
Association Between the Korean Healthy Eating Index (KHEI) and Healthcare Costs Among Adults: The Korea National Health and Nutrition Examination Survey (KNHANES) 2016 and 2021


Abstract
1. Introduction
2. Materials and Methods
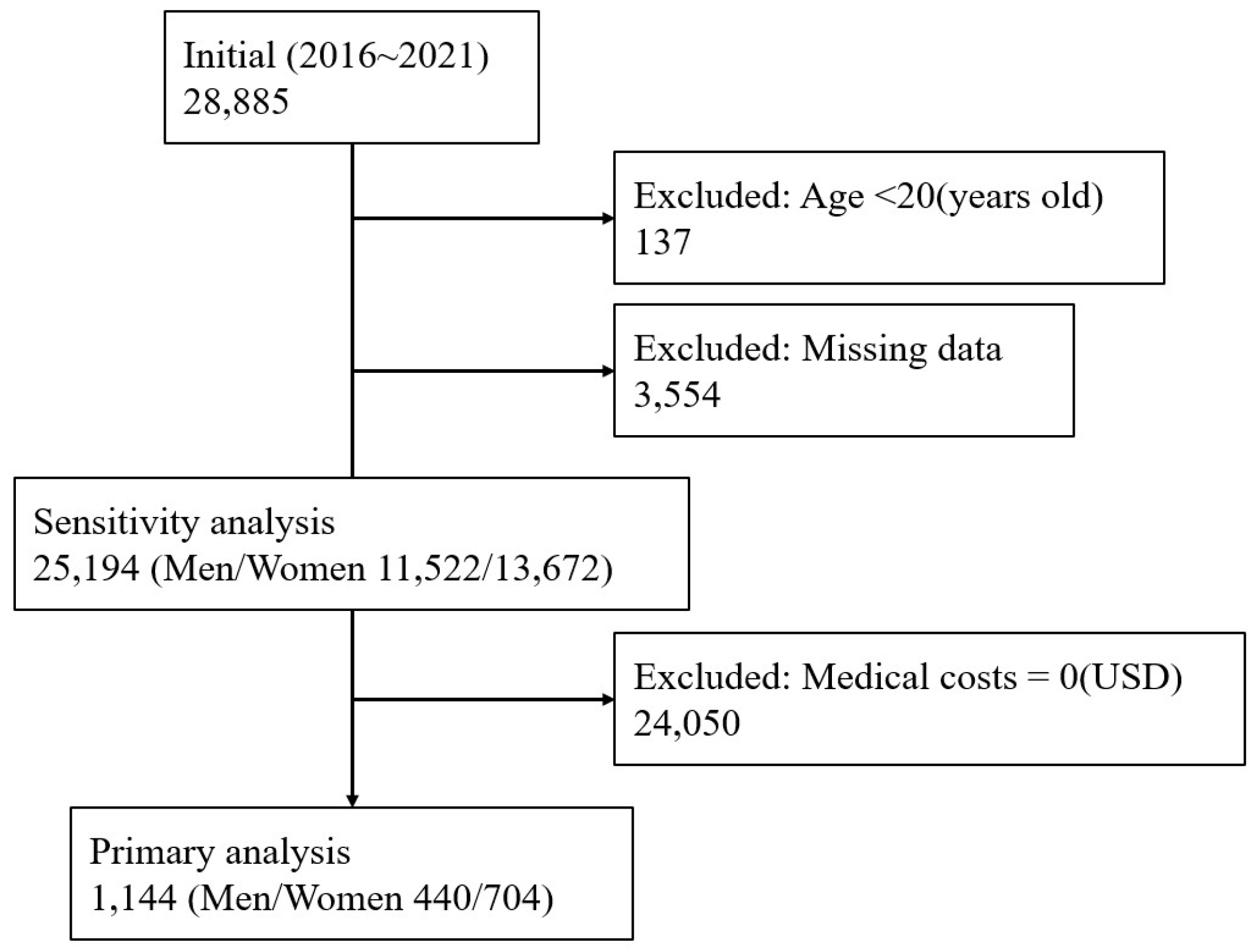
2.1. Study Design and Participants
2.2. Dietary Assessment and Korean Healthy Eating Index (KHEI)
2.3. Assessment of Healthcare Costs
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Populations
3.2. Comparison of Clinical Characteristics and Medical Costs According to KHEI Quartiles
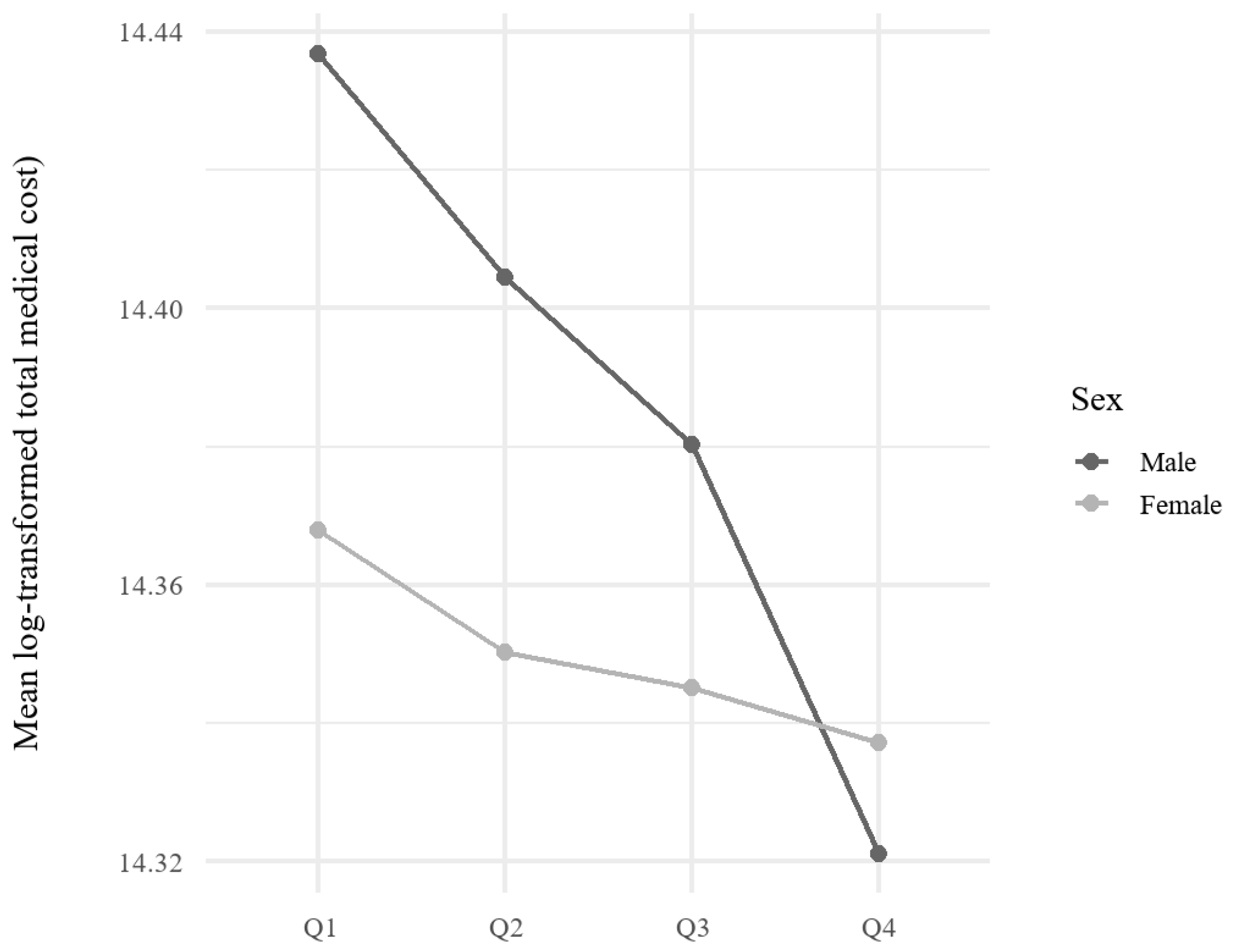
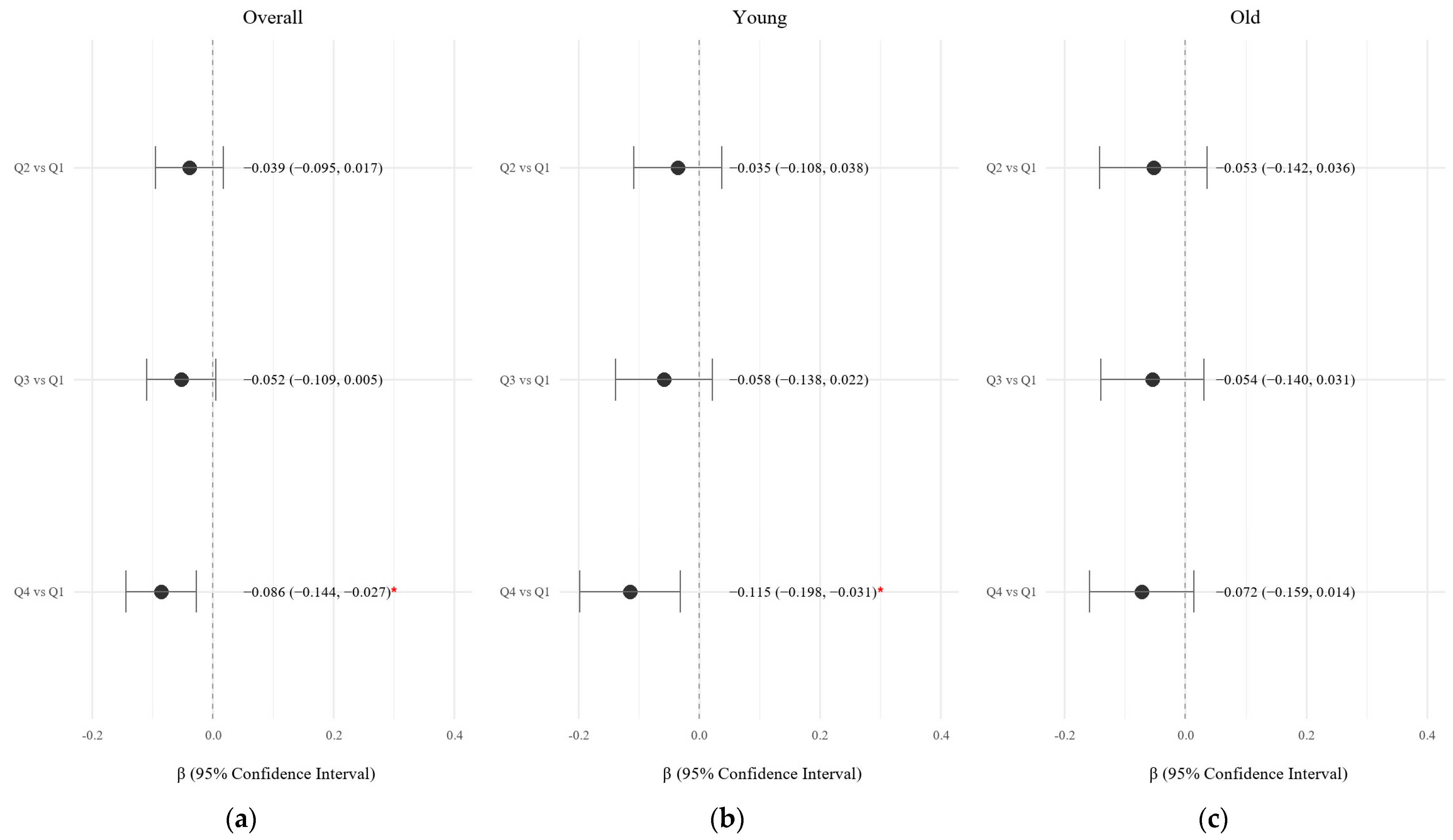
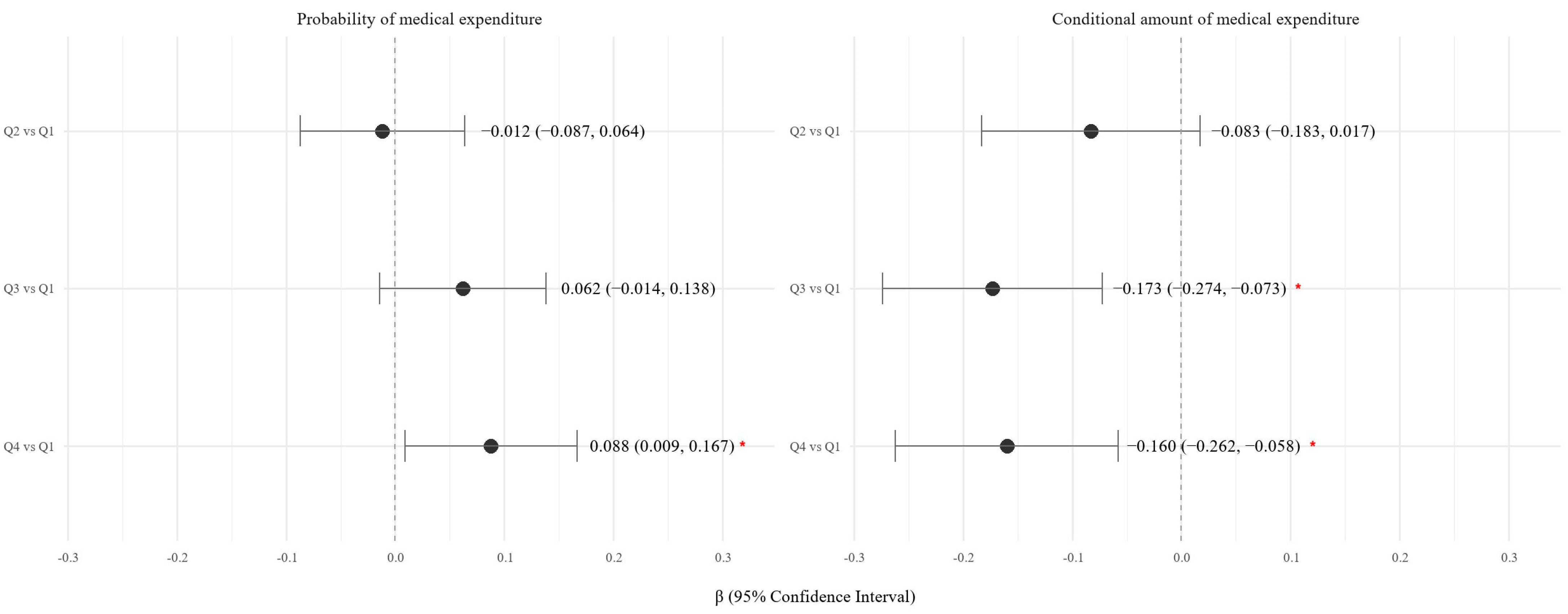
3.3. Association Between KHEI and Medical Costs
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| KHEI | Korean Healthy Eating Index |
References
- Berkowitz, S.A.; Seligman, H.K.; Meigs, J.B.; Basu, S. Food insecurity, healthcare utilization, and high cost: A longitudinal cohort study. Am. J. Manag. Care 2018, 24, 399–404. [Google Scholar] [PubMed]
- Patterson, A.; Hure, A.; Burrows, T.; Jackson, J.; Collins, C. Diet quality and 10-year healthcare costs by BMI categories in the mid-age cohort of the Australian Longitudinal Study on Women’s Health. J. Hum. Nutr. Diet. 2018, 31, 463–472. [Google Scholar] [CrossRef]
- Yun, S.; Park, S.; Yook, S.-M.; Kim, K.; Shim, J.E.; Hwang, J.Y.; Oh, K. Development of the Korean Healthy Eating Index for adults, based on the Korea National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2022, 16, 233–247. [Google Scholar] [CrossRef] [PubMed]
- EunJung, L.; Ji-Myung, K. The association of the Korean Healthy Eating Index with chronic conditions in middle-aged single-person households. Nutr. Res. Pract. 2023, 17, 316–329. [Google Scholar]
- Bae, Y.-J.; Yu, K.-W.; Lee, K.-H.; Jang, K.-I. Association of the Healthy Eating Index with Metabolic Abnormalities among Middle-Aged Adults Living in Single-Person Households in Korea. Nutrients 2021, 13, 3937. [Google Scholar] [CrossRef] [PubMed]
- Jo, G.; Park, D.; Lee, J.; Kim, R.; Subramanian, S.V.; Oh, H.; Shin, M.J. Trends in Diet Quality and Cardiometabolic Risk Factors among Korean Adults, 2007–2018. JAMA Netw. Open 2022, 5, e2218297. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Park, S. Regional differences in the associations of diet quality, obesity, and possible sarcopenia using the seventh Korea National Health and Nutrition Examination Survey (2016–2018). Epidemiol. Health 2023, 45, e2023059. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Kang, D.T. 2021 National Health Insurance Statistical Yearbook. National Health Insurance Service; Health Insurance Review & Assessment Service, Wonju, Korea. 2023. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAJ030000007001&brdScnBltNo=4&brdBltNo=6&pageIndex=1&pageIndex2=1#none (accessed on 10 June 2025).
- Kollerup, A.; Kjellberg, J.; Ibsen, R. Ageing and health care expenditures: The importance of age per se, steepening of the individual-level expenditure curve, and the role of morbidity. Eur. J. Health Econ. 2022, 23, 1121–1149. [Google Scholar] [CrossRef] [PubMed]
- Azzani, M.; Roslani, A.C.; Su, T.T. Determinants of Household Catastrophic Health Expenditure: A Systematic Review. Malays. J. Med. Sci. 2019, 26, 15–43. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.G.; Williamson, D.F.; Glick, H.A. Direct medical cost of overweight and obesity in the USA: A quantitative systematic review. Obes. Rev. 2011, 12, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y. The effects of smoking, alcohol consumption, obesity, and physical inactivity on healthcare costs: A longitudinal cohort study. BMC Public Health 2025, 25, 873. [Google Scholar] [CrossRef] [PubMed]
- Duan, N.; Manning, W.G.; Morris, C.N.; Newhouse, J.P. A Comparison of Alternative Models for the Demand for Medical Care. J. Bus. Econ. Stat. 1983, 1, 115–126. [Google Scholar] [CrossRef]
- Kim, J.H.; Jun, S.; Kim, J. Dietary intake and cancer incidence in Korean adults: A systematic review and meta-analysis of observational studies. Epidemiol. Health 2023, 45, e2023102-30. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Jo, G.; Kim, O.Y.; Lim, H.; Song, S.; Choi, J.H.; Bae, J.H.; Jin, E.S.; Kim, R.; Lee, Y.; et al. Fact sheet: Nationwide trends in dietary intakes among Korean adults, 2013–2022. Korean J. Intern. Med. 2025, 40, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Kang, M.; Lim, H. Age-specific association between meal-skipping patterns and the risk of hyperglycemia in Korean adults: A national cross-sectional study using the KNHANES data. BMC Public Health 2024, 24, 1697. [Google Scholar] [CrossRef] [PubMed]
- Jee-seon, S.; Kyoung Hwa, H.; Dae Jung, K.; Hyeon Chang, K. Ultra-Processed Food Consumption and Obesity in Korean Adults. Diabetes Metab. J. (DMJ) 2023, 47, 547. [Google Scholar]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Sisto, A.; Marzetti, E. Anorexia of Aging: Risk Factors, Consequences, and Potential Treatments. Nutrients 2016, 8, 69. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Unweighted (N = 1144) |
|---|---|
| Continuous variabales, Median [IQR] | |
| Age | 57.00 [42.00, 68.00] |
| BMI | 24.18 [21.96, 26.29] |
| Number of Chronic diseases | 1.00 [0.00, 2.00] |
| Medical costs ($) | |
| Inpatient costs | 1295.84 [1193.10, 1393.09] |
| Outpatient costs | 41.65 [22.87, 62.47] |
| Total medical costs | 1320.03 [1231.46, 1448.37] |
| Categorical variables, N (%) | |
| Sex | |
| Male | 440 (38.5) |
| Female | 704 (61.5) |
| Income | |
| Low | 469 (41.0) |
| High | 675 (59.0) |
| Education | |
| Low | 462 (40.4) |
| High | 682 (59.6) |
| Smoking | |
| Never | 671 (58.7) |
| Ever | 473 (41.3) |
| Alcohol drinking | |
| Never | 361 (31.6) |
| Ever | 783 (68.4) |
| Korean Healthy Eating Index | |||||
|---|---|---|---|---|---|
| Q1 [18.14–53.55] | Q2 [53.55–63.09] | Q3 [63.09–72.12] | Q4 [72.12–98.20] | p-value | |
| Unweighted N | 272 | 290 | 292 | 290 | |
| Continuous variables, Median [IQR] | |||||
| Age | 47.00 [34.00, 61.00] | 56.00 [39.00, 69.00] | 60.00 [47.00, 71.00] | 61.00 [50.00, 69.00] | <0.001 * |
| BMI | 24.24 [21.81, 26.60] | 24.14 [21.76, 26.51] | 24.37 [22.56, 26.25] | 23.83 [21.70, 26.05] | 0.287 |
| Number of Chronic diseases | 0.00 [0.00, 2.00] | 1.00 [0.00, 2.00] | 1.00 [0.00, 2.00] | 1.00 [0.00, 2.00] | <0.001 * |
| Medical costs ($) | |||||
| Inpatient costs | 1295.84 [1209.77, 1393.09] | 1295.84 [1193.10, 1393.09] | 1295.84 [1193.10, 1393.09] | 1209.77 [1193.10, 1322.09] | 0.007 * |
| Outpatient costs | 27.64 [22.87, 62.47] | 41.65 [24.19, 62.47] | 41.65 [24.19, 65.08] | 27.64 [22.87, 51.44] | 0.395 |
| Total medical costs | 1347.81 [1248.97, 1746.41] | 1344.23 [1234.74, 1448.37] | 1320.03 [1234.74, 1441.50] | 1319.13 [1231.46, 1420.73] | 0.005 * |
| Categorical variables, N (%) | |||||
| Sex | 0.003 * | ||||
| Male | 106 (39.0) | 111 (38.3) | 134 (45.9) | 89 (30.7) | |
| Female | 166 (61.0) | 179 (61.7) | 158 (54.1) | 201 (69.3) | |
| Income | 0.004 * | ||||
| Low | 124 (45.6) | 136 (46.9) | 109 (37.3) | 100 (34.5) | |
| High | 148 (54.4) | 154 (53.1) | 183 (62.7) | 190 (65.5) | |
| Education | <0.001 * | ||||
| Low | 81 (29.8) | 118 (40.7) | 132 (45.2) | 131 (45.2) | |
| High | 191 (70.2) | 172 (59.3) | 160 (54.8) | 159 (54.8) | |
| Smoking | <0.001 * | ||||
| Never | 136 (50.0) | 162 (55.9) | 161 (55.1) | 212 (73.1) | |
| Ever | 136 (50.0) | 128 (44.1) | 131 (44.9) | 78 (26.9) | |
| Alcohol Drinking | 0.062 | ||||
| Never | 69 (25.4) | 91 (31.4) | 99 (33.9) | 102 (35.2) | |
| Ever | 203 (74.6) | 199 (68.6) | 193 (66.1) | 188 (64.8) | |
| Inpatient Costs | Outpatient Costs | Total Medical Costs | |||
|---|---|---|---|---|---|
| Comparison | p-Value | Comparison | p-Value | Comparison | p-Value |
| Q1–Q2 | 1.000 | Q1–Q2 | 1.000 | Q1–Q2 | 0.896 |
| Q1–Q3 | 0338 | Q1–Q3 | 1.000 | Q1–Q3 | 0.507 |
| Q1–Q4 | 0.004 * | Q1–Q4 | 1.000 | Q1–Q4 | 0.002 * |
| Q2–Q3 | 1.000 | Q2–Q3 | 1.000 | Q2–Q3 | 1.000 |
| Q2–Q4 | 0.172 | Q2–Q4 | 0.986 | Q2–Q4 | 0.186 |
| Q3–Q4 | 0.746 | Q3–Q4 | 0.710 | Q3–Q4 | 0.364 |
| KHEI Quartiles (vs. Q1) | β (Estimate) | 95% CI | p-Value |
|---|---|---|---|
| Inpatient Costs | |||
| Q2 | −0.033 | (−0.090, 0.024) | 0.257 |
| Q3 | −0.050 | (−0.108, 0.009) | 0.100 |
| Q4 | −0.080 | (−0.139, −0.020) | 0.009 * |
| Outpatient costs | |||
| Q2 | −0.028 | (−0.141, 0.085) | 0.626 |
| Q3 | −0.028 | (−0.143, 0.088) | 0.636 |
| Q4 | −0.121 | (−0.238, −0.003) | 0.045 * |
| Total medical costs | |||
| Q2 | −0.039 | (−0.095, 0.017) | 0.175 |
| Q3 | −0.052 | (−0.109, 0.005) | 0.073 |
| Q4 | −0.086 | (−0.144, −0.027) | 0.004 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Park, M. Association Between the Korean Healthy Eating Index (KHEI) and Healthcare Costs Among Adults: The Korea National Health and Nutrition Examination Survey (KNHANES) 2016 and 2021. Nutrients 2025, 17, 2237. https://doi.org/10.3390/nu17132237
Kim S, Park M. Association Between the Korean Healthy Eating Index (KHEI) and Healthcare Costs Among Adults: The Korea National Health and Nutrition Examination Survey (KNHANES) 2016 and 2021. Nutrients. 2025; 17(13):2237. https://doi.org/10.3390/nu17132237
Chicago/Turabian StyleKim, Soyoung, and Minseon Park. 2025. "Association Between the Korean Healthy Eating Index (KHEI) and Healthcare Costs Among Adults: The Korea National Health and Nutrition Examination Survey (KNHANES) 2016 and 2021" Nutrients 17, no. 13: 2237. https://doi.org/10.3390/nu17132237
APA StyleKim, S., & Park, M. (2025). Association Between the Korean Healthy Eating Index (KHEI) and Healthcare Costs Among Adults: The Korea National Health and Nutrition Examination Survey (KNHANES) 2016 and 2021. Nutrients, 17(13), 2237. https://doi.org/10.3390/nu17132237