
Customizing Nutrients: Vitamin D and Iron Deficiencies in Overweight and Obese Children—Insights from a Romanian Study

Highlights
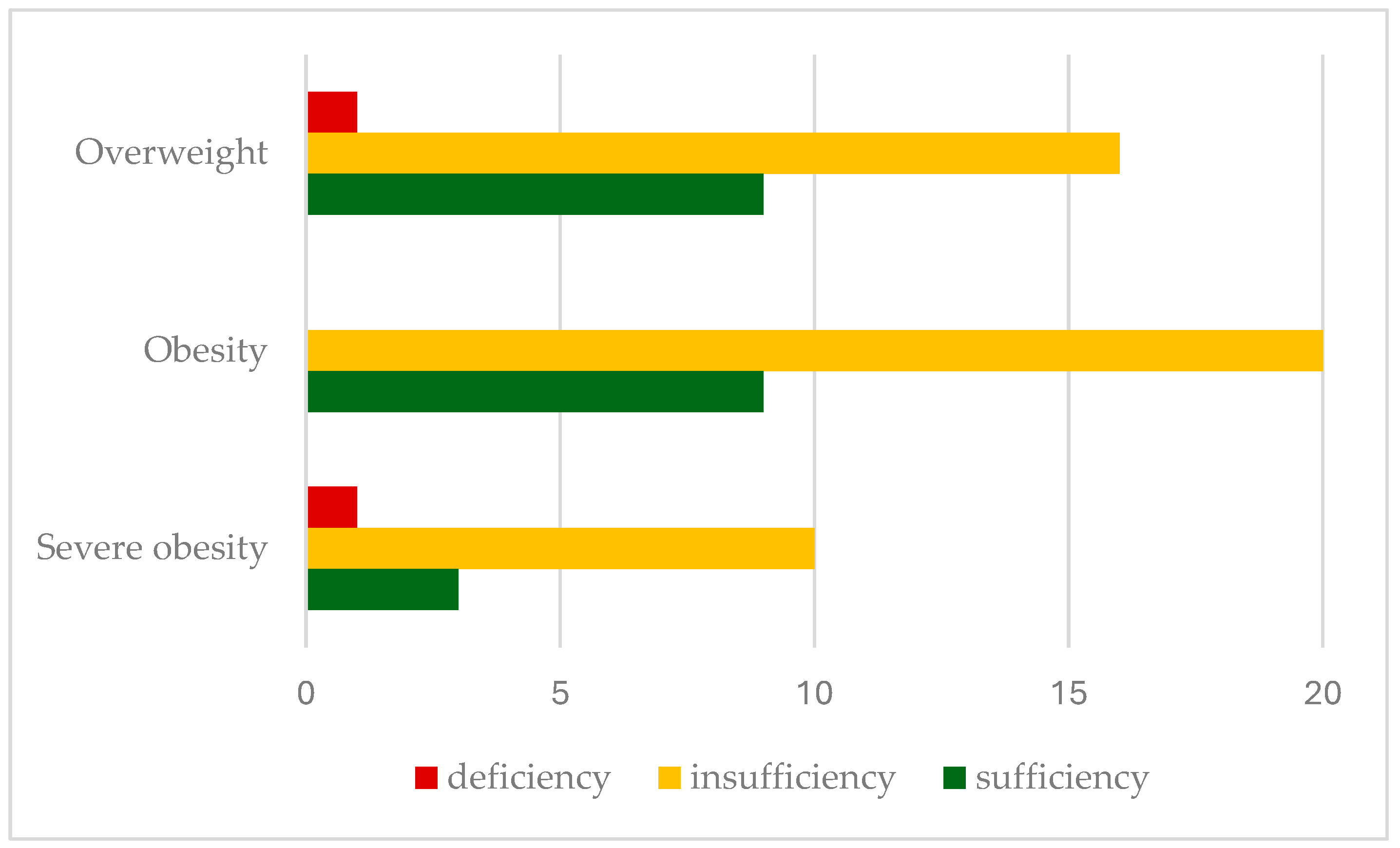
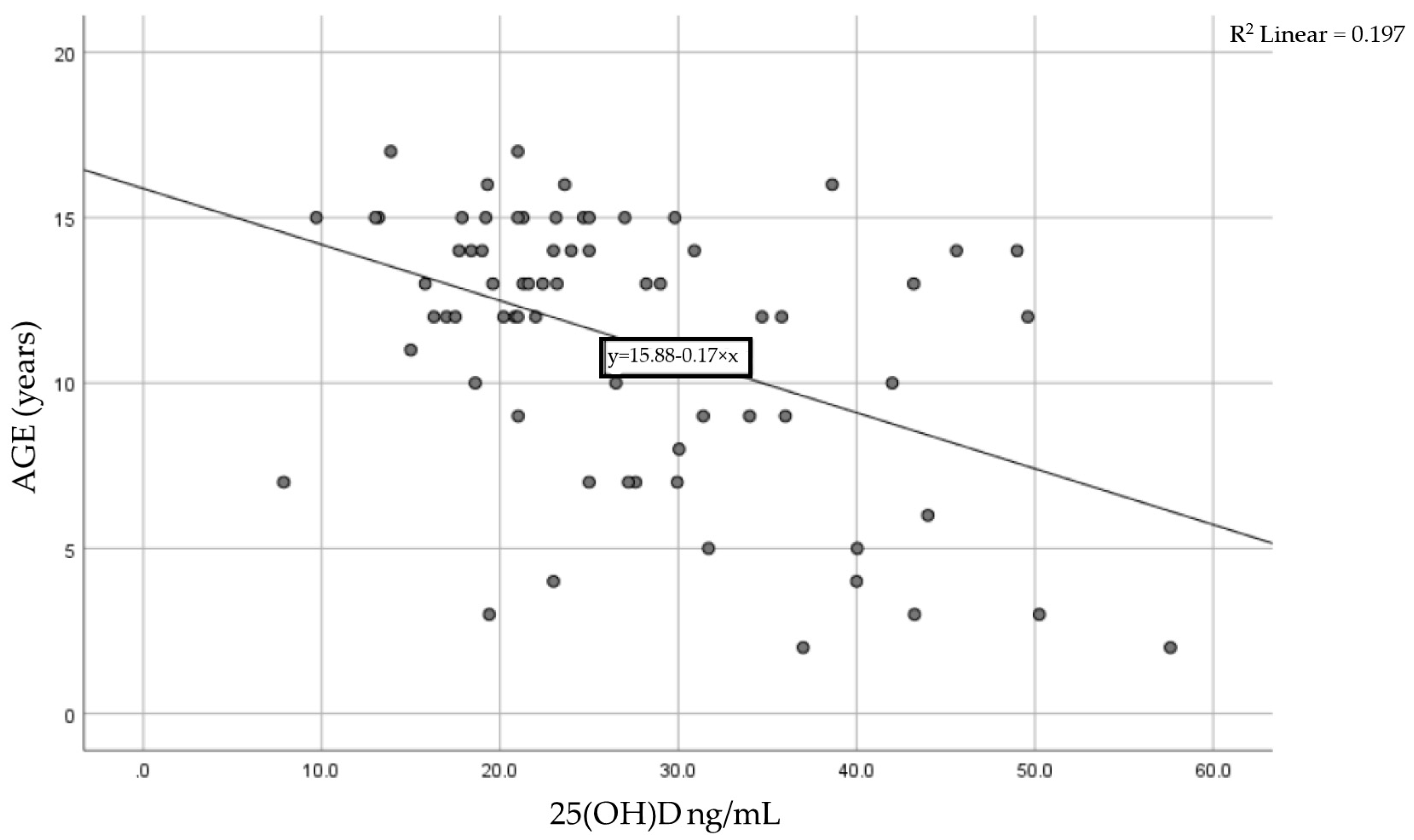
- Vitamin D insufficiency is highly prevalent in severely obese children, with significantly lower serum 25(OH)D levels recorded as BMI increases.
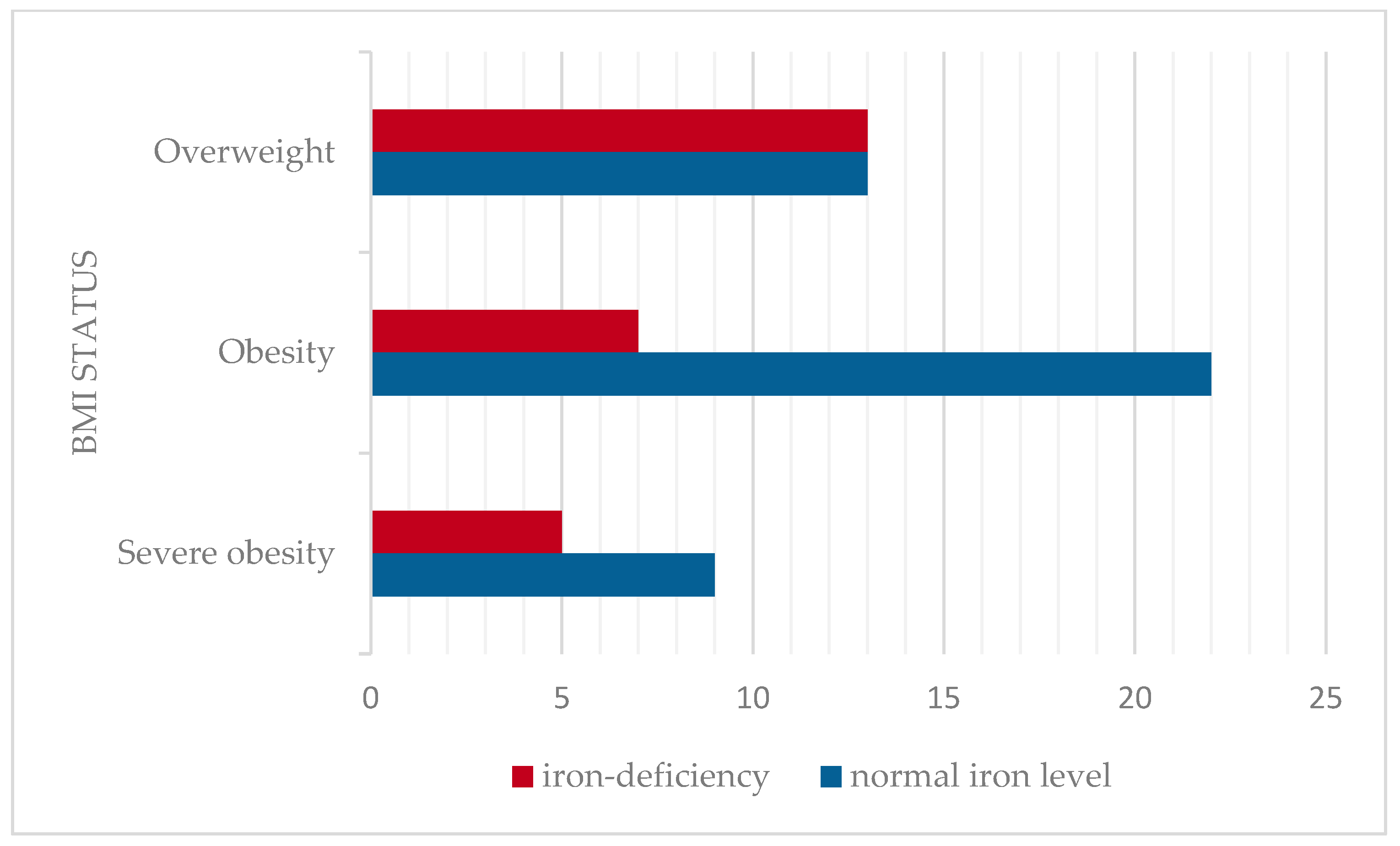
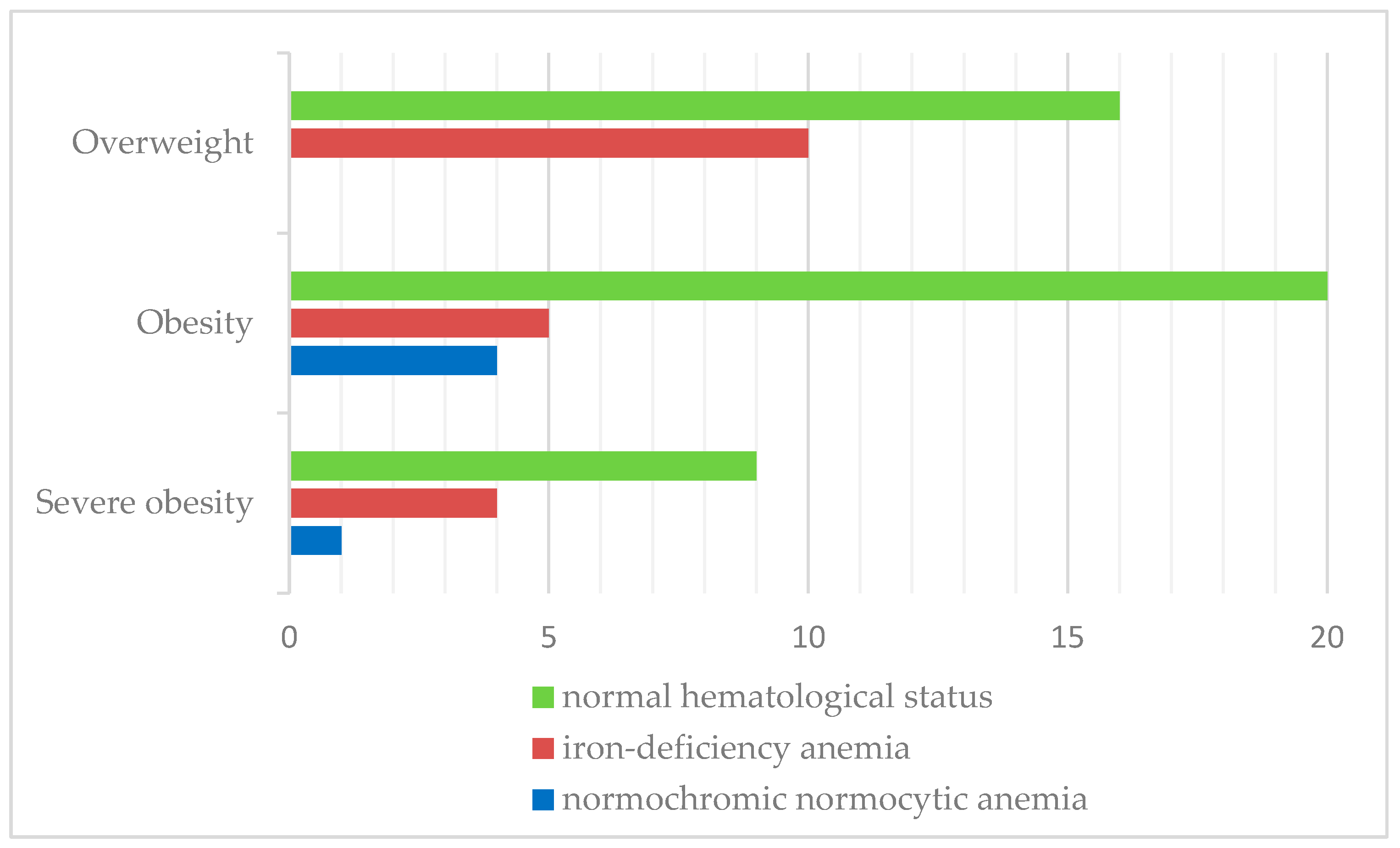
- Iron deficiency and iron deficiency anemia were both more prevalent in overweight subjects, suggesting that adipose tissue contributes to chronic inflammation.
- The findings of the present study emphasize the need for targeted screening for iron and vitamin D deficiencies in overweight/obese children, combined with appropriate dietary interventions and supplementation for these high-risk groups.
- The main findings highlight the potential for future research, including interventional studies, to assess the effects of supplementation on metabolic outcomes.
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Samples Collection
2.3. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| 25(OH)D | 25-hydroxyvitamin D |
| CDC2022 | The Centers for Disease Control |
| MCV | Mean Corpuscular Volume |
| MCH | Mean Corpuscular Hemoglobin |
| SD | Standard Deviation |
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Gillis, L.; Gillis, A. Nutrient Inadequacy in Obese and Non-Obese Youth. Can. J. Diet. Pract. Res. 2007, 66, 237–242. [Google Scholar] [CrossRef]
- Gregg, E.W.; Shaw, J.E. Global Health Effects of Overweight and Obesity. N. Engl. J. Med. 2017, 377, 80–81. [Google Scholar] [CrossRef]
- Constantin, A.T.; Delia, C.; Tudor, L.M.; Rosca, I.; Irimie, A.D.; Năstase, L.; Gherghina, I. Dyslipidemia in Pediatric Patients: A Cross-Sectional Study. Medicina 2023, 59, 1434. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Kunutsor, S.; Franco, O.H.; Chowdhury, R. Vitamin D, type 2 diabetes and other metabolic outcomes: A systematic review and meta-analysis of prospective studies. Proc. Nutr. Soc. 2013, 72, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Arhire, A.I.; Ioacara, D.S.; Papuc, T.; Parcalibioru, G.G.; Fica, S. Exploring the severity and early onset of familial type 1 diabetes in Romania: Genetic and microbiota insights. Arch. Clin. Cases 2024, 11, 29–33. [Google Scholar] [CrossRef]
- Belykh, N.A.; Blokhova, E.E. Vitamin D status and calcium-phosphoric metabolism in children with excessive body weight and obesity. Vopr. Pitan. 2021, 90, 83–90. [Google Scholar] [CrossRef]
- Calcaterra, V.; Verduci, E.; Milanta, C.; Agostinelli, M.; Todisco, C.F.; Bona, F.; Dolor, J.; La Mendola, A.; Tosi, M.; Zuccotti, G. Micronutrient Deficiency in Children and Adolescents with Obesity—A Narrative Review. Children 2023, 10, 695. [Google Scholar] [CrossRef]
- Turer, C.B.; Lin, H.; Flores, G. Prevalence of vitamin D deficiency among overweight and obese US children. Pediatrics 2013, 131, e152–e161. [Google Scholar] [CrossRef]
- Pereira-Santos, M.; Costa, P.R.F.; Assis, A.M.O.; Santos, C.A.S.T.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef]
- Corsello, A.; Macchi, M.; D’Oria, V.; Pigazzi, C.; Alberti, I.; Treglia, G.; De Cosmi, V.; Mazzocchi, A.; Agostoni, C.; Milani, G.P. Effects of vitamin D supplementation in obese and overweight children and adolescents: A systematic review and meta-analysis. Pharmacol. Res. 2023, 192, 106793. [Google Scholar] [CrossRef] [PubMed]
- Migliaccio, S.; Di Nisio, A.; Mele, C.; Scappaticcio, L.; Savastano, S.; Colao, A. Obesity and hypovitaminosis D: Causality or casualty? Int. J. Obes. Suppl. 2019, 9, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Olson, M.L.; Maalouf, N.M.; Oden, J.D.; White, P.C.; Hutchison, M.R. Vitamin D deficiency in obese children and its relationship to glucose homeostasis. J. Clin. Endocrinol. Metab. 2012, 97, 279–285. [Google Scholar] [CrossRef]
- Rusconi, R.E.; De Cosmi, V.; Gianluca, G.; Giavoli, C.; Agostoni, C. Vitamin D insufficiency in obese children and relation with lipid profile. Int. J. Food Sci. Nutr. 2015, 66, 132–134. [Google Scholar] [CrossRef]
- Richardson, M.W.; Ang, L.; Visintainer, P.F.; Wittcopp, C.A. The abnormal measures of iron homeostasis in pediatric obesity are associated with the inflammation of obesity. Int. J. Pediatr. Endocrinol. 2009, 2009, 713269. [Google Scholar] [CrossRef] [PubMed]
- McCann, J.C.; Ames, B.N. An overview of evidence for a causal relation between iron deficiency during development and deficits in cognitive or behavioral function. Am. J. Clin. Nutr. 2007, 85, 931–945. [Google Scholar] [CrossRef]
- Alshwaiyat, N.M.; Ahmad, A.; Wan Hassan, W.M.R.; Al-Jamal, H.A.N. Association between obesity and iron deficiency (Review). Exp. Ther. Med. 2021, 22, 1268. [Google Scholar] [CrossRef]
- Saad, R.A.; Qutob, H.M.H. The relationship between anemia and obesity. Expert Rev. Hematol. 2022, 15, 911–926. [Google Scholar] [CrossRef]
- Nead, K.G.; Halterman, J.S.; Kaczorowski, J.M.; Auinger, P.; Weitzman, M. Overweight children and adolescents: A risk group for iron deficiency. Pediatrics 2004, 114, 104–108. [Google Scholar] [CrossRef]
- Pinhas-Hamiel, O.; Newfield, R.S.; Koren, I.; Agmon, A.; Lilos, P.; Phillip, M. Greater prevalence of iron deficiency in overweight and obese children and adolescents. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 416–418. [Google Scholar] [CrossRef]
- Aeberli, I.; Hurrell, R.F.; Zimmermann, M.B. Overweight children have higher circulating hepcidin concentrations and lower iron status but have dietary iron intakes and bioavailability comparable with normal weight children. Int. J. Obes. 2009, 33, 1111–1117. [Google Scholar] [CrossRef]
- Aigner, E.; Feldman, A.; Datz, C. Obesity as an emerging risk factor for iron deficiency. Nutrients 2014, 6, 3587–3600. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T.; Nemeth, E. Iron imports. IV. Hepcidin and regulation of body iron metabolism. Am. J. Physiol. Gastrointest. Liver Physiol. 2006, 290, G199–G203. [Google Scholar] [CrossRef]
- Growth Charts—CDC Extended BMI-for-Age Growth Charts. Available online: https://www.cdc.gov/growthcharts/extended-bmi.htm (accessed on 25 February 2025).
- Shields, M.; Tremblay, M.S. Canadian childhood obesity estimates based on WHO, IOTF and CDC cut-points. Int. J. Pediatr. Obes. 2010, 5, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Fiamenghi, V.I.; de Mello, E.D. Vitamin D deficiency in children and adolescents with obesity: A meta-analysis. J. Pediatr. 2021, 97, 273–279. [Google Scholar] [CrossRef]
- Gilbert-Diamond, D.; Baylin, A.; Mora-Plazas, M.; Marin, C.; Arsenault, J.E.; Hughes, M.D.; Willett, W.C.; Villamor, E. Vitamin D deficiency and anthropometric indicators of adiposity in school-age children: A prospective study. Am. J. Clin. Nutr. 2010, 92, 1446–1451. [Google Scholar] [CrossRef] [PubMed]
- Cediel, G.; Pacheco-Acosta, J.; Castillo-Durán, C. Vitamin D deficiency in pediatric clinical practice. Arch Argent Pediatr. 2018, 116, e75–e81. [Google Scholar] [CrossRef]
- Marginean, C.D.; Tomsa, N.; Aron, B.; Ciobanu, D.; Melit, L.E. Demographic, anthropometric and laboratory characteristics in obese children. Rom. J. Pediatr. 2020, 69, 64–68. [Google Scholar] [CrossRef]
- Lenders, C.M.; Feldman, H.A.; Von Scheven, E.; Merewood, A.; Sweeney, C.; Wilson, D.M.; Lee, P.D.; Abrams, S.H.; Gitelman, S.E.; Wertz, M.S.; et al. Relation of body fat indexes to vitamin D status and deficiency among obese adolescents. Am. J. Clin. Nutr. 2009, 90, 459–467. [Google Scholar] [CrossRef]
- Sarı, E.; Çoban, G.; Öztek Çelebi, F.Z.; Altınel Açoğlu, E. The Status of Vitamin D Among Children Aged 0 to 18 Years. J. Pediatr. Res. 2021, 8, 438–443. [Google Scholar] [CrossRef]
- Durá-Travé, T.; Gallinas-Victoriano, F.; Chueca-Guindulain, M.J.; Berrade-Zubiri, S. Prevalence of hypovitaminosis D and associated factors in obese Spanish children. Nutr. Diabetes 2017, 7, e248. [Google Scholar] [CrossRef] [PubMed]
- Alemzadeh, R.; Kichler, J.; Babar, G.; Calhoun, M. Hypovitaminosis D in obese children and adolescents: Relationship with adiposity, insulin sensitivity, ethnicity, and season. Metabolism 2008, 57, 183–191. [Google Scholar] [CrossRef]
- Chen, Z.; Lv, X.; Hu, W.; Qian, X.; Wu, T.; Zhu, Y. Vitamin D Status and Its Influence on the Health of Preschool Children in Hangzhou. Front. Public Health 2021, 9, 675403. [Google Scholar] [CrossRef] [PubMed]
- Durá-Travé, T.; Gallinas-Victoriano, F. Vitamin D deficiency in adolescents with obesity - Altered metabolism or environmental factors? Nutr. Hosp. 2023, 40, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Barja-Fernández, S.; Aguilera, C.M.; Martínez-Silva, I.; Vazquez, R.; Gil-Campos, M.; Olza, J.; Bedoya, J.; Cadarso-Suárez, C.; Gil, Á.; Seoane, L.M.; et al. 25-Hydroxyvitamin D levels of children are inversely related to adiposity assessed by body mass index. J. Physiol. Biochem. 2018, 74, 111–118. [Google Scholar] [CrossRef]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef]
- Coelho, S.R.; Faria, J.C.P.; Fonseca, F.L.A.; De Souza, F.I.S.; Sarni, R.O.S. Is There an Association between Vitamin D Concentrations and Overweight in Children and Adolescents? J. Trop. Pediatr. 2022, 68, fmac033. [Google Scholar] [CrossRef]
- Pacifico, L.; Anania, C.; Osborn, J.F.; Ferraro, F.; Bonci, E.; Olivero, E.; Chiesa, C. Low 25(OH)D3 levels are associated with total adiposity, metabolic syndrome, and hypertension in Caucasian children and adolescents. Eur. J. Endocrinol. 2011, 165, 603–611. [Google Scholar] [CrossRef]
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A.; et al. Vitamin D Insufficiency in Overweight and Obese Children and Adolescents. Front. Endocrinol. 2019, 10, 103. [Google Scholar] [CrossRef]
- Huang, Y.F.; Tok, T.S.; Lu, C.L.; Ko, H.C.; Chen, M.Y.; Chen, S.C.C. Relationship Between being Overweight and Iron Deficiency in Adolescents. Pediatr. Neonatol. 2015, 56, 386–392. [Google Scholar] [CrossRef]
- Ghadimi, R.; Esmaili, H.; Kheirkhah, D.; Tamaddoni, A. Is Childhood Obesity Associated with Iron Deficiency Anemia? Casp. J. Pediatr. 2015, 1, 59–66. [Google Scholar] [CrossRef]
- Sal, E.; Yenicesu, I.; Celik, N.; Pasaoglu, H.; Celik, B.; Pasaoglu, O.T.; Kaya, Z.; Kocak, U.; Camurdan, O.; Bideci, A.; et al. Relationship between obesity and iron deficiency anemia: Is there a role of hepcidin? Hematology 2018, 23, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Cepeda-Lopez, A.C.; Aeberli, I.; Zimmermann, M.B. Does obesity increase risk for iron deficiency? A review of the literature and the potential mechanisms. Int. J. Vitam. Nutr. Res. 2010, 80, 263–270. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, X.; Shen, Y.; Fang, X.; Wang, Y.; Wang, F. Obesity and iron deficiency: A quantitative meta-analysis. Obes. Rev. 2015, 16, 1081–1093. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overweight, n (%) | Obesity, n (%) | Severe Obesity, n (%) | p Value | |
|---|---|---|---|---|
| Sex | p = 0.178 | |||
| Male | 10 (34.5%) | 14 (48.3%) | 5 (17.2%) | |
| Female | 16 (40%) | 15 (37.5%) | 9 (22.5%) | |
| Age group | p = 0.178 | |||
| 2–5 years old | 4 (44.4%) | 3 (33.3%) | 2 (22.2%) | |
| 6–9 years old | 3 (27.3%) | 6 (54.5%) | 2 (18.2%) | |
| 10–13 years old | 11 (47.8%) | 11 (47.8%) | 1 (4.3%) | |
| 14–18 years old | 8 (30.8%) | 9 (34.6%) | 9 (34.6%) | |
| Residence | p = 0.065 | |||
| Rural | 5 (21.7%) | 14 (60.9%) | 4 (17.4%) | |
| Urban | 21 (45.7%) | 15 (32.6%) | 10 (21.7%) |
| Overweight, n = 26 | Obesity, n = 29 | Severe Obesity, n = 14 | p Value | |
|---|---|---|---|---|
| Age | 11.04 ± 4.09 | 11.24 ± 3.55 | 12.07 ± 5.06 | p = 0.740 |
| BMI | 22.70 ± 2.97 | 27.02 ± 3.36 | 35.84 ± 7.22 | |
| Hemoglobin (g/dL) | 12.76 ± 1.55 | 13.30 ± 1.71 | 13.42 ± 1.35 | p = 0.273 |
| MCH (pg) | 27.56 ± 3.18 | 27.39 ± 2.09 | 25.96 ± 2.62 | p = 0.167 |
| MCV (fL) | 79.84 ± 5.66 | 80.38 ± 5.44 | 78.53 ± 6.43 | p = 0.613 |
| Serum iron level (mcg/dL) | 70.58 ± 48.03 | 65.69 ± 29.08 | 56.71 ± 19.90 | p = 0.517 |
| Vitamin D (ng/mL) | 28.40 ± 11.59 | 26.40 ± 8.62 | 24.80 ± 12.68 | p = 0.575 |
| Calcium level | 9.79 ± 0.42 | 10.04 ± 0.33 | 10.04 ± 0.39 | p = 0.092 |
| Phosphorus | 4.64 ± 0.83 | 5.42 ± 1.68 | 5.43 ± 1.00 | p = 0.379 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlad, R.M.; Istrate-Grigore, O.-A.; Pacurar, D. Customizing Nutrients: Vitamin D and Iron Deficiencies in Overweight and Obese Children—Insights from a Romanian Study. Nutrients 2025, 17, 1193. https://doi.org/10.3390/nu17071193
Vlad RM, Istrate-Grigore O-A, Pacurar D. Customizing Nutrients: Vitamin D and Iron Deficiencies in Overweight and Obese Children—Insights from a Romanian Study. Nutrients. 2025; 17(7):1193. https://doi.org/10.3390/nu17071193
Chicago/Turabian StyleVlad, Raluca Maria, Oana-Andreea Istrate-Grigore, and Daniela Pacurar. 2025. "Customizing Nutrients: Vitamin D and Iron Deficiencies in Overweight and Obese Children—Insights from a Romanian Study" Nutrients 17, no. 7: 1193. https://doi.org/10.3390/nu17071193
APA StyleVlad, R. M., Istrate-Grigore, O.-A., & Pacurar, D. (2025). Customizing Nutrients: Vitamin D and Iron Deficiencies in Overweight and Obese Children—Insights from a Romanian Study. Nutrients, 17(7), 1193. https://doi.org/10.3390/nu17071193