

Factors That May Affect Breast Milk Macronutrient and Energy Content: A Critical Review



Abstract

1. Introduction
1.1. State of the Art
1.2. Collection and Analysis of Breast Milk
1.3. Methods of Feeding Preterm Infants Based on Breast Milk
1.4. Inaccuracy in Breast Milk Nutritional Content Estimates
1.5. Factors That May Affect the Macronutrient and Energy Content of Breast Milk
2. Objective
3. Literature Search and Data Analysis
4. Review Results
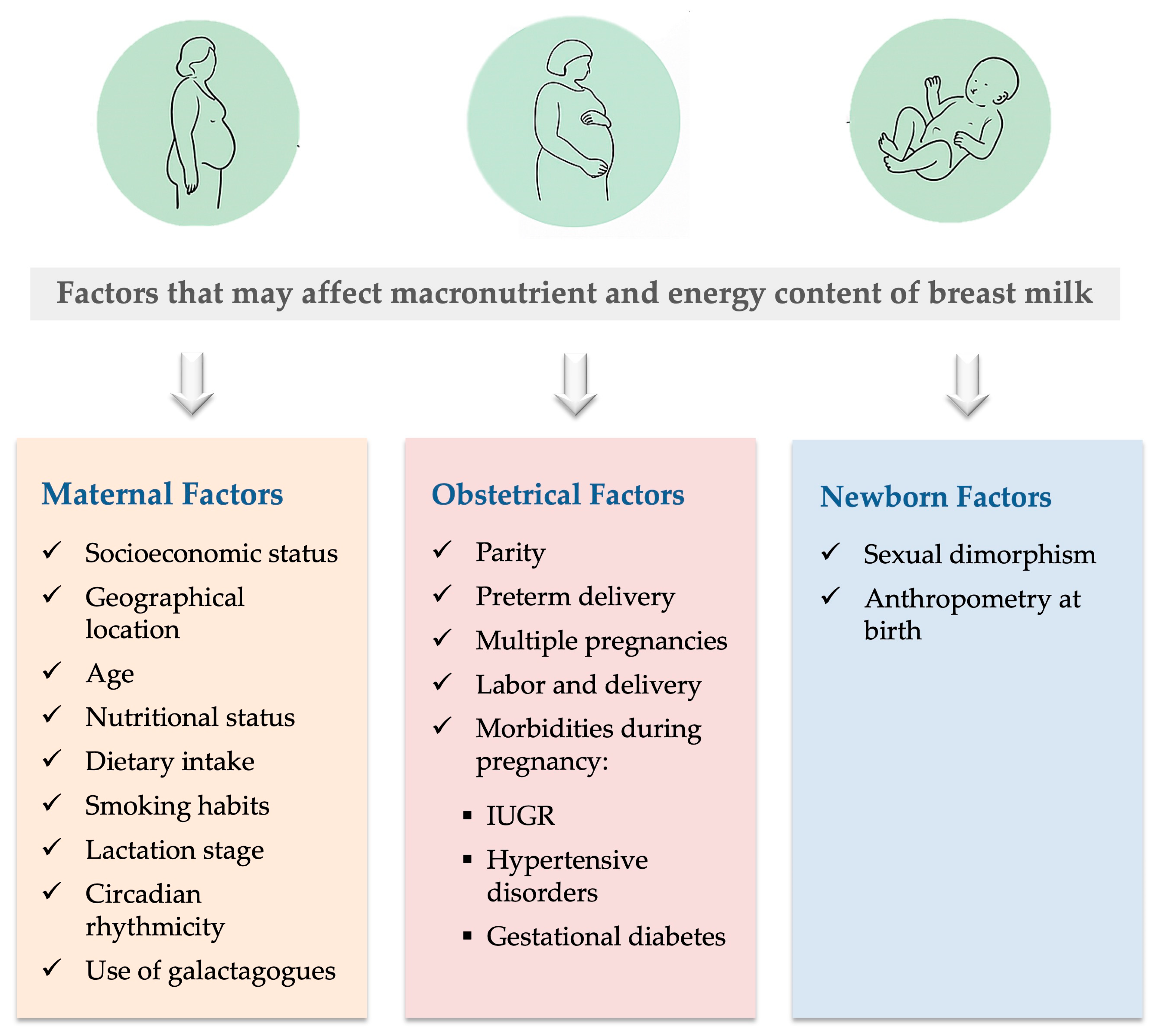
- -
- Maternal factors, including: maternal age, maternal nutritional status and dietary intake, lactation stage, circadian rhythmicity, and galactagogues use;
- -
- Obstetrical factors, including: socioeconomic status, geographical location, parity, preterm delivery, multiple pregnancy, labor, type of delivery, and pregnancy morbidities that comprise intrauterine growth restriction, hypertensive disorders, and gestational diabetes mellitus;
- -
- Neonatal factors, including sexual dimorphism and anthropometry at birth.
4.1. Maternal Factors
4.1.1. Socioeconomic Status
4.1.2. Geographical Location
4.1.3. Maternal Age
4.1.4. Maternal Nutritional Status and Dietary Intake
4.1.5. Smoking Habits
4.1.6. Lactation Stage
4.1.7. Circadian Rhythmicity
4.1.8. Galactagogues Use
4.2. Obstetrical Factors
4.2.1. Parity
4.2.2. Preterm Delivery
4.2.3. Multiple Pregnancy
4.2.4. Labor and Delivery
4.2.5. Pregnancy Morbidities
Intrauterine Growth Restriction
Hypertensive Disorders
Gestational Diabetes Mellitus
4.3. Neonatal Factors
4.3.1. Sexual Dimorphism
4.3.2. Anthropometry at Birth
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cao, Y.; Jiang, S.; Sun, J.; Hei, M.; Wang, L.; Zhang, H.; Ma, X.; Wu, H.; Li, X.; Sun, H.; et al. Assessment of neonatal intensive care unit practices, morbidity, and mortality among very preterm infants in China. JAMA Netw. Open 2021, 4, e2118904. [Google Scholar] [CrossRef]
- Alanazi, M.; Altawili, M.A.; Khayyal, A.I.; Alahmari, A.S.; Alhakami, A.A.; Alshehri, A.M.A. Impact of early nutrition interventions on the growth and development of preterm infants: A narrative review. Cureus 2024, 16, e54888. [Google Scholar] [CrossRef] [PubMed]
- Ruys, C.A.; van de Lagemaat, M.; Rotteveel, J.; Finken, M.J.J.; Lafeber, H.N. Improving long-term health outcomes of preterm infants: How to implement the findings of nutritional intervention studies into daily clinical practice. Eur. J. Pediatr. 2021, 180, 1665–1673. [Google Scholar] [CrossRef]
- Notarbartolo di Villarosa do Amaral, Y.; Marano Rocha, D.; Lopes da Silva, L.M.; Valente Mendes Soares, F.; Lopes Moreira, M.E. Do maternal morbidities change the nutritional composition of human milk?—A systematic review. Cienc. Saude Coletiva 2019, 24, 2491–2498. [Google Scholar] [CrossRef]
- Petersohn, I.; Hellinga, A.H.; van Lee, L.; Keukens, N.; Bont, L.; Hettinga, K.A.; Feskens, E.J.M.; Brouwer-Brolsma, E.M. Maternal diet and human milk composition: An updated systematic review. Front. Nutr. 2024, 10, 1320560. [Google Scholar] [CrossRef]
- Bauer, J.; Gerss, J. Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants. Clin. Nutr. 2011, 30, 215–220. [Google Scholar] [CrossRef]
- Borràs-Novell, C.; Herranz Barbero, A.; Balcells Esponera, C.; López-Abad, M.; Aldecoa Bilbao, V.; Izquierdo Renau, M.; Iglesias Platas, I. Influence of maternal and perinatal factors on macronutrient content of very preterm human milk during the first weeks after birth. J. Perinatol. 2022, 43, 52–59. [Google Scholar] [CrossRef]
- Favara, G.; Maugeri, A.; Barchitta, M.; Lanza, E.; Magnano San Lio, R.; Agodi, A. Maternal lifestyle factors affecting breast milk composition and infant health: A systematic review. Nutrients 2024, 17, 62. [Google Scholar] [CrossRef]
- Hashemi Javaheri, F.S.; Karbin, K.; Senobari, M.A.; Hakim, H.G.; Hashemi, M. The association between maternal body mass index and breast milk composition: A systematic review. Nutr. Rev. 2025, 83, 83–111. [Google Scholar] [CrossRef]
- Voerman, E.; Santos, S.; Patro Golab, B.; Amiano, P.; Ballester, F.; Barros, H.; Bergström, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: An individual participant data meta-analysis. PLoS Med. 2019, 16, e1002744. [Google Scholar] [CrossRef] [PubMed]
- Ellsworth, L.; Perng, W.; Harman, E.; Das, A.; Pennathur, S.; Gregg, B. Impact of maternal overweight and obesity on milk composition and infant growth. Matern. Child. Nutr. 2020, 16, e12979. [Google Scholar] [CrossRef]
- Mimouni, F.B.; Lubetzky, R.; Yochpaz, S.; Mandel, D. Preterm Human Milk Macronutrient and Energy Composition—A systematic review and meta-analysis. Clin. Perinatol. 2017, 44, 165–172. [Google Scholar] [CrossRef]
- Correia, L.; Cardoso, M.; Papoila, A.L.; Alves, M.; Virella, D.; Ramalho, R.; Pereira, P.; Macedo, I.; Tomé, T.; Cohen, Á.; et al. Does fetal growth adequacy affect the nutritional composition of mothers’ milk? A historical cohort study. Am. J. Perinatol. 2021, 40, 163–171. [Google Scholar] [CrossRef]
- Arenas, G.; Barrera, M.J.; Contreras-Duarte, S. The impact of maternal chronic inflammatory conditions on breast milk composition: Possible influence on offspring metabolic programming. Nutrients 2025, 17, 387. [Google Scholar] [CrossRef]
- Shapira, D.; Mandel, D.; Mimouni, F.B.; Moran-Lev, H.; Marom, R.; Mangel, L.; Lubetzky, R. The effect of gestational diabetes mellitus on human milk macronutrients content. J. Perinatol. 2019, 39, 820–823. [Google Scholar] [CrossRef]
- Viswanathan, S.; Thoene, M.; Alja’nini, Z.; Alur, P.; McNelis, K. Body composition in preterm infants: Current insights and emerging perspectives. Children 2025, 12, 53. [Google Scholar] [CrossRef]
- Alur, P.; Ramarao, S. Sex differences in preterm nutrition and growth: The evidence from human milk associated studies. J. Perinatol. 2022, 42, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Galante, L.; Milan, A.M.; Reynolds, C.M.; Cameron-Smith, D.; Vickers, M.H.; Pundir, S. Sex-specific human milk composition: The role of infant sex in determining early life nutrition. Nutrients 2018, 10, 1194. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Boquien, C.-Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of human milk for preterm infants: Update and recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef] [PubMed]
- Leghi, G.E.; Middleton, P.F.; Netting, M.J.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. A systematic review of collection and analysis of human milk for macronutrient composition. J. Nutr. 2020, 150, 1652–1670. [Google Scholar] [CrossRef] [PubMed]
- Czosnykowska-Łukacka, M.; Królak-Olejnik, B.; Orczyk-Pawiłowicz, M. Breast milk macronutrient components in prolonged lactation. Nutrients 2018, 10, 1893. [Google Scholar] [CrossRef]
- Billard, H.; Simon, L.; Desnots, E.; Sochard, A.; Boscher, C.; Riaublanc, A.; Alexandre-Gouabau, M.-C.; Boquien, C.-Y. Calibration adjustment of the mid-infrared analyzer for an accurate determination of the macronutrient composition of human milk. J. Hum. Lact. 2015, 32, NP19–NP27. [Google Scholar] [CrossRef] [PubMed]
- Giuffrida, F.; Austin, S.; Cuany, D.; Sanchez-Bridge, B.; Longet, K.; Bertschy, E.; Sauser, J.; Thakkar, S.K.; Lee, L.Y.; Affolter, M. Comparison of macronutrient content in human milk measured by mid-infrared human milk analyzer and reference methods. J. Perinatol. 2018, 39, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.; Kudla, U.; Nyakayiru, J.; Brouwer-Brolsma, E.M. Maternal dietary intake, nutritional status and macronutrient composition of human breast milk: Systematic review. Br. J. Nutr. 2022, 127, 1796–1820. [Google Scholar] [CrossRef]
- Leghi, G.E.; Netting, M.J.; Middleton, P.F.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. The impact of maternal obesity on human milk macronutrient composition: A systematic review and meta-analysis. Nutrients 2020, 12, 934. [Google Scholar] [CrossRef]
- Embleton, N.D.M.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.M.; Iacobelli, S.; et al. Enteral nutrition in preterm infants (2022): A position paper from the ESPGHAN Committee on Nutrition and Invited Experts. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 248–268. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Recommendations for Care of the Preterm or Low-Birth-Weight Infant. 2022. Available online: https://www.who.int/publications/i/item/9789240058262 (accessed on 28 July 2025).
- Brown, J.V.E.; Lin, L.; Embleton, N.D.; Harding, J.E.; McGuire, W. Multi-nutrient fortification of human milk for preterm infants. Cochrane Database Syst. Rev. 2020, 6, CD000343. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. Adjustable fortification of human milk fed to preterm infants: Does it make a difference? J. Perinatol. 2006, 26, 614–621. [Google Scholar] [CrossRef]
- Cardoso, M.; Virella, D.; Papoila, A.L.; Alves, M.; Macedo, I.; Silva, D.E.; Pereira-Da-Silva, L. Individualized fortification based on measured macronutrient content of human milk improves growth and body composition in infants born less than 33 weeks: A mixed-cohort study. Nutrients 2023, 15, 1533. [Google Scholar] [CrossRef]
- World Health Organization. Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 23 July 2025).
- Miris. About Us. Available online: https://www.mirissolutions.com/about-us (accessed on 20 July 2025).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The levels of evidence and their role in evidence-based medicine. Plast. Reconstr. Surg. 2011, 128, 305–310. [Google Scholar] [CrossRef]
- Burianova, I.; Bronsky, J.; Pavlikova, M.; Janota, J.; Maly, J. Maternal body mass index, parity and smoking are associated with human milk macronutrient content after preterm delivery. Early Hum. Dev. 2019, 137, 104832. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, C.J.; Kang, N.M. Maternal factors affecting the macronutrient composition of transitional human milk. Int. J. Environ. Res. Public Health 2022, 19, 3308. [Google Scholar] [CrossRef]
- Thakur, A.; Kler, N.; Garg, P.; Gandhi, P.; Srivastava, S. Macronutrient analysis of human milk and factors associated with its composition in mothers of preterm infants ≤ 32 weeks. Eur. J. Pediatr. 2021, 180, 3527–3534. [Google Scholar] [CrossRef]
- Sahin, S.; Ozdemir, T.; Katipoglu, N.; Akcan, A.B.; Kaynak Turkmen, M. Comparison of changes in breast milk macronutrient content during the first month in preterm and term infants. Breastfeed. Med. 2020, 15, 56–62. [Google Scholar] [CrossRef]
- Fischer Fumeaux, C.J.; Garcia-Rodenas, C.L.; De Castro, C.A.; Courtet-Compondu, M.-C.; Thakkar, S.K.; Beauport, L.; Tolsa, J.-F.; Affolter, M. Longitudinal analysis of macronutrient composition in preterm and term human milk: A prospective cohort study. Nutrients 2019, 11, 1525. [Google Scholar] [CrossRef]
- Hahn, W.-H.; Song, J.-H.; Song, S.; Kang, N.M. Do gender and birth height of infant affect calorie of human milk? An association study between human milk macronutrient and various birth factors. J. Matern. Fetal Neonatal Med. 2016, 30, 1608–1612. [Google Scholar] [CrossRef]
- Powe, C.E.; Knott, C.D.; Conklin-Brittain, N. Infant sex predicts breast milk energy content. Am. J. Hum. Biol. 2009, 22, 50–54. [Google Scholar] [CrossRef]
- Dritsakou, K.; Liosis, G.; Valsami, G.; Polychronopoulos, E.; Skouroliakou, M. The impact of maternal- and neonatal-associated factors on human milk’s macronutrients and energy. J. Matern. Fetal Neonatal Med. 2016, 30, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Koutsiafti, P.; Soultani, G.; Kechagias, S.; Grivea, I.; Malissiova, E. Macronutrient composition of breast milk for full term and premature infants: Correlation to nutritional and socioeconomic factors. Int. J. Caring Sci. 2021, 14, 608–616. [Google Scholar]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef] [PubMed]
- Dizdar, E.A.; Sari, F.N.; Degirmencioglu, H.; Canpolat, F.E.; Oguz, S.S.; Uras, N.; Dilmen, U. Effect of mode of delivery on macronutrient content of breast milk. J. Matern. Fetal Neonatal Med. 2013, 27, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Marano, D.; Melo, R.X.; da Silva, D.A.; Vilarim, M.M.; Moreira, M.E.L. Nutritional composition of human milk and its association with maternal and perinatal factors. Rev. Paul. Pediatr. 2023, 42, e2023001. [Google Scholar] [CrossRef]
- Bachour, P.; Yafawi, R.; Jaber, F.; Choueiri, E.; Abdel-Razzak, Z. Effects of smoking, mother’s age, body mass index, and parity number on lipid, protein, and secretory immunoglobulin a concentration of human milk. Breastfeed. Med. 2012, 7, 179–188. [Google Scholar] [CrossRef]
- Campbell-Yeo, M.L.; Allen, A.C.; Joseph, K.S.; Ledwidge, J.M.; Caddell, K.; Allen, V.M.; Dooley, K.C. Effect of domperidone on the composition of preterm human breast milk. Pediatrics 2010, 125, e107–e114. [Google Scholar] [CrossRef] [PubMed]
- Chathyushya, K.B.; Hemalatha, R.; Ananthan, R.; Babu, J.J.; Devraj, J.P.; Banjara, S.K.; Alimelu, M.; Pradeep, R.K.; Nitasha, B.; Shiva, P.M. Macronutrient composition of term and preterm human milk of different socio economic groups. Prostaglandins Leukot. Essent. Fat. Acids 2023, 192, 102571. [Google Scholar] [CrossRef]
- Samuel, T.M.; Zhou, Q.; Giuffrida, F.; Munblit, D.; Verhasselt, V.; Thakkar, S.K. Nutritional and non-nutritional composition of human milk is modulated by maternal, infant, and methodological factors. Front. Nutr. 2020, 7, 576133. [Google Scholar] [CrossRef]
- Khelouf, N.; Haoud, K.; Meziani, S.; Fizir, M.; Ghomari, F.N.; Khaled, M.B.; Kadi, N. Effect of infant’s gender and lactation period on biochemical and energy breast milk composition of lactating mothers from Algeria. J. Food Compos. Anal. 2023, 115, 104889. [Google Scholar] [CrossRef]
- Bottin, J.H.; Eussen, S.R.B.M.; Igbinijesu, A.J.; Mank, M.; Koyembi, J.J.; Nyasenu, Y.T.; Ngaya, G.; Mad-Bondo, D.; Kongoma, J.B.; Stahl, B.; et al. Food insecurity and maternal diet influence human milk composition between the infant’s birth and 6 months after birth in Central-Africa. Nutrients 2022, 14, 4015. [Google Scholar] [CrossRef]
- Argov-Argaman, N.; Mandel, D.; Lubetzky, R.; Hausman Kedem, M.; Cohen, B.-H.; Berkovitz, Z.; Reifen, R. Human Milk Fatty acids composition is affected by maternal age. J. Matern. Neonatal Med. 2016, 30, 34–37. [Google Scholar] [CrossRef]
- Italianer, M.F.; Naninck, E.F.G.; Roelants, J.A.; Van Der Horst, G.T.; Reiss, I.K.M.; van Goudoever, J.B.; Joosten, K.F.M.; Chaves, I.; Vermeulen, M.J. Circadian variation in human milk composition, a systematic review. Nutrients 2020, 12, 2328. [Google Scholar] [CrossRef]
- Hosseini, M.; Valizadeh, E.; Hosseini, N.; Khatibshahidi, S.; Raeisi, S. The Role of Infant Sex on Human Milk Composition. Breastfeed. Med. 2020, 15, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Bravi, F.; Wiens, F.; Decarli, A.; Dal Pont, A.; Agostoni, C.; Ferraroni, M. Impact of maternal nutrition on breast-milk composition: A systematic review. Am. J. Clin. Nutr. 2016, 104, 646–662. [Google Scholar] [CrossRef] [PubMed]
- Mammaro, A.; Carrara, S.; Cavaliere, A.; Ermito, S.; Dinatale, A.; Pappalardo, E.M.; Militello, M.; Pedata, R. Hypertensive disorders of pregnancy. J. Prenat. Med. 2009, 3, 1–5. [Google Scholar]
- Quinn, E.A. No evidence for sex biases in milk macronutrients, energy, or breastfeeding frequency in a sample of Filipino mothers. Am. J. Phys. Anthropol. 2013, 152, 209–216. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Maternal nutritional status | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | The mature milk from overweight and obese mothers had a higher energy content, over the first 4 weeks postpartum. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Maternal nutritional status | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | The milk from mothers with pre-pregnancy BMI 30 kg/m2 or higher had a higher energy content. LOE II-1 | Burianova, et al. (2019) [35] |
| Maternal nutritional status | Systematic review of 14 studies | Not specified | The milk from overweight mothers had a higher energy content. | Notarbartolo di Villarosa do Amaral, et al. (2019) [4] |
| Maternal dietary intake | Systematic review of 20 studies | Not specified | Protein intake was positively associated with milk energy content. | Favara, et al. (2024) [8] |
| Maternal dietary intake | Cross-sectional, at 2 weeks postpartum | 159 mothers of term infants | Energy percentages from carbohydrates and fat intake were positively correlated with milk energy content. LOE II-1 | Ryoo, et al. (2022) [36] |
| Lactation stage | Prospective, during the first 4 weeks postpartum | 60 mothers delivering before or at 32 weeks of gestation | Energy content increased during the first 4 weeks of lactation. LOE II-1 | Thakur, et al. (2021) [37] |
| Lactation stage | Prospective, during the first 4 weeks postpartum | 60 mothers (39 of term and 21 of preterm infants) | Energy content increased over time in term but not in preterm milk. LOE II-1 | Sahin, et al. (2020) [38] |
| Lactation stage | Prospective, during 4 months for preterm and 2 months for term infants | 61 mothers (34 of term and 27 of preterm infants) | Energy content of preterm milk was higher than that of term milk during the first two weeks of lactation, whereas in term milk it was higher later during lactation. LOE II-1 | Fischer Fumeaux, et al. (2019) [39] |
| Lactation stage | Systematic review and meta-analysis during the first 12 weeks postpartum | Not specified | Energy content initially increased, and then it reached a steady state in preterm milk. | Mimouni, et al. (2017) [12] |
| Preterm delivery | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 28 weeks of gestation | The milk from mothers who delivered more prematurely had a higher total energy content than the milk from mothers who delivered at term. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Preterm delivery | Historical cohort, during the first 4 weeks postpartum | 73 mothers delivering before 37 weeks of gestation | The degree of prematurity was positively associated with the energy content in milk, which was significantly higher in extremely preterm infants compared with very preterm infants (average: +5.95 kcal/dL; 95% CI: 2.16–9.73; p = 0.003). LOE II-1 | Correia, et al. (2023) [13] |
| Preterm delivery | Prospective, during the first 8 weeks postpartum | 113 mothers delivering between 23–33 weeks of gestation and 10 mothers delivering at term | The milk from mothers delivering prematurely had a significantly higher energy content than the milk from mothers who delivered at term. LOE II-1 | Bauer, et al. (2011) [6] |
| Multiple pregnancy | Historical cohort, during the first 4 weeks postpartum | 73 mothers delivering before 37 weeks of gestation | A week positive association was found between total energy content and single pregnancies (average: +3.38 kcal/dL; 95% CI: 0.07–6.83; p = 0.057). LOE II-1 | Correia, et al. (2023) [13] |
| Hypertensive disorders | Narrative review | Not specified | The milk from mothers with arterial hypertension had a higher energy content than the milk from normotensive mothers. | Arenas, et al. (2025) [14] |
| Hypertensive disorders | Historical cohort, during the first 4 weeks postpartum | 73 mothers delivering before 37 weeks of gestation | Chronic hypertension was positively associated with total energy content (average: +6.28 kcal/dL; 95% CI: 0.54–12.01; p = 0.034). LOE II-1 | Correia, et al. (2023) [13] |
| Sexual dimorphism | Narrative review | Not specified | The milk from mothers of males had higher energy content than the milk from mothers of females. | Alur, et al. (2022) [17] |
| Sexual dimorphism | Prospective, during 4 and 2 months postpartum for preterm and term deliveries, respectively | 61 mothers (34 of term and 27 of preterm infants) | Male gender was positively associated with the energy content of preterm and term milk. LOE II-1 | Fischer Fumeaux, et al. (2019) [39] |
| Sexual dimorphism | Cross-sectional | 418 mothers | The milk from mothers of females had a higher energy content (OR = 0.33, p = 0.017) than the milk from mothers of males. LOE II-1 | Hahn, et al. (2016) [40] |
| Sexual dimorphism | Cross-sectional | 25 mothers | The milk from mothers of males had a significantly higher energy content than the milk from mothers of females. LOE II-1 | Powe, et al. (2009) [41] |
| Anthropometry at birth | Cross-sectional | 418 mothers | The infant’s height at birth was positively associated with the milk energy content (OR = 0.74, p < 0.001). LOE II-1 | Hahn, et al. (2016) [40] |
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Preterm delivery | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 28 weeks of gestation | Gestational age was negatively correlated with the milk total energy content (rho: −0.193, p = 0.003) content. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Preterm delivery | Prospective, on the 3rd, 7th and 30th day of lactation | 305 mothers of preterm and term infants | Gestational age was negatively associated with the energy content in the colostrum, transitional and mature milk. LOE II-1 | Dritsakou, et al. (2017) [42] |
| Multiple pregnancy | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | Multiple pregnancy was negatively associated with the total energy content of milk over the first 4 weeks postpartum. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Hypertensive disorders | Narrative review | Not specified | Milk from mothers with gestational arterial hypertension had a lower energy content than the milk from mothers without this condition. | Arenas, et al. (2025) [14] |
| Hypertensive disorders | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | Hypertensive disorders were negatively associated with the total energy content in the early milk. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Gestational diabetes mellitus | Prospective, at 14 days postpartum | 62 mothers of term infants | Gestational diabetes mellitus was negatively associated with the milk energy content. | Shapira, et al. (2019) [15] |
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Maternal socioeconomic status | Prospective | 50 mothers of preterm and full-term infants | The milk from mothers working in the private sector or that were self-employed had a significantly higher protein content than the milk from mothers working in the public sector or that were unemployed (p < 0.01). LOE II-1 | Koutsiafti, et al. (2021) [43] |
| Maternal age | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | The milk from mothers aged 35 years or older was weakly positively correlated with the protein content at weeks 1 and 2 postpartum (r = 0.216, p = 0.037 and r = 0.322, p = 0.001, respectively), compared to younger mothers. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Maternal nutritional status | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | The mature milk from overweight and obese mothers was positively associated with the protein content, over the first 4 weeks postpartum. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Maternal dietary intake | Systematic review of 20 studies | Not specified | Maternal protein intake was positively associated with the milk protein content. | Favara, et al. (2024) [8] |
| Preterm delivery | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | The milk from mothers delivering more prematurely had a higher true protein content than the milk from mothers who delivered at term (rho: −0.307, p < 0.001). LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Preterm delivery | Historical cohort, during the first 4 weeks postpartum | 73 mothers delivering before 37 weeks of gestation | The degree of prematurity was positively associated with the true protein content in milk, which was significantly higher in extremely preterm infants compared with very preterm and moderate preterm infants (average +0.19 g/dL; 95% CI: 0.01–0.38; p = 0.043 and average +0.28 g/dL; 95% CI: 0.05–0.51; p = 0.017, respectively). LOE II-1 | Correia, et al. (2023) [13] |
| Preterm delivery | Systematic review and meta-analysis of 41 studies | 3142 mothers of preterm and term infants | The milk from mothers delivering prematurely had a higher true protein content than the milk from mothers delivering at term, with maximum mean differences up to 35% in the first 3 days after birth. | Gidrewicz, et al. (2014) [44] |
| Preterm delivery | Prospective, during the first 8 weeks postpartum | 113 mothers delivering between 23–33 weeks of gestation and 10 mothers delivering at term | The milk from mothers delivering before 28 weeks of gestation had a significantly higher protein content than the milk from mothers delivering later (between 32–33 weeks of gestation or after 37 weeks of gestation). LOE II-1 | Bauer, et al. (2011) [6] |
| Labor and delivery | Prospective, during the first 4 weeks postpartum | 60 mothers (39 of term and 21 of preterm infants) | The milk from mothers who delivered by cesarean section had a higher protein content than the milk from mothers who delivered by vaginal delivery (1.794–0.848 g/dL; 1.543–0.514 g/dL respectively; p = 0.021). LOE II-1 | Sahin, et al. (2020) [38] |
| Labor and delivery | Prospective, on the 2nd postpartum day | 24 mothers of term infants | Vaginal delivery was associated with a higher protein content in the colostrum. LOE II-1 | Dizdar, et al. (2014) [45] |
| Intrauterine growth restriction | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | The milk from mothers of infants with intrauterine growth restriction had a higher protein content at or after 4 weeks postpartum than the milk from mothers of infants with normal growth. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Hypertensive disorders | Narrative review | Not specified | The milk from mothers with arterial hypertension had a higher protein content than the milk from normotensive mothers. | Arenas, et al. (2025) [14] |
| Hypertensive disorders | Historical cohort, during the first 4 weeks postpartum | 73 mothers delivering before 37 weeks of gestation | Positive association with chronic hypertension and true protein content (average +0.91 g/dL; 95% CI: 0.63–1.19; p < 0.001) LOE II-1 Positive association with hypertension induced by pregnancy and true protein content (average +0.25 g/dL; 95% CI: 0.07–0.44; p = 0.007) LOE II-1 | Correia, et al. (2023) [13] |
| Hypertensive disorders | Systematic review of 14 studies | Not specified | Hypertension disorders were positively associated with total protein content in colostrum and mature milk compared to the milk from normotensive mothers. | Notarbartolo di Villarosa do Amaral, et al. (2019) [4] |
| Preeclampsia | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | Preeclampsia was positively associated with the total protein content in early milk. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Maternal nutritional status | Cross-sectional study | 181 mothers | Pre-pregnancy obesity and gestational weight gain were associated with a lower protein content in milk compared to eutrophic mothers and those with adequate gestational weight gain, respectively. LOE II-1 | Marano, et al. (2023) [46] |
| Maternal nutritional status | Systematic review of 50 studies | Not specified | Higher body fat was associated with a lower milk protein content. | Adhikari, et al. (2022) [24] |
| Smoking habits | Cross-sectional | 66 mothers | Smoking habits were negatively associated with milk protein content. LOE II-1 | Bachour, et al. (2012) [47] |
| Lactation stage | Prospective, during the first 4 weeks postpartum | 60 mothers delivering before or at 32 weeks of gestation | True protein content decreased during the first 4 weeks of lactation. LOE II-1 | Thakur, et al. (2021) [37] |
| Lactation stage | Prospective, during the first 4 weeks postpartum | 60 mothers (39 of term and 21 of preterm infants) | The milk protein content decreased over time in the milk from mothers delivering prematurely and at term. LOE II-1 | Sahin, et al. (2020) [38] |
| Lactation stage | Prospective, during 4 and 2 months postpartum for preterm and term deliveries, respectively | 61 mothers (34 of term and 27 of preterm infants) | The protein content of both preterm and term milk decreased from birth to four months postpartum. Although there were no significant differences in the protein content between the two groups during this period, preterm milk had a lower protein content when reached term equivalent age. LOE II-1 | Fischer Fumeaux, et al. (2019) [39] |
| Lactation stage | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | The milk protein content decreased for the first three weeks postpartum and then remained stable until the end of the 6th week. LOE II-1 | Burianova, et al. (2019) [35] |
| Lactation stage | Systematic review and meta-analysis of preterm milk composition during the first 12 weeks postpartum | Not specified | There was a progressive decrease in milk total protein content. | Mimouni, et al. (2017) [12] |
| Lactation stage | Cross-sectional | 66 mothers | Protein content was lower in mature milk than in transitional milk. LOE II-1 | Bachour, et al. (2012) [47] |
| Galactagogues | Clinical trial, at 7 and 14 days postpartum | 46 mothers | The milk from mothers who used domperidone had a lower protein content than the milk from mothers who used placebo. LOE I | Campbell-Yeo et al. (2010) [48] |
| Parity | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | Parity was negatively associated with the milk protein content. LOE II-1 | Burianova, et al. (2019) [35] |
| Preterm delivery | Prospective, on the 3rd, 7th and 30th day of lactation | 305 mothers of preterm and term infants | The more preterm the birth, the higher the protein content in mature milk. LOE II-1 | Dritsakou, et al. (2017) [42] |
| Multiple pregnancy | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | Multiple pregnancy was negatively associated with the total protein content in milk over the first 4 weeks postpartum. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Labor and delivery | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | Labor before birth was associated with a lower protein content of milk at 4 weeks postpartum. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Maternal socioeconomic status | Cross-sectional | 120 mothers of term and preterm infants | The milk from mothers with a lower socioeconomic status was significantly richer in monounsaturated and n-9 fatty acids, while mothers with an upper socioeco-nomic status was significantly richer in polyunsaturated, n-3, and n-6 fatty acids. LOE II-1 | Chathyushya, et al. (2023) [49] |
| Maternal socioeconomic status | Prospective | 50 mothers of preterm and full-term infants | The milk from mothers working in the private sector or that were self-employed had a significantly higher fat content than the milk from mothers working in the public sector or that were unemployed (p < 0.01). LOE II-1 | Koutsiafti, et al. (2021) [43] |
| Geographical location | Narrative review | Not specified | Swedish mothers’ breast milk had higher EPA and DHA content compared to Chinese mothers’ breast milk. | Samuel, et al. (2020) [50] |
| Maternal age | Prospective, on the 3rd, 7th and 30th day of lactation | 305 mothers of pre-term and term infants | Maternal age was positively correlated with the fat content in colostrum, transitional and mature milk. LOE II-1 | Dritsakou, et al. (2017) [42] |
| Maternal nutritional status | Systematic review of 83 studies | 11,310 mothers | Higher maternal BMI was associated with a higher ratio of n-6/n-3 polyunsaturated fatty acids. | Hashemi Javaheri, et al. (2025) [9] |
| Maternal nutritional status | Narrative review | Not specified | The milk from obese mothers had a higher total fat content and a higher ratio of n-6/n-3 polyunsaturated fatty acids. | Arenas, et al. (2025) [14] |
| Maternal nutritional status | Systematic review of 20 studies | Not specified | The milk from overweight and obese mothers had a higher saturated fatty acids content, a higher n-6/n-3 ratio, and a higher monounsaturated fatty acids content, compared to normal-weight mothers. | Favara, et al. (2024) [8] |
| Maternal nutritional status | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | Mature milk from overweight and obese mothers had a higher fat content over the first 4 weeks postpartum. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Maternal nutritional status | Systematic review of 50 studies | Not specified | Higher maternal body fat was associated with a higher milk fat content | Adhikari, et al. (2022) [24] |
| Maternal nutritional status | Systematic review and meta-analysis | 5078 lactating mothers in the review, 872 in the meta-analysis | Maternal overweight and obesity were positively correlated with milk fat content. However, in transitional milk, the fat content was lower in overweight/obese mothers than in normal-weight mothers. | Leghi, et al. (2020) [25] |
| Maternal nutritional status | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | The milk from mothers with a pre-pregnancy BMI of 30 kg/m2 or higher had a higher fat content. LOE II-1 | Burianova, et al. (2019) [35] |
| Maternal nutritional status | Systematic review of 14 studies | Not specified | The milk from overweight mothers had a higher fat content. | Notarbartolo di Villarosa do Amaral, et al. (2019) [4] |
| Maternal dietary intake | Systematic review of 27 studies | 7138 mothers | Maternal fish intake was positively associated with the ALA, DHA, and EPA content in milk. | Petersohn, et al. (2024) [5] |
| Maternal dietary intake | Systematic review of 27 studies | 7138 mothers | Maternal PUFAs intake was positively correlated with the PUFAs content in milk. | Petersohn, et al. (2024) [5] |
| Maternal dietary intake | Systematic review of 20 studies | Not specified | Maternal protein intake was positively associated with the milk fat content. | Favara, et al. (2024) [8] |
| Lactation stage | Prospective, during the first 4 weeks postpartum | 60 mothers delivering before or at 32 weeks of gestation | The milk fat content increased during the first 4 weeks of lactation. LOE II-1 | Thakur, et al. (2021) [37] |
| Lactation stage | Prospective, during the first 4 weeks postpartum | 60 mothers (39 of term and 21 of preterm infants) | Fat content increased both in preterm and term milk over lactation time. LOE II-1 | Sahin, et al. (2020) [38] |
| Lactation stage | Prospective, during 4 and 2 months postpartum for preterm and term deliveries, respectively | 61 mothers (34 of term and 27 of preterm infants) | Fat content of preterm milk was higher than of term milk in the first two weeks of lactation, whereas fat content in term milk was higher later in the lactation period. LOE II-1 | Fischer Fumeaux, et al. (2019) [39] |
| Lactation stage | Systematic review and meta-analysis of preterm milk composition during the first 12 weeks postpartum | Not specified | The milk fat content progressively increased during lactation. | Mimouni, et al. (2017) [12] |
| Lactation stage | Cross-sectional | 66 mothers | Fat content was higher in mature milk than in transitional milk. LOE II-1 | Bachour, et al. (2012) [47] |
| Parity | Narrative review | Not specified | The milk from multiparous mothers had a higher fat content than the milk from nulliparous mothers. | Arenas, et al. (2025) [14] |
| Parity | Cross-sectional | 66 mothers | The milk fat content increased in parallel with an increase in parity number up to 3. LOE II-1 | Bachour, et al. (2012) [47] |
| Preterm delivery | Prospective, during the first 8 weeks postpartum | 113 mothers delivering between 23–33 weeks of gestation and 10 mothers delivering at term | The milk from mothers delivering before 28 weeks of gestation had a significantly higher fat content than the milk from mothers delivering at term. LOE II-1 | Bauer, et al. (2011) [6] |
| Labor and delivery | Cross-sectional | 418 mothers | The milk from mothers who had a cesarean section had a higher fat content than the milk from mothers who delivered vaginally (OR = 2.47, p < 0.001). LOE II-1 | Hahn, et al. (2016) [40] |
| Hypertensive disorders | Narrative review | Not specified | The milk from mothers with arterial hypertension had a higher fat content compared with normotensive mothers. | Arenas, et al. (2025) [14] |
| Sexual dimorphism | Prospective, during 720 days postpartum | 92 mothers | Colostrum and mature milk from mothers of males had a higher fat content than the milk from mothers of females. LOE II-1 | Khelouf, et al. (2023) [51] |
| Sexual dimorphism | Narrative review | Not specified | The milk from mothers of males had higher fat content than the milk from mothers of females. | Alur, et al. (2022) [17] |
| Sexual dimorphism | Prospective, during 4 and 2 months postpartum for preterm and term deliveries, respectively | 61 mothers (34 of term and 27 of preterm infants) | The milk from mothers of males had a higher fat content, both in preterm and term milk. LOE II-1 | Fischer Fumeaux, et al. (2019) [39] |
| Anthropometry at birth | Cross-sectional | 418 mothers | Infant’s height at birth was positively associated with the milk fat content (OR = 0.84, p = 0.004). LOE II-1 | Hahn, et al. (2016) [40] |
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Maternal socioeconomic status | Prospective, at weeks 1, 4, 11, 18, and 25 postpartum | 48 mothers | High food insecurity indexes were significantly associated with lower fatty acid (aß-coef = −7.2, p value = 0.03). LOE II-1 | Bottin, et al. (2022) [52] |
| Maternal socioeconomic status | Narrative review | Not specified | No consistent evidence of the effect of socioeconomic status on breast milk composition was found except that lower socioeconomic status was associated with lower n-3 long-chain polyunsaturated fatty acid content. | Samuel, et al. (2020) [50] |
| Geographical location | Narrative review | Not specified | Swedish mothers’ breast milk had a lower linoleic acid content compared to Chinese mothers’ breast milk. | Samuel, et al. (2020) [50] |
| Maternal age | Prospective, 14 days postpartum | 49 mothers | The transition milk from younger mothers had a lower total fat content and a higher n-6 fatty acids, EPA and ARA content than that from older mothers. LOE II-1 | Argov-Argaman, et al. (2016) [53] |
| Maternal nutritional status | Systematic review of 20 studies | Not specified | Overweight or obese mother conditions were negatively associated with milk ARA, total n-3 fatty acids, ALA, and DHA content, compared to normal-weight mothers. | Favara, et al. (2024) [8] |
| Maternal nutritional status | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | Fat content in mature milk decreased overtime, both in normal-weight and overweight mothers. LOE II-1 | Burianova, et al. (2019) [35] |
| Maternal dietary intake | Systematic review of 27 studies | 7138 mothers | The saturated fatty acids intake was negatively associated with several fatty acids content in milk. | Petersohn, et al. (2024) [5] |
| Maternal dietary intake | Systematic review of 20 studies | Not specified | The fat intake was negatively associated with the milk EPA and DHA content. | Favara, et al. (2024) [8] |
| Smoking habits | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | Smoking habits were negatively associated with the fat content in mature milk (p = 0.026). LOE II-1 | Burianova, et al. (2019) [35] |
| Smoking habits | Cross-sectional | 66 mothers | Smoking habits were negatively associated with the fat content in milk. | Bachour, et al. (2012) [47] |
| Circadian rhythmicity | Systematic review of 83 studies | 200 mothers of term infants | There is a circadian variation in milk total fat content with the acrophase in the evening. LOE II-1 | Italianer, et al. (2020) [54] |
| Preterm delivery | Prospective, on the 3rd, 7th and 30th day of lactation | 305 mothers of preterm and term infants | The more preterm the birth, the higher the fat content in colostrum, transitional, and mature milk. LOE II-1 | Dritsakou, et al. (2017) [42] |
| Intrauterine growth restriction | Historical cohort, during the first 4 weeks postpartum | 73 mothers delivering before 37 weeks of gestation | Fat content was weakly and negatively associated with IUGR, both in SGA infants and AGA infants with fetal growth deceleration (average 0.44 g/dL; 95% CI: 0.92 to 0.05; p = 0.079 and average 0.36 g/dL; 95% CI: 0.74 to 0.02; p = 0.066, respectively). LOE II-1 | Correia, et al. (2023) [13] |
| Hypertensive disorders | Narrative review | Not specified | The milk from mothers with gestational hypertension had a lower fat content compared with milk from normotensive mothers. | Arenas, et al. (2025) [14] |
| Hypertensive disorders | Narrative review | Not specified | The milk from mothers with preeclampsia was associated with a lower DHA content. | Arenas, et al. (2025) [14] |
| Hypertensive disorders | Prospective, during the first 8 weeks postpartum | 117 mothers delivering before 32 weeks of gestation | The early milk from mothers with hypertensive disorders during pregnancy, including preeclampsia, had a lower fat content than that from normotensive mothers. LOE II-1 | Borràs-Novell, et al. (2023) [7] |
| Diabetes mellitus | Systematic review of 14 studies | Not specified | Diabetes mellitus was negatively associated with the milk fat content. | Notarbartolo di Villarosa do Amaral, et al. (2019) [4] |
| Gestational diabetes mellitus | Prospective, at 14 days postpartum | 62 mothers of term infants | Gestational diabetes mellitus was negatively associated with the milk fat content. LOE II-1 | Shapira, et al. (2019) [15] |
| Sexual dimorphism | Cross-sectional | 119 mothers | The milk from mothers of males had a significantly lower fat content than the milk from mothers of females. LOE II-1 | Hosseini, et al. (2020) [55] |
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Maternal socioeconomic status | Prospective, at weeks 1, 4, 11, 18, and 25 postpartum | 48 mothers | High food insecurity indexes were significantly associated with higher lactose content in the breast milk. LOE II-1 | Bottin, et al. (2022) [52] |
| Maternal nutritional status | Narrative review | Not specified | The milk from obese mothers was associated with a higher glucose content. | Arenas, et al. (2025) [14] |
| Maternal nutritional status | Systematic review and meta-analysis | 5078 lactating mothers included in the review, and 872 in the meta-analysis | Maternal BMI and/or fat mass was positively correlated with the milk lactose content. Of note, lactose content may depend on the stage of lactation, with a higher content found in the colostrum. | Leghi, et al. (2020) [25] |
| Maternal dietary intake | Systematic review of 20 studies | Not specified | Maternal protein intake was positively associated with the milk carbohydrate content. | Favara, et al. (2024) [8] |
| Lactation stage | Prospective, during the first 4 weeks postpartum | 60 mothers (39 of term and 21 of preterm infants) | Carbohydrate content of preterm and term milk increased over time. LOE II-1 | Sahin, et al. (2020) [38] |
| Lactation stage | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | Lactation stage was positively associated with the milk carbohydrate content until the end of 3rd week postpartum. LOE II-1 | Burianova, et al. (2019) [35] |
| Lactation stage | Systematic review and meta-analysis of preterm milk composition during the first 12 weeks postpartum | Not specified | The milk carbohydrate content initially increased and then reached a steady state. | Mimouni, et al. (2017) [12] |
| Galactagogues | Clinical trial, at 7 and 14 days postpartum | 46 mothers | The milk from mothers who used domperidone had a higher carbohydrate content than in milk from those who used placebo. LOE I | Campbell-Yeo et al. (2010) [48] |
| Parity | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | Parity was positively correlated with the carbohydrate content in colostrum. LOE II-1 | Burianova, et al. (2019) [35] |
| Preterm delivery | Prospective, during the first 8 weeks postpartum | 113 mothers delivering between 23–33 weeks of gestation and 10 mothers delivering at term | The milk carbohydrate content was significantly higher in the milk from mothers delivering before 28 weeks of gestation than milk from mothers delivering at term. LOE II-1 | Bauer, et al. (2011) [6] |
| Labor and delivery | Prospective, during 6 weeks postpartum | 192 mothers of preterm infants | Vaginal delivery was positively associated with the colostrum carbohydrate content (p = 0.021). LOE II-1 | Burianova, et al. (2019) [35] |
| Labor and delivery | Cross-sectional | 418 mothers | Vaginal delivery was positively associated with the milk carbohydrate content (OR = 0.50, p = 0.005). LOE II-1 | Hahn, et al. (2016) [40] |
| Hypertensive disorders | Narrative review | Not specified | The milk from mothers with hypertension had a higher carbohydrate content, compared with the milk from normotensive mothers. | Arenas, et al. (2025) [14] |
| Sexual dimorphism | Narrative review | Not specified | The milk from mothers of males had higher carbohydrate content the milk from mothers of females. | Alur, et al. (2022) [17] |
| Sexual dimorphism | Cross-sectional | 418 mothers | The milk from mothers of females had a higher carbohydrate content (OR = 0.56, p = 0.012). LOE II-1 | Hahn, et al. (2016) [40] |
| Factor | Study Design | Sample | Outcomes | Reference |
|---|---|---|---|---|
| Maternal dietary intake | Prospective, at weeks 1, 4, 11, 18, and 25 postpartum | 48 mothers | Intake of meat, poultry, and fish was associated with lower lactose content (aß-coef = −15.6, p value = 0.01). | Bottin, et al. (2022) [52] |
| Preterm delivery | Prospective, on the 3rd, 7th and 30th day of lactation | 305 mothers of pre-term and term infants | Gestational age was negatively associated with carbohydrate content in colostrum and mature milk. LOE II-1 | Dritsakou, et al. (2017) [42] |
| Preterm delivery | Systematic review and meta-analysis of 41 studies | 3142 mothers of preterm and term infants | The lactose content was significantly lower in the milk from mothers delivering prematurely than in the milk from mothers delivering at term. | Gidrewicz, et al. (2014) [44] |
| Diabetes mellitus | Systematic review of 14 studies | Not specified | Diabetes mellitus was negatively associated with the milk lactose content. | Notarbartolo di Villarosa do Amaral, et al. (2019) [4] |
| Sexual dimorphism | Prospective, during 720 days postpartum | 92 mothers | Colostrum and mature milk from mothers of males had a lower carbohydrate and lactose content. LOE II-1 | Khelouf, et al. (2023) [51] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocha-Pinto, I.; Pereira-da-Silva, L.; Silva, D.e.; Cardoso, M. Factors That May Affect Breast Milk Macronutrient and Energy Content: A Critical Review. Nutrients 2025, 17, 2503. https://doi.org/10.3390/nu17152503
Rocha-Pinto I, Pereira-da-Silva L, Silva De, Cardoso M. Factors That May Affect Breast Milk Macronutrient and Energy Content: A Critical Review. Nutrients. 2025; 17(15):2503. https://doi.org/10.3390/nu17152503
Chicago/Turabian StyleRocha-Pinto, Inês, Luís Pereira-da-Silva, Diana e Silva, and Manuela Cardoso. 2025. "Factors That May Affect Breast Milk Macronutrient and Energy Content: A Critical Review" Nutrients 17, no. 15: 2503. https://doi.org/10.3390/nu17152503
APA StyleRocha-Pinto, I., Pereira-da-Silva, L., Silva, D. e., & Cardoso, M. (2025). Factors That May Affect Breast Milk Macronutrient and Energy Content: A Critical Review. Nutrients, 17(15), 2503. https://doi.org/10.3390/nu17152503