foregut J. Am. Foregut Soc. 2024, 4, 428–441. [Google Scholar] [CrossRef]
- Mesinovic, J.; Rodriguez, A.J.; Cervo, M.M.; Gandham, A.; Xu, C.L.; Glavas, C.; De Courten, B.; Zengin, A.; Ebeling, P.R.; Scott, D. Vitamin D supplementation and exercise for improving physical function, body composition and metabolic health in overweight or obese older adults with vitamin D deficiency: A pilot randomized, double-blind, placebo-controlled trial. Eur. J. Nutr. 2022, 62, 951–964. [Google Scholar] [CrossRef]
- Fleet, J.L.; McIntyre, A.; Janzen, S.; Saikaley, M.; Qaqish, M.; Cianfarani, R.; Papaioannou, A. A systematic review examining the effect of vitamin D supplementation on functional outcomes post-stroke. Clin. Rehabil. 2023, 37, 1451–1466. [Google Scholar] [CrossRef]
- Bendotti, G.; Biamonte, E.; Leporati, P.; Goglia, U.; Ruggeri, R.M.; Gallo, M. Vitamin D supplementation: Practical advice in different clinical settings. Nutrients 2025, 17, 783. [Google Scholar] [CrossRef]
- Giustina, A.; Di Filippo, L.; Facciorusso, A.; Adler, R.A.; Binkley, N.; Bollerslev, J.; Bouillon, R.; Casanueva, F.F.; Cavestro, G.M.; Chakhtoura, M.; et al. Vitamin D status and supplementation before and after Bariatric Surgery: Recommendations based on a systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2023, 24, 1011–1029. [Google Scholar] [CrossRef]
- Mayo, B.C.; Massel, D.H.; Yacob, A.; Narain, A.S.; Hijji, F.Y.; Jenkins, N.W.; Parrish, J.M.; Modi, K.D.; Long, W.W.; Hrynewycz, N.M.; et al. A review of Vitamin D in Spinal Surgery: Deficiency Screening, treatment, and outcomes. Int. J. Spine Surg. 2020, 14, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Trummer, C.; Theiler-Schwetz, V.; Grübler, M.R.; Verheyen, N.D.; Odler, B.; Karras, S.N.; Zittermann, A.; März, W. Critical appraisal of large vitamin D randomized controlled trials. Nutrients 2022, 14, 303. [Google Scholar] [CrossRef] [PubMed]
- Vaughan-Shaw, P.G.; Buijs, L.F.; Blackmur, J.P.; Ewing, A.; Becher, H.; Theodoratou, E.; Ooi, L.Y.; Din, F.V.N.; Farrington, S.M.; Dunlop, M.G. A feasibility study of perioperative vitamin D supplementation in patients undergoing colorectal cancer resection. Front. Nutr. 2023, 10, 1106431. [Google Scholar] [CrossRef] [PubMed]
- Mousa, H.; Saei, A.A.; Razali, R.M.; Zughaier, S.M. Vitamin D status affects proteomic profile of HDL-associated proteins and inflammatory mediators in dyslipidemia. J. Nutr. Biochem. 2023, 123, 109472. [Google Scholar] [CrossRef]
- Kerezoudis, P.; Rinaldo, L.; Drazin, D.; Kallmes, D.; Krauss, W.; Hassoon, A.; Bydon, M. Association between vitamin D deficiency and outcomes following spinal fusion surgery: A systematic review. World Neurosurg. 2016, 95, 71–76. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]

{kind=link}
| References | Title of Study | Year | Authors | Type of Study | Country | Type of Surgery | Dose of Vitamin D | Key Outcomes Measured | JBI Score |
|---|---|---|---|---|---|---|---|---|---|
| [21] | Positive Effects of Anabolic Steroids, Vitamin D, and Calcium on Muscle Mass, Bone Mineral Density, and Clinical Function After a Hip Fracture: A Randomised Study of 63 Women | 2002 | Hedstrom, M, Sjoberg, K, Brosjo, E, Astrom, K, Sjoberg, H, Dalen, N | Randomised Controlled Trial | Sweden | Orthopaedics, Hip Replacement | 1-alpha-hydroxylated vitamin D3 (alphacalcidol 0.25 g) |
| 11/13 |
| [22] | Preoperative Vitamin D Status in Adults Undergoing Spinal Fusion | 2011 | Buchowski J., Stoker G., Bridwell K., Lenke L., Daniel Riew K.K., Zebala L. | Cohort Study | United States | Orthopaedics, Spinal Fusion | Vitamin D deficiency defined as <20 ng/mL; supplementation regimen: 50,000 IU D2 (ergocalciferol) |
| 10/11 |
| [23] | Effects of Protein-Rich Nutritional Supplementation and Bisphosphonates on Body Composition, Handgrip Strength, and Quality of Life After Hip Fracture: A 12-month Randomised Controlled Study | 2015 | Flodin L, Cederholm T, Sääf M, Samnegård E, Ekström W, Al-Ani AN, Hedström M | Randomised Controlled Trial | Sweden | Orthopaedics, Hip Replacement | 800 IU daily vitamin D3 for all study groups |
| 11/13 |
| [24] | Effect of Preoperative Vitamin D Levels on Functional Performance After Total Knee Arthroplasty | 2016 | Maniar RN, Patil AM, Maniar AR, Gangaraju B, Singh J | Cohort Study | India | Orthopaedics, Knee Replacement | Vitamin D supplementation postoperatively (0.5 µg/day) |
| 10/11 |
| [25] | Timeline of Functional Recovery After Hip Fracture in Seniors Aged 65 and Older: A Prospective Observational Analysis | 2019 | Fischer K, Trombik M, Freystätter G, Egli A, Theiler R, Bischoff-Ferrari HA | Randomised Controlled Trial | Switzerland | Orthopaedics, Hip Replacement | 800 IU or 2000 IU daily of vitamin D3 (from primary study protocol) |
| 10/11 |
| [26] | The Effect of Vitamin D Deficiency Correction on the Outcomes in Women After Carpal Tunnel Release | 2019 | Lee MH, Gong HS, Cho KJ, Kim J, Baek GH | Cohort Study | South Korea | Orthopaedics, Carpal Tunnel Release | 1000 IU daily vitamin D3 for six months |
| 10/11 |
| [27] | Assessment of Physical Fitness After Bariatric Surgery and Its Association With Protein Intake and Type of Cholecalciferol Supplementation | 2019 | Smelt HJM, Pouwels S, Celik A, Gupta A, Smulders JF | Cohort Study | Netherlands | General Surgery, Bariatric Surgery | Group A: 800 IU daily; Group B: 800 IU daily + 50,000 IU monthly vitamin D3 |
| 10/11 |
| [28] | Effect of 800 IU Versus 2000 IU Vitamin D3 With or Without a Simple Home Exercise Program on Functional Recovery After Hip Fracture: A Randomised Controlled Trial | 2019 | Stemmle J, Marzel A, Chocano-Bedoya PO, Orav EJ, Dawson-Hughes B, Freystaetter G, Egli A, Theiler R, Staehelin HB, Bischoff-Ferrari HA | Randomised Controlled Trial | Switzerland | Orthopaedics, Hip Replacement | 800 IU or 2000 IU daily of vitamin D3 |
| 11/13 |
| [29] | Adding Branched-Chain Amino Acids and Vitamin D to Whey Protein Is More Effective Than Protein Alone in Preserving Fat-Free Mass and Muscle Strength After Sleeve Gastrectomy | 2024 | Schiavo L, Santella B, Paolini B; Rahimi F, Giglio E, Martinelli B, Boschetti S, Bertolani L, Gennai K, Arolfo S, Bertani MP, Pilone V | Cohort Study | Italy | General Surgery, Gastrectomy | Vitamin D dose integrated into supplementation regimen (2000 IU) |
| 11/13 |
| [30] | Effect of Vitamin D Deficiency on Periprosthetic Joint Infection and Complications After Primary Total Joint Arthroplasty | 2024 | Birinci M., Hakyemez O.S., Geckalan M.A., Mutlu M.; Yildiz F.; Bilgen O.F., Azboy I. | Cohort Study | Turkey | Orthopaedics, Hip Or Knee Replacement | Vitamin D deficiency corrected with a single dose of 300,000 IU D3 two weeks preoperatively |
| 10/11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.J.-D.; Quak, G.S.-W.; Lee, H.-B.; Foo, L.-X.; Tay, P.; Mah, S.-M.; Tong, C.; Koh, F.H.-X. The Role of Vitamin D Supplementation in Enhancing Muscle Strength Post-Surgery: A Systemic Review. Nutrients 2025, 17, 1512. https://doi.org/10.3390/nu17091512
Wang JJ-D, Quak GS-W, Lee H-B, Foo L-X, Tay P, Mah S-M, Tong C, Koh FH-X. The Role of Vitamin D Supplementation in Enhancing Muscle Strength Post-Surgery: A Systemic Review. Nutrients. 2025; 17(9):1512. https://doi.org/10.3390/nu17091512
Chicago/Turabian StyleWang, James Jia-Dong, Glenys Shu-Wei Quak, Hui-Bing Lee, Li-Xin Foo, Phoebe Tay, Shi-Min Mah, Cherie Tong, and Frederick Hong-Xiang Koh. 2025. "The Role of Vitamin D Supplementation in Enhancing Muscle Strength Post-Surgery: A Systemic Review" Nutrients 17, no. 9: 1512. https://doi.org/10.3390/nu17091512
APA StyleWang, J. J.-D., Quak, G. S.-W., Lee, H.-B., Foo, L.-X., Tay, P., Mah, S.-M., Tong, C., & Koh, F. H.-X. (2025). The Role of Vitamin D Supplementation in Enhancing Muscle Strength Post-Surgery: A Systemic Review. Nutrients, 17(9), 1512. https://doi.org/10.3390/nu17091512