
The Effect of Dietary Supplements on Male Infertility in Terms of Pregnancy, Live Birth, and Sperm Parameters: A Systematic Review and Meta-Analysis
 , , ,
, , , 
Highlights
- It has previously been suggested that dietary supplements improve male infertility.
- The current study, however, found no convincing evidence to support this.
- Larger and more well-conducted experimental studies that focus on specific dietary supplements and include pregnancy-related outcomes are needed.
Abstract

1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria, Search Strategy, and Selection Process
2.2. Data Collection
2.3. Risk of Bias Assessments
2.4. Synthesis Methods
2.5. Certainty Assessments
3. Results
3.1. Study Selection
3.2. Study Characteristics
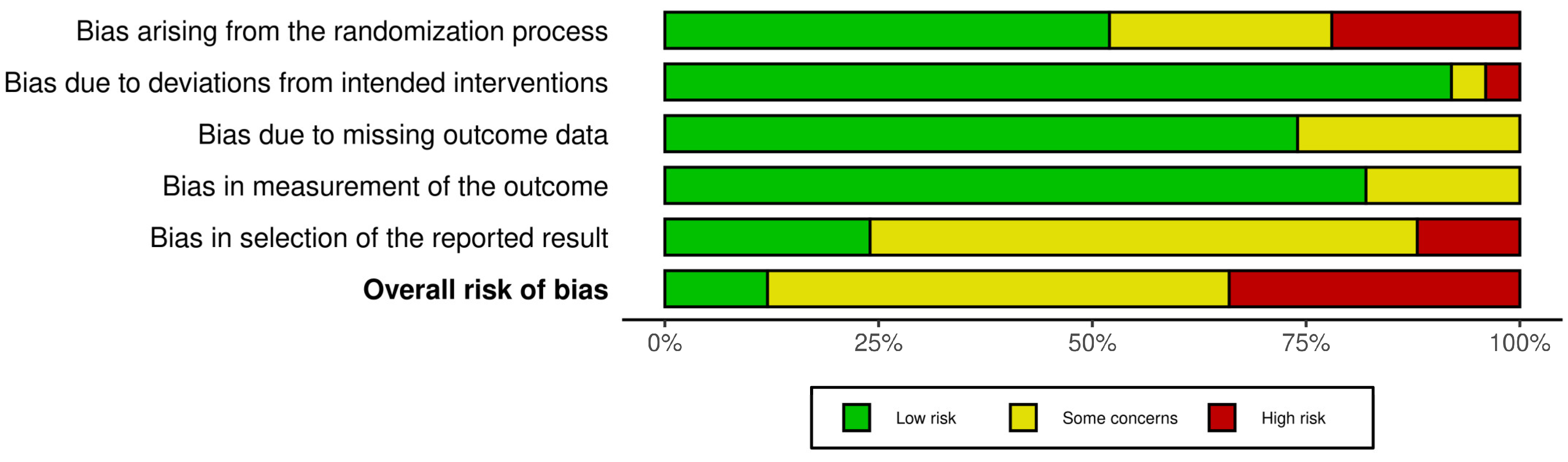
3.3. Risk of Bias in Studies
3.4. Qualitative Synthesis
3.4.1. Vitamin D
3.4.2. L-carnitine and L-acetyl-carnitine
3.4.3. Zinc and Folic Acid
3.4.4. Coenzyme Q10
3.4.5. Alpha-Lipoic Acid
3.4.6. Omega-3 Fatty Acids
3.4.7. Vitamin E
3.4.8. Selenium
3.4.9. Multiple Substance Dietary Supplements
3.4.10. Other Dietary Supplements
3.5. Quantitative Synthesis
3.5.1. Vitamin D
3.5.2. L-carnitine and L-acetyl-carnitine
3.5.3. Zinc and Folic Acid
3.5.4. Coenzyme Q10
3.5.5. Alpha-Lipoic Acid
3.5.6. Omega-3 Fatty Acids
3.5.7. Vitamin E
3.5.8. Selenium
3.5.9. Multiple Substance Dietary Supplements
3.5.10. Explorative Subgroup Analysis
3.6. Reporting Bias
3.7. Certainty of Evidence
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANCOVA | Analysis of covariance |
| ART | Assisted reproductive technology |
| DHA | Docosahexaenoic acid |
| EFSA | European Food Safety Authority |
| GRADE | Grading of recommendations, assessment, development, and evaluation |
| IOM | Institute of Medicine |
| LAC | L-acetyl-carnitine |
| LC | L-carnitine |
| MD | Mean difference |
| OS | Oxidative stress |
| PICOTS | Population–intervention–comparison–outcome–ime–study design |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-analyses |
| Pseudo-IDP | Pseudo individual participant data |
| RCT | Randomized controlled trial |
| RoB2 | Revised Cochrane risk of bias |
| ROS | Reactive oxygen species |
| RR | Risk ratio |
| SE | Standard errors |
| UL | Tolerable upper intake level |
| 95%CI | 95% confidence interval |
References
- Harris, E. Infertility Affects 1 in 6 People Globally. JAMA 2023, 329, 1443. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Singh, A.K. Trends of male factor infertility, an important cause of infertility: A review of literature. J. Hum. Reprod. Sci. 2015, 8, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Sermondade, N.; Faure, C.; Fezeu, L.; Shayeb, A.G.; Bonde, J.P.; Jensen, T.K.; Van Wely, M.; Cao, J.; Martini, A.C.; Eskandar, M.; et al. BMI in relation to sperm count: An updated systematic review and collaborative meta-analysis. Hum. Reprod. Update 2013, 19, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Bundhun, P.K.; Janoo, G.; Bhurtu, A.; Teeluck, A.R.; Soogund, M.Z.S.; Pursun, M.; Huang, F. Tobacco smoking and semen quality in infertile males: A systematic review and meta-analysis. BMC Public Health 2019, 19, 36. [Google Scholar] [CrossRef]
- Nguyen-Thanh, T.; Hoang-Thi, A.P.; Anh Thu, D.T. Investigating the association between alcohol intake and male reproductive function: A current meta-analysis. Heliyon 2023, 9, e15723. [Google Scholar] [CrossRef]
- Belladelli, F.; Muncey, W.; Eisenberg, M.L. Reproduction as a window for health in men. Fertil. Steril. 2023, 120 Pt 1, 429–437. [Google Scholar] [CrossRef]
- Chao, H.H.; Zhang, Y.; Dong, P.Y.; Gurunathan, S.; Zhang, X.F. Comprehensive review on the positive and negative effects of various important regulators on male spermatogenesis and fertility. Front. Nutr. 2022, 9, 1063510. [Google Scholar] [CrossRef]
- Osadchuk, L.; Kleshchev, M.; Danilenko, A.; Osadchuk, A. Impact of seminal and serum zinc on semen quality and hormonal status: A population-based cohort study of Russian young men. J. Trace Elem. Med. Biol. 2021, 68, 126855. [Google Scholar] [CrossRef]
- Salas-Huetos, A.; Rosique-Esteban, N.; Becerra-Tomás, N.; Vizmanos, B.; Bulló, M.; Salas-Salvadó, J. The Effect of Nutrients and Dietary Supplements on Sperm Quality Parameters: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Adv. Nutr. 2018, 9, 833–848. [Google Scholar] [CrossRef]
- Takeshima, T.; Usui, K.; Mori, K.; Asai, T.; Yasuda, K.; Kuroda, S.; Yumura, Y. Oxidative stress and male infertility. Reprod. Med. Biol. 2021, 20, 41–52. [Google Scholar] [CrossRef]
- Omar, M.I.; Pal, R.P.; Kelly, B.D.; Bruins, H.M.; Yuan, Y.; Diemer, T.; Krausz, C.; Tournaye, H.; Kopa, Z.; Jungwirth, A.; et al. Benefits of Empiric Nutritional and Medical Therapy for Semen Parameters and Pregnancy and Live Birth Rates in Couples with Idiopathic Infertility: A Systematic Review and Meta-analysis. Eur. Urol. 2019, 75, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Gaskins, A.J.; Chavarro, J.E. Diet and fertility: A review. Am. J. Obstet. Gynecol. 2018, 218, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Khaw, S.C.; Wong, Z.Z.; Anderson, R.; Martins da Silva, S. l-carnitine and l-acetylcarnitine supplementation for idiopathic male infertility. Reprod. Fertil. 2020, 1, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Lafuente, R.; González-Comadrán, M.; Solà, I.; López, G.; Brassesco, M.; Carreras, R.; Checa, M.A. Coenzyme Q10 and male infertility: A meta-analysis. J. Assist. Reprod. Genet. 2013, 30, 1147–1156. [Google Scholar] [CrossRef]
- Zafar, M.I.; Mills, K.E.; Baird, C.D.; Jiang, H.; Li, H. Effectiveness of Nutritional Therapies in Male Factor Infertility Treatment: A Systematic Review and Network Meta-analysis. Drugs 2023, 83, 531–546. [Google Scholar] [CrossRef]
- de Ligny, W.; Smits, R.M.; Mackenzie-Proctor, R.; Jordan, V.; Fleischer, K.; de Bruin, J.P.; Showell, M.G. Antioxidants for male subfertility. Cochrane Database Syst. Rev. 2022, 5, Cd007411. [Google Scholar] [CrossRef]
- Buhling, K.; Schumacher, A.; Eulenburg, C.Z.; Laakmann, E. Influence of oral vitamin and mineral supplementation on male infertility: A meta-analysis and systematic review. Reprod. Biomed. Online 2019, 39, 269–279. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2020, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Papadimitropoulou, K.; Stijnen, T.; Riley, R.D.; Dekkers, O.M.; le Cessie, S. Meta-analysis of continuous outcomes: Using pseudo IPD created from aggregate data to adjust for baseline imbalance and assess treatment-by-baseline modification. Res. Synth. Methods 2020, 11, 780–794. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Li, T.; Deeks, J.J. Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions, 6.5 ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions, 6.4 ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2023. [Google Scholar]
- Page, M.J.; Higgins, J.P.; Sterne, J.A. Assessing risk of bias due to missing evidence in a meta-analysis. In Cochrane Handbook for Systematic Reviews of Interventions, 6.5 ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef]
- Blomberg Jensen, M.; Lawaetz, J.G.; Petersen, J.H.; Juul, A.; Jørgensen, N. Effects of Vitamin D Supplementation on Semen Quality, Reproductive Hormones, and Live Birth Rate: A Randomized Clinical Trial. J. Clin. Endocrinol. Metab. 2018, 103, 870–881. [Google Scholar] [CrossRef] [PubMed]
- Amini, L.; Mohammadbeigi, R.; Vafa, M.; Haghani, H.; Vahedian-Azimi, A.; Karimi, L.; Jahanfar, S.; Jamialahmadi, T.; Talebi, A.; Sahebkar, A. Evaluation of the effect of vitamin D3 supplementation on quantitative and qualitative parameters of spermograms and hormones in infertile men: A Randomized controlled trial. Complement. Ther. Med. 2020, 53, 102529. [Google Scholar] [CrossRef]
- Maghsoumi-Norouzabad, L.; Zare Javid, A.; Mansoori, A.; Dadfar, M.; Serajian, A. Vitamin D3 Supplementation Effects on Spermatogram and Oxidative Stress Biomarkers in Asthenozoospermia Infertile Men: A Randomized, Triple-Blind, Placebo-Controlled Clinical Trial. Reprod. Sci. 2022, 29, 823–835. [Google Scholar] [CrossRef]
- Gheflati, A.; Mirjalili, S.A.M.; Kaviani, M.; Salehi-Abargouei, A.; Hosseini-Marnani, E.; Nadjarzadeh, A. Effects of vitamin D supplementation on semen quality and reproductive hormones in patients with asthenozoospermia: A randomized double-blind placebo-controlled clinical trial. J. Nutr. Food Secur. 2021, 6, 31–42. [Google Scholar] [CrossRef]
- Cavallini, G.; Ferraretti, A.P.; Gianaroli, L.; Biagiotti, G.; Vitali, G. Cinnoxicam and L-carnitine/acetyl-L-carnitine treatment for idiopathic and varicocele-associated oligoasthenospermia. J. Androl. 2004, 25, 761–770; discussion 771–762. [Google Scholar] [CrossRef]
- Lenzi, A.; Sgrò, P.; Salacone, P.; Paoli, D.; Gilio, B.; Lombardo, F.; Santulli, M.; Agarwal, A.; Gandini, L. A placebo-controlled double-blind randomized trial of the use of combined l-carnitine and l-acetyl-carnitine treatment in men with asthenozoospermia. Fertil. Steril. 2004, 81, 1578–1584. [Google Scholar] [CrossRef]
- Balercia, G.; Regoli, F.; Armeni, T.; Koverech, A.; Mantero, F.; Boscaro, M. Placebo-controlled double-blind randomized trial on the use of L-carnitine, L-acetylcarnitine, or combined L-carnitine and L-acetylcarnitine in men with idiopathic asthenozoospermia. Fertil. Steril. 2005, 84, 662–671. [Google Scholar] [CrossRef]
- Haje, M.; Naoom, K. Combined tamoxifen and L-carnitine therapies for the treatment of idiopathic male infertility attending intracytoplasmic sperm injection: A randomized controlled trial. Int. J. Infertil. Fetal Med. 2015, 6, 20–24. [Google Scholar] [CrossRef]
- Moslemi Mehni, N.; Ketabchi, A.A.; Hosseini, E. Combination effect of Pentoxifylline and L-carnitine on idiopathic oligoasthenoteratozoospermia. Iran. J. Reprod. Med. 2014, 12, 817–824. [Google Scholar] [PubMed]
- Azizollahi, G.; Azizollahi, S.; Babaei, H.; Kianinejad, M.; Baneshi, M.R.; Nematollahi-mahani, S.N. Effects of supplement therapy on sperm parameters, protamine content and acrosomal integrity of varicocelectomized subjects. J. Assist. Reprod. Genet. 2013, 30, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.Y.; Merkus, H.M.; Thomas, C.M.; Menkveld, R.; Zielhuis, G.A.; Steegers-Theunissen, R.P. Effects of folic acid and zinc sulfate on male factor subfertility: A double-blind, randomized, placebo-controlled trial. Fertil. Steril. 2002, 77, 491–498. [Google Scholar] [CrossRef]
- Raigani, M.; Yaghmaei, B.; Amirjannti, N.; Lakpour, N.; Akhondi, M.M.; Zeraati, H.; Hajihosseinal, M.; Sadeghi, M.R. The micronutrient supplements, zinc sulphate and folic acid, did not ameliorate sperm functional parameters in oligoasthenoteratozoospermic men. Andrologia 2014, 46, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Dadgar, Z.; Shariatzadeh, S.M.A.; Mehranjani, M.S.; Kheirolahi, A. The therapeutic effect of co-administration of pentoxifylline and zinc in men with idiopathic infertility. Ir. J. Med. Sci. 2023, 192, 431–439. [Google Scholar] [CrossRef]
- Sharifzadeh, F.; Norouzi, S.; Ashrafi, M.; Aminimoghaddam, S.; Koohpayezadeh, J. Effects of Zinc Sulfate on Subfertility Related to Male Factors: A Prospective Double-Blind, Randomized, Placebo-Controlled Clinical Trial. J. Obstet. Gynecol. Cancer Res. 2022, 1, e7242. [Google Scholar] [CrossRef]
- Huang, W.J.; Lu, X.L.; Li, J.T.; Zhang, J.M. Effects of folic acid on oligozoospermia with MTHFR polymorphisms in term of seminal parameters, DNA fragmentation, and live birth rate: A double-blind, randomized, placebo-controlled trial. Andrology 2020, 8, 110–116. [Google Scholar] [CrossRef]
- da Silva, T.M.; Maia, M.C.S.; Arruda, J.T.; Approbato, F.C.; Mendonça, C.R.; Approbato, M.S. Folic acid does not improve semen parametrs in subfertile men: A double-blin, randomized, placebo-controlled study. J. Bras. De Reprod. Assistida 2013, 17, 152–157. [Google Scholar] [CrossRef]
- Boonyarangkul, A.; Vinayanuvattikhun, N.; Chiamchanya, C.; Visutakul, P. Comparative Study of the Effects of Tamoxifen Citrate and Folate on Semen Quality of the Infertile Male with Semen Abnormality. J. Med. Assoc. Thai 2015, 98, 1057–1063. [Google Scholar]
- Gharakhani Bahar, T.; Masoumi, S.Z.; Pilehvari, S.; Kazemi, F.; Moradkhani, S.; Mahmoudi, S. Effect of CoQ10 Supplement on Spermogram Parameters and Sexual Function of Infertile Men Referred to The Infertility Center of Fatemieh Hospital, Hamadan, Iran, 2019: A Randomized Controlled Trial Study. Int. J. Fertil. Steril. 2023, 17, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Balercia, G.; Buldreghini, E.; Vignini, A.; Tiano, L.; Paggi, F.; Amoroso, S.; Ricciardo-Lamonica, G.; Boscaro, M.; Lenzi, A.; Littarru, G. Coenzyme Q10 treatment in infertile men with idiopathic asthenozoospermia: A placebo-controlled, double-blind randomized trial. Fertil. Steril. 2009, 91, 1785–1792. [Google Scholar] [CrossRef] [PubMed]
- Saeed Alkumait, M.H.M.; Abdul-Aziz, M.M.; Nima, M.H. The effect of glutathione versus co-enzyme q10 on male infertility original study. Medico-Legal Update 2020, 20, 409–414. [Google Scholar] [CrossRef]
- Nadjarzadeh, A.; Sadeghi, M.R.; Amirjannati, N.; Vafa, M.R.; Motevalian, S.A.; Gohari, M.R.; Akhondi, M.A.; Yavari, P.; Shidfar, F. Coenzyme Q10 improves seminal oxidative defense but does not affect on semen parameters in idiopathic oligoasthenoteratozoospermia: A randomized double-blind, placebo controlled trial. J. Endocrinol. Investig. 2011, 34, e224–e228. [Google Scholar] [CrossRef]
- Haghighian, H.K.; Haidari, F.; Mohammadi-Asl, J.; Dadfar, M. Randomized, triple-blind, placebo-controlled clinical trial examining the effects of alpha-lipoic acid supplement on the spermatogram and seminal oxidative stress in infertile men. Fertil. Steril. 2015, 104, 318–324. [Google Scholar] [CrossRef]
- Hodeeb, Y.M.; El-Rewiny, E.M.; Gaafar, A.M.; Zayed, A.N.; Hasan, M.S.; Elsaie, M.L. The effect of alpha lipoic acid supplementation on sperm functions in idiopathic asthenozoospermic patients: A case-controlled study. Human. Fertility, 2022; in press. [Google Scholar] [CrossRef]
- Eslamian, G.; Amirjannati, N.; Noori, N.; Sadeghi, M.R.; Hekmatdoost, A. Effects of coadministration of DHA and vitamin E on spermatogram, seminal oxidative stress, and sperm phospholipids in asthenozoospermic men: A randomized controlled trial. Am. J. Clin. Nutr. 2020, 112, 707–719. [Google Scholar] [CrossRef]
- Conquer, J.A.; Martin, J.B.; Tummon, I.; Watson, L.; Tekpetey, F. Effect of DHA supplementation on DHA status and sperm motility in asthenozoospermic males. Lipids 2000, 35, 149–154. [Google Scholar] [CrossRef]
- Safarinejad, M.R. Effect of omega-3 polyunsaturated fatty acid supplementation on semen profile and enzymatic anti-oxidant capacity of seminal plasma in infertile men with idiopathic oligoasthenoteratospermia: A double-blind, placebo-controlled, randomised study. Andrologia 2011, 43, 38–47. [Google Scholar] [CrossRef]
- Kessopoulou, E.; Powers, H.J.; Sharma, K.K.; Pearson, M.J.; Russell, J.M.; Cooke, I.D.; Barratt, C.L. A double-blind randomized placebo cross-over controlled trial using the antioxidant vitamin E to treat reactive oxygen species associated male infertility. Fertil. Steril. 1995, 64, 825–831. [Google Scholar] [CrossRef]
- Sabeti, P.; Pourmasumi, S.; Fagheirelahee, N. Effect of Selenium and Vitamin E on the Level of Sperm HSPA2+, Intracellular Superoxide Anion and Chromatin Integrity in Idiopathic Asthenoteratozoospermia: A Double-Blind, Randomized, Placebo- Controlled Trial. Urol. J. 2021, 18, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.; MacPherson, A.; Yates, R.W.; Hussain, B.; Dixon, J. The effect of oral selenium supplementation on human sperm motility. Br. J. Urol. 1998, 82, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Busetto, G.M.; Agarwal, A.; Virmani, A.; Antonini, G.; Ragonesi, G.; Del Giudice, F.; Micic, S.; Gentile, V.; De Berardinis, E. Effect of metabolic and antioxidant supplementation on sperm parameters in oligo-astheno-teratozoospermia, with and without varicocele: A double-blind placebo-controlled study. Andrologia 2018, 50, e12927. [Google Scholar] [CrossRef] [PubMed]
- Kopets, R.; Kuibida, I.; Chernyavska, I.; Cherepanyn, V.; Mazo, R.; Fedevych, V.; Gerasymov, S. Dietary supplementation with a novel l-carnitine multi-micronutrient in idiopathic male subfertility involving oligo-, astheno-, teratozoospermia: A randomized clinical study. Andrology 2020, 8, 1184–1193. [Google Scholar] [CrossRef]
- Stenqvist, A.; Oleszczuk, K.; Leijonhufvud, I.; Giwercman, A. Impact of antioxidant treatment on DNA fragmentation index: A double-blind placebo-controlled randomized trial. Andrology 2018, 6, 811–816. [Google Scholar] [CrossRef]
- Steiner, A.Z.; Hansen, K.R.; Barnhart, K.T.; Cedars, M.I.; Legro, R.S.; Diamond, M.P.; Krawetz, S.A.; Usadi, R.; Baker, V.L.; Coward, R.M.; et al. The effect of antioxidants on male factor infertility: The Males, Antioxidants, and Infertility (MOXI) randomized clinical trial. Fertil. Steril. 2020, 113, 552–560.e553. [Google Scholar] [CrossRef]
- Bahmyari, R.; Ariafar, A.; Sayadi, M.; Hossieni, S.; Azima, S. The Effect of Daily Intake of Selenium, Vitamin E and Folic Acid on Sperm Parameters in Males with Idiopathic Infertility: A Single-Blind Randomized Controlled Clinical Trial. Int. J. Fertil. Steril. 2021, 15, 8–14. [Google Scholar] [CrossRef]
- Kumar, R.; Saxena, V.; Shamsi, M.B.; Venkatesh, S.; Dada, R. Herbo-mineral supplementation in men with idiopathic oligoasthenoteratospermia: A double blind randomized placebo-controlled trial. Indian J. Urol. 2011, 27, 357–362. [Google Scholar] [CrossRef]
- Gopinath, P.M.; Kalra, B.; Saxena, A.; Malik, S.; Kochhar, K.; Kalra, S.; Zaveri, H. Fixed dose combination therapy of antioxidants in treatment of idiopathic oligoasthenozoospermia: Results of a randomized, double-blind, placebo-controlled clinical trial. Int. J. Infertil. Fetal Med. 2013, 4, 6–13. [Google Scholar] [CrossRef]
- Zhaku, V.; Beadin, S.; Çeka, X.; Beadini, N.; Durmishi, N. Efficacy and Rationale Behind Combination of the Antioxidant Therapy in Men with Oligoastenozoospermia and Elevated Caspase-3 Activity. Int. J. Med. Sci. 2022, 7, 184–193. [Google Scholar]
- Patki, A.; Shelatkar, R.; Singh, M.; Agarwal, S.; M, V.; Umbardand, S.; Reddy, A.; Kannan, P.; Gorthi, S.; Khastgir, G.; et al. Impact of antioxidants in improving semen parameters like count, motility and DNA fragmentation in sub-fertile males: A randomized, double-blind, placebo-controlled clinical trial. Transl. Clin. Pharmacol. 2023, 31, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Cyrus, A.; Kabir, A.; Goodarzi, D.; Moghimi, M. The effect of adjuvant vitamin C after varicocele surgery on sperm quality and quantity in infertile men: A double blind placebo controlled clinical trial. Int. Braz. J. Urol. 2015, 41, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Calogero, A.E.; Gullo, G.; La Vignera, S.; Condorelli, R.A.; Vaiarelli, A. Myoinositol improves sperm parameters and serum reproductive hormones in patients with idiopathic infertility: A prospective double-blind randomized placebo-controlled study. Andrology 2015, 3, 491–495. [Google Scholar] [CrossRef] [PubMed]
- Ciftci, H.; Verit, A.; Savas, M.; Yeni, E.; Erel, O. Effects of N-acetylcysteine on semen parameters and oxidative/antioxidant status. Urology 2009, 74, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Závaczki, Z.; Szöllõsi, J.; Kiss, S.A.; Koloszár, S.; Fejes, I.; Kovács, L.; Pál, A. Magnesium-orotate supplementation for idiopathic infertile male patients: A randomized, placebo-controlled clinical pilot study. Magnes. Res. 2003, 16, 131–136. [Google Scholar]
- Pryor, J.P.; Blandy, J.P.; Evans, P.; Chaput De Saintonge, D.M.; Usherwood, M. Controlled clinical trial of arginine for infertile men with oligozoospermia. Br. J. Urol. 1978, 50, 47–50. [Google Scholar] [CrossRef]
- Lu, X.L.; Liu, J.J.; Li, J.T.; Yang, Q.A.; Zhang, J.M. Melatonin therapy adds extra benefit to varicecelectomy in terms of sperm parameters, hormonal profile and total antioxidant capacity: A placebo-controlled, double-blind trial. Andrologia 2018, 50, e13033. [Google Scholar] [CrossRef]
- Maretti, C.; Cavallini, G. The association of a probiotic with a prebiotic (Flortec, Bracco) to improve the quality/quantity of spermatozoa in infertile patients with idiopathic oligoasthenoteratospermia: A pilot study. Andrology 2017, 5, 439–444. [Google Scholar] [CrossRef]
- Kumalic, S.I.; Klun, I.V.; Bokal, E.V.; Pinter, B. Effect of the oral intake of astaxanthin on semen parameters in patients with oligo-astheno-teratozoospermia: A randomized double-blind placebo-controlled trial. Radiol. Oncol. 2020, 55, 97–105. [Google Scholar] [CrossRef]
- Nouri, M.; Amani, R.; Nasr-Esfahani, M.; Tarrahi, M.J. The effects of lycopene supplement on the spermatogram and seminal oxidative stress in infertile men: A randomized, double-blind, placebo-controlled clinical trial. Phytother. Res. 2019, 33, 3203–3211. [Google Scholar] [CrossRef]
- Safarinejad, M.R.; Shafiei, N.; Safarinejad, S. A prospective double-blind randomized placebo-controlled study of the effect of saffron (Crocus sativus Linn.) on semen parameters and seminal plasma antioxidant capacity in infertile men with idiopathic oligoasthenoteratozoospermia. Phytother. Res. 2011, 25, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Choe, S.; Park, N.C. Effects of Korean red ginseng on semen parameters in male infertility patients: A randomized, placebo-controlled, double-blind clinical study. Chin. J. Integr. Med. 2016, 22, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Shahmirzadi, A.S.; Shafi, H.; Shirafkan, H.; Memariani, Z.; Gorji, N.; Moeini, R. Effect of Medicago sativa seed powder (Plus vitamin E vs. vitamin E alone) on semen analysis in men with idiopathic infertility: A double blind randomized clinical trial. J. Ethnopharmacol. 2024, 322, 117606. [Google Scholar] [CrossRef]
- Bonde, J.P.; Ernst, E.; Jensen, T.K.; Hjollund, N.H.; Kolstad, H.; Henriksen, T.B.; Scheike, T.; Giwercman, A.; Olsen, J.; Skakkebaek, N.E. Relation between semen quality and fertility: A population-based study of 430 first-pregnancy planners. Lancet 1998, 352, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Mariappen, U.; Keane, K.N.; Hinchliffe, P.M.; Dhaliwal, S.S.; Yovich, J.L. Neither male age nor semen parameters influence clinical pregnancy or live birth outcomes from IVF. Reprod. Biol. 2018, 18, 324–329. [Google Scholar] [CrossRef]
- Findeklee, S.; Radosa, J.C.; Radosa, M.P.; Hammadeh, M.E. Correlation between total sperm count and sperm motility and pregnancy rate in couples undergoing intrauterine insemination. Sci. Rep. 2020, 10, 7555. [Google Scholar] [CrossRef]
- Villani, M.T.; Morini, D.; Spaggiari, G.; Falbo, A.I.; Melli, B.; La Sala, G.B.; Romeo, M.; Simoni, M.; Aguzzoli, L.; Santi, D. Are sperm parameters able to predict the success of assisted reproductive technology? A retrospective analysis of over 22,000 assisted reproductive technology cycles. Andrology 2022, 10, 310–321. [Google Scholar] [CrossRef]
- European Food Safety Authority, Overview on Tolerable Upper Intake Levels as Derived by the Scientific Committee on Food (SCF) and the EFSA Panel on Dietetic Products; Nutrition and Allergies (NDA): Parma, Italy, 2024; Available online: https://www.efsa.europa.eu/sites/default/files/2024-05/ul-summary-report.pdf (accessed on 7 May 2025).
- Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids, 1st ed.; National Academies Press: Washington, DC, USA, 2000.
- Deshmukh, G.; Venkataramaiah, S.B.; Doreswamy, C.M.; Umesh, M.C.; Subbanna, R.B.; Pradhan, B.K.; Seekallu, S.; Sekar, R.; Prabhu, K.; Sadagopan, S.; et al. Safety Assessment of Ubiquinol Acetate: Subchronic Toxicity and Genotoxicity Studies. J. Toxicol. 2019, 2019, 3680757. [Google Scholar] [CrossRef]
- Derosa, G.; D’Angelo, A.; Preti, P.; Maffioli, P. Safety and Efficacy of Alpha Lipoic Acid During 4 Years of Observation: A Retrospective, Clinical Trial in Healthy Subjects in Primary Prevention. Drug Des. Devel Ther. 2020, 14, 5367–5374. [Google Scholar] [CrossRef]
- Yilmaz, R. Efficacy and safety of single or consecutive double high-dose oral cholecalciferol supplementation in adult patients with vitamin D deficiency. Steroids 2023, 199, 109308. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academies Press: Washington, DC, USA, 1998. [Google Scholar] [CrossRef]
- Piera-Jordan, C.; Prieto Huecas, L.; Serrano De La Cruz Delgado, V.; Zaragoza Martí, A.; García Velert, M.B.; Tordera Terrades, C.; Sánchez-SanSegundo, M.; Hurtado-Sánchez, J.A.; Tuells, J.; Martín Manchado, L. Influence of the Mediterranean diet on seminal quality-a systematic review. Front. Nutr. 2024, 11, 1287864. [Google Scholar] [CrossRef] [PubMed]
- Tomada, I.; Tomada, N. Mediterranean Diet and Male Fertility. Endocrines 2023, 4, 394–406. [Google Scholar] [CrossRef]
- Perrone, P.; D’Angelo, S. Gut Microbiota Modulation Through Mediterranean Diet Foods: Implications for Human Health. Nutrients 2025, 17, 948. [Google Scholar] [CrossRef] [PubMed]
- Kaltsas, A.; Zachariou, A.; Markou, E.; Dimitriadis, F.; Sofikitis, N.; Pournaras, S. Microbial Dysbiosis and Male Infertility: Understanding the Impact and Exploring Therapeutic Interventions. J. Pers. Med. 2023, 13, 1491. [Google Scholar] [CrossRef]
- Magill, R.G.; MacDonald, S.M. Male infertility and the human microbiome. Front. Reprod. Health 2023, 5, 1166201. [Google Scholar] [CrossRef]
- Barone, M.; D’Amico, F.; Brigidi, P.; Turroni, S. Gut microbiome-micronutrient interaction: The key to controlling the bioavailability of minerals and vitamins? Biofactors 2022, 48, 307–314. [Google Scholar] [CrossRef]
- Hadadi, N.; Berweiler, V.; Wang, H.; Trajkovski, M. Intestinal microbiota as a route for micronutrient bioavailability. Curr. Opin. Endocr. Metab. Res. 2021, 20, 100285. [Google Scholar] [CrossRef]
- Vanderhout, S.M.; Rastegar Panah, M.; Garcia-Bailo, B.; Grace-Farfaglia, P.; Samsel, K.; Dockray, J.; Jarvi, K.; El-Sohemy, A. Nutrition, genetic variation and male fertility. Transl. Androl. Urol. 2021, 10, 1410–1431. [Google Scholar] [CrossRef]
- de Ligny, W.R.; Fleischer, K.; Grens, H.; Braat, D.D.M.; de Bruin, J.P. The lack of evidence behind over-the-counter antioxidant supplements for male fertility patients: A scoping review. Hum. Reprod. Open 2023, 2023, hoad020. [Google Scholar] [CrossRef]
- Grande, G.; Cosmin Petre, G.; Francini Pesenti, F.; Toni, L.D.; Vitagliano, A.; Nisio, A.D.; Ferlin, A.; Foresta, C.; Garolla, A. Systematic review and critical analysis on dietary supplements for male infertility: From a blend of ingredients to a rationale strategy. J. Endocr. Soc. 2022, 6, A702. [Google Scholar] [CrossRef]
- Beeder, L.; Samplaski, M.K. Analysis of online discussion boards for male infertility. Andrologia, 2019; in press. [Google Scholar] [CrossRef]
- Henkel, R.; Sandhu, I.S.; Agarwal, A. The excessive use of antioxidant therapy: A possible cause of male infertility? Andrologia 2019, 51, e13162. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Males with confirmed infertility or male partners in couples with unexplained infertility * | Female factor infertility; male infertility caused by obstruction of the genital tract; transgender persons |
| Intervention | Dietary supplements | Diets; foods; medications |
| Comparison | Placebo | - |
| Outcome | Primary outcomes: biochemical pregnancy, clinical pregnancy, undefined pregnancy and live birth rate Secondary outcomes: sperm concentration, sperm count, total and progressive motility, normal morphology and sperm DNA Fragmentation Index | - |
| Time | Intervention planned for use for a minimum of 12 weeks to account for the length of the spermatogenesis | Intervention planned for use for less than 12 weeks |
| Study design | Randomized controlled trials | - |
| Other | - | Duplications; unavailable full texts; abstract-only papers; articles where the journal had issued an expression of concern at the time of the search; article not written in the Latin alphabet; studies conducted on animals or in vitro |
| Number of Studies | Effect Measure (95% CI) | I2 | Chi2 | |
|---|---|---|---|---|
| Vitamin D | ||||
| Pregnancy | 1 | - | - | - |
| Live birth | 1 | - | - | - |
| Sperm concentration | 3 | MD −2.09 106/mL (−6.38; 2.19) | 0.00% | p = 0.77 |
| Sperm count | 3 | MD 0.06 106/ejaculate (−3.81; 3.94) | 0.00% | p = 0.68 |
| Total motility | 2 | MD 1.20% (−8.45; 10.84) | 88.26% | p = 0.00 |
| Progressive motility | 4 | MD 0.55% (−4.00; 5.10) | 66.42% | p = 0.01 |
| Normal morphology | 4 | MD −0.07% (−0.92; 0.77) | 56.84% | p = 0.09 |
| DNA Fragmentation Index | 1 | - | - | - |
| L-carnitine and L-acetyl-carnitine | ||||
| Pregnancy | 0 | - | - | - |
| Live birth | 0 | - | - | - |
| Sperm concentration | 4 | MD 2.84 106/mL (−1.79; 7.47) | 96.28% | p = 0.00 |
| Sperm count | 1 | - | - | - |
| Total motility | 3 | MD 9.80% (0.21; 19.39) | 95.60% | p = 0.00 |
| Progressive motility | 2 | MD 8.47% (−6.47; 23.42) | 95.21% | p = 0.00 |
| Normal morphology | 2 | MD 5.28% (−0.88; 11.44) | 99.90% | p = 0.00 |
| DNA Fragmentation Index | 0 | - | - | - |
| Zinc and folic acid | ||||
| Pregnancy | 0 | - | - | - |
| Live birth | 0 | - | - | - |
| Sperm concentration | 6 | MD 7.81 106/mL (1.49; 14.13) | 81.95% | p = 0.00 |
| Sperm count | 1 | - | - | - |
| Total motility | 5 | MD 1.00% (−1.25; 3.25) | 0.00% | p = 0.96 |
| Progressive motility | 3 | MD 4.38% (−3.61; 12.37) | 87.41% | p = 0.00 |
| Normal morphology | 6 | MD 0.69% (−0.54; 1.92) | 92.22% | p = 0.00 |
| DNA Fragmentation Index | 1 | - | - | - |
| Coenzyme Q10 | ||||
| Pregnancy | 0 | - | - | - |
| Live birth | 0 | - | - | - |
| Sperm concentration | 2 | MD −0.56 106/mL (−6.53; 5.41) | 0.00% | p = 0.84 |
| Sperm count | 1 | - | - | - |
| Total motility | 2 | MD 4.35% (0.71; 8.00) | 0.00% | p = 0.87 |
| Progressive motility | 2 | MD 4.95% (2.11; 7.79) | 0.00% | p = 0.92 |
| Normal morphology | 1 | - | - | - |
| DNA Fragmentation Index | 0 | - | - | - |
| Alpha-lipoic acid | ||||
| Pregnancy | 0 | - | - | - |
| Live birth | 0 | - | - | - |
| Sperm concentration | 2 | MD 15.46 106/mL (−8.30; 39.21) | 98.70% | p = 0.00 |
| Sperm count | 1 | - | - | - |
| Total motility | 2 | MD 17.52% (−7.90; 42.94) | 98.80% | p = 0.00 |
| Progressive motility | 2 | MD 15.29% (−2.37; 32.94) | 98.89% | p = 0.00 |
| Normal morphology | 2 | MD 0.95% (0.27; 1.63) | 0.00% | p = 0.54 |
| DNA Fragmentation Index | 0 | - | - | - |
| Omega-3 fatty acids | ||||
| Pregnancy | 0 | - | - | - |
| Live birth | 0 | - | - | - |
| Sperm concentration | 3 | MD 5.73 106/mL (−4.51; 15.98) | 99.09% | p = 0.00 |
| Sperm count | 2 | MD 10.73 106/ejaculate (−8.39; 29.86) | 99.21% | p = 0.00 |
| Total motility | 3 | MD 1.57% (−8.04; 11.18) | 98.88% | p = 0.00 |
| Progressive motility | 1 | - | - | - |
| Normal morphology | 2 | MD 2.64% (−2.64; 7.91) | 98.17% | p = 0.00 |
| DNA Fragmentation Index | 0 | - | - | - |
| Vitamin E | ||||
| Pregnancy | 1 | - | - | - |
| Live birth | 1 | - | - | - |
| Sperm concentration | 2 | MD 0.53 106/mL (−0.36; 1.42) | 0.00% | p = 0.66 |
| Sperm count | 1 | - | - | - |
| Total motility | 2 | MD 8.31% (−5.14; 21.75) | 97.87% | p = 0.00 |
| Progressive motility | 1 | - | - | - |
| Normal morphology | 2 | MD 0.40% (−0.09; 0.89) | 6.76% | p = 0.30 |
| DNA Fragmentation Index | 0 | - | - | - |
| Selenium | ||||
| Pregnancy | 1 | - | - | - |
| Live birth | 0 | - | - | - |
| Sperm concentration | 2 | MD 6.32 106/mL (−14.88; 27.51) | 60.70% | p = 0.11 |
| Sperm count | 0 | - | - | - |
| Total motility | 2 | MD 15.25% (11.71; 18.80) | 0.00% | p = 0.96 |
| Progressive motility | 0 | - | - | - |
| Normal morphology | 1 | - | - | - |
| DNA Fragmentation Index | 0 | - | - | - |
| Multiple substance dietary supplements | ||||
| Pregnancy | 4 | RR 1.75 (0.58; 5.31) | 72.65% | p = 0.01 |
| Live birth | 1 | - | - | - |
| Sperm concentration | 10 | MD 10.53 106/mL (3.00; 18.07) | 91.03% | p = 0.00 |
| Sperm count | 3 | MD 3.10 106/ejaculate (−38.05; 44.24) | 81.22% | p = 0.00 |
| Total motility | 8 | MD 2.73% (−1.75; 7.21) | 76.88% | p = 0.00 |
| Progressive motility | 6 | MD 5.55% (−1.31; 12.41) | 89.28% | p = 0.00 |
| Normal morphology | 6 | MD −0.04% (−0.54; 0.46) | 0.00% | p = 0.11 |
| DNA Fragmentation Index | 2 | MD 1.27% (−2.79; 5.33) | 0.00% | p = 0.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michaelsen, M.P.; Poulsen, M.; Bjerregaard, A.A.; Borgstrøm, M.; Poulsen, L.K.; Chortsen, M.B.; Henriksen, S.G.; Kesmodel, U.S. The Effect of Dietary Supplements on Male Infertility in Terms of Pregnancy, Live Birth, and Sperm Parameters: A Systematic Review and Meta-Analysis. Nutrients 2025, 17, 1710. https://doi.org/10.3390/nu17101710
Michaelsen MP, Poulsen M, Bjerregaard AA, Borgstrøm M, Poulsen LK, Chortsen MB, Henriksen SG, Kesmodel US. The Effect of Dietary Supplements on Male Infertility in Terms of Pregnancy, Live Birth, and Sperm Parameters: A Systematic Review and Meta-Analysis. Nutrients. 2025; 17(10):1710. https://doi.org/10.3390/nu17101710
Chicago/Turabian StyleMichaelsen, Mette Peters, Michelle Poulsen, Anne Ahrendt Bjerregaard, Maria Borgstrøm, Lotte Kraglund Poulsen, Maria Bach Chortsen, Sahra Gatten Henriksen, and Ulrik Schiøler Kesmodel. 2025. "The Effect of Dietary Supplements on Male Infertility in Terms of Pregnancy, Live Birth, and Sperm Parameters: A Systematic Review and Meta-Analysis" Nutrients 17, no. 10: 1710. https://doi.org/10.3390/nu17101710
APA StyleMichaelsen, M. P., Poulsen, M., Bjerregaard, A. A., Borgstrøm, M., Poulsen, L. K., Chortsen, M. B., Henriksen, S. G., & Kesmodel, U. S. (2025). The Effect of Dietary Supplements on Male Infertility in Terms of Pregnancy, Live Birth, and Sperm Parameters: A Systematic Review and Meta-Analysis. Nutrients, 17(10), 1710. https://doi.org/10.3390/nu17101710