
Intake or Blood Levels of Magnesium and Risk of Metabolic Syndrome: A Meta-Analysis of Observational Studies



Abstract
1. Introduction
2. Materials and Methods
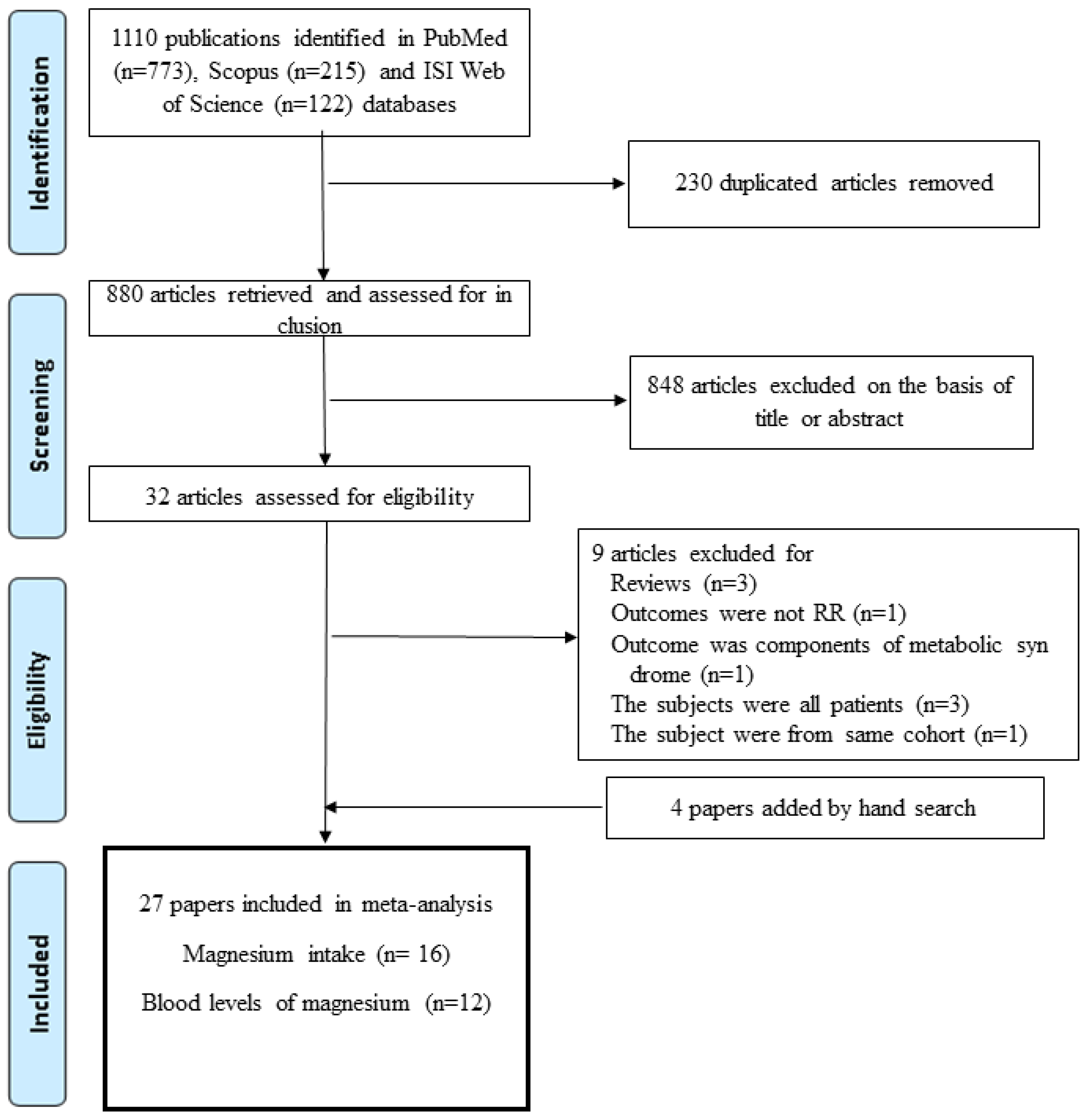
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
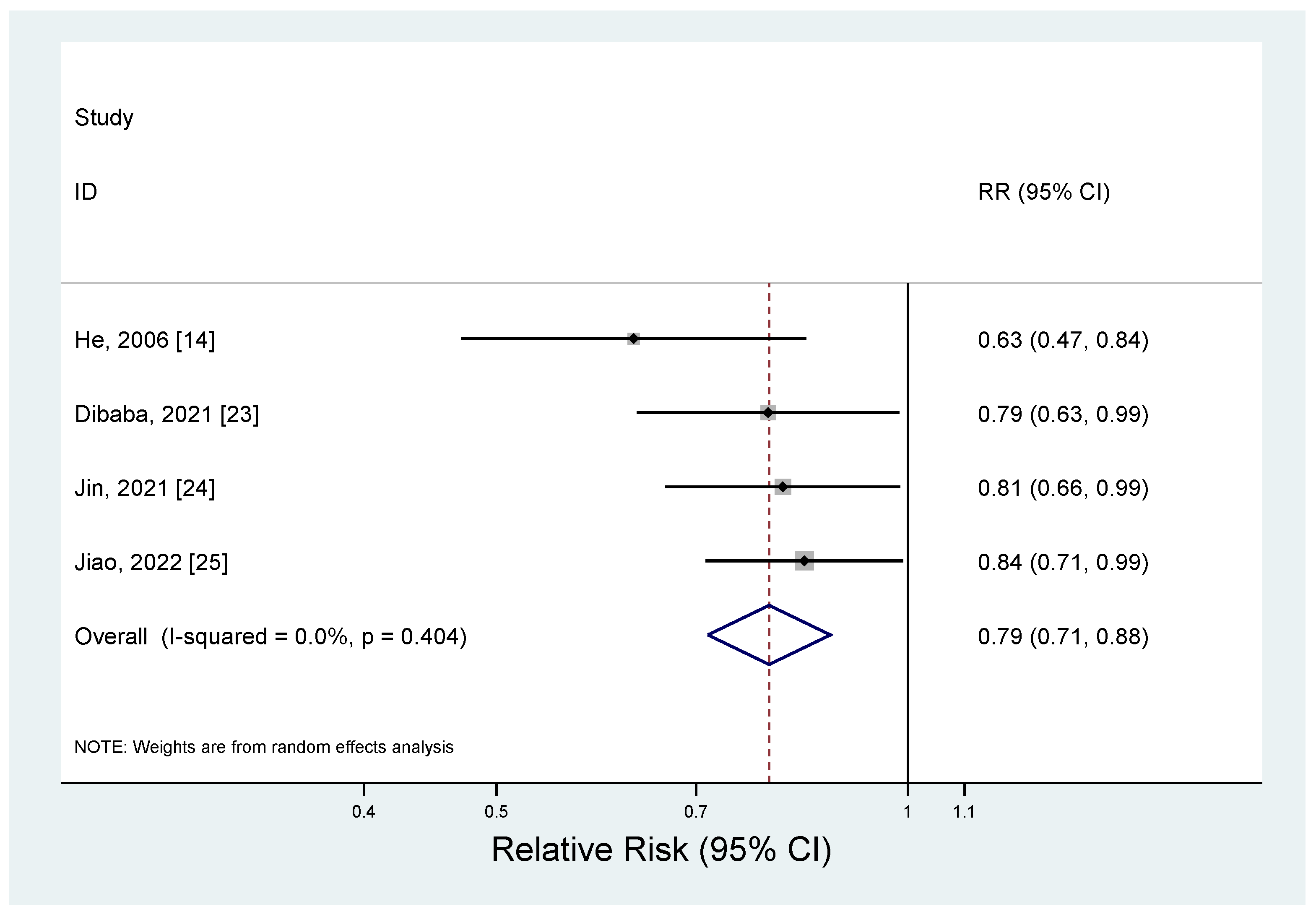
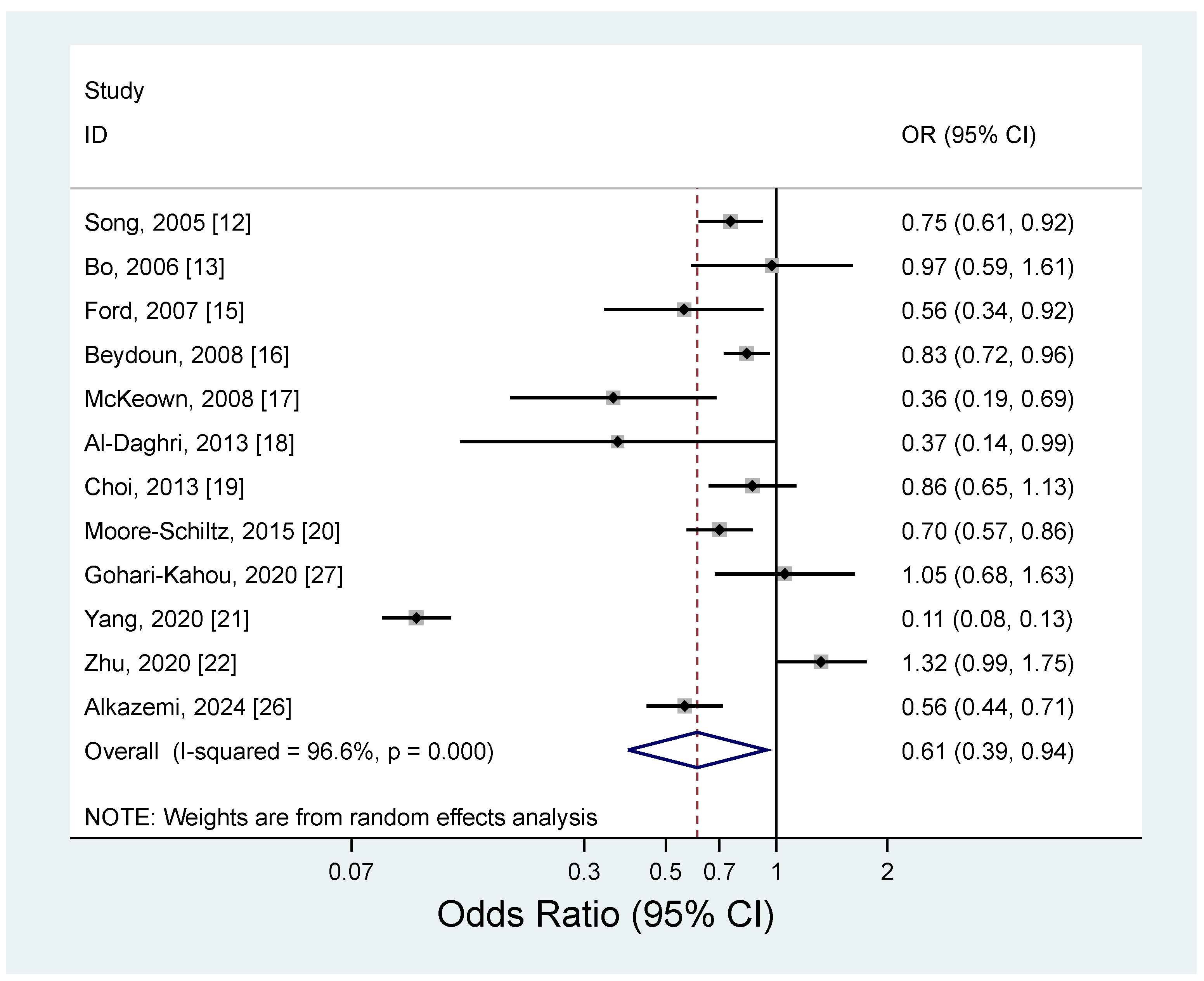
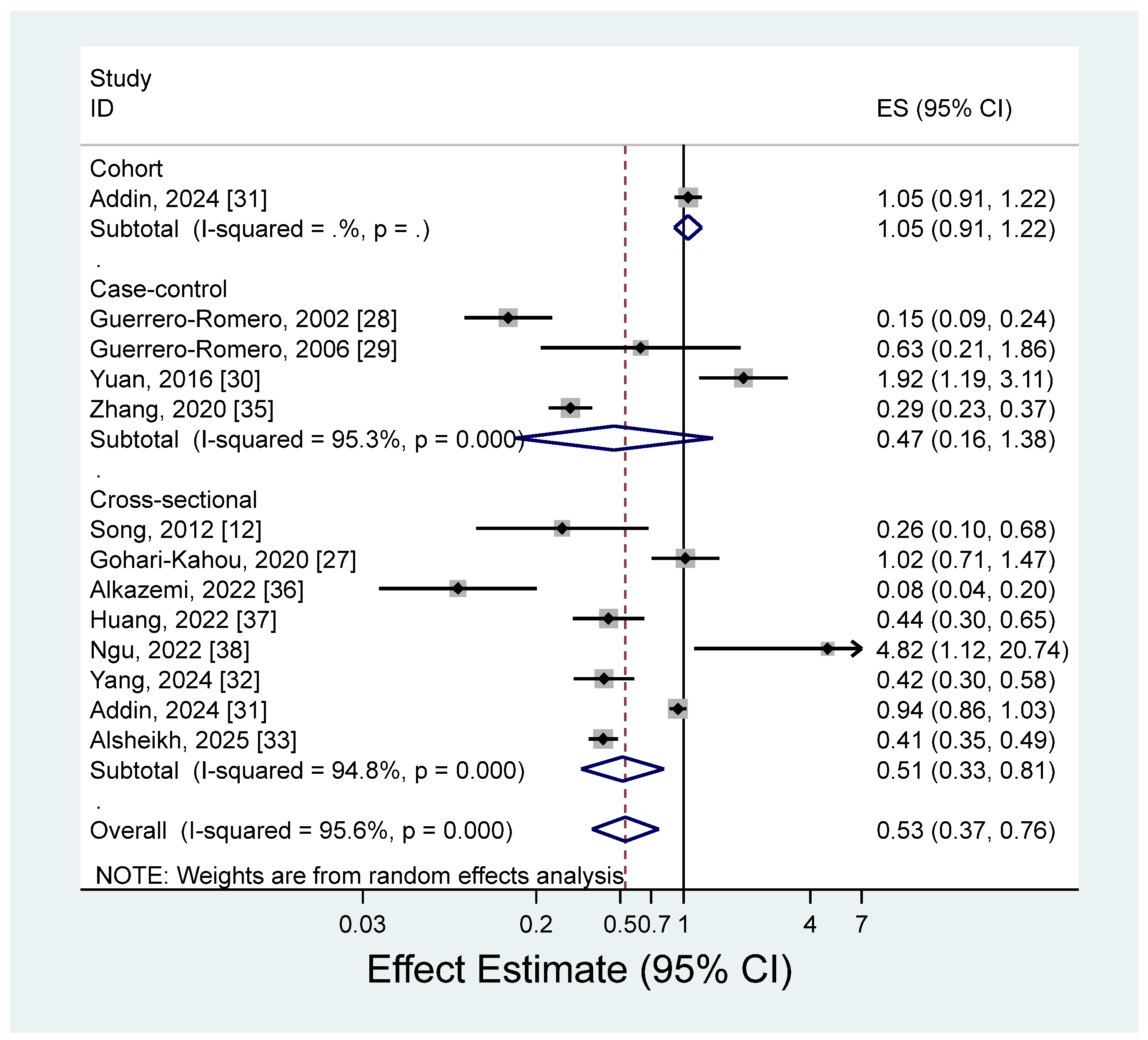
3.2. Magnesium and Metabolic Syndrome
3.3. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DNA | Deoxyribonucleic acid |
| HDL | High-density lipoprotein |
| CVD | Cardiovascular disease |
| RR | Relative risk |
| OR | Odds ratio |
| ES | Estimate |
| CI | Confidence interval |
| BMI | Body mass index |
| LDL | Low-density lipoprotein |
| LPL | Lipoprotein lipase |
| LCAT | Lecithin–cholesterol acyltransferase |
References
- Tarleton, E.K. Factors influencing magnesium consumption among adults in the United States. Nutr. Rev. 2018, 76, 526–538. [Google Scholar] [CrossRef]
- Volpe, S.L. Magnesium in disease prevention and overall health. Adv. Nutr. 2013, 4, 378S–383S. [Google Scholar] [CrossRef] [PubMed]
- de Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Rubin, H. The membrane, magnesium, mitosis (MMM) model of cell proliferation control. Magnes. Res. 2005, 18, 268–274. [Google Scholar] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Silveira Rossi, J.L.; Barbalho, S.M.; Reverete de Araujo, R.; Bechara, M.D.; Sloan, K.P.; Sloan, L.A. Metabolic syndrome and cardiovascular diseases: Going beyond traditional risk factors. Diabetes Metab. Res. Rev. 2022, 38, e3502. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.L.; Foka, A.J.; Ndoadoumgue, A.L.; et al. Geographic distribution of metabolic syndrome and its components in the general adult population: A meta-analysis of global data from 28 million individuals. Diabetes Res. Clin. Pract. 2022, 188, 109924. [Google Scholar] [CrossRef]
- Di Marzo, V.; Silvestri, C. Lifestyle and Metabolic Syndrome: Contribution of the Endocannabinoidome. Nutrients 2019, 11, 1956. [Google Scholar] [CrossRef]
- Codazzi, V.; Frontino, G.; Galimberti, L.; Giustina, A.; Petrelli, A. Mechanisms and risk factors of metabolic syndrome in children and adolescents. Endocrine 2024, 84, 16–28. [Google Scholar] [CrossRef]
- Yamaoka, K.; Tango, T. Effects of lifestyle modification on metabolic syndrome: A systematic review and meta-analysis. BMC Med. 2012, 10, 138. [Google Scholar] [CrossRef]
- Soltani, S.; Kolahdouz Mohammadi, R.; Shab-Bidar, S.; Vafa, M.; Salehi-Abargouei, A. Sodium status and the metabolic syndrome: A systematic review and meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Ridker, P.M.; Manson, J.E.; Cook, N.R.; Buring, J.E.; Liu, S. Magnesium intake, C-reactive protein, and the prevalence of metabolic syndrome in middle-aged and older U.S. women. Diabetes Care 2005, 28, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Durazzo, M.; Guidi, S.; Carello, M.; Sacerdote, C.; Silli, B.; Rosato, R.; Cassader, M.; Gentile, L.; Pagano, G. Dietary magnesium and fiber intakes and inflammatory and metabolic indicators in middle-aged subjects from a population-based cohort. Am. J. Clin. Nutr. 2006, 84, 1062–1069. [Google Scholar] [CrossRef]
- He, K.; Liu, K.; Daviglus, M.L.; Morris, S.J.; Loria, C.M.; Van Horn, L.; Jacobs, D.R., Jr.; Savage, P.J. Magnesium intake and incidence of metabolic syndrome among young adults. Circulation 2006, 113, 1675–1682. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; McGuire, L.C.; Mokdad, A.H.; Liu, S. Intake of dietary magnesium and the prevalence of the metabolic syndrome among U.S. adults. Obesity 2007, 15, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Gary, T.L.; Caballero, B.H.; Lawrence, R.S.; Cheskin, L.J.; Wang, Y. Ethnic differences in dairy and related nutrient consumption among US adults and their association with obesity, central obesity, and the metabolic syndrome. Am. J. Clin. Nutr. 2008, 87, 1914–1925. [Google Scholar] [CrossRef]
- McKeown, N.M.; Jacques, P.F.; Zhang, X.L.; Juan, W.; Sahyoun, N.R. Dietary magnesium intake is related to metabolic syndrome in older Americans. Eur. J. Nutr. 2008, 47, 210–216. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Khan, N.; Alkharfy, K.M.; Al-Attas, O.S.; Alokail, M.S.; Alfawaz, H.A.; Alothman, A.; Vanhoutte, P.M. Selected dietary nutrients and the prevalence of metabolic syndrome in adult males and females in Saudi Arabia: A pilot study. Nutrients 2013, 5, 4587–4604. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.K.; Bae, Y.J. Relationship between dietary magnesium, manganese, and copper and metabolic syndrome risk in Korean adults: The Korea National Health and Nutrition Examination Survey (2007–2008). Biol. Trace Elem. Res. 2013, 156, 56–66. [Google Scholar] [CrossRef]
- Moore-Schiltz, L.; Albert, J.M.; Singer, M.E.; Swain, J.; Nock, N.L. Dietary intake of calcium and magnesium and the metabolic syndrome in the National Health and Nutrition Examination (NHANES) 2001–2010 data. Br. J. Nutr. 2015, 114, 924–935. [Google Scholar] [CrossRef]
- Yang, N.; He, L.; Li, Y.; Xu, L.; Ping, F.; Li, W.; Zhang, H. Reduced Insulin Resistance Partly Mediated the Association of High Dietary Magnesium Intake with Less Metabolic Syndrome in a Large Chinese Population. Diabetes Metab. Syndr. Obes. 2020, 13, 2541–2550. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; He, Y.; Wu, F.; Zhao, L.; Wu, C.; Lu, Y.; Zang, J.; Wang, Z.; Sun, J.; Huang, J.; et al. The Associations of Dietary Iron, Zinc and Magnesium with Metabolic Syndrome in China’s Mega Cities. Nutrients 2020, 12, 659. [Google Scholar] [CrossRef]
- Dibaba, D.T.; Chen, C.; Lu, L.; Bidulescu, A.; Fly, A.D.; Xun, P.; Judd, S.E.; Cushman, M.; Kahe, K. Magnesium intake is inversely associated with the risk of metabolic syndrome in the REasons for geographic and racial differences in stroke (REGARDS) cohort study. Clin. Nutr. 2021, 40, 2337–2342. [Google Scholar] [CrossRef]
- Jin, S.; Liu, J.; Jia, Y.; Han, T.; Zhao, X.; Sun, C.; Na, L. The association of dietary flavonoids, magnesium and their interactions with the metabolic syndrome in Chinese adults: A prospective cohort study. Br. J. Nutr. 2021, 126, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Y.; Li, W.; Wang, L.; Jiang, H.; Wang, S.; Jia, X.; Wang, Z.; Wang, H.; Zhang, B.; Ding, G. Relationship between Dietary Magnesium Intake and Metabolic Syndrome. Nutrients 2022, 14, 2013. [Google Scholar] [CrossRef]
- Alkazemi, D.U.Z.; Zafar, T.A.; Alsouri, N.Y.; Aljahdali, A.A.; Kubow, S. Low dietary magnesium and fiber intakes among women with metabolic syndrome in Kuwait. Front. Nutr. 2024, 11, 1451220. [Google Scholar] [CrossRef]
- Gohari-Kahou, M.; Darroudi, S.; Saberi-Karimian, M.; Parizadeh, S.; Asadi, Z.; Javandoost, A.; Safarian, M.; Mouhebati, M.; Ebrahimi, M.; Ferns, G.A.; et al. The association between serum and dietary magnesium with cardiovascular disease risk factors in Iranian adults with metabolic syndrome. Transl. Metab. Syndr. Res. 2020, 3, 42–48. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodríguez-Morán, M. Low serum magnesium levels and metabolic syndrome. Acta Diabetol. 2002, 39, 209–213. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodriguez-Moran, M. Hypomagnesemia, oxidative stress, inflammation, and metabolic syndrome. Diabetes Metab. Res. Rev. 2006, 22, 471–476. [Google Scholar] [CrossRef]
- Yuan, Z.; Liu, C.; Tian, Y.; Zhang, X.; Ye, H.; Jin, L.; Ruan, L.; Sun, Z.; Zhu, Y. Higher Levels of Magnesium and Lower Levels of Calcium in Whole Blood Are Positively Correlated with the Metabolic Syndrome in a Chinese Population: A Case-Control Study. Ann. Nutr. Metab. 2016, 69, 125–134. [Google Scholar] [CrossRef]
- Addin, N.S.; Niedermayer, F.; Thorand, B.; Linseisen, J.; Seissler, J.; Peters, A.; Rospleszcz, S. Association of serum magnesium with metabolic syndrome and the role of chronic kidney disease: A population-based cohort study with Mendelian randomization. Diabetes Obes. Metab. 2024, 26, 1808–1820. [Google Scholar] [CrossRef]
- Yang, J.; Cao, Y.; Zhang, H.; Hu, Y.; Lu, J.; Wang, R.; Feng, J.; Yang, L. Association and dose-response relationship of plasma magnesium with metabolic syndrome in Chinese adults older than 45 years. Front. Nutr. 2024, 11, 1346825. [Google Scholar] [CrossRef]
- Alsheikh, R.; Aldulaimi, H.; Hinawi, R.; Al-Sadi, F.; Al-Baker, A.; Alkuwari, A.; Sameer, M.; Al-Abdulla, G.; Shi, Z.; Rathnaiah Babu, G. Association of serum magnesium and calcium with metabolic syndrome: A cross-sectional study from the Qatar-biobank. Nutr. Metab. 2025, 22, 8. [Google Scholar] [CrossRef]
- Song, I.J.; Park, C.; Uh, W.C.; Yang, J.Y.; Lee, J.; Lee, S.; Ga, H. The Relationship Between Serum Magnesium Levels and Metabolic Syndrome in Korean Adults. J. Obes. Metab. Syndr. 2012, 21, 11–17. [Google Scholar] [CrossRef]
- Zhang, W.; Du, J.; Li, H.; Yang, Y.; Cai, C.; Gao, Q.; Xing, Y.; Shao, B.; Li, G. Multiple-element exposure and metabolic syndrome in Chinese adults: A case-control study based on the Beijing population health cohort. Environ. Int. 2020, 143, 105959. [Google Scholar] [CrossRef] [PubMed]
- Alkazemi, D.; Alsouri, N.; Zafar, T.; Kubow, S. Hypomagnesemia and the Metabolic Syndrome among Apparently Healthy Kuwaiti Adults: A Cross-Sectional Study. Nutrients 2022, 14, 5257. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Zhong, D.; Lv, Z.; Cheng, J.; Zou, X.; Wang, T.; Wen, Y.; Wang, C.; Yu, S.; Huang, H.; et al. Associations of multiple plasma metals with the risk of metabolic syndrome: A cross-sectional study in the mid-aged and older population of China. Ecotoxicol. Environ. Saf. 2022, 231, 113183. [Google Scholar] [CrossRef]
- Ngu, Y.J.; Skalny, A.V.; Tinkov, A.A.; Tsai, C.S.; Chang, C.C.; Chuang, Y.K.; Nikolenko, V.N.; Zotkin, D.A.; Chiu, C.F.; Chang, J.S. Association Between Essential and Non-essential Metals, Body Composition, and Metabolic Syndrome in Adults. Biol. Trace Elem. Res. 2022, 200, 4903–4915. [Google Scholar] [CrossRef]
- Dibaba, D.T.; Xun, P.; Fly, A.D.; Yokota, K.; He, K. Dietary magnesium intake and risk of metabolic syndrome: A meta-analysis. Diabet. Med. 2014, 31, 1301–1309. [Google Scholar] [CrossRef]
- Sarrafzadegan, N.; Khosravi-Boroujeni, H.; Lotfizadeh, M.; Pourmogaddas, A.; Salehi-Abargouei, A. Magnesium status and the metabolic syndrome: A systematic review and meta-analysis. Nutrition 2016, 32, 409–417. [Google Scholar] [CrossRef]
- Al Shammaa, A.; Al-Thani, A.; Al-Kaabi, M.; Al-Saeed, K.; Alanazi, M.; Shi, Z. Serum Magnesium is Inversely Associated with Body Composition and Metabolic Syndrome. Diabetes Metab. Syndr. Obes. 2023, 16, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 May 2025).
- Herzog, R.; Alvarez-Pasquin, M.J.; Diaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, A. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Cleeman, J.I. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Morais, J.B.S.; Severo, J.S.; de Alencar, G.R.R.; de Oliveira, A.R.S.; Cruz, K.J.C.; Marreiro, D.D.N.; Freitas, B.; de Carvalho, C.M.R.; Martins, M.; Frota, K.M.G. Effect of magnesium supplementation on insulin resistance in humans: A systematic review. Nutrition 2017, 38, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Li, X.; Wang, X.; Xu, M. Effects of magnesium supplementation on improving hyperglycemia, hypercholesterolemia, and hypertension in type 2 diabetes: A pooled analysis of 24 randomized controlled trials. Front. Nutr. 2022, 9, 1020327. [Google Scholar] [CrossRef] [PubMed]
- Asbaghi, O.; Moradi, S.; Nezamoleslami, S.; Moosavian, S.P.; Hojjati Kermani, M.A.; Lazaridi, A.V.; Miraghajani, M. The Effects of Magnesium Supplementation on Lipid Profile Among Type 2 Diabetes Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Biol. Trace Elem. Res. 2021, 199, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Hariri, M.; Sohrabi, M.; Gholami, A. The effect of magnesium supplementation on serum concentration of lipid profile: An updated systematic review and dose-response meta-analysis on randomized controlled trials. Nutr. J. 2025, 24, 24. [Google Scholar] [CrossRef]
- Askari, M.; Mozaffari, H.; Jafari, A.; Ghanbari, M.; Darooghegi Mofrad, M. The effects of magnesium supplementation on obesity measures in adults: A systematic review and dose-response meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2021, 61, 2921–2937. [Google Scholar] [CrossRef]
- Vinals, F.; Camps, M.; Testar, X.; Palacin, M.; Zorzano, A. Effect of cations on the tyrosine kinase activity of the insulin receptor: Inhibition by fluoride is magnesium dependent. Mol. Cell Biochem. 1997, 171, 69–73. [Google Scholar] [CrossRef]
- Gommers, L.M.; Hoenderop, J.G.; Bindels, R.J.; de Baaij, J.H. Hypomagnesemia in Type 2 Diabetes: A Vicious Circle? Diabetes 2016, 65, 3–13. [Google Scholar] [CrossRef]
- Suarez, A.; Pulido, N.; Casla, A.; Casanova, B.; Arrieta, F.J.; Rovira, A. Impaired tyrosine-kinase activity of muscle insulin receptors from hypomagnesaemic rats. Diabetologia 1995, 38, 1262–1270. [Google Scholar] [CrossRef]
- Louvet, L.; Bazin, D.; Buchel, J.; Steppan, S.; Passlick-Deetjen, J.; Massy, Z.A. Characterisation of calcium phosphate crystals on calcified human aortic vascular smooth muscle cells and potential role of magnesium. PLoS ONE 2015, 10, e0115342. [Google Scholar] [CrossRef]
- Dominguez, L.; Veronese, N.; Barbagallo, M. Magnesium and Hypertension in Old Age. Nutrients 2020, 13, 139. [Google Scholar] [CrossRef]
- Satake, K.; Lee, J.D.; Shimizu, H.; Uzui, H.; Mitsuke, Y.; Yue, H.; Ueda, T. Effects of magnesium on prostacyclin synthesis and intracellular free calcium concentration in vascular cells. Magnes. Res. 2004, 17, 20–27. [Google Scholar]
- Verma, H.; Garg, R. Effect of magnesium supplementation on type 2 diabetes associated cardiovascular risk factors: A systematic review and meta-analysis. J. Hum. Nutr. Diet. 2017, 30, 621–633. [Google Scholar] [CrossRef] [PubMed]
- Rosanoff, A.; Seelig, M.S. Comparison of mechanism and functional effects of magnesium and statin pharmaceuticals. J. Am. Coll. Nutr. 2004, 23, 501S–505S. [Google Scholar] [CrossRef]
- Viljoen, A.; Wierzbicki, A.S. Dyslipidemia: Diabetes Lipidtherapies. In Textbook of Diabetes; Holt Rig, C.C., Flyvbjerg, A., Goldstein, B.J., Eds.; Blackwell Science: Boston, MA, USA, 2010. [Google Scholar]
- Shamnani, G.R.C.; Gupta, V.; Singh, S.; Tiwari, S.; Bhartiy, S.S.; Sharma, P. Serum magnesium in relation with obesity. Natl. J. Physiol. Pharm. Pharmacol. 2018, 8, 1074–1077. [Google Scholar] [CrossRef]
- Kazuko, M.; Gavin, W.L. Epinephrine and its Role in the Development of Obesity and Hypertension. Curr. Hypertens. Rev. 2011, 7, 144–152. [Google Scholar] [CrossRef]
- Noori, N.; Nafar, M.; Poorrezagholi, F.; Ahmadpoor, P.; Samadian, F.; Firouzan, A.; Einollahi, B. Dietary intakes of fiber and magnesium and incidence of metabolic syndrome in first year after renal transplantation. J. Ren. Nutr. 2010, 20, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.H.; Lu, Y.F.; Cheng, F.C.; Lee, J.N.; Tsai, L.C. Correlation of magnesium intake with metabolic parameters, depression and physical activity in elderly type 2 diabetes patients: A cross-sectional study. Nutr. J. 2012, 11, 41. [Google Scholar] [CrossRef]
- Elin, R.J. Assessment of magnesium status for diagnosis and therapy. Magnes. Res. 2010, 23, S194–S198. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Country | Study Name | Follow-Up Years | Age at Baseline (Years) | Sex | Study Size | Adjustment for Covariates | |
|---|---|---|---|---|---|---|---|---|
| Subjects | No. of Cases | |||||||
| He, 2006 [14] | U.S. | The Coronary Artery Risk Development in Young Adults | 15 | 18–30 | Male and female | 4637 | 608 | Age, sex, race, education, smoking, physical activity, family history of diabetes, alcohol consumption, baseline BMI, and intakes of fiber, polyunsaturated fat, saturated fat, total carbohydrates, and total energy |
| Dibaba, 2021 [23] | U.S. | The Reasons for Geographic and Racial Differences in Stroke | 10 | ≥45 | Male and female | 6802 | 1470 | Age, sex, race, region, the interaction between age and race, education, income, smoking, alcohol consumption, physical activity, energy intake, regular aspirin use, calcium intake, and LDL cholesterol |
| Jin, 2021 [24] | China | The Harbin Cohort Study on Diet, Nutrition and Chronic Non-Communicable Diseases | 5.3 | 20–74 | Male and female | 6417 | 1283 | Age, sex, drinking, smoking, physical activity, BMI, fat, protein, carbohydrate, fiber, and total energy |
| Jiao, 2022 [25] | China | China Health and Nutrition Survey | 6.1 | ≥18 | Male and female | 6104 | 2024 | Age, sex, education, urban and rural areas, income, smoking, drinking, physical activity, energy, dietary fiber, calcium, and BMI |
| First Author, Year | Country | Study Name | Age at Baseline (Years) | Sex | Study Size | Adjustment for Covariates | |
|---|---|---|---|---|---|---|---|
| Subjects | No. of Cases | ||||||
| Song, 2005 [12] | U.S. | Women’s Health Study | ≥45 | Female | 9887 | 2411 | Age, smoking, exercise, total calories, alcohol use, multivitamin use, parental history of myocardial infarction before 60 years, dietary intake of total fat, cholesterol, folate, glycemic load, fiber, and plasma C-reactive protein concentrations |
| Bo, 2006 [13] | Italy | NA | 45–64 | Male and female | 1653 | 384 | Age, sex, BMI, smoking, alcohol intake, level of physical activity, dietary intake of total calories, total percentage of fat, and dietary intake of fiber |
| Ford, 2007 [15] | U.S. | The Third National Health and Nutrition Examination Survey (1988–1994) | ≥20 | Male and female | 7669 | 1981 | Age, sex, race or ethnicity, education, smoking, concentration of C-reactive protein, alcohol use, physical activity, family history of early coronary heart disease, use of vitamins or supplements, history of diabetes, percentage of calories as fat, percentage of calories as carbohydrate, fiber intake, and total energy intake |
| Beydoun, 2008 [16] | U.S. | National Health and Nutrition Examination Survey (1999–2004) | ≥18 | Male and female | 4519 | 1166 | Age, sex, ethnicity, socioeconomic status (education and poverty income ratio), energy intake, and physical activity |
| McKeown, 2008 [17] | U.S. | NA | ≥60 | Male and female | 535 | 214 | Age, sex, race, educational attainment, marital status, smoking, alcohol intake, exercise, BMI, total energy intake, percentage energy of saturated fatty acid intake, lipid-lowering medication use, and blood pressure medication |
| Al-Daghri, 2013 [18] | Saudi Arabia | NA | 19–60 | Male and female | 185 | 72 | Age, energy, BMI, and physical activity |
| Choi, 2013 [19] | South Korea | The Korea National Health and Nutrition Examination Survey | ≥19 | Male and female | 5136 | 1288 | Age, energy intake, and alcohol frequency (only in males) |
| Moore-Schiltz, 2015 [20] | U.S. | National Health and Nutrition Examination Survey (2001–2010) | ≥20 | Male and female | 9148 | 3577 | Age, sex, ethnicity, education, household income, total energy intake, fiber intake, and calcium intake |
| Gohari-Kahou, 2020 [27] | Iran | Mashhad Stroke and Heart Atherosclerotic Disorder study | 35–65 | Male and female | 853 | 269 | Age, sex, and BMI |
| Yang, 2020 [21] | China | The China Health and Nutrition Survey | ≥18 | Male and female | 8120 | 2168 | Age, sex, total energy intake, smoking, current alcohol consumption, education level, residence, and intake of protein, carbohydrate, and fat |
| Zhu, 2020 [22] | China | China Nutrition and Health Survey and Shanghai Diet and Health Survey | ≥18 | Male and female | 5323 | 1836 | Age, sex, region, years of education, physical activity level, intended physical exercises, smoking, alcohol use, daily energy intake, iron, and zinc |
| Alkazemi, 2024 [26] | Kuwait | NA | 18–65 | Female | 170 | 41 | Age, regular menses, and BMI |
| First Author, Year | Country | Study Design | Study Name | Age at Baseline (Years) | Sex | Study Size | Adjustment for Covariates | |
|---|---|---|---|---|---|---|---|---|
| Subjects | No. of Cases | |||||||
| Addin, 2024 [31] | Germany | Cohort | KORA (Cooperative Health Research in the Region of Augsburg) Survey | 32–81 | Male and female | 1358 | 232 | Age, sex, smoking, physical activity, alcohol consumption, serum potassium, and diuretic medication |
| Guerrero-Romero, 2002 [28] | Mexico | Case-control | NA | 42.3 (cases) 41.5 (controls) | Male and female | 384 | 192 | Age and the homeostasis model assessment of insulin resistance (HOMA-IR) index |
| Guerrero-Romero, 2006 [29] | Mexico | Case-control | NA | 44.0 (cases) 43.0 (control) | Male and female | 441 | 147 | Age, sex, BMI, waist-to-hip ratio, total adiposity, C-reactive protein, and malondialdehyde |
| Yuan, 2016 [30] | China | Case-control | NA | 64.0 (cases) 64.1 (controls) | Male and female | 408 | 204 | Age and sex |
| Zhang, 2020 [35] | China | Case-control | NA | 60.1 (cases) 59.9 (controls) | Male and female | 4134 | 2095 | Age, sex, education level, smoking, alcohol intake, BMI, physical activity, and family history of disease |
| Song, 2012 [34] | South Korea | Cross-sectional | NA | 37.6; mean | Male and female | 514 | 35 | Age, sex, exercise, smoking, and drinking |
| Gohari-Kahou, 2020 [27] | Iran | Cross-sectional | Mashhad Stroke and Heart Atherosclerotic Disorder Study | 35–65 | Male and female | 853 | 269 | Age, sex, and BMI |
| Alkazemi, 2022 [36] | Kuwait | Cross-sectional | Al-Addan Hospital and Mubarak Al-Kabeer Hospital | 18–65 | Male and female | 231 | 51 | Age, nationality, education level, employment status, total annual income, menstrual cycle (for women), BMI, and physical activity |
| Huang, 2022 [37] | China | Cross-sectional | The Eighth Affiliated Hospital of Sun Yat-Sen University | 59.22; mean | Male and female | 1274 | 149 | Age, sex, smoking, drinking, and estimate glomerular filtration rate |
| Ngu, 2022 [38] | Taiwan | Cross-sectional | NA | 20–64 | Male and female | 150 | 40 | Age, gender, BMI, and smoking |
| Yang, 2024 [32] | China | Cross-sectional | China Nutrition and Health Surveillance 2015–2017 | ≥45 | Male and female | 2101 | NA | Age, sex, education, nationality, area, residence, BMI, and heart rate |
| Addin, 2024 [31] | Germany | Cross-sectional | KORA (Cooperative Health Research in the Region of Augsburg) Survey | 32–81 | Male and female | 2609 | 817 | Age, sex, smoking status, physical activity, alcohol consumption, serum potassium, and diuretic medication |
| Alsheikh, 2025 [33] | Qatar | Cross-sectional | Qatar Biobank Study | ≥20 | Male and female | 9389 | 1929 | Age, sex, smoking, physical activity, diet, and education |
| Factor | No. of Studies | OR | 95% CIs | p for Difference |
|---|---|---|---|---|
| All studies | 12 | 0.61 | 0.39–0.94 | |
| Stratified by sex | ||||
| Male | 2 | 0.77 | 0.59–1.01 | 0.55 |
| Female | 4 | 0.69 | 0.58–0.83 | |
| Stratified by geographical region | ||||
| U.S. | 5 | 0.71 | 0.60–0.84 | |
| Asia | 3 | 0.49 | 0.10–2.53 | 0.67 a |
| Middle East | 3 | 0.66 | 0.39–1.11 | 0.99 a |
| Europe | 1 | 0.97 | 0.59–1.61 | 0.63 a |
| Sample size | ||||
| ≥Median | 6 | 0.57 | 0.28–1.15 | 0.73 |
| <Median | 6 | 0.69 | 0.51–0.95 | |
| Adjustment for smoking | ||||
| Yes | 6 | 0.52 | 0.20–1.33 | 0.46 |
| No | 6 | 0.75 | 0.62–0.89 | |
| Adjustment for alcohol | ||||
| Yes | 7 | 0.56 | 0.25–1.24 | 0.65 |
| No | 5 | 0.72 | 0.58–0.89 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Je, Y. Intake or Blood Levels of Magnesium and Risk of Metabolic Syndrome: A Meta-Analysis of Observational Studies. Nutrients 2025, 17, 1667. https://doi.org/10.3390/nu17101667
Kim Y, Je Y. Intake or Blood Levels of Magnesium and Risk of Metabolic Syndrome: A Meta-Analysis of Observational Studies. Nutrients. 2025; 17(10):1667. https://doi.org/10.3390/nu17101667
Chicago/Turabian StyleKim, Youngyo, and Youjin Je. 2025. "Intake or Blood Levels of Magnesium and Risk of Metabolic Syndrome: A Meta-Analysis of Observational Studies" Nutrients 17, no. 10: 1667. https://doi.org/10.3390/nu17101667
APA StyleKim, Y., & Je, Y. (2025). Intake or Blood Levels of Magnesium and Risk of Metabolic Syndrome: A Meta-Analysis of Observational Studies. Nutrients, 17(10), 1667. https://doi.org/10.3390/nu17101667