
The Impact of Education Sources on Patient Compliance with the Recommended Oral Nutritional Supplement (ONS) Intake: A Qualitative Survey
 , , , and
, , , and
Abstract
1. Introduction
- -
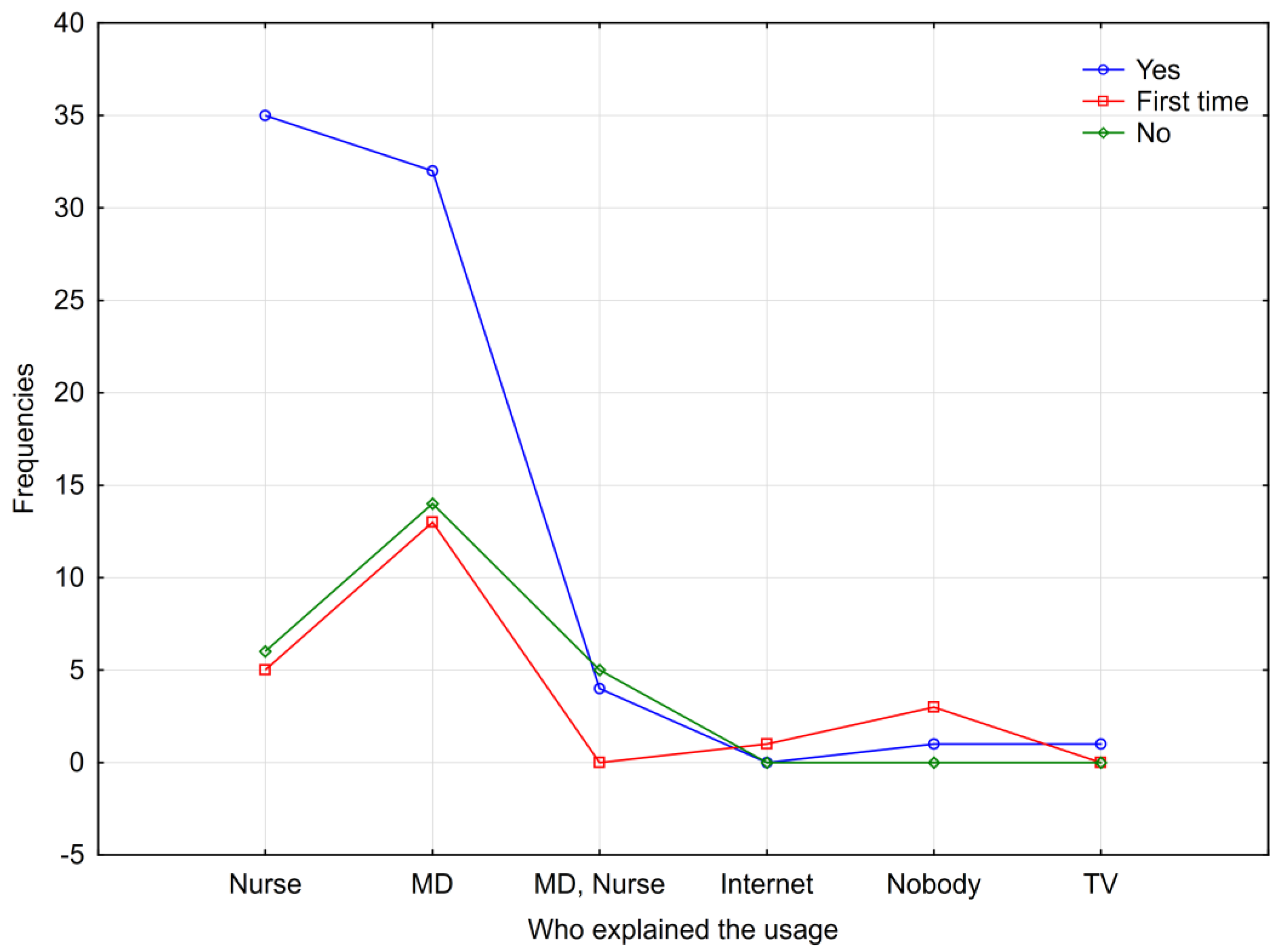
- The source of information on how to consume ONSs (nurse, medical doctor (MD), nurse and MD, and other sources: Internet, nobody, TV)
- -
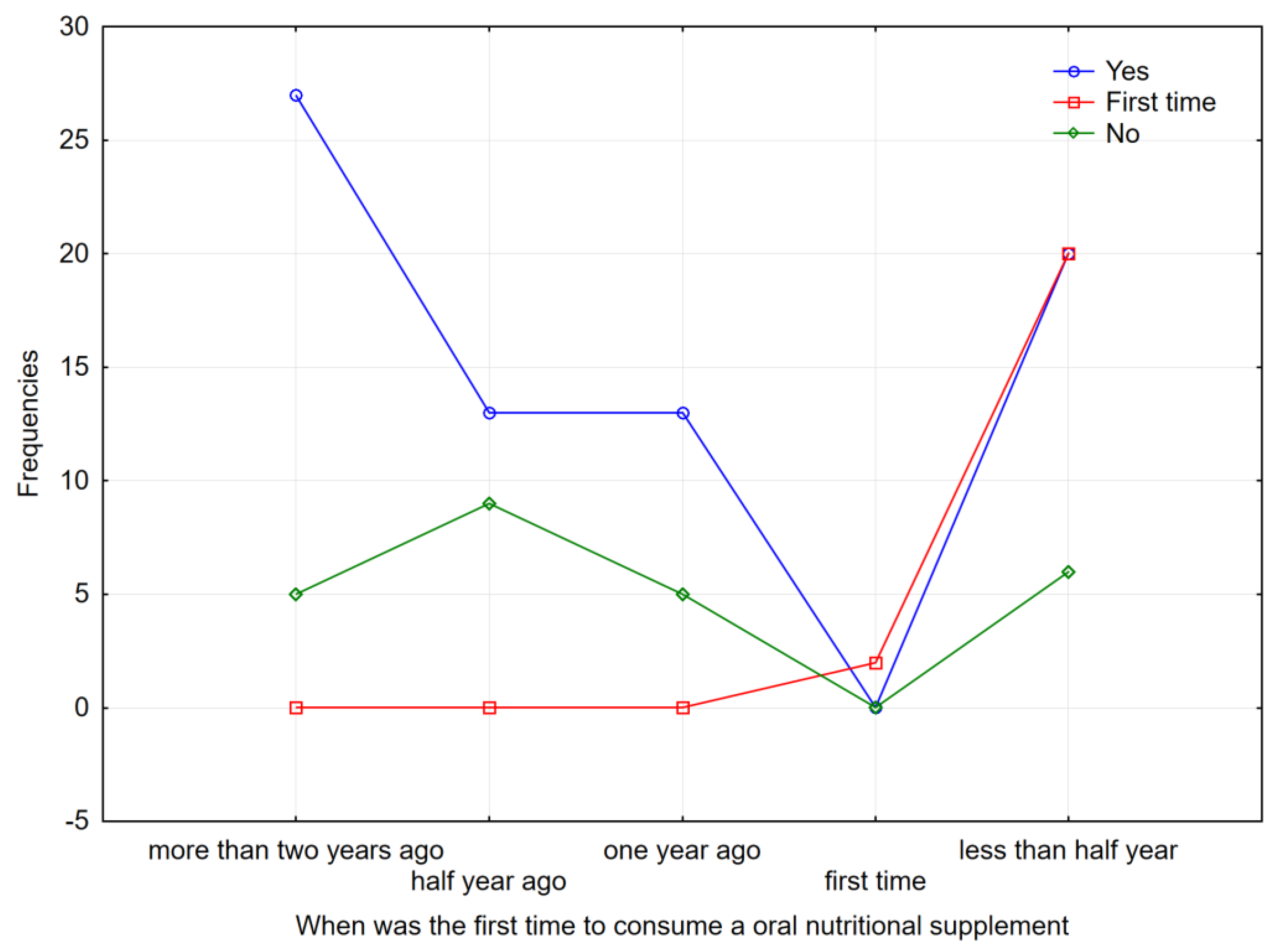
- The time of the first ONS consumption (more than two years ago, half a year ago, one year ago, for the first time, less than half a year ago)
2. Materials and Methods
2.1. Design and Participants
2.2. Research Procedure
2.3. Statistical Processing
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Daher, G.S.; Choi, K.Y.; Wells, J.W.; Goyal, N. A Systematic Review of Oral Nutritional Supplement and Wound Healing. Ann. Otol. Rhinol. Laryngol. 2022, 131, 1358–1368. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Altamirano, K.; Bejarano-Rosales, M.P.; González-Rodríguez, B.K.; Mondragón-Nieto, G.; Alatriste-Ortiz, G.; Noguez, L.J.J.; Gutiérrez-Salmeán, G.; Fuchs-Tarlovsky, V. Prevalence of Nutritional Risk and Malnutrition in Hospitalized Patients: A Retrospective, Cross-Sectional Study of Single-Day Screening. Appl. Physiol. Nutr. Metab. 2024, 49, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Starace, E.; De Pasquale, G.; Morenghi, E.; Crippa, C.; Matteucci, S.; Pieri, G.; Soekeland, F.; Gibbi, S.M.; Lo Cricchio, G.; Reggiani, F.; et al. Hospital Malnutrition in the Medicine and Neurology Departments: A Complex Challenge. Nutrients 2023, 15, 5061. [Google Scholar] [CrossRef]
- Uršulin-Trstenjak, N.; Dodlek Šarkanj, I.; Sajko, M.; Vitez, D.; Živoder, I. Determination of the Personal Nutritional Status of Elderly Populations Based on Basic Foodomics Elements. Foods 2021, 10, 2391. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, C.; de van der Schueren, M.A.E.; Kruizenga, H.M.; Weekes, C.E. Dietary Advice with or without Oral Nutritional Supplements for Disease-Related Malnutrition in Adults. Cochrane Database Syst. Rev. 2021, 12, 1465–1858. [Google Scholar] [CrossRef]
- Cass, A.R.; Charlton, K.E. Prevalence of Hospital-Acquired Malnutrition and Modifiable Determinants of Nutritional Deterioration during Inpatient Admissions: A Systematic Review of the Evidence. J. Hum. Nutr. Diet. 2022, 35, 1043–1058. [Google Scholar] [CrossRef]
- BAPEN. Oral Nutritional Supplements (ONS). Available online: https://www.bapen.org.uk/education/nutrition-support/nutrition-by-mouth/oral-nutritional-supplements-ons/ (accessed on 24 February 2025).
- IJpma, I.; Renken, R.J.; Ter Horst, G.J.; Reyners, A.K.L. The Palatability of Oral Nutritional Supplements: Before, during, and after Chemotherapy. Support. Care Cancer 2016, 24, 4301–4308. [Google Scholar] [CrossRef]
- Ravasco, P. Aspects of Taste and Compliance in Patients with Cancer. Eur. J. Oncol. Nurs. 2005, 9 (Suppl. 2), S84–S91. [Google Scholar] [CrossRef]
- Hyrkas, K.; Wiggins, M. A Comparison of Usual Care, a Patient-Centred Education Intervention and Motivational Interviewing to Improve Medication Adherence and Readmissions of Adults in an Acute-Care Setting. J. Nurs. Manag. 2014, 22, 350–361. [Google Scholar] [CrossRef]
- Cutilli, C.C. Excellence in Patient Education: Evidence-Based Education That “Sticks” and Improves Patient Outcomes. Nurs. Clin. N. Am. 2020, 55, 267–282. [Google Scholar] [CrossRef]
- Leonard, K. Essentials of Patient Education, by Susan B. Bastable. J. Consum. Health Internet 2017, 21, 319–320. [Google Scholar] [CrossRef]
- Parnell, T.A. Health Literacy in Nursing; Springer Publishing Company: New York, NY, USA, 2015. [Google Scholar]
- Fereidouni, Z.; Sabet Sarvestani, R.; Hariri, G.; Kuhpaye, S.A.; Amirkhani, M.; Najafi Kalyani, M. Moving Into Action: The Master Key to Patient Education. J. Nurs. Res. 2019, 27, e6. [Google Scholar] [CrossRef]
- Aghakhani, N.; Nia, H.S.; Ranjbar, H.; Rahbar, N.; Beheshti, Z. Nurses’ Attitude to Patient Education Barriers in Educational Hospitals of Urmia University of Medical Sciences. Iran. J. Nurs. Midwifery Res. 2012, 17, 12. [Google Scholar]
- Pouresmail, Z.; Heshmati Nabavi, F.; Zare, N.V. Outcomes of Patient Education in Nurse-Led Clinics: A Systematic Review. J. Caring Sci. 2023, 12, 188–200. [Google Scholar] [CrossRef]
- Masamha, R.; Alfred, L.; Harris, R.; Bassett, S.; Burden, S.; Gilmore, A. “Barriers to Overcoming the Barriers”: A Scoping Review Exploring 30 Years of Clinical Supervision Literature. J. Adv. Nurs. 2022, 78, 2678–2692. [Google Scholar] [CrossRef] [PubMed]
- Driever, E.M.; Brand, P.L.P. Education Makes People Take Their Medication: Myth or Maxim? Breathe 2020, 16, 190338. [Google Scholar] [CrossRef] [PubMed]
- Magill, M.; Gaume, J.; Apodaca, T.R.; Walthers, J.; Mastroleo, N.R.; Borsari, B.; Longabaugh, R. The Technical Hypothesis of Motivational Interviewing: A Meta-Analysis of MI’s Key Causal Model. J. Consult. Clin. Psychol. 2014, 82, 973. [Google Scholar] [CrossRef]
- Desselle, S.P. Construction, Implementation, and Analysis of Summated Rating Attitude Scales. Am. J. Pharm. Educ. 2005, 69, 97. [Google Scholar] [CrossRef]
- Draugalis, J.L.R.; Coons, S.J.; Plaza, C.M. Best Practices for Survey Research Reports: A Synopsis for Authors and Reviewers. Am. J. Pharm. Educ. 2008, 72, 11. [Google Scholar] [CrossRef]
- WHO. Model Lists of Essential Medicines. Available online: https://www.who.int/groups/expert-committee-on-selection-and-use-of-essential-medicines/essential-medicines-lists (accessed on 24 February 2025).
- Brown, M.T.; Bussell, J.K. Medication Adherence: WHO Cares? Mayo Clin. Proc. 2011, 86, 304–314. [Google Scholar] [CrossRef]
- Robin Dimatteo, M.; Giordani, P.J.; Lepper, H.S.; Croghan, T.W. Patient Adherence and Medical Treatment Outcomes: A Meta-Analysis. Med. Care 2002, 40, 794–811. [Google Scholar] [CrossRef] [PubMed]
- Somanchi, M.; Tao, X.; Mullin, G.E. The Facilitated Early Enteral and Dietary Management Effectiveness Trial in Hospitalized Patients with Malnutrition. JPEN. J. Parenter. Enteral Nutr. 2011, 35, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Lawson, R.M.; Doshi, M.K.; Barton, J.R.; Cobden, I. The Effect of Unselected Post-Operative Nutritional Supplementation on Nutritional Status and Clinical Outcome of Orthopaedic Patients. Clin. Nutr. 2003, 22, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Beattie, A.H.; Prach, A.T.; Baxter, J.P.; Pennington, C.R. A Randomised Controlled Trial Evaluating the Use of Enteral Nutritional Supplements Postoperatively in Malnourished Surgical Patients. Gut 2000, 46, 813–818. [Google Scholar] [CrossRef]
- Gariballa, S.; Forster, S. Effects of Dietary Supplements on Depressive Symptoms in Older Patients: A Randomised Double-Blind Placebo-Controlled Trial. Clin. Nutr. 2007, 26, 545–551. [Google Scholar] [CrossRef]
- Norman, K.; Kirchner, H.; Freudenreich, M.; Ockenga, J.; Lochs, H.; Pirlich, M. Three Month Intervention with Protein and Energy Rich Supplements Improve Muscle Function and Quality of Life in Malnourished Patients with Non-Neoplastic Gastrointestinal Disease—A Randomized Controlled Trial. Clin. Nutr. 2008, 27, 48–56. [Google Scholar] [CrossRef]
- Deutz, N.E.; Matheson, E.M.; Matarese, L.E.; Luo, M.; Baggs, G.E.; Nelson, J.L.; Hegazi, R.A.; Tappenden, K.A.; Ziegler, T.R. Readmission and Mortality in Malnourished, Older, Hospitalized Adults Treated with a Specialized Oral Nutritional Supplement: A Randomized Clinical Trial. Clin. Nutr. 2016, 35, 18–26. [Google Scholar] [CrossRef]
- Jensen, M.B.; Hessov, I. Dietary Supplementation at Home Improves the Regain of Lean Body Mass after Surgery. Nutrition 1997, 13, 422–430. [Google Scholar] [CrossRef]
- Regulation (EU) No 609/2013 of the European Parliament and of the Council of 12 June 2013 Regulation—609/2013—EN—EUR-Lex. Available online: https://eur-lex.europa.eu/eli/reg/2013/609/oj/eng (accessed on 24 February 2025).
- National Institute for Health and Care Excellence Nutrition Support for Adults: Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition. Available online: https://www.nice.org.uk/guidance/cg32 (accessed on 24 February 2025).
- Hegney, D.; Plank, A.; Watson, J.; Raith, L.; McKeon, C. Patient Education and Consumer Medicine Information: A Study of Provision by Queensland Rural and Remote Area Registered Nurses. J. Clin. Nurs. 2005, 14, 855–862. [Google Scholar] [CrossRef]
- Rees, S.; Williams, A. Promoting and Supporting Self-Management for Adults Living in the Community with Physical Chronic Illness: A Systematic Review of the Effectiveness and Meaningfulness of the Patient-Practitioner Encounter. JBI Libr. Syst. Rev. 2009, 7, 492–582. [Google Scholar] [CrossRef]
- Bowen, J.F.; Rotz, M.E.; Patterson, B.J.; Sen, S. Nurses’ Attitudes and Behaviors on Patient Medication Education. Pharm. Pract. 2017, 15(2), 930. [Google Scholar] [CrossRef] [PubMed]
- Chugh, A.; Williams, M.V.; Grigsby, J.; Coleman, E.A. Better Transitions: Improving Comprehension of Discharge Instructions. Front. Health Serv. Manag. 2009, 25, 11–32. [Google Scholar] [CrossRef]
- Koelling, T.M.; Johnson, M.L.; Cody, R.J.; Aaronson, K.D. Discharge Education Improves Clinical Outcomes in Patients with Chronic Heart Failure. Circulation 2005, 111, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Kendall, S.; Deacon-Crouch, M.; Raymond, K. Nurses’ Attitudes toward Their Role in Patient Discharge Medication Education and toward Collaboration with Hospital Pharmacists: A Staff Development Issue. J. Nurses Staff Dev. 2007, 23, 173–179. [Google Scholar] [CrossRef]
- Auyeung, V.; Patel, G.; McRobbie, D.; Weinman, J.; Davies, G. Information about Medicines to Cardiac In-Patients: Patient Satisfaction alongside the Role Perceptions and Practices of Doctors, Nurses and Pharmacists. Patient Educ. Couns. 2011, 83, 360–366. [Google Scholar] [CrossRef]
- WHO. Global Patient Safety Action Plan 2021–2030. Available online: https://www.who.int/teams/integrated-health-services/patient-safety/policy/global-patient-safety-action-plan (accessed on 24 February 2025).
- Thakore, S. Training Clinicians to Become Leaders of Complex Change: Lessons from Scotland. Pediatr. Anesth. 2022, 32, 1216–1222. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| S O U R C E | |||||||
|---|---|---|---|---|---|---|---|
| Do You Comply with the Recommended Intake Dose? | Nurse | MD | MD; Nurse | Internet | Nobody | TV | Row Totals |
| YES, at home | 35 | 32 | 4 | 0 | 1 | 1 | 73 |
| Column Percent | 76.09% | 54.24% | 44.44% | 0.00% | 25.00% | 100.00% | |
| Row Percent | 47.95% | 43.84% | 5.48% | 0.00% | 1.37% | 1.37% | ∑ = 100% |
| Total Percent | 29.17% | 26.67% | 3.33% | 0.00% | 0.83% | 0.83% | 60.83% |
| Now, for the first time in hospital | 5 | 13 | 0 | 1 | 3 | 0 | 22 |
| Column Percent | 10.87% | 22.03% | 0.00% | 100.00% | 75.00% | 0.00% | |
| Row Percent | 22.73% | 59.09% | 0.00% | 4.55% | 13.64% | 0.00% | ∑ = 100% |
| Total Percent | 4.17% | 10.83% | 0.00% | 0.83% | 2.50% | 0.00% | 18.33% |
| NO, at home | 6 | 14 | 5 | 0 | 0 | 0 | 25 |
| Column Percent | 13.04% | 23.73% | 55.56% | 0.00% | 0.00% | 0.00% | |
| Row Percent | 24.00% | 56.00% | 20.00% | 0.00% | 0.00% | 0.00% | ∑ = 100% |
| Total Percent | 5.00% | 11.67% | 4.17% | 0.00% | 0.00% | 0.00% | 20.83% |
| All Groups (∑ = 100%) | 46 | 59 | 9 | 1 | 4 | 1 | 120 |
| Total Percentage | 38.33% | 49.17% | 7.50% | 0.83% | 3.33% | 0.83% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uršulin-Trstenjak, N.; Poljak, D.; Šarkanj, B.; Sajko, M.; Šarkanj, I.D. The Impact of Education Sources on Patient Compliance with the Recommended Oral Nutritional Supplement (ONS) Intake: A Qualitative Survey. Nutrients 2025, 17, 889. https://doi.org/10.3390/nu17050889
Uršulin-Trstenjak N, Poljak D, Šarkanj B, Sajko M, Šarkanj ID. The Impact of Education Sources on Patient Compliance with the Recommended Oral Nutritional Supplement (ONS) Intake: A Qualitative Survey. Nutrients. 2025; 17(5):889. https://doi.org/10.3390/nu17050889
Chicago/Turabian StyleUršulin-Trstenjak, Natalija, Damir Poljak, Bojan Šarkanj, Melita Sajko, and Ivana Dodlek Šarkanj. 2025. "The Impact of Education Sources on Patient Compliance with the Recommended Oral Nutritional Supplement (ONS) Intake: A Qualitative Survey" Nutrients 17, no. 5: 889. https://doi.org/10.3390/nu17050889
APA StyleUršulin-Trstenjak, N., Poljak, D., Šarkanj, B., Sajko, M., & Šarkanj, I. D. (2025). The Impact of Education Sources on Patient Compliance with the Recommended Oral Nutritional Supplement (ONS) Intake: A Qualitative Survey. Nutrients, 17(5), 889. https://doi.org/10.3390/nu17050889