

Associations Between Maternal Meal Frequency Patterns During Pregnancy and Neonatal Anthropometric Outcomes: A Quantitative Cross-Sectional Study

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Sample Size
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
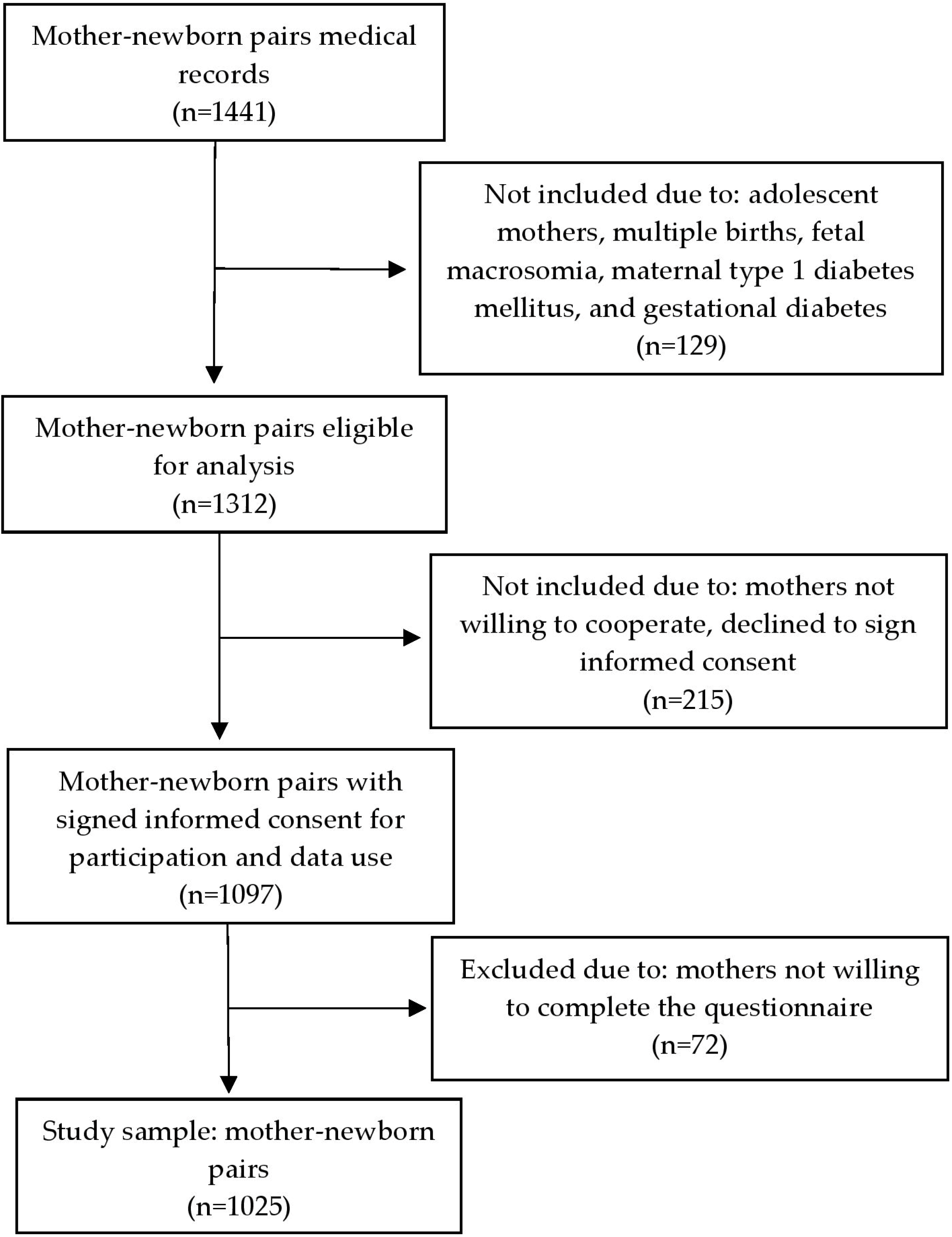
3.1. Participant Flow, Maternal Characteristics, and Neonatal Anthropometric Outcomes
3.2. Maternal Meal Patterns and Frequency
3.2.1. Weekly Meal Frequencies and Daily Consumption
3.2.2. Maternal Meal Frequency Patterns and Distribution During Pregnancy
3.3. Associations Between Maternal Meal Frequency Patterns and Neonatal Anthropometric Outcomes
3.3.1. Bivariate Analysis of Neonatal Outcomes by Maternal Meal Frequency Patterns
3.3.2. Multivariable Regression Analysis of Maternal Meal Frequency and Neonatal Outcomes
3.3.3. Interaction Analyses of Maternal Meal Frequency Patterns, Education Level, and Household Income in Relation to Neonatal Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MoBa | Norwegian Mother and Child Cohort Study |
| FFQ | Food Frequency Questionnaire |
| MUAC | Mid-upper arm circumference |
| BMI | Body mass index |
| DASH | Dietary Approaches to Stop Hypertension |
| GDM | Gestational diabetes mellitus |
| PIH | Pregnancy-induced hypertension |
References
- Adeoye, I.A.; Unogu, C.O.; Adediran, K.; Gbadebo, B.M. Determinants of Adverse Perinatal Outcomes in Ibadan, Nigeria: The Influence of Maternal Lifestyle. PLoS Glob. Public Health 2025, 5, e0004199. [Google Scholar] [CrossRef] [PubMed]
- Magnano San Lio, R.; Barchitta, M.; Maugeri, A.; Campisi, E.; Favara, G.; Granados, C.O.; La Mastra, C.; La Rosa, M.C.; Galvani, F.; Pappalardo, E.; et al. Sex Differences in Delivery and Neonatal Characteristics of New-Borns from the “MAMI-MED” Cohort. Front. Public Health 2025, 13, 1498125. [Google Scholar] [CrossRef]
- Wrottesley, S.V.; Lamper, C.; Pisa, P.T. Review of the Importance of Nutrition During the First 1000 Days: Maternal Nutritional Status and Its Associations with Fetal Growth and Birth, Neonatal and Infant Outcomes Among African Women. J. Dev. Orig. Health Dis. 2015, 7, 144–162. [Google Scholar] [CrossRef]
- Rugină, C.; Mărginean, C.O.; Meliţ, L.E.; Giga, D.V.; Modi, V.; Mărginean, C. Relationships Between Excessive Gestational Weight Gain and Energy and Macronutrient Intake in Pregnant Women. J. Int. Med. Res. 2020, 48, 8. [Google Scholar] [CrossRef]
- Iacob, O.M.; Bacârea, A.; Ruța, F.D.; Bacârea, V.C.; Gliga, F.I.; Buicu, F.; Tarcea, M.; Avram, C.; Costea, G.C.; Sin, A.I. Anthropometric Indices of the Newborns Related with Some Lifestyle Parameters of Women during Pregnancy in Tirgu Mures Region—A Pilot Study. Prog. Nutr. 2018, 20, 585–591. [Google Scholar] [CrossRef]
- Kana, M.A.; Usman, B.; Mohammed-Durosinlorun, A.; Ahmed, J.; Abubakar, H.H.; Abdulmalik, Y.; Pradella, F. Ramadan during Pregnancy and the Role of Dietary Intake for Neonatal Health in Kaduna, Northwestern Nigeria: A Cross-Sectional Study. BMC Pregnancy Childbirth 2025, 25, 59. [Google Scholar] [CrossRef]
- Satkunanathan, P.; Allard, C.; Doyon, M.; Perron, P.; Bouchard, L.; Hivert, M.F.; Peters, T.M. Physical Behaviours during Pregnancy May Alter the Association of Maternal Insulin Sensitivity with Neonatal Adiposity: A Prospective Pre-Birth Cohort of Mother-Child Pairs. BMC Pregnancy Childbirth 2025, 25, 41. [Google Scholar] [CrossRef]
- Adeoye, I.A.; Fakorede, J.I.; Salawu, M.M.; Adediran, K.I. Associations of Macrosomia with Sociodemographic, Anthropometric, Lifestyle Factors and Perinatal Outcomes in Southwest Nigeria. BMC Pediatr. 2025, 25, 61. [Google Scholar] [CrossRef]
- Kaur, S.; Bustami, N.A.; Masaki, T.; Shukri, N.H.M.; Shafie, S.R.; Shibata, S.; Teoh, A.N. Maternal Circadian Rhythm and Its Association with Meal Timing and Density: A Prospective Cohort Study. Curr. Dev. Nutr. 2022, 6, 124. [Google Scholar] [CrossRef]
- Loy, S.L.; Wee, P.H.; Colega, M.T.; Cheung, Y.B.; Aris, I.M.; Chan, J.K.Y.; Godfrey, K.M.; Gluckman, P.D.; Tan, K.H.; Shek, L.P.C.; et al. Maternal Night-Fasting Interval During Pregnancy Is Directly Associated with Neonatal Head Circumference and Adiposity in Girls but Not Boys. J. Nutr. 2017, 147, 1384–1391. [Google Scholar] [CrossRef]
- Chen, Y.E.; Loy, S.L.; Chen, L.W. Chrononutrition during Pregnancy and Its Association with Maternal and Offspring Outcomes: A Systematic Review and Meta-Analysis of Ramadan and Non-Ramadan Studies. Nutrients 2023, 15, 756. [Google Scholar] [CrossRef]
- Varcoe, T.J.; Boden, M.J.; Voultsios, A.; Salkeld, M.D.; Rattanatray, L.; Kennaway, D.J. Characterisation of the Maternal Response to Chronic Phase Shifts During Gestation in the Rat: Implications for Fetal Metabolic Programming. PLoS ONE 2013, 8, e53800. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.; Moore, R.Y. Development of a Fetal Circadian Rhythm After Disruption of the Maternal Circadian System. Dev. Brain Res. 1988, 41, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Meng, X.; Cui, L.; Wang, S. Circadian Regulation of Lipid Metabolism During Pregnancy. Int. J. Mol. Sci. 2024, 25, 11491. [Google Scholar] [CrossRef] [PubMed]
- Melnikova, V.; Lifantseva, N.; Voronova, S.; Bondarenko, N. Prenatal Stress Modulates Placental and Fetal Serotonin Levels and Determines Behavior Patterns in Offspring of Mice. Int. J. Mol. Sci. 2024, 25, 13565. [Google Scholar] [CrossRef]
- Liu, S.; Hua, L.; Mo, X.; Lei, B.; Zhang, R.; Zhou, S.; Jiang, X.; Fang, Z.; Feng, B.; Che, L.; et al. Comparative Impact of Alternate-Day Fasting and Time-Restricted Feeding on Placental Function and Fetal Development in Maternal Obesity. Nutrients 2025, 17, 25. [Google Scholar] [CrossRef]
- Kaur, S.; Teoh, A.N.; Shukri, N.H.M.; Shafie, S.R.; Bustami, N.A.; Takahashi, M.; Lim, P.J.; Shibata, S. Circadian Rhythm and Its Association with Birth and Infant Outcomes: Research Protocol of a Prospective Cohort Study. BMC Pregnancy Childbirth 2020, 20, 96. [Google Scholar] [CrossRef]
- Smith, H.A.; Betts, J.A. Circadian Rhythms, Feeding Patterns and Metabolic Regulation: Implications for Critical Care. Proc. Nutr. Soc. 2024, 1–5. [Google Scholar] [CrossRef]
- Chan, H.K.C. Circadian Rhythms and Memory: Exploring the Mechanisms of Synaptic Plasticity, Hormonal Modulation, and Cognitive Function. Theor. Nat. Sci. 2025, 77, 98–106. [Google Scholar] [CrossRef]
- Laulhe, M.; Martinerie, L.; Carel, J.-C. Getting in Sync: When Do Babies’ Cortisol Rhythms Start to Tick. J. Clin. Endocrinol. Metab. 2025, dgaf003. [Google Scholar] [CrossRef]
- Kentistou, K.A.; Lim, B.E.M.; Kaisinger, L.R.; Steinthorsdottir, V.; Sharp, L.N.; Patel, K.A.; Tragante, V.; Hawkes, G.; Gardner, E.J.; Olafsdottir, T.; et al. Rare Variant Associations with Birth Weight Identify Genes Involved in Adipose Tissue Regulation, Placental Function and Insulin-like Growth Factor Signalling. Nat. Commun. 2025, 16, 648. [Google Scholar] [CrossRef] [PubMed]
- Khant Aung, Z.; Grattan, D.R.; Ladyman, S.R. Pregnancy-Induced Adaptation of Central Sensitivity to Leptin and Insulin. Mol. Cell. Endocrinol. 2020, 516, 110933. [Google Scholar] [CrossRef] [PubMed]
- Jansson, N.; Greenwood, S.L.; Johansson, B.R.; Powell, T.L.; Jansson, T. Leptin Stimulates the Activity of the System A Amino Acid Transporter in Human Placental Villous Fragments. J. Clin. Endocrinol. Metab. 2003, 88, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Lazreg, T.B.; Zaouali, M.; Chaieb, M.; Dallel, N.; Chaieb, L.; Tabka, Z.; Zbidi, A. Circadian Leptin, Insulin and Cortisol Rhythms in Obese Subjects. Biol. Rhythm Res. 2007, 38, 9–17. [Google Scholar] [CrossRef]
- Guadix, P.; Corrales, I.; Vilariño-García, T.; Rodríguez-Chacón, C.; Sánchez-Jiménez, F.; Jiménez-Cortegana, C.; Dueñas, J.L.; Sánchez-Margalet, V.; Pérez-Pérez, A. Expression of Nutrient Transporters in Placentas Affected by Gestational Diabetes: Role of Leptin. Front. Endocrinol. 2023, 14, 1172831. [Google Scholar] [CrossRef]
- Alves-Santos, N.H.; Cocate, P.G.; Benaim, C.; Farias, D.R.; Emmett, P.M.; Kac, G. Prepregnancy Dietary Patterns and Their Association with Perinatal Outcomes: A Prospective Cohort Study. J. Acad. Nutr. Diet. 2019, 119, 1439–1451. [Google Scholar] [CrossRef]
- Loy, S.L.; Cheung, Y.B.; Cai, S.; Colega, M.T.; Godfrey, K.M.; Chong, Y.S.; Shek, L.P.C.; Tan, K.H.; Chong, M.F.F.; Yap, F.; et al. Maternal Night-Time Eating and Sleep Duration in Relation to Length of Gestation and Preterm Birth. Clin. Nutr. 2020, 39, 1935–1942. [Google Scholar] [CrossRef]
- Ganpule-Rao, A.V.; Roy, D.; Karandikar, B.A.; Yajnik, C.S.; Rush, E.C. Food Access and Nutritional Status of Rural Adolescents in India: Pune Maternal Nutrition Study. Am. J. Prev. Med. 2020, 58, 728–735. [Google Scholar] [CrossRef]
- Li, T.; He, Y.; Wang, N.; Feng, C.; Zhou, P.; Qi, Y.; Wang, Z.; Lin, X.; Mao, D.; Sun, Z.; et al. Maternal Dietary Patterns during Pregnancy and Birth Weight: A Prospective Cohort Study. Nutr. J. 2024, 23, 100. [Google Scholar] [CrossRef]
- Javadi, M.; Saffari, F.; Amerzadeh, M.; Rafiei, S. Maternal Dietary Diversity and Its Association with Infant Birth Weight: A Healthcare Centre Based Cross-Sectional Study. Discov. Public Health 2024, 21, 27. [Google Scholar] [CrossRef]
- Wibowo, N.; Irwinda, R.; Rachman, L. First Trimester Maternal Upper Arm Circumference Correlated to Placental Size and Neonatal Anthropometry. Med. J. Indones. 2020, 29, 38–41. [Google Scholar] [CrossRef]
- Tosson, A.M.S.; Sherif, I.K.; Sharaf, M.F.; Elmazzahy, E.A. Neonatal Anthropometric Measurements and Its Relation to Maternal Anthropometry and Demographics. Egypt. Pediatr. Assoc. Gaz. 2023, 71, 43. [Google Scholar] [CrossRef]
- Ramos, S.Z.; Rosenthal, A.; Panton, C.; Gimovsky, A.C. Neonatal Outcomes in Fetal Growth Restriction Diagnosed Using Estimated Fetal Weight versus Abdominal Circumference. Am. J. Obstet. Gynecol. 2022, 226, S252. [Google Scholar] [CrossRef]
- Mantel, Ä.; Hirschberg, A.L.; Stephansson, O. Association of Maternal Eating Disorders with Pregnancy and Neonatal Outcomes. JAMA Psychiatry 2020, 77, 285–293. [Google Scholar] [CrossRef]
- Yisahak, S.F.; Mumford, S.L.; Grewal, J.; Li, M.; Zhang, C.; Grantz, K.L.; Hinkle, S.N. Maternal Diet Patterns During Early Pregnancy in Relation to Neonatal Outcomes. Am. J. Clin. Nutr. 2021, 114, 358–367. [Google Scholar] [CrossRef]
- Puche-Juarez, M.; Toledano, J.M.; Hinojosa-Nogueira, D.; de Paco Matallana, C.; Sánchez-Romero, J.; Ochoa, J.J.; Carrillo, M.P.; Martín-Álvarez, E.; Diaz-Castro, J.; Moreno-Fernandez, J. Diet, Advanced Maternal Age, and Neonatal Outcomes: Results from the GESTAGE Study. Nutrients 2025, 17, 321. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 15. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45 (Suppl. 1), S232–S243. [Google Scholar] [CrossRef] [PubMed]
- Suciu, N.; Brătilă, E. (Eds.) Hipertensiunea Asociată Sarcinii; Societatea de Obstetrică şi Ginecologie din România și Colegiul Medicilor din România: Bucharest, Romania, 2019; Available online: https://sogr.ro/wp-content/uploads/2019/05/12.-Hipertensiunea-asociată-sarcinii.pdf (accessed on 17 June 2025).
- World Health Organization (WHO). Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-MNM-11.1 (accessed on 3 December 2022).
- Rasmussen, K.; Yaktine, A.; Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight. Weight Gain During Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- World Health Organization (WHO). A Healthy Lifestyle—WHO Recommendations. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 3 December 2022).
- Ministerul Muncii și Solidarității Sociale. Salariul de Bază Minim Brut pe Ţară Garantat în Plată se Majorează la 4.050 lei Lunar Începând cu 1 Ianuarie 2025. Comunicate de Presă. Available online: https://mmuncii.ro/j33/index.php/ro/comunicare/comunicate-de-presa/7516-20241127-cp-salariu-minim-ianuarie-2025 (accessed on 17 June 2025).
- Pregnancy and Diet—BDA. Available online: https://www.bda.uk.com/resource/pregnancy-diet.html (accessed on 17 July 2025).
- Institutul Național de Sănătate Publică și Centrul Național de Studii pentru Medicina Familiei. Probleme de Nutritie, Crestere si Dezvoltare la Copil: Alimentatia 0-2 Ani, Tulburarile de Crestere si Dezvoltare; Ghid de preventie; Institutul Național de Sănătate Publică și Centrul Național de Studii pentru Medicina Familiei: Bucharest, Romania, 2023; Volume 6. [Google Scholar]
- Englund-Ögge, L.; Birgisdottir, B.E.; Sengpiel, V.; Brantsæter, A.L.; Haugen, M.; Myhre, R.; Meltzer, H.M.; Jacobsson, B. Meal Frequency Patterns and Glycemic Properties of Maternal Diet in Relation to Preterm Delivery: Results from a Large Prospective Cohort Study. PLoS ONE 2017, 12, e172896. [Google Scholar] [CrossRef]
- Salunkhe, A.; Mohite, V.; Hiremath, P.; Salunkhe, J. Frequency and Nutrient Content of Meals of the Mothers and the Birth Weight and Gestational Age of the Baby. J. Krishna Inst. Med. Sci. 2018, 7, 33–41. [Google Scholar]
- Ainscough, K.M.; Kennelly, M.A.; Lindsay, K.L.; O’Brien, E.C.; O’Sullivan, E.J.; Mehegan, J.; Gibney, E.R.; McAuliffe, F.M. An Observational Analysis of Meal Patterns in Overweight and Obese Pregnancy: Exploring Meal Pattern Behaviours and the Association with Maternal and Fetal Health Measures. Ir. J. Med. Sci. 2020, 189, 585–594. [Google Scholar] [CrossRef]
- Yakar, S.; Werner, H.; Rosen, C.J. 40 YEARS OF IGF1: Insulin-like Growth Factors: Actions on the Skeleton. J. Mol. Endocrinol. 2018, 61, T115–T137. [Google Scholar] [CrossRef]
- Mazurkiewicz, D.; Bronkowska, M. Circulating Insulin and Igf-1 and Frequency of Food Consumption during Pregnancy as Predictors of Birth Weight and Length. Nutrients 2021, 13, 2344. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, E.; Oikonomou, C.; Nychas, G.; Dimitriadis, G.D. Effects of Diet, Lifestyle, Chrononutrition and Alternative Dietary Interventions on Postprandial Glycemia and Insulin Resistance. Nutrients 2022, 14, 823. [Google Scholar] [CrossRef] [PubMed]
- Miele, M.J.; Souza, R.T.; Calderon, I.M.; Feitosa, F.E.; Leite, D.F.; Rocha Filho, E.A.; Vettorazzi, J.; Mayrink, J.; Fernandes, K.G.; Vieira, M.C.; et al. Head Circumference as an Epigenetic Risk Factor for Maternal Nutrition. Front. Nutr. 2022, 9, 867727. [Google Scholar] [CrossRef] [PubMed]
- da Mota Santana, J.; de Oliveira Queiroz, V.A.; Pereira, M.; Paixão, E.S.; Brito, S.M.; dos Santos, D.B.; Oliveira, A.M. Associations between Maternal Dietary Patterns and Infant Birth Weight in the NISAMI Cohort: A Structural Equation Modeling Analysis. Nutrients 2021, 13, 4054. [Google Scholar] [CrossRef]
- Dieberger, A.M.; van Poppel, M.N.M.; Desoye, G.; Simmons, D.; Harreiter, J.; Devlieger, R.; Medina, C.; Lawlor, D.A.; Elhakeem, A.; Desoye, G.; et al. Effect of a Physical Activity and Healthy Eating Lifestyle Intervention in Pregnancy on Fetal Growth Trajectories: The DALI Randomised Controlled Trial. Pediatr. Obes. 2025, 20, e13199. [Google Scholar] [CrossRef]
- Siargkas, A.; Tranidou, A.; Magriplis, E.; Tsakiridis, I.; Apostolopoulou, A.; Xenidis, T.; Pazaras, N.; Chourdakis, M.; Dagklis, T. Impact of Maternal Macronutrient Intake on Large for Gestational Age Neonates’ Risk Among Women with Gestational Diabetes Mellitus: Results from the Greek BORN2020 Cohort. Nutrients 2025, 17, 269. [Google Scholar] [CrossRef]
- Kim, M.K.; Lee, S.M.; Bae, S.H.; Kim, H.J.; Lim, N.G.; Yoon, S.J.; Lee, J.Y.; Jo, M.-W. Socioeconomic Status Can Affect Pregnancy Outcomes and Complications, Even with a Universal Healthcare System. Int. J. Equity Health 2018, 17, 2. [Google Scholar] [CrossRef]
- Karcz, K.; Królak-Olejnik, B. Impact of Gestational Diabetes Mellitus on Fetal Growth and Nutritional Status in Newborns. Nutrients 2024, 16, 4093. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | n (%) | |
|---|---|---|
| Sociodemographic | ||
| Mother’s age (years) | 18–34 | 903 (88.1) |
| ≥35 | 122 (11.9) | |
| Place of residence | Rural | 503 (49.1) |
| Urban | 522 (50.9) | |
| Mother education | Low (≤8 years in school) | 158 (15.5) |
| Medium | 475 (46.3) | |
| University degree | 392 (38.2) | |
| Marital status | Married | 945 (92.2) |
| Single | 80 (7.8) | |
| Employment status of the mother | Housewife | 434 (42.3) |
| Employed | 591 (57.7) | |
| Household income/month (RON) | ≤4000 RON (low) | 661 (64) |
| >4000 RON (high) | 364 (36) | |
| Clinical | ||
| Anemia | No | 707 (69) |
| Yes | 318 (31) | |
| Hypertension | No | 1019 (99.4) |
| Yes | 6 (0.6) |
| Characteristics | n (%) | |
|---|---|---|
| Delivery mode | Vaginal | 534 (52.1) |
| Caesarean section | 491 (47.9) | |
| Parity | Primiparous | 371 (36.6) |
| Multiparous | 654 (63.4) | |
| Gestational week | Term | 844 (82.3) |
| Preterm (≤37 weeks’ gestation) | 181 (17.7) | |
| Prenatal weight (kg) | 65.0 (57.0–74.0) | |
| Maternal weight at admission (kg) | 78.0 (70.0–87.0) | |
| Gestational weight gain (kg) | 13.0 (9.0–16.0) | |
| Mother height (cm) | 1.65 (1.60–1.69) | |
| Pre-pregnancy BMI (kg/m2) | 23.7 (21.3–27.0) | |
| Pregestational BMI (kg/m2) | Underweight (<18.5) | 52 (5.1) |
| Normal weight (≥18.5 and <25.0) | 580 (56.6) | |
| Overweight (≥25.0 and <30.0) | 258 (25.2) | |
| Obese (≥30.0) | 135 (13.2) | |
| Sex | Male | 508 (49.6) |
| Female | 517 (50.4) | |
| Birth weight (g) | <2500 g | 107 (10.4) |
| 2500–4000 g | 918 (89.6) | |
| Birth weight (g) | 3270 (2900–3560) | |
| Birth height (cm) | 50 (48–51) | |
| Head circumference (cm) | 31 (31–33) | |
| Chest circumference (cm) | 33 (32–34) | |
| Abdominal circumference (cm) | 35 (34–36) | |
| Apgar score | 9 (8–9) |
| Meal Type | Median (IQR), Days/Week | % Women’s Daily Consumption (7/7 Days) |
|---|---|---|
| Breakfast | 4 (1–7) | 30.9 |
| Morning snack | 3 (1–6) | 19.7 |
| Lunch | 6 (3–7) | 47.2 |
| Afternoon snack | 4 (1–6) | 21.4 |
| Dinner | 6 (3–7) | 44.6 |
| Evening snack | 2 (0–4) | 12.8 |
| Night meal | 0 (0–2) | 5.6 |
| Meal Frequency Patterns | n (%) |
|---|---|
| Structured patterns | 201 (19.6) |
| 3 main meals and ≥2 snacks/day | 71 (6.9) |
| 3 main meals and 1 snack | 74 (7.2) |
| 3 main meals only | 56 (5.5) |
| Moderately irregular patterns | 422 (41.2) |
| 2 main meals and ≥2 snacks | 42 (4.1) |
| 2 main meals and 1 snack | 245 (23.9) |
| 2 main meals only | 135 (13.2) |
| Highly irregular patterns | 402 (39.2) |
| 1 main meal and snacks | 211 (20.6) |
| No main meals, only snacks | 191 (18.6) |
| Neonatal Outcomes | Maternal Meal Frequency Patterns | Kruskal–Wallis p-Value | ||
|---|---|---|---|---|
| Structured (n = 201) | Moderately Irregular (n = 422) | Highly Irregular (n = 402) | ||
| Birth weight (g) | 3150 (2765–3452.5) | 3300 (2950–3600) | 3280 (2900–3590) | 0.006 |
| Birth height (cm) | 49 (48–50) | 50 (49–51) | 50 (48–51) | <0.001 |
| Head circumference (cm) | 35 (34–35) | 35 (34–36) | 35 (34–36) | 0.03 |
| Chest circumference (cm) | 33 (31–34) | 33 (32–34) | 33 (32–34) | 0.008 |
| Abdominal circumference (cm) | 31 (29–32) | 32 (30–33) | 31 (30–33) | 0.05 |
| Apgar score | 8 (8–9) | 8 (8–9) | 8 (8–9) | 0.02 |
| Neonatal Outcomes | β (95% CI) Moderately Irregular vs. Highly Irregular | p-Value | β (95% CI) Structured vs. Highly Irregular | p-Value |
|---|---|---|---|---|
| Birth weight (g) | −16.47 (−67.44, 34.50) | 0.52 | −63.82 (−128.87, 1.23) | 0.05 |
| Birth height (cm) | 0.12 (−0.12, 0.36) | 0.32 | −0.36 (−0.68, −0.04) | 0.02 |
| Head circumference (cm) | 0.04 (−0.14, 0.21) | 0.69 | −0.05 (−0.28, 0.18) | 0.66 |
| Chest circumference (cm) | 0.01 (−0.21, 0.24) | 0.89 | −0.20 (−0.49, 0.09) | 0.18 |
| Abdominal circumference (cm) | −0.09 (−0.35, 0.17) | 0.50 | −0.07 (−0.39, 0.26) | 0.32 |
| Apgar score | 0.06 (−0.04, 0.17) | 0.26 | 0.08 (−0.07, 0.23) | 0.30 |
| Neonatal Outcomes | Interaction Term (Meal Patterns × Education/Income) | |||||||
|---|---|---|---|---|---|---|---|---|
| Structured Patterns × Education Level | Structured Patterns × Household Income | Moderately Irregular Patterns × Education Level | Moderately Irregular Patterns × Household Income | |||||
| β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Birth weight (g) | −9.08 (−74.42, 56.27) | 0.78 | −2.58 (−34.03, 28.88) | 0.87 | −32.86 (−89.27, 23.54) | 0.25 | 17.24 (−6.51, 40.99) | 0.15 |
| Birth height (cm) | 0.002 (−0.320, 0.324) | 0.98 | 0.015 (−0.140, 0.169) | 0.85 | −0.15 (−0.42, 0.11) | 0.25 | 0.05 (−0.06, 0.16) | 0.37 |
| Head circumference (cm) | −0.20 (−0.43, 0.02) | 0.08 | −0.03 (−0.14, 0.08) | 0.56 | −0.09 (−0.29, 0.09) | 0.33 | 0.05 (−0.02, 0.13) | 0.18 |
| Chest circumference (cm) | −0.01 (−0.30, 0.28) | 0.93 | 0.02 (−0.11, 0.16) | 0.71 | 0.15 (0.04, 0.25) | 0.003 | 0.06 (−0.17, 0.31) | 0.59 |
| Abdominal circumference (cm) | 0.11 (−0.21, 0.44) | 0.50 | 0.07 (−0.09, 0.22) | 0.39 | 0.05 (−0.23, 0.35) | 0.69 | 0.14 (0.02, 0.26) | 0.02 |
| Apgar score | −0.02 (−0.17, 0.11) | 0.69 | 0.01 (−0.05, 0.09) | 0.60 | 0.02 (−0.09, 0.14) | 0.66 | 0.03 (−0.01, 0.08) | 0.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atomei, O.L.; Vicoveanu, P.; Iațcu, C.O.; Gliga, F.I.; Craciun, C.C.; Tarcea, M. Associations Between Maternal Meal Frequency Patterns During Pregnancy and Neonatal Anthropometric Outcomes: A Quantitative Cross-Sectional Study. Nutrients 2025, 17, 2437. https://doi.org/10.3390/nu17152437
Atomei OL, Vicoveanu P, Iațcu CO, Gliga FI, Craciun CC, Tarcea M. Associations Between Maternal Meal Frequency Patterns During Pregnancy and Neonatal Anthropometric Outcomes: A Quantitative Cross-Sectional Study. Nutrients. 2025; 17(15):2437. https://doi.org/10.3390/nu17152437
Chicago/Turabian StyleAtomei, Oana Liliana, Petronela Vicoveanu, Camelia Oana Iațcu, Florina Ioana Gliga, Calin Coriolan Craciun, and Monica Tarcea. 2025. "Associations Between Maternal Meal Frequency Patterns During Pregnancy and Neonatal Anthropometric Outcomes: A Quantitative Cross-Sectional Study" Nutrients 17, no. 15: 2437. https://doi.org/10.3390/nu17152437
APA StyleAtomei, O. L., Vicoveanu, P., Iațcu, C. O., Gliga, F. I., Craciun, C. C., & Tarcea, M. (2025). Associations Between Maternal Meal Frequency Patterns During Pregnancy and Neonatal Anthropometric Outcomes: A Quantitative Cross-Sectional Study. Nutrients, 17(15), 2437. https://doi.org/10.3390/nu17152437