
Do Obesity and Adipose Tissue Cytokines Influence the Response to Janus Kinase Inhibitors in Rheumatoid Arthritis?

 , ,
, ,  , , ,
, , ,
Abstract
1. Background
2. Methods
2.1. Data Collection
2.2. Assessment of Clinical Disease Activity and Response to Treatment
2.3. Measurement of Serum Adipokines
3. Results
3.1. Baseline Clinical and Sociodemographic Characteristics
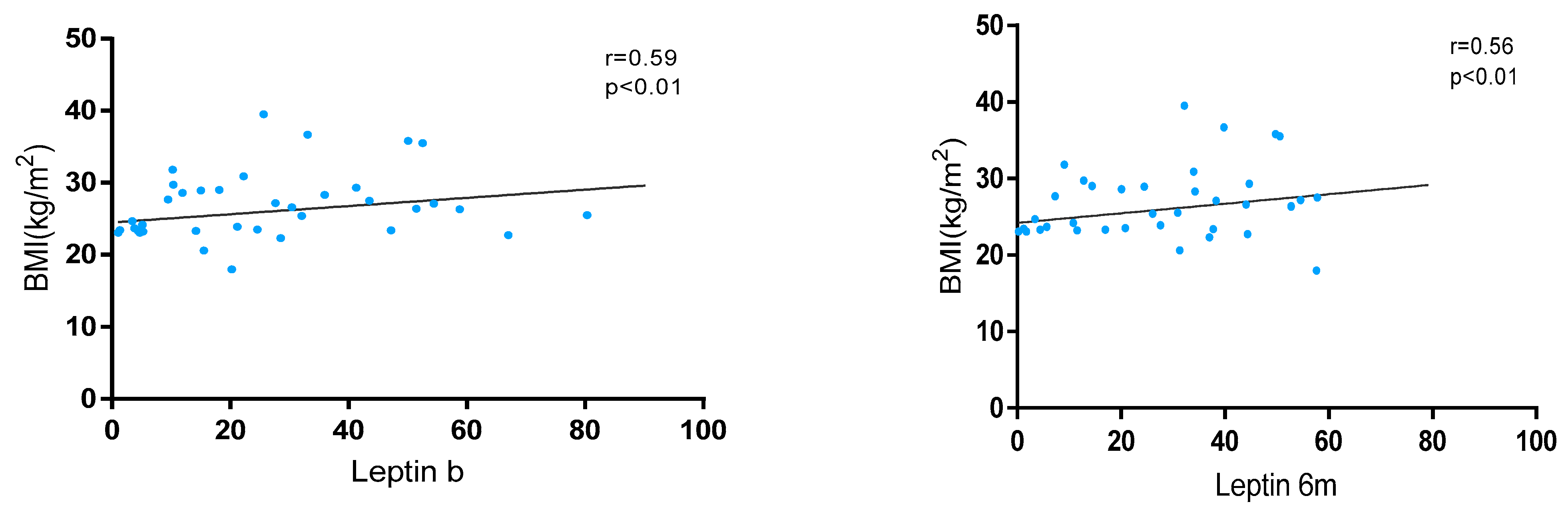
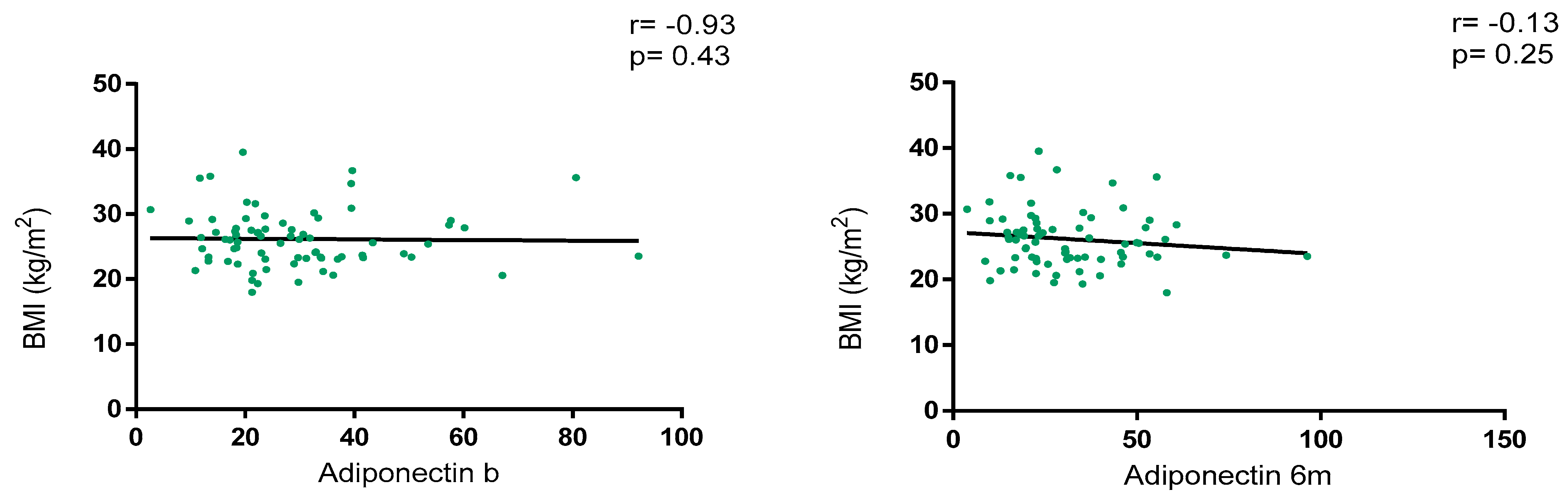
3.2. Association Between BMI and Serum Adipokines
3.3. Association Between BMI and Disease Activity
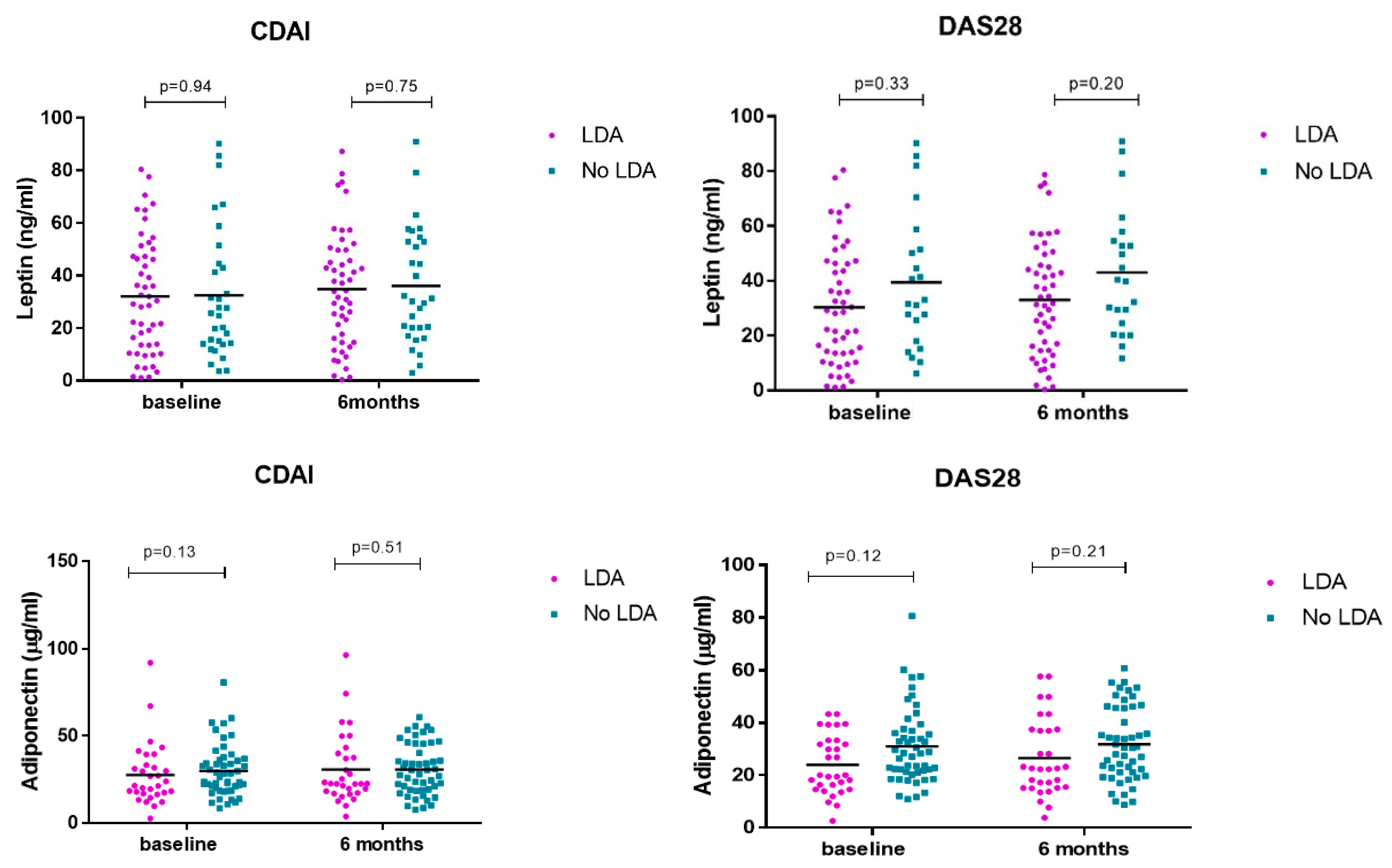
3.4. Association Serum Adipokines and Treatment Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Gremese, E.; Tolusso, B.; Gigante, M.R.; Ferraccioli, C. Obesity as a risk and severity factor in rheumatic diseases (autoimmune chronic inflammatory diseases). Front. Immunol. 2014, 5, 576. [Google Scholar] [CrossRef] [PubMed]
- Cildir, G.; Akıncılar, S.C.; Tergaonkar, V. Chronic adipose tissue inflammation: All immune cells on the stage. Trends Mol. Med. 2013, 19, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Hauner, H. Secretory factors from human adipose tissue and their functional role. Proc. Nutr. Soc. 2005, 64, 163–169. [Google Scholar] [CrossRef]
- Maximus, P.S.; Al Achkar, Z.; Hamid, P.F.; Hasnain, S.S.; Peralta, C.A. Adipocytokines: Are they the theory of everything? Cytokine 2020, 133, 155144. [Google Scholar] [CrossRef] [PubMed]
- Francisco, V.; Pino, J.; Gonzalez-Gay, M.A.; Mera, A.; Lago, F.; Gómez, R.; Mobasheri, A.; Gualillo, O. Adipokines and inflammation: Is it a question of weight? Br. J. Pharmacol. 2018, 175, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Francisco, V.; Pino, J.; Campos-Cabaleiro, V.; Ruiz-Fernandez, C.; Mera, A.; Gonzalez-Gay, M.A.; Gómez, R.; Gualillo, O. Obesity, fat mass and immune system: Role for leptin. Front. Physiol. 2018, 9, 640. [Google Scholar] [CrossRef]
- Fatel, E.C.S.; Rosa, F.T.; Simão, A.N.C.; Dichi, I. Adipokines in rheumatoid arthritis. Adv. Rheumatol. 2018, 58, 25. [Google Scholar] [CrossRef] [PubMed]
- Del Prete, A.; Salvi, V.; Sozzani, S. Adipokines as potential biomarkers in rheumatoid arthritis. Mediat. Inflamm. 2014, 2014, 425068. [Google Scholar] [CrossRef]
- Poudel, D.; George, M.D.; Baker, J.F. The Impact of Obesity on Disease Activity and Treatment Response in Rheumatoid Arthritis. Curr. Rheumatol. Rep. 2020, 22, 56. [Google Scholar] [CrossRef]
- Baker, J.F.; Reed, G.; Poudel, D.R.; Harrold, L.R.; Kremer, J.R. Obesity and Response to Advanced Therapies in Rheumatoid Arthritis. Arthritis Care Res. 2022, 74, 1909–1916. [Google Scholar] [CrossRef] [PubMed]
- Gialouri, C.G.; Pappa, M.; Evangelatos, G.; Nikiphorou, E.; Fragoulis, G.E. Effect of body mass index on treatment response of biologic/targeted-synthetic DMARDs in patients with rheumatoid arthritis, psoriatic arthritis or axial spondyloarthritis. A systematic review. Autoimmun. Rev. 2023, 22, 103357. [Google Scholar] [CrossRef]
- Dey, M.; Zhao, S.S.; Moots, R.J.; Bergstra, S.A.; Landewe, R.B.; Goodson, N.J. The association between increased body mass index and response to conventional synthetic disease-modifying anti-rheumatic drug treatment in rheumatoid arthritis: Results from the METEOR database. Rheumatology 2022, 61, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos-Kalinoglou, A.; Metsios, G.S.; Koutedakis, Y.; Kitas, G.D. Obesity in rheumatoid arthritis. Rheumatology 2011, 50, 450–462. [Google Scholar] [CrossRef] [PubMed]
- Braga, G.C.; Simões, J.L.B.; Teixeira Dos Santos, Y.J.; Menta-Filho, J.C.; Dulce Bagatini, M. The impacts of obesity in rheumatoid arthritis and insights into therapeutic purinergic modulation. Int. Immunopharmacol. 2024, 136, 112357. [Google Scholar] [CrossRef]
- Lupoli, R.; Pizzicato, P.; Scalera, A.; Ambrosino, P.; Amato, M.; Peluso, R.; Di Minno, M.N.D. Impact of body weight on the achievement of minimal disease activity in patients with rheumatic diseases: A systematic review and meta-analysis. Arthritis Res. Ther. 2016, 18, 297. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gremese, E.; Carletto, A.; Padovan, M.; Azteni, F.; Raffeiner, B.; Giardina, A.R.; Favalli, E.G.; Erre, G.L.; Gorla, R.; Galeazzi, M.; et al. Gruppo Italiano di Studio sulle Early Arthritis (GISEA). Obesity and reduction of the response rate to anti-tumor necrosis factor α in rheumatoid arthritis: An approach to a personalized medicine. Arthritis Care Res. 2013, 65, 94–100. [Google Scholar] [CrossRef]
- Klaasen, R.; Wijbrandts, C.A.; Gerlag, D.M.; Tak, P.P. Body mass index and clinical response to infliximab in rheumatoid arthritis. Arthritis Rheum. 2011, 63, 359–364. [Google Scholar] [CrossRef]
- Novella-Navarro, M.; Genre, F.; Hernández-Breijo, B.; Remuzgo-Martínez, S.; Martínez-Feito, A.; Peiteado, D.; Monjo, I.; Gonzalez-Gay, M.A.; Plasencia-Rodríguez, C.H.; Balsa, A. Obesity and response to biological therapy in rheumatoid arthritis: The role of body mass index and adipose tissue cytokines. Clin. Exp. Rheumatol. 2022, 40, 1726–1732. [Google Scholar] [CrossRef] [PubMed]
- Novella-Navarro, M.; Genre, F.; Martínez-Feito, A.; Pulito-Cueto, V.; Plasencia-Rodríguez, C.H.; Balsa, A. Obesity and adipose tissue cytokines in rheumatoid arthritis treated with IL-6 inhibitors: Does the route of administration matter? Clin. Exp. Rheumatol. 2023, 41, 1563–1564. [Google Scholar] [CrossRef] [PubMed]
- Gardette, A.; Ottaviani, S.; Sellam, J.; Berenbaum, F.; Lioté, F.; Meyer, A.; Sibilia, J.; Fautrel, B.; Palazzo, E.; Dieudé, P. Body mass index and response to tocilizumab in rheumatoid arthritis: A real life study. Clin. Rheumatol. 2016, 35, 857–861. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, M.A.; Alten, R.; Mysler, E.; Le Bars, M.; Ye, J.; Murthy, B.; Heitzman, J.; Vadanici, R.; Ferracioli, G. Body mass index and clinical response to intravenous or subcutaneous abatacept in patients with rheumatoid arthritis. Clin. Rheumatol. 2017, 36, 2655–2665. [Google Scholar] [CrossRef]
- Ottaviani, S.; Gardette, A.; Roy, C.; Tubach, F.; Gill, G.; Palazzo, E.; Meyer, O.; Dieudé, P. Body Mass Index and response to rituximab in rheumatoid arthritis. Jt. Bone Spine 2015, 82, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Kremer, J.M.; Schiff, M.; Muram, D.; Zhong, J.; Alam, J.; Genovese, M.C. Response to baricitinib therapy in patients with rheumatoid arthritis with inadequate response to csDMARDs as a function of baseline characteristics. RMD Open 2018, 4, e000581. [Google Scholar] [CrossRef]
- Weinblatt, M.; Mysler, E.; Ostor, A.; Broadwell, A.; Jeka, S.; Dunlap, K.; Suboticki, J.; Enejosa, J.; Hendrickson, B.; Zhong, S. Fri0140 Impact of Baseline Demographics and Disease Activity on Outcomes in Patients with Rheumatoid Arthritis Receiving Upadacitinib. Ann. Rheum. Dis. 2020, 79, 653–654. [Google Scholar] [CrossRef]
- Dikranian, A.H.; Gonzalez-Gay, M.A.; Wellborne, F.; Alvaro-Gracia, J.M.; Takiya, L.; Stockert, L.; Paulissen, J.; Shi, H.; Tatulych, S.; Curtis, J.R. Efficacy of tofacitinib in patients with rheumatoid arthritis stratified by baseline body mass index: An analysis of pooled data from phase 3 studies. RMD Open 2022, 8, e002103. [Google Scholar] [CrossRef]
- Balsa, A.; Wassenberg, S.; Tanaka, Y.; Tournadre, A.; Orzechowski, H.D.; Rajendran, V.; Lendi, U.; Stiers, P.J.; Watson, C.; Caporali, R.; et al. Effect of Filgotinib on Body Mass Index (BMI) and Effect of Baseline BMI on the Efficacy and Safety of Filgotinib in Rheumatoid Arthritis. Rheumatol. Ther. 2023, 10, 1555–1574. [Google Scholar] [CrossRef]
- Corrado, A.; Colia, R.; Rotondo, C.; Sanpaolo, E.; Cantatore, F.P. Changes in serum adipokines profile and insulin resistance in patients with rheumatoid arthritis treated with anti-TNF-α. Curr. Med. Res. Opin. 2019, 35, 2197–2205. [Google Scholar] [CrossRef]
- Gonzalez-Gay, M.A.; Garcia-Unzueta, M.T.; Berja, A.; Gonzalez-Juanatey, C.; Miranda-Filloy, J.A.; Vazquez-Rodriguez, T.R.; De Matias, M.J.; Martin, J.; Dessein, P.H.; Llorca, J. Anti-TNF-alpha therapy does not modulate leptin in patients with severe rheumatoid arthritis. Clin. Exp. Rheumatol. 2009, 27, 222–228. [Google Scholar]
- Pulito-Cueto, V.; Remuzgo-Martínez, S.; Genre, F.; Calvo-Alen, J.; Aurrecoechea, E.; Llorente, I.; Triguero-Martinez, A.; Blanco, R.; Llorca, J.; Ruiz-Lucea, E.; et al. Anti-IL-6 therapy reduces leptin serum levels in patients with rheumatoid arthritis. Clin. Exp. Rheumatol. 2020, 38, 1201–1205. [Google Scholar] [PubMed]
- Hoffman, E.; Rahat, M.A.; Feld, J.; Elias, M.; Rosner, I.; Kaly, S.; Lavie, I.; Gazitt, T.; Zisman, D. Effects of Tocilizumab, an Anti-Interleukin-6 Receptor Antibody, on Serum Lipid and Adipokine Levels in Patients with Rheumatoid Arthritis. Int. J. Mol. Sci. 2019, 20, 4633. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; He, C. Pro-inflammatory cytokines: The link between obesity and osteoarthritis. Cytokine Growth Factor Rev. 2018, 44, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Frühbeck, G. Intracellular signalling pathways activated by leptin. Biochem. J. 2006, 393 Pt 1, 7–20. [Google Scholar] [CrossRef]
- Ghantous, C.M.; Azrak, A.; Hanache, S.; Abou-Kheir, W.; Zeidan, A. Differential Role of Leptin and Adiponectin in Cardiovascular System. Int. J. Endocrinol. 2015, 2015, 534320. [Google Scholar] [CrossRef] [PubMed]
- Dodington, D.W.; Desai, H.R.; Woo, M. JAK/STAT—Emerging Players in Metabolism. Trends Endocrinol. Metab. 2018, 29, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Pulito-Cueto, V.; Remuzgo-Martínez, S.; Genre, F.; Calvo-Alen, J.; Aurrecoechea, E.; Llorente, I.; Triguero-Martinez, A.; Blanco, R.; Llorca, J.; Ruiz-Lucea, E.; et al. Role of adiponectin in non-diabetic patients with rheumatoid arthritis undergoing anti-IL-6 therapy. Clin. Exp. Rheumatol. 2022, 40, 988–992. [Google Scholar] [CrossRef]
- Fioravanti, A.; Tenti, S.; Bacarelli, M.R.; Damiani, A.; Li Gobbi, F.; Bandinelli, F.; Cheleschi, S.; Galeazzi, M.; Benucci, M. Tocilizumab modulates serum levels of adiponectin and chemerin in patients with rheumatoid arthritis: Potential cardiovascular protective role of IL-6 inhibition. Clin. Exp. Rheumatol. 2019, 37, 293–300. [Google Scholar] [PubMed]
- Virone, A.; Bastard, J.P.; Fellahi, S.; Capeau, J.; Rouanet, S.; Sibilia, J.; Ravaud, P.; Berenbaum, F.; Gottenberg, J.E.; Sellam, J. Comparative effect of tumour necrosis factor inhibitors versus other biological agents on cardiovascular risk-associated biomarkers in patients with rheumatoid arthritis. RMD Open 2019, 5, e000897. [Google Scholar] [CrossRef]
- Baker, J.F.; Odell, J.R.; England, B.R.; Giles, J.T.; Newcomb, J.A.; George, M.D.; Thiele, G.; Morelan, L.; Bridges, S.L.; Curtis, J.R.; et al. Lower body mass and lower adiposity are associated with differential responses to two treatment strategies for rheumatoid arthritis. Ann. Rheum. Dis. 2024, 83, 429–436. [Google Scholar] [CrossRef]
- Giardullo, L.; Corrado, A.; Maruotti, N.; Cici, D.; Mansueto, N.; Cantatore, F.P. Adipokine role in physiopathology of inflammatory and degenerative musculoskeletal diseases. Int. J. Immunopathol. Pharmacol. 2021, 35, 20587384211015034. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 81) | BMI ≥ 25 kg/m2 (n = 44) | BMI < 25 kg/m2 (n = 37) | p-Value |
|---|---|---|---|---|
| Age mean (SD) | 55.6 (11.6) | 59.3 (10.6) | 51.1 (11.1) | 0.01 |
| Sex (female) n (%) | 70 (86.4) | 36 (81.8) | 34 (91.9) | 0.16 |
| Disease duration (years) mean (SD) | 17.7 (10.2) | 19.7 (10.2) | 15.2 (9.7) | 0.04 |
| Smoking habit n (%) | 0.08 | |||
| Current | 19 (23.5) | 11 (25.0) | 8 (21.6) | |
| Past | 26 (32.1) | 18 (40.9) | 8 (21.6) | |
| Never | 34 (42.0) | 14 (31.8) | 20 (54.1) | |
| JAKi | 0.05 | |||
| Baricitinib | 37 (45.7) | 16 (36.4) | 21 (56.8) | |
| Filgotinib | 17 (21.0) | 8 (18.2) | 9 (24.3) | |
| Tofacitinib | 13 (16.0) | 11 (25.0) | 2 (5.4) | |
| Upadacitinib | 14 (17.3) | 9 (20.5) | 5 (13.5) | |
| JAKi monotherapy | 20 (24.7) | 10 (22.7) | 10 (27.0) | 0.42 |
| Use of concomitant methotrexate | 34 (42.0) | 18 (40.9) | 16 (43.2) | 0.50 |
| bDMARD naïve n (%) | 24 (29.6) | 13 (29.5) | 11 (29.7) | 0.58 |
| Number of previous bDMARDs | 1 (0–3) | 1 (0–3) | 1 (0–2.5) | 0.62 |
| RF-positive (UI/mL) n (%) | 70 (86.4) | 37 (84.1) | 33 (89.2) | 0.36 |
| ACPA-positive (UI/mL) n (%) | 65 (80.2) | 37 (84.1) | 28 (75.7) | 0.33 |
| CRP b (mg/L) median (IQR) | 3.5 (0.8–9.6) | 4.4 (0.9–9.8) | 2.9 (0.7–7.1) | 0.76 |
| DAS28 b mean (SD) | 4.3 (1.1) | 4.3 (1.0) | 4.3 (1.2) | 0.98 |
| CDAI b mean (SD) | 23.1 (11.1) | 22.9 (11.5) | 23.4 (10.7) | 0.84 |
| CRP 6 m (mg/L) | 1.1 (0.5–4.5) | 2.2 (0.5–6.0) | 0.8 (0.5–4.1) | 0.52 |
| DAS28 6 m mean (SD) | 2.8 (1.2) | 3.0 (1.1) | 2.9 (1.4) | 0.65 |
| CDAI 6 m mean (SD) | 11.1 (9.5) | 11.1 (8.8) | 11.1 (10.5) | 0.99 |
| LDA-DAS28 n (%) | 50 (61.7) | 26 (59.1) | 24 (64.9) | 0.32 |
| LDA-CDAI n (%) | 50 (61.7) | 29 (65.9) | 21 (56.8) | 0.26 |
| Adipokine Levels | CDAI | DAS28 | ||||
|---|---|---|---|---|---|---|
| LDA | No-LDA | p-Value | LDA | No-LDA | p-Value | |
| Leptin b (ng/mL) | 29.7 (12.6–47.9) | 25.6 (13.9–44.5) | 0.94 | 28.2 (12.6–46.5) | 27.6 (13.9–51.4) | 0.33 |
| Leptin 6 m (ng/mL) | 34.1 (15.6–49.6) | 31.2 (20.6–52.7) | 0.75 | 31.4 (14.4–46.6) | 39.7 (20.4–52.7) | 0.20 |
| Adiponectin b (μg/mL) | 27.4 (19.8–36.3) | 21.4 (16.8–33.3) | 0.19 | 28.4 (21.2–37.1) | 20.1 (13.9–31.8) | 0.12 |
| Adiponectin 6 m (μg/mL) | 29.2 (19.2–45.6) | 22.6 (17.3–39.9) | 0.51 | 29.1 (18.9–45.8) | 22.5 (15.5–37.5) | 0.31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novella-Navarro, M.; Van Den Rym, A.; López-Pedrera, C.; Martínez-Feito, A.; Nieto-Carvalhal, B.; Reche, K.; López-Medina, C.; Escudero-Contreras, A.; Nozal, P.; Miranda-Carús, M.E.; et al. Do Obesity and Adipose Tissue Cytokines Influence the Response to Janus Kinase Inhibitors in Rheumatoid Arthritis? Nutrients 2025, 17, 820. https://doi.org/10.3390/nu17050820
Novella-Navarro M, Van Den Rym A, López-Pedrera C, Martínez-Feito A, Nieto-Carvalhal B, Reche K, López-Medina C, Escudero-Contreras A, Nozal P, Miranda-Carús ME, et al. Do Obesity and Adipose Tissue Cytokines Influence the Response to Janus Kinase Inhibitors in Rheumatoid Arthritis? Nutrients. 2025; 17(5):820. https://doi.org/10.3390/nu17050820
Chicago/Turabian StyleNovella-Navarro, Marta, Ana Van Den Rym, Chary López-Pedrera, Ana Martínez-Feito, Beatriz Nieto-Carvalhal, Keren Reche, Clementina López-Medina, Alejandro Escudero-Contreras, Pilar Nozal, Maria Eugenia Miranda-Carús, and et al. 2025. "Do Obesity and Adipose Tissue Cytokines Influence the Response to Janus Kinase Inhibitors in Rheumatoid Arthritis?" Nutrients 17, no. 5: 820. https://doi.org/10.3390/nu17050820
APA StyleNovella-Navarro, M., Van Den Rym, A., López-Pedrera, C., Martínez-Feito, A., Nieto-Carvalhal, B., Reche, K., López-Medina, C., Escudero-Contreras, A., Nozal, P., Miranda-Carús, M. E., Monjo, I., De Miguel, E., Balsa, A., Pérez-De Diego, R., & Plasencia-Rodríguez, C. (2025). Do Obesity and Adipose Tissue Cytokines Influence the Response to Janus Kinase Inhibitors in Rheumatoid Arthritis? Nutrients, 17(5), 820. https://doi.org/10.3390/nu17050820