
Benefits of Short-Term (4-Week) Daily Walnut Consumption in Middle-Aged Adults at Risk for Metabolic Syndrome: Outcomes of a Randomized Controlled Trial

 ,
,  , ,
, ,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
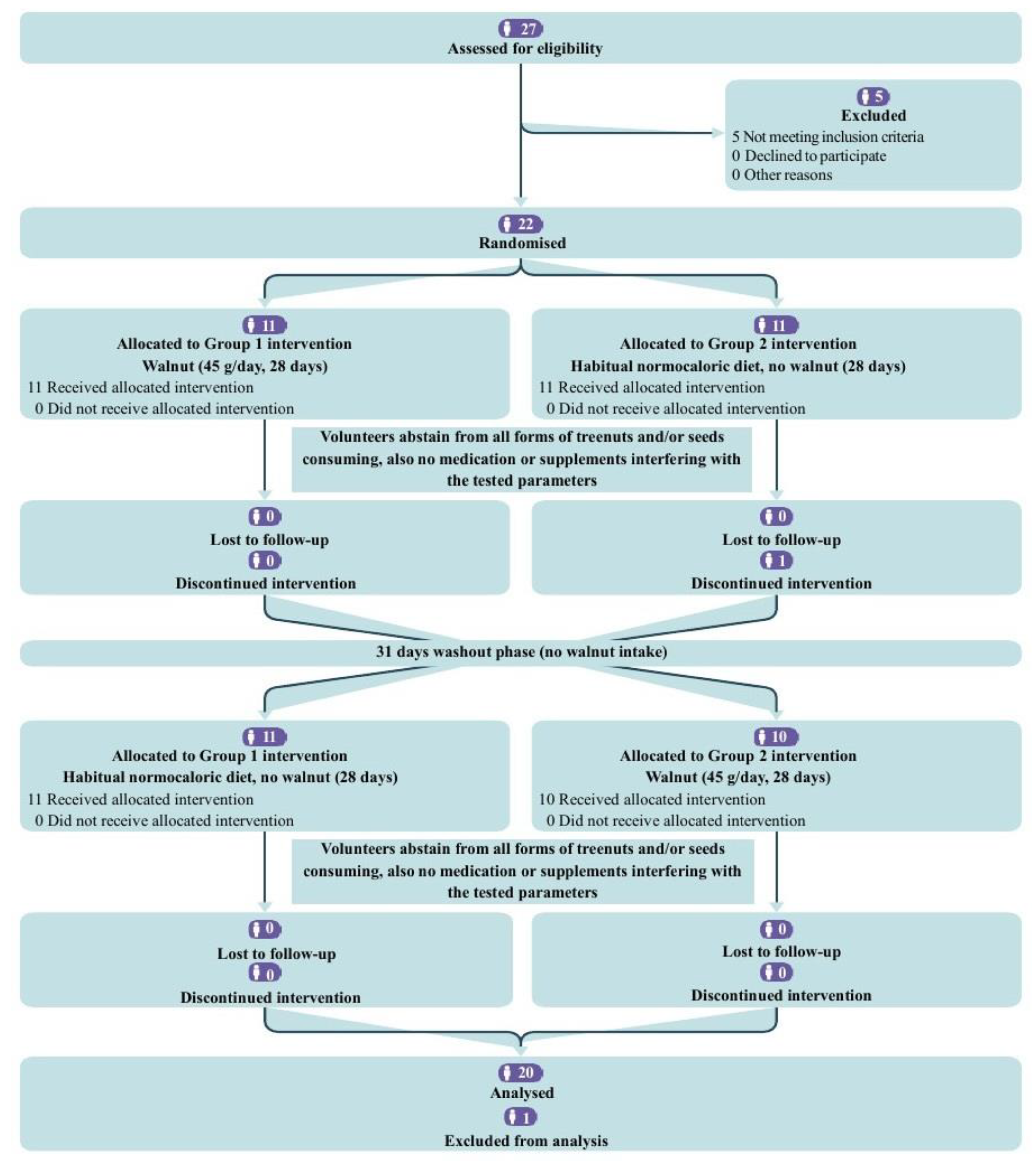
2.1. Study Design
2.2. Participants
2.3. Interventions
2.4. Randomization and Blinding
2.5. Data Collection and Outcome Measures
2.5.1. Anthropometric Measurements
2.5.2. sVCAM-1 Assessment
2.5.3. Cardiometabolic Parameters
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Baseline Characteristics
3.2. Nutrient Profile
3.3. Study Outcomes
4. Discussion
4.1. Anthropometric Profile
4.2. sVCAM-1
4.3. Blood Pressure
4.4. Lipid Profile
4.5. Glycemic Profile
5. Strengths, Limitations, and Future Prospects
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ambroselli, D.; Masciulli, F.; Romano, E.; Catanzaro, G.; Besharat, Z.M.; Massari, M.C.; Ferretti, E.; Migliaccio, S.; Izzo, L.; Ritieni, A.; et al. New Advances in Metabolic Syndrome, from Prevention to Treatment: The Role of Diet and Food. Nutrients 2023, 15, 640. [Google Scholar] [CrossRef]
- Di Cesare, M.; McGhie, D.V.; Perel, P.; Mwangi, J.; Taylor, S.; Pervan, B.; Kabudula, C.; Narula, J.; Bixby, H.; Pineiro, D.; et al. The Heart of the World. Glob. Heart 2024, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Fahed, G.; Aoun, L.; Zerdan, M.B.; Allam, S.; Zerdan, M.B.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics-2016 Update A Report from the American Heart Association. Circulation 2015, 133, 38–360. [Google Scholar] [CrossRef]
- Zhu, Y.; Bing, J.; Zheng, L.; Hao, P.; Teng, X.; Wan, L. The Association between Composite Dietary Antioxidant Index and the Metabolic Syndrome: NHANES 2007–2018. J. Funct. Foods 2024, 116, 106200. [Google Scholar] [CrossRef]
- Varona, J.F.; Ortiz-Regalón, R.; Sánchez-Vera, I.; López-Melgar, B.; García-Durango, C.; Castellano Vázquez, J.M.; Solís, J.; Fernández-Friera, L.; Vidal-Vanaclocha, F. Soluble ICAM 1 and VCAM 1 Blood Levels Alert on Subclinical Atherosclerosis in Non Smokers with Asymptomatic Metabolic Syndrome. Arch. Med. Res. 2019, 50, 20–28. [Google Scholar] [CrossRef]
- Troncoso, M.F.; Ortiz-Quintero, J.; Garrido-Moreno, V.; Sanhueza-Olivares, F.; Guerrero-Moncayo, A.; Chiong, M.; Castro, P.F.; García, L.; Gabrielli, L.; Corbalán, R.; et al. VCAM-1 as a Predictor Biomarker in Cardiovascular Disease. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166170. [Google Scholar] [CrossRef]
- Bhardwaj, R.; Dod, H.; Sandhu, M.S.; Bedi, R.; Dod, S.; Konat, G.; Chopra, H.K.; Sharma, R.; Jain, A.C.; Nanda, N. Acute Effects of Diets Rich in Almonds and Walnuts on Endothelial Function. Indian Heart J. 2018, 70, 497–501. [Google Scholar] [CrossRef]
- Rizzoni, D.; Muiesan, M.L.; Porteri, E.; Castellano, M.; Salvetti, M.; Monteduro, C.; De Ciuceis, C.; Boari, G.; Valentini, U.; Cimino, A.; et al. Circulating Adhesion Molecules and Carotid Artery Structural Changes in Patients with Noninsulin-Dependent Diabetes Mellitus. J. Hum. Hypertens. 2003, 17, 463–470. [Google Scholar] [CrossRef]
- Abdrabalnabi, A.A.; Rajaram, S.; Bitok, E.; Oda, K.; Beeson, W.L.; Kaur, A.; Cofán, M.; Serra-Mir, M.; Roth, I.; Ros, E.; et al. Effects of Supplementing the Usual Diet with a Daily Dose of Walnuts for Two Years on Metabolic Syndrome and Its Components in an Elderly Cohort. Nutrients 2020, 12, 451. [Google Scholar] [CrossRef]
- Lopez-Neyman, S.M.; Zohoori, N.; Broughton, K.S.; Miketinas, D.C. Association of Tree Nut Consumption with Cardiovascular Disease and Cardiometabolic Risk Factors and Health Outcomes in US Adults: NHANES 2011–2018. Curr. Dev. Nutr. 2023, 7, 102007. [Google Scholar] [CrossRef] [PubMed]
- Rusu, M.E.; Gheldiu, A.M.; Mocan, A.; Vlase, L.; Popa, D.S. Anti-Aging Potential of Tree Nuts with a Focus on the Phytochemical Composition, Molecular Mechanisms and Thermal Stability of Major Bioactive Compounds. Food Funct. 2018, 9, 2554–2575. [Google Scholar] [CrossRef]
- Ni, Z.J.; Zhang, Y.G.; Chen, S.X.; Thakur, K.; Wang, S.; Zhang, J.G.; Shang, Y.F.; Wei, Z.J. Exploration of Walnut Components and Their Association with Health Effects. Crit. Rev. Food Sci. Nutr. 2022, 62, 5113–5129. [Google Scholar] [CrossRef]
- Fan, N.; Fusco, J.L.; Rosenberg, D.W. Antioxidant and Anti-Inflammatory Properties of Walnut Constituents: Focus on Personalized Cancer Prevention and the Microbiome. Antioxidants 2023, 12, 982. [Google Scholar] [CrossRef] [PubMed]
- Mateș, L.; Banc, R.; Zaharie, F.A.; Rusu, M.E.; Popa, D.-S. Mechanistic Insights into the Biological Effects and Antioxidant Activity of Walnut (Juglans regia L.) Ellagitannins: A Systematic Review. Antioxidants 2024, 13, 974. [Google Scholar] [CrossRef]
- Rusu, M.E.; Mocan, A.; Ferreira, I.C.F.R.; Popa, D.S. Health Benefits of Nut Consumption in Middle-Aged and Elderly Population. Antioxidants 2019, 8, 302. [Google Scholar] [CrossRef] [PubMed]
- Rudrapal, M.; Rakshit, G.; Singh, R.P.; Garse, S.; Khan, J.; Chakraborty, S. Dietary Polyphenols: Review on Chemistry/Sources, Bioavailability/Metabolism, Antioxidant Effects, and Their Role in Disease Management. Antioxidants 2024, 13, 429. [Google Scholar] [CrossRef] [PubMed]
- Canales, A.; Sánchez-Muniz, F.J.; Bastida, S.; Librelotto, J.; Nus, M.; Corella, D.; Guillen, M.; Benedi, J. Effect of Walnut-Enriched Meat on the Relationship between VCAM, ICAM, and LTB4 Levels and PON-1 Activity in ApoA4 360 and PON-1 Allele Carriers at Increased Cardiovascular Risk. Eur. J. Clin. Nutr. 2011, 65, 703–710. [Google Scholar] [CrossRef]
- Cofán, M.; Rajaram, S.; Sala-Vila, A.; Valls-Pedret, C.; Serra-Mir, M.; Roth, I.; Freitas-Simoes, T.M.; Bitok, E.; Sabaté, J.; Ros, E. Effects of 2-Year Walnut-Supplemented Diet on Inflammatory Biomarkers. J. Am. Coll. Cardiol. 2020, 76, 2282–2284. [Google Scholar] [CrossRef]
- Damasceno, N.R.T.; Pérez-Heras, A.; Serra, M.; Cofán, M.; Sala-Vila, A.; Salas-Salvadó, J.; Ros, E. Crossover Study of Diets Enriched with Virgin Olive Oil, Walnuts or Almonds. Effects on Lipids and Other Cardiovascular Risk Markers. Nutr. Metab. Cardiovasc. Dis. 2011, 21, S14–S20. [Google Scholar] [CrossRef]
- Wu, L.; Piotrowski, K.; Rau, T.; Waldmann, E.; Broedl, U.C.; Demmelmair, H.; Koletzko, B.; Stark, R.G.; Nagel, J.M.; Mantzoros, C.S.; et al. Walnut-Enriched Diet Reduces Fasting Non-Hdl-Cholesterol and Apolipoprotein b in Healthy Caucasian Subjects: A Randomized Controlled Cross-over Clinical Trial. Metabolism 2014, 63, 382–391. [Google Scholar] [CrossRef]
- Ros, E.; Núñez, I.; Pérez-Heras, A.; Serra, M.; Gilabert, R.; Casals, E.; Deulofeu, R. A Walnut Diet Improves Endothelial Function in Hypercholesterolemic Subjects: A Randomized Crossover Trial. Circulation 2004, 109, 1609–1614. [Google Scholar] [CrossRef]
- Hwang, H.J.; Liu, Y.; Kim, H.S.; Lee, H.; Lim, Y.; Park, H. Daily Walnut Intake Improves Metabolic Syndrome Status and Increases Circulating Adiponectin Levels: Randomized Controlled Crossover Trial. Nutr. Res. Pract. 2019, 13, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Tuccinardi, D.; Farr, O.M.; Upadhyay, J.; Oussaada, S.M.; Klapa, M.I.; Candela, M.; Rampelli, S.; Lehoux, S.; Lázaro, I.; Sala-Vila, A.; et al. Mechanisms Underlying the Cardiometabolic Protective Effect of Walnut Consumption in Obese People: A Cross-over, Randomized, Double-Blind, Controlled Inpatient Physiology Study. Diabetes Obes. Metab. 2019, 21, 2086–2095. [Google Scholar] [CrossRef]
- Tindall, A.M.; McLimans, C.J.; Petersen, K.S.; Kris-Etherton, P.M.; Lamendella, R. Walnuts and Vegetable Oils Containing Oleic Acid Differentially Affect the Gut Microbiota and Associations with Cardiovascular Risk Factors: Follow-up of a Randomized, Controlled, Feeding Trial in Adults at Risk for Cardiovascular Disease. J. Nutr. 2020, 150, 806–817. [Google Scholar] [CrossRef]
- Tsaban, G.; Yaskolka Meir, A.; Rinott, E.; Zelicha, H.; Kaplan, A.; Shalev, A.; Katz, A.; Rudich, A.; Tirosh, A.; Shelef, I.; et al. The Effect of Green Mediterranean Diet on Cardiometabolic Risk; A Randomised Controlled Trial. Heart 2021, 107, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Rajaram, S.; Cofán, M.; Sala-Vila, A.; Haddad, E.; Serra-Mir, M.; Bitok, E.; Roth, I.; Freitas-Simoes, T.M.; Kaur, A.; Valls-Pedret, C.; et al. Effects of Walnut Consumption for 2 Years on Lipoprotein Subclasses among Healthy Elders: Findings from the WAHA Randomized Controlled Trial. Circulation 2021, 144, 1083–1085. [Google Scholar] [CrossRef]
- Soares, A.; Costa, C.; Barbosa, B.; Gomes, L.R.; Neves, J. Evaluation of the Effects of Consumption of Portuguese Walnuts (Juglans regia L.) on the Risk Factors Related to Cardiovascular Diseases. Dietetics 2024, 3, 129–143. [Google Scholar] [CrossRef]
- Mateș, L.; Popa, D.S.; Rusu, M.E.; Fizeșan, I.; Leucuța, D. Walnut Intake Interventions Targeting Biomarkers of Metabolic Syndrome and Inflammation in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2022, 11, 1412. [Google Scholar] [CrossRef]
- Dwan, K.; Li, T.; Altman, D.G.; Elbourne, D. CONSORT 2010 Statement: Extension to Randomised Crossover Trials. BMJ 2019, 366, l4378. [Google Scholar] [CrossRef]
- Swarup, S.; Ahmed, I.; Grigorova, Y.; Zeltser, R. Metabolic Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Forster, H.; Fallaize, R.; Gallagher, C.; O’Donovan, C.B.; Woolhead, C.; Walsh, M.C.; Macready, A.L.; Lovegrove, J.A.; Mathers, J.C.; Gibney, M.J.; et al. Online Dietary Intake Estimation: The Food4me Food Frequency Questionnaire. J. Med. Internet Res. 2014, 16, e150. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.J.; Livingstone, K.M.; Celis-Morales, C.; Forster, H.; Fallaize, R.; O’Donovan, C.B.; Woolhead, C.; Marsaux, C.F.M.; Macready, A.L.; Navas-Carretero, S.; et al. Reproducibility of the Online Food4Me Food-Frequency Questionnaire for Estimating Dietary Intakes across Europe. J. Nutr. 2016, 146, 1068–1075. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. DRI Calculator for Healthcare Professionals. Available online: https://nal.usda.gov/human-nutrition-and-food-safety/dri-calculator (accessed on 27 August 2024).
- Snetselaar, L.G.; De Jesus, J.M.; Desilva, D.M.; Stoody, E.E. Dietary Guidelines for Americans, 2020-2025: Understanding the Scientific Process, Guidelines, and Key Recommendations. Nutr. Today 2021, 56, 287–295. [Google Scholar] [CrossRef]
- European Commision. Food-Based Dietary Guidelines in Europe. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/topic/food-based-dietary-guidelines-europe_en (accessed on 27 August 2024).
- Bosy-Westphal, A.; Booke, C.A.; Blöcker, T.; Kossel, E.; Goele, K.; Later, W.; Hitze, B.; Heller, M.; Glüer, C.C.; Müller, M.J. Measurement Site for Waist Circumference Affects Its Accuracy as an Index of Visceral and Abdominal Subcutaneous Fat in a Caucasian Population. J. Nutr. 2010, 140, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.Y.; Yang, C.Y.; Shih, S.R.; Hsieh, H.J.; Hung, C.S.; Chiu, F.C.; Lin, M.S.; Liu, P.H.; Hua, C.H.; Hsein, Y.C.; et al. Measurement of Waist Circumference: Midabdominal or Iliac Crest? Diabetes Care 2013, 36, 1660–1666. [Google Scholar] [CrossRef]
- Jaeschke, L.; Steinbrecher, A.; Pischon, T. Measurement of Waist and Hip Circumference with a Body Surface Scanner: Feasibility, Validity, Reliability, and Correlations with Markers of the Metabolic Syndrome. PLoS ONE 2015, 10, e0119430. [Google Scholar] [CrossRef] [PubMed]
- Purnell, J.Q. Definitions, Classification, and Epidemiology of Obesity. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK279167/ (accessed on 4 May 2023).
- Tarantino, L.M. Qualified Health Claims: Letter of Enforcement Discretion—Walnuts and Coronary Heart Disease (Docket No 02P0292). Available online: http://wayback.archive-it.org/7993/20171114183725 (accessed on 27 August 2024).
- Houston, L.; Probst, Y.C.; Chandra Singh, M.; Neale, E.P. Tree Nut and Peanut Consumption and Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2023, 14, 1029–1049. [Google Scholar] [CrossRef]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Chiva-Blanch, G.; Fiol, M.; Gómez-Gracia, E.; Arós, F.; Lapetra, J.; et al. Effect of a High-Fat Mediterranean Diet on Bodyweight and Waist Circumference: A Prespecified Secondary Outcomes Analysis of the PREDIMED Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2019, 7, E6–E17. [Google Scholar] [CrossRef]
- Yi, S.Y.; Steffen, L.M.; Zhou, X.; Shikany, J.M.; Jacobs, D.R. Association of Nut Consumption with CVD Risk Factors in Young to Middle-Aged Adults: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2321–2329. [Google Scholar] [CrossRef]
- Rock, C.L.; Flatt, S.W.; Barkai, H.S.; Pakiz, B.; Heath, D.D. Walnut Consumption in a Weight Reduction Intervention: Effects on Body Weight, Biological Measures, Blood Pressure and Satiety. Nutr. J. 2017, 16, 76. [Google Scholar] [CrossRef]
- Bitok, E.; Rajaram, S.; Jaceldo-Siegl, K.; Oda, K.; Sala-Vila, A.; Serra-Mir, M.; Ros, E.; Sabaté, J. Effects of Long-Term Walnut Supplementation on Body Weight in Free-Living Elderly: Results of a Randomized Controlled Trial. Nutrients 2018, 10, 1317. [Google Scholar] [CrossRef] [PubMed]
- Petrović-Oggiano, G.; Debeljak-Martačić, J.; Ranković, S.; Pokimica, B.; Mirić, A.; Glibetić, M.; Popović, T. The Effect of Walnut Consumption on n-3 Fatty Acid Profile of Healthy People Living in a Non-Mediterranean West Balkan Country, a Small Scale Randomized Study. Nutrients 2020, 12, 192. [Google Scholar] [CrossRef] [PubMed]
- Nishi, S.K.; Viguiliouk, E.; Blanco Mejia, S.; Kendall, C.W.C.; Bazinet, R.P.; Hanley, A.J.; Comelli, E.M.; Salas Salvadó, J.; Jenkins, D.J.A.; Sievenpiper, J.L. Are Fatty Nuts a Weighty Concern? A Systematic Review and Meta-Analysis and Dose–Response Meta-Regression of Prospective Cohorts and Randomized Controlled Trials. Obes. Rev. 2021, 22, e13330. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Mesas, A.E.; Garrido-Miguel, M.; Martínez-Ortega, I.A.; Jiménez-López, E.; Martínez-Vizcaíno, V. The Relationship of Tree Nuts and Peanuts with Adiposity Parameters: A Systematic Review and Network Meta-Analysis. Nutrients 2021, 13, 2251. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Dang, M.; Zhang, W.; Wang, Y.; Kord-Varkaneh, H.; Nazary-Vannani, A.; Santos, H.O.; Tan, S.C.; Clark, C.C.T.; Zanghelini, F.; et al. Effects of Walnut Intake on Anthropometric Characteristics: A Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Complement. Ther. Med. 2020, 50, 102395. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Alzahrani, A.A.; Maabreh, H.G.; Prasad, K.D.V.; Bokov, D.O.; Kareem, A.H.; Alawadi, A.; Ihsan, A.; Shakir, M.N.; Alasheqi, M.Q. Effect of Walnut Consumption on Markers of Endothelial Function in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phytother. Res. 2024, 38, 1358–1366. [Google Scholar] [CrossRef]
- Cortés, B.; Núñez, I.; Cofán, M.; Gilabert, R.; Pérez-Heras, A.; Casals, E.; Deulofeu, R.; Ros, E. Acute Effects of High-Fat Meals Enriched with Walnuts or Olive Oil on Postprandial Endothelial Function. J. Am. Coll. Cardiol. 2006, 48, 1666–1671. [Google Scholar] [CrossRef]
- Ros, E.; Doménech, M.; Roman, P.; Lapetra, J.; García De La Corte, F.J.; Sala-Vila, A.; De La Torre, R.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; et al. Mediterranean Diet Reduces 24-Hour Ambulatory Blood Pressure, Blood Glucose, and Lipids: One-Year Randomized, Clinical Trial. Clinical Trial: PREDIMED Trial. Hypertension 2014, 64, 69–76. [Google Scholar] [CrossRef]
- Tindall, A.M.; Petersen, K.S.; Skulas-Ray, A.C.; Richter, C.K.; Proctor, D.N.; Kris-Etherton, P.M. Replacing Saturated Fat with Walnuts or Vegetable Oils Improves Central Blood Pressure and Serum Lipids in Adults at Risk for Cardiovascular Disease: A Randomized Controlled-Feeding Trial. J. Am. Heart Assoc. 2019, 8, 011512. [Google Scholar] [CrossRef]
- Domènech, M.; Serra-Mir, M.; Roth, I.; Freitas-Simoes, T.; Valls-Pedret, C.; Cofán, M.; López, A.; Sala-Vila, A.; Calvo, C.; Rajaram, S.; et al. Effect of a Walnut Diet on Office and 24-Hour Ambulatory Blood Pressure in Elderly Individuals: Findings from the WAHA Randomized Trial. Hypertension 2019, 73, 1049–1057. [Google Scholar] [CrossRef]
- Li, J.; Jiang, B.; Santos, H.O.; Santos, D.; Singh, A.; Wang, L. Effects of Walnut Intake on Blood Pressure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phytother. Res. 2020, 34, 2921–2931. [Google Scholar] [CrossRef]
- Arabi, S.M.; Bahrami, L.S.; Milkarizi, N.; Nematy, M.; Kalmykov, V.; Sahebkar, A. Impact of Walnut Consumption on Cardio Metabolic and Anthropometric Parameters in Metabolic Syndrome Patients: GRADE-Assessed Systematic Review and Dose-Response Meta-Analysis of Data from Randomized Controlled Trials. Pharmacol. Res. 2022, 178, 106190. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Joan, S.; Gary, F.; Kenneth, B.; Synove, K.; Hannelore, B.; Kristian, L. Effects of Walnuts on Serum Lipid Levels and Blood Pressure in Normal Men. N. Engl. J. Med. 1993, 328, 603–607. [Google Scholar]
- Natto, Z.S.; Siapco, G.; Jaceldo-Siegl, K.; Haddad, E.H.; Sabaté, J. Food and Nutrient Displacement by Walnut Supplementation in a Randomized Crossover Study. Nutrients 2022, 14, 1017. [Google Scholar] [CrossRef]
- Bamberger, C.; Rossmeier, A.; Lechner, K.; Wu, L.; Waldmann, E.; Stark, R.G.; Altenhofer, J.; Henze, K.; Parhofer, K.G. A Walnut-Enriched Diet Reduces Lipids in Healthy Caucasian Subjects, Independent of Recommended Macronutrient Replacement and Time Point of Consumption: A Prospective, Randomized, Controlled Trial. Nutrients 2017, 9, 1097. [Google Scholar] [CrossRef]
- Gil-Zamorano, J.; Cofán, M.; de las Hazas, M.C.L.; García-Blanco, T.; García-Ruiz, A.; Doménech, M.; Serra-Mir, M.; Roth, I.; Valls-Pedret, C.; Rajaram, S.; et al. Interplay of Walnut Consumption, Changes in Circulating MiRNAs and Reduction in LDL-Cholesterol in Elders. Nutrients 2022, 14, 1473. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Li, J.; Hu, F.B.; Salas-Salvadó, J.; Tobias, D.K. Effects of Walnut Consumption on Blood Lipids and Other Cardiovascular Risk Factors: An Updated Meta-Analysis and Systematic Review of Controlled Trials. Am. J. Clin. Nutr. 2018, 108, 174–187. [Google Scholar] [CrossRef]
- Alshahrani, S.M.; Mashat, R.M.; Almutairi, D.; Mathkour, A.; Alqahtani, S.S.; Alasmari, A.; Alzahrani, A.H.; Ayed, R.; Asiri, M.Y.; Elsherif, A.; et al. The Effect of Walnut Intake on Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 4660. [Google Scholar] [CrossRef]
- Njike, V.Y.; Costales, V.C.; Petraro, P.; Annam, R.; Yarandi, N.; Katz, D.L. The Resulting Variation in Nutrient Intake with the Inclusion of Walnuts in the Diets of Adults at Risk for Type 2 Diabetes: A Randomized, Controlled, Crossover Trial. Am. J. Health Promot. 2019, 33, 430–438. [Google Scholar] [CrossRef]
- Cronometer. Cronometer (Version 4.0.0) [Desktop App]; Spurrell Technology Inc.: Minnetonka, MN, USA, 2024; Available online: https://www.cronometer.com (accessed on 14 August 2023).
- Schulz, K.F.; Altman, D.G.; Moher, D.; the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Control–Walnut (n = 9) | Walnut–Control (n = 11) |
|---|---|---|
| Age (years) | 47.67 (3.28) | 49 (4.22) |
| Female, n (%) | 4 (44.44) | 6 (54.55) |
| Height (cm) | 173.78 (5.87) | 171 (8.04) |
| Waist circumference (cm) | 102 (5.66) | 96 (7.16) |
| Hip circumference (cm) | 109.33 (7.42) | 107.55 (4.52) |
| Waist–hip ratio | 0.93 (0.05) | 0.89 (0.07) |
| Body weight (kg) | 91.81 (11.86) | 82.33 (10.92) |
| BMI (kg/m2) | 30.02 (2.85) | 28.14 (2.73) |
| Body fat mass (%) | 30.73 (9.36) | 31.55 (9) |
| Body water (%) | 50.32 (5.93) | 49.8 (5.86) |
| VAFR | 10.22 (2.22) | 9.18 (2.26) |
| s-VCAM-1 (ng/mL) | 968.25 (209.13) | 796.78 (228.25) |
| SBP (mmHg) | 127.22 (10.93) | 115.45 (9.34) |
| DBP (mmHg) | 83.33 (9.01) | 73.18 (7.83) |
| TG (mg/dL) | 138.33 (56.72) | 115 (37.38) |
| TC (mg/dL) | 197.44 (21.78) | 233.91 (49.61) |
| LDL-c (mg/dL) | 120.33 (22.39) | 148.73 (38.78) |
| HDL-c (mg/dL) | 49.44 (8.25) | 62.18 (10.88) |
| FBG (mg/dL) | 90.67 (6.78) | 85.73 (8.51) |
| HbA1c (%) | 5.6 (0.25) | 5.66 (0.28) |
| Variables | Control (n = 20) | Walnut (n = 20) | Difference LS (95% CI) | p-Value |
|---|---|---|---|---|
| Waist circumference (cm) | −0.7 (1.53) | −1.45 (1.19) | −1.22 (−2.44–−0.01) | 0.049 |
| Hip circumference (cm) | −0.4 (1.35) | −0.6 (0.99) | −0.73 (−1.81–0.36) | 0.181 |
| Waist–hip ratio | 0 (0.01) | −0.01 (0.01) | −0.01 (−0.02–0.01) | 0.308 |
| Body weight (kg) | −0.44 (1.69) | −0.52 (1.18) | −0.72 (−2.04–0.6) | 0.275 |
| BMI (kg/m2) | −0.16 (0.56) | −0.19 (0.4) | −0.26 (−0.7–0.18) | 0.235 |
| Body fat mass (%) | −0.42 (1.69) | 0.05 (1.05) | 0.05 (−1.23–1.34) | 0.933 |
| Body water (%) | 0.11 (1.39) | −0.09 (0.87) | 0.31 (−0.73–1.35) | 0.551 |
| VAFR | −0.1 (0.52) | −0.15 (0.46) | −0.15 (−0.6–0.3) | 0.513 |
| s-VCAM-1 (ng/mL) | −46.54 (98.06) | −38.63 (147.84) | 2.87 (−114.24–119.98) | 0.961 |
| SBP (mmHg) | 1.5 (10.4) | −2.65 (10.58) | −1.21 (−10.78–8.35) | 0.798 |
| DBP (mmHg) | 2.75 (11.18) | 0.75 (7.83) | −1.62 (−10.57–7.34) | 0.716 |
| TG (mg/dL) | 12.3 (46.95) | −6.3 (43.47) | −32.12 (−74.09–9.85) | 0.129 |
| TC (mg/dL) | 10.15 (21.83) | −1.65 (28.3) | −18.26 (−41.73–5.2) | 0.123 |
| LDL-c (mg/dL) | 6.1 (15.66) | −3.6 (24.82) | −12.16 (−31.42–7.1) | 0.208 |
| HDL-c (mg/dL) | 1.65 (4.97) | 3.3 (6.63) | 0.37 (−5–5.75) | 0.888 |
| FBG (mg/dL) | −2.2 (5.75) | 2.45 (6.83) | 4.24 (−0.68–9.17) | 0.089 |
| HbA1c (%) | −0.12 (0.17) | −0.06 (0.12) | 0.01 (−0.12–0.13) | 0.933 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mateș, L.; Albert-Ani, D.; Fizeșan, I.; Petru, A.-E.; Banc, R.; Rusu, M.E.; Costache, C.; Filip, L.; Popa, D.-S.; Leucuța, D.-C. Benefits of Short-Term (4-Week) Daily Walnut Consumption in Middle-Aged Adults at Risk for Metabolic Syndrome: Outcomes of a Randomized Controlled Trial. Nutrients 2025, 17, 2072. https://doi.org/10.3390/nu17132072
Mateș L, Albert-Ani D, Fizeșan I, Petru A-E, Banc R, Rusu ME, Costache C, Filip L, Popa D-S, Leucuța D-C. Benefits of Short-Term (4-Week) Daily Walnut Consumption in Middle-Aged Adults at Risk for Metabolic Syndrome: Outcomes of a Randomized Controlled Trial. Nutrients. 2025; 17(13):2072. https://doi.org/10.3390/nu17132072
Chicago/Turabian StyleMateș, Letiția, Doina Albert-Ani, Ionel Fizeșan, Andreea-Elena Petru, Roxana Banc, Marius Emil Rusu, Carmen Costache, Lorena Filip, Daniela-Saveta Popa, and Daniel-Corneliu Leucuța. 2025. "Benefits of Short-Term (4-Week) Daily Walnut Consumption in Middle-Aged Adults at Risk for Metabolic Syndrome: Outcomes of a Randomized Controlled Trial" Nutrients 17, no. 13: 2072. https://doi.org/10.3390/nu17132072
APA StyleMateș, L., Albert-Ani, D., Fizeșan, I., Petru, A.-E., Banc, R., Rusu, M. E., Costache, C., Filip, L., Popa, D.-S., & Leucuța, D.-C. (2025). Benefits of Short-Term (4-Week) Daily Walnut Consumption in Middle-Aged Adults at Risk for Metabolic Syndrome: Outcomes of a Randomized Controlled Trial. Nutrients, 17(13), 2072. https://doi.org/10.3390/nu17132072