
Psychometric Properties of the Turkish Version of the Soft Drink Addiction Scale


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measurements
2.2.1. Soft Drink Addiction Scale
2.2.2. BEVQ-15
2.2.3. Soft Drink Self-Efficacy and Attitude Toward Alternatives
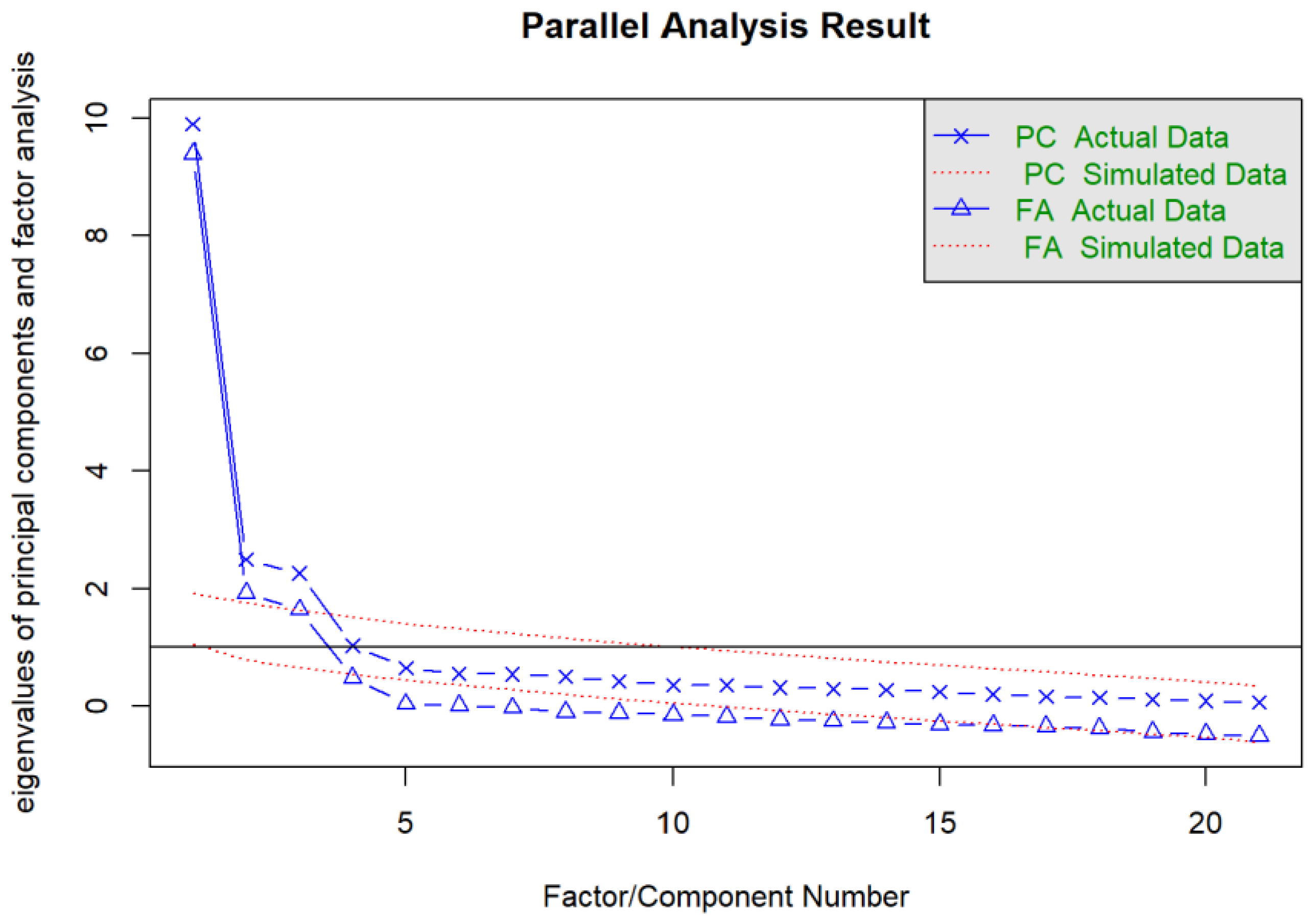
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- British Soft Drink Association. UK Soft Drinks Annual Report 2024. Available online: https://www.britishsoftdrinks.com/write/MediaUploads/BSDAAnnualReport2024.pdf (accessed on 3 September 2024).
- Statista. Soft Drinks—Worldwide. Available online: https://www.statista.com/outlook/cmo/non-alcoholic-drinks/soft-drinks/worldwide (accessed on 3 September 2024).
- Union of Chambers and Commodity Exchanges of Turkiye. Türkiye Food Sector Compilation Report. Available online: https://www.tobb.org.tr/Documents/yayinlar/2024/TürkiyeGıdaSektörDerlemeRaporu.pdf (accessed on 3 September 2024).
- Luger, M.; Lafontan, M.; Bes-Rastrollo, M.; Winzer, E.; Yumuk, V.; Farpour-Lambert, N. Sugar-Sweetened Beverages and Weight Gain in Children and Adults: A Systematic Review from 2013 to 2015 and a Comparison with Previous Studies. Obes. Facts 2017, 10, 674–693. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; O'Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015, 351, h3576. [Google Scholar] [CrossRef] [PubMed]
- Torres-Ibarra, L.; Rivera-Paredez, B.; Hernández-López, R.; Canto-Osorio, F.; Sánchez-Romero, L.M.; López-Olmedo, N.; González-Morales, R.; Ramírez, P.; Salmerón, J.; Barrientos-Gutiérrez, T. Regular consumption of soft drinks is associated with type 2 diabetes incidence in Mexican adults: Findings from a prospective cohort study. Nutr. J. 2020, 19, 126. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.S.V.; Vegi, A.S.F.; Meireles, A.L.; Machado, Í.E.; de Menezes, M.C. Burden of non-communicable chronic diseases attributable to the consumption of sugar-sweetened beverage, 1990–2019. Clin. Nutr. ESPEN 2022, 51, 253–261. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Malcangi, G.; Ferrante, L.; Del Vecchio, G.; Viapiano, F.; Mancini, A.; Inchingolo, F.; Inchingolo, A.D.; Di Venere, D.; Dipalma, G.; et al. Damage from carbonated soft drinks on enamel: A systematic review. Nutrients 2023, 15, 1785. [Google Scholar] [CrossRef]
- Yen, C.; Huang, Y.L.; Chung, M.; Chen, Y.C. Sugar Content and Warning Criteria Evaluation for Popular Sugar-Sweetened Beverages in Taipei, Taiwan. Nutrients 2022, 14, 3339. [Google Scholar] [CrossRef]
- Terry-McElrath, Y.M.; O'Malley, P.M.; Johnston, L.D. Energy drinks, soft drinks, and substance use among United States secondary school students. J. Addict. Med. 2014, 8, 6–13. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-V); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Volkow, N.D.; Wang, G.J.; Tomasi, D.; Baler, R.D. Obesity and addiction: Neurobiological overlaps. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2013, 14, 2–18. [Google Scholar] [CrossRef]
- Avena, N.M.; Rada, P.; Hoebel, B.G. Evidence for sugar addiction: Behavioral and neurochemical effects of intermittent, excessive sugar intake. Neurosci. Biobehav. Rev. 2008, 32, 20–39. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Davis, C.; Kuschner, R.; Brownell, K.D. The addiction potential of hyperpalatable foods. Curr. Drug Abus. Rev. 2011, 4, 140–145. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; O'Keefe, J.H.; Wilson, W.L. Sugar addiction: Is it real? A narrative review. Br. J. Sports Med. 2018, 52, 910–913. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Song, J.; MacGregor, G.A.; He, F.J. Consumption of Soft Drinks and Overweight and Obesity Among Adolescents in 107 Countries and Regions. JAMA Netw. Open 2023, 6, e2325158. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; He, H.; Zhang, Q.; Wu, H.; Du, H.; Liu, L.; Wang, C.; Shi, H.; Xia, Y.; Guo, X.; et al. Soft drink consumption is associated with depressive symptoms among adults in China. J. Affect. Disord. 2015, 172, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Kadel, P.; Schneider, S.; Mata, J. Soft drink consumption and mental health problems: Longitudinal relations in children and adolescents. Soc. Sci. Med. 2020, 258, 113123. [Google Scholar] [CrossRef]
- Campos-Ramírez, C.; Camacho-Calderon, N.; Villagran-Herrera, M.E.; Aguilar-Galarza, A.; Anaya-Loyola, M.A.; Palacios-Delgado, J. Soft Drink Addiction Scale: Reliability and Validity Analysis in Young Mexican People. Beverages 2024, 10, 15. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. How to use a Monte Carlo study to decide on sample size and determine power. Struct. Equ. Model. 2002, 9, 599–620. [Google Scholar] [CrossRef]
- Hedrick, V.E.; Savla, J.; Comber, D.L.; Flack, K.D.; Estabrooks, P.A.; Nsiah-Kumi, P.A.; Ortmeier, S.; Davy, B.M. Development of a brief questionnaire to assess habitual beverage intake (BEVQ-15): Sugar-sweetened beverages and total beverage energy intake. J. Acad. Nutr. Diet. 2012, 112, 840–849. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Development of the Yale Food Addiction Scale Version 2.0. Psychol. Addict. Behav. 2016, 30, 113. [Google Scholar] [CrossRef]
- Glynn, S.M.; Ruderman, A.J. The development and validation of an Eating Self-Efficacy Scale. Cogn. Ther. Res. 1986, 10, 403–420. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 4 September 2024).
- Larsson, F.; Engström, Å.; Strömbäck, U.; Gustafsson, S. Development and psychometric evaluation of the feeling safe during surgery scale. Nurs. Open 2021, 8, 2452–2460. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. Psychol. Assess. 1995, 7, 309–319. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Yockey, R.D. SPSS Demystified: A Simple Guide and Reference, 4th ed.; Taylor & Francis: New York, NY, USA, 2023. [Google Scholar]
- Lim, S.; Jahng, S. Determining the number of factors using parallel analysis and its recent variants. Psychol. Methods 2019, 24, 452–467. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Merenda, P.F. A guide to the proper use of factor analysis in the conduct and reporting of research: Pitfalls to avoid. Meas. Eval. Couns. Dev. 1997, 30, 156–164. [Google Scholar] [CrossRef]
- Friis, K.; Lyng, J.I.; Lasgaard, M.; Larsen, F.B. Energy drink consumption and the relation to socio-demographic factors and health behaviour among young adults in Denmark. A population-based study. Eur. J. Public Health 2014, 24, 840–844. [Google Scholar] [CrossRef]
- Mies, G.W.; Treur, J.L.; Larsen, J.K.; Halberstadt, J.; Pasman, J.A.; Vink, J.M. The prevalence of food addiction in a large sample of adolescents and its association with addictive substances. Appetite 2017, 118, 97–105. [Google Scholar] [CrossRef]
- Marlatt, G.A.; Baer, J.S.; Quigley, L.A. 10. Self-efficacy and addictive behavior. In Selfefficacy in Changing Societies; Cambridge University Press: Cambridge, UK, 1997; pp. 289–315. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IA and EFA Group (n = 339) | CFA Group (n = 330) | p | Total | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Sex | |||||||
| Female | 314 | 92.63 | 313 | 94.85 | 0.305 a | 627 | 93.72 |
| Male | 25 | 7.37 | 17 | 5.15 | 42 | 6.28 | |
| Educational Level | |||||||
| Primary school | 2 | 0.59 | 0 | 0.00 | 0.464 b | 2 | 0.30 |
| Secondary school | 2 | 0.59 | 2 | 0.61 | 4 | 0.60 | |
| High school | 23 | 6.78 | 18 | 5.45 | 41 | 6.13 | |
| Bachelor’s degree | 214 | 63.13 | 206 | 62.42 | 420 | 62.78 | |
| MSc/PhD | 98 | 28.91 | 104 | 31.52 | 202 | 30.19 | |
| Occupation | |||||||
| Civil servant | 68 | 20.06 | 68 | 20.61 | 0.214 c | 136 | 20.33 |
| Retired | 16 | 4.72 | 7 | 2.12 | 23 | 3.44 | |
| Housewife | 22 | 6.49 | 11 | 3.33 | 33 | 4.93 | |
| Self-employed | 35 | 10.32 | 45 | 13.64 | 80 | 11.96 | |
| Private sector employee | 116 | 34.22 | 117 | 35.45 | 233 | 34.83 | |
| Student | 54 | 15.93 | 53 | 16.06 | 107 | 15.99 | |
| Unemployed | 28 | 8.26 | 29 | 8.79 | 57 | 8.52 | |
| Marital Status | |||||||
| Single | 150 | 42.25 | 155 | 46.97 | 0.529 c | 305 | 45.59 |
| Married | 189 | 58.75 | 175 | 53.03 | 364 | 54.41 | |
| Smoking Status | |||||||
| Yes | 96 | 28.32 | 84 | 25.45 | 0.454 c | 180 | 26.91 |
| No | 243 | 71.68 | 246 | 74.55 | 489 | 73.09 | |
| 150 min exercise per week | |||||||
| Yes | 138 | 40.71 | 124 | 37.58 | 0.453 c | 262 | 39.16 |
| No | 201 | 59.29 | 206 | 62.42 | 407 | 60.84 | |
| Lifestyle | |||||||
| I am single and live with my child/children | 9 | 2.65 | 11 | 3.33 | 0.430 c | 20 | 2.99 |
| I live with roommates | 10 | 2.95 | 13 | 3.94 | 23 | 3.44 | |
| I am not married and live with family members | 95 | 28.02 | 98 | 29.70 | 193 | 28.85 | |
| I live with a spouse/partner, and we have a child | 145 | 42.77 | 121 | 36.67 | 266 | 39.76 | |
| I live with a spouse/partner, and we have no children | 45 | 13.27 | 58 | 17.58 | 103 | 15.40 | |
| I live alone | 35 | 10.32 | 29 | 8.79 | 64 | 9.57 | |
| Min–Max | ± s Q2 (Q1–Q3) | Min–Max | ± s Q2 (Q1–Q3) | ||||
| Age (years) | 18–65 | 34.74 ± 9.77 34 (27–40) | 19–63 | 33.35 ± 8.66 32 (27–39) | 0.051 d | 18–65 | 34.05 ± 9.26 33 (27–40) |
| Body weight (kg) | 38–130 | 68.38 ± 15.24 65.00 (56.50–76.00) | 43–116 | 66.47 ± 13.49 63.00 (57.00–74.00) | 0.168 e | 38–130 | 67.44 ± 14.43 65 (57–75) |
| BMI (kg/m2) | 13.46–42.97 | 24.90 ± 4.93 23.99 (21.45–27.68) | 17.10–42.87 | 24.22 ± 4.55 23.36 (20.77–27.03) | 0.064 e | 146–195 | 165.55 ± 6.88 165 (160–170) |
| 13.46–42.97 | 24.56 ± 4.76 23.73 (21.11–27.25) | ||||||
| Item No. | CITC | Μ ± Σ | DI (%27) | Alpha If Deleted Any Item |
|---|---|---|---|---|
| 1 | 0.674 | 1.27 ± 0.79 | 0.935 | 0.926 |
| 2 | 0.711 | 1.22 ± 0.70 | 0.793 | 0.925 |
| 3 | 0.712 | 1.21 ± 0.67 | 0.728 | 0.925 |
| 4 | 0.770 | 1.30 ± 0.82 | 1.043 | 0.924 |
| 5 | 0.773 | 1.31 ± 0.83 | 1.109 | 0.924 |
| 6 | 0.709 | 1.23 ± 0.70 | 0.837 | 0.925 |
| 7 | 0.463 | 1.41 ± 0.84 | 0.837 | 0.930 |
| 8 | 0.674 | 1.22 ± 0.65 | 0.652 | 0.926 |
| 9 | 0.622 | 1.19 ± 0.63 | 0.598 | 0.927 |
| 10 | 0.734 | 1.22 ± 0.69 | 0.761 | 0.925 |
| 11 | 0.519 | 2.11 ± 1.28 | 2.272 | 0.932 |
| 12 | 0.483 | 1.61 ± 1.14 | 1.728 | 0.931 |
| 13 | 0.645 | 1.45 ± 0.95 | 1.391 | 0.926 |
| 14 | 0.593 | 1.43 ± 0.98 | 1.326 | 0.928 |
| 15 | 0.651 | 1.53 ± 1.00 | 1.533 | 0.926 |
| 16 | 0.685 | 1.52 ± 1.01 | 1.554 | 0.926 |
| 17 | 0.595 | 1.12 ± 0.54 | 0.435 | 0.928 |
| 18 | 0.602 | 1.07 ± 0.39 | 0.272 | 0.929 |
| 19 | 0.558 | 1.10 ± 0.47 | 0.337 | 0.929 |
| 20 | 0.587 | 1.10 ± 0.52 | 0.370 | 0.928 |
| 21 | 0.522 | 1.08 ± 0.43 | 0.283 | 0.929 |
| English and Turkish Versions of the Items | Factor 1 (Withdrawal Syndrome Symptoms) | Factor 2 (Decrease in Social and Recreational Activities) | Factor 3 (Persistent Desire) | |
|---|---|---|---|---|
| I1 | My behavior toward my soft drink consumption causes me stress or distress./Alkolsüz içecek tüketimime yönelik davranışlarım strese veya sıkıntıya neden oluyor. | −0.806 | 0.185 | −0.115 |
| I2 | I have experienced anxiety when I decrease or avoid drinking soft drinks./Alkolsüz içecekleri azalttığımda veya içmekten kaçındığımda kaygı yaşadım. | −0.819 | 0.199 | −0.186 |
| I3 | I experience agitation or any other physical symptoms when I decrease or avoid drinking soft drinks./Alkolsüz içecekleri azalttığımda veya içmekten kaçındığımda ajitasyon veya diğer fiziksel semptomlar yaşıyorum. | −0.844 | 0.161 | - |
| I4 | I drink the same types and amounts of soft drinks even when they cause me emotional trouble./Bana duygusal sıkıntı yarattıklarında bile aynı türde ve miktarda alkolsüz içecek içiyorum. | −0.819 | 0.135 | −0.26 |
| I5 | I drink soft drinks to the point where I feel bad physically./Fiziksel olarak kötü hissettiğim noktaya kadar alkolsüz içecekler içiyorum. | −0.853 | 0.106 | −0.283 |
| I6 | I must increase the regular amount of soft drinks because I have to feel satisfied./Memnun hissetmem için alkolsüz içecek miktarını artırmam gerekiyor. | −0.834 | - | −0.212 |
| I7 | I feel exhausted after drinking soft drinks in excess./Fazla alkolsüz içecekler içtikten sonra kendimi yorgun hissediyorum. | −0.560 | - | - |
| I8 | My soft drink consumption has caused me depression, anxiety, anger, or guilt./Alkolsüz içecek tüketimim depresyona, kaygıya, öfkeye veya suçluluğa neden oldu. | −0.792 | 0.182 | - |
| I9 | My soft drink consumption has caused a health problem or made one worse./Alkolsüz içecek tüketimim bir sağlık sorununa neden oldu veya daha da kötüleştirdi. | −0.546 | 0.150 | −0.161 |
| I10 | I have drunk soft drinks to avoid sensations of agitation or any other physical symptoms I live with./Ajitasyon hissinden veya birlikte yaşadığım diğer cziksel semptomlardan kaçınmak için alkolsüz içecekler içtim. | −0.613 | 0.208 | −0.308 |
| I11 | I drink soft drinks with most of the meals I have during the day./Gün içinde yediğim öğünlerin çoğuyla birlikte alkolsüz içecekler içerim. | −0.113 | - | −0.646 |
| I12 | My soft drink consumption is high; however, I do not consider it an issue./Alkolsüz içecek tüketimim yüksek ama bunu bir sorun olarak görmüyorum. | −0.155 | - | −0.687 |
| I13 | I drink soft drinks even when I am not thirsty anymore./Artık susamadığım zamanlarda bile alkolsüz içecekler içerim. | −0.136 | 0.200 | −0.747 |
| I14 | When soft drinks are not available, I attempt to obtain them even if I have other options, such as regular or flavored water./Alkolsüz içecekler mevcut olmadığında, normal veya aromalı su gibi başka seçeneklerim olsa bile onları almaya çalışıyorum. | −0.128 | 0.272 | −0.664 |
| I15 | When I am drinking soft drinks, I end up having more than I had planned./Alkolsüz içecekler içerken, planladığımdan daha fazlasını alıyorum. | −0.191 | 0.211 | −0.659 |
| I16 | I experience a significant craving or urgency to consume soft drinks when I have decreased or avoided its consumption./Alkolsüz içecek tüketimini azalttığımda veya tüketimden kaçındığımda büyük bir özlemim veya isteğim var. | −0.211 | 0.208 | −0.685 |
| I17 | I avoid certain social/professional situations because there will not be soft drinks available./Bazı sosyal/profesyonel desteklerden kaçınıyorum çünkü alkolsüz içecekler olmayacak. | −0.197 | 0.665 | −0.278 |
| I18 | My soft drink consumption is such that I stop performing activities, including working, spending time with my family/friends, and other activities I like./Alkolsüz içecek tüketimim nedeniyle çalışmak, ailemle/arkadaşlarımla vakit geçirmek ve sevdiğim aktiviteleri yapmayı bırakıyorum. | −0.227 | 0.848 | −0.189 |
| I19 | I have avoided certain family, social, or professional situations where there will be soft drinks available because I am afraid of drinking in excess./Fazla içmekten korktuğum için alkolsüz içeceklerin bulunacağı belirli aile, sosyal veya profesyonel desteklerden kaçındım. | −0.19 | 0.815 | −0.185 |
| I20 | My soft drink consumption is such that I experience depression, anxiety, anger, or guilt in such a way that I stop performing activities, including working, spending time with my family/friends, or other activities I like./Alkolsüz içecek tüketimim nedeniyle depresyon, kaygı, öfke veya suçluluk duyuyorum, bu nedenle çalışmak, ailemle/arkadaşlarımla vakit geçirmek veya sevdiğim diğer aktiviteler gibi aktiviteler yapmayı bırakıyorum. | −0.272 | 0.819 | −0.134 |
| I21 | I experience issues with my work and school skills, family, or social activities owing to my soft drink consumption./Alkolsüz içecek tüketimim nedeniyle iş ve okul becerilerim, ailem veya sosyal aktivitelerimle ilgili sorunlar yaşıyorum. | - | 0.767 | −0.188 |
| Fit Index and Thresholds Used | Analysis Value | ||||
|---|---|---|---|---|---|
| χ2/df ≤ 5.00 | 2.446 | ||||
| χ2/df using the Yuan–Bentler correction ≤ 2.00 | 1.574 | ||||
| 0.90 ≤ CFI ≤ 1.00 | 0.936 | ||||
| 0.90 ≤ Robust CFI ≤ 1.00 | 0.947 | ||||
| 0.90 ≤ TLI ≤ 1.00 | 0.918 | ||||
| 0.90 ≤ Robust TLI ≤ 1.00 | 0.932 | ||||
| RMSEA < 0.08 | 0.042 | ||||
| Robust RMSEA < 0.08 | 0.067 | ||||
| sRMR < 0.08 | 0.039 | ||||
| 0.85 ≤ GFI ≤ 1.00 | 0.909 | ||||
| 0.85 ≤ AGFI ≤ 1.00 | 0.857 | ||||
| Item | Standardized Factor Loading Bifactor S Model | Standardized Factor Loading Bifactor G Model | |||
| Withdrawal Syndrome Symptoms | Persistent Desire | Decrease in Social and Recreational Activities | Soft Drink Addiction | ||
| I1 | 0.780 *** | - | - | 0.767 *** | |
| I2 | 0.852 *** | - | - | 0.838 *** | |
| I3 | 0.814 *** | - | - | 0.811 *** | |
| I4 | 0.755 *** | - | - | 0.767 *** | |
| I5 | 0.900 *** | - | - | 0.872 *** | |
| I6 | 0.903 *** | - | - | 0.863 *** | |
| I7 | 0.583 *** | - | - | 0.583 *** | |
| I8 | 0.730 *** | - | - | 0.727 *** | |
| I9 | 0.711 *** | - | - | 0.720 *** | |
| I10 | 0.766 *** | - | - | 0.755 *** | |
| I11 | - | 0.586 *** | - | 0.383 *** | |
| I12 | - | 0.594 *** | - | 0.372 *** | |
| I13 | - | 0.726 *** | - | 0.465 *** | |
| I14 | - | 0.794 *** | - | 0.504 *** | |
| I15 | - | 0.833 *** | - | 0.563 *** | |
| I16 | - | 0.781 *** | - | 0.574 *** | |
| I17 | - | - | 0.674 *** | 0.536 *** | |
| I18 | - | - | 0.819 *** | 0.381 ** | |
| I19 | - | - | 0.651 *** | 0.338 * | |
| I20 | - | - | 0.854 *** | 0.451 ** | |
| I21 | - | - | 0.620 *** | 0.337 ** | |
| Factors | CR | AVE | CA | ||
| Withdrawal Syndrome Symptoms | 0.967 | 0.750 | 0.943 | ||
| Persistent Desire | 0.845 | 0.481 | 0.872 | ||
| Decrease in Social and Recreational Activities | 0.976 | 0.894 | 0.848 | ||
| Beverage Addiction | 0.954 | 0.518 | 0.917 | ||
| n | WSS | PD | DSRA | SDA | |
|---|---|---|---|---|---|
| Q2 (Q1–Q3) | Q2 (Q1–Q3) | Q2 (Q1–Q3) | Q2 (Q1–Q3) | ||
| Sex | |||||
| Female | 627 | 10.00 (10.00–12.00) | 8.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.00–29.00) |
| Male | 42 | 10.00 (10.00–10.00) | 9.50 (6.00–15.50) | 5.00 (5.00–5.00) | 24.50 (21.00–33.00) |
| z | −1.512 | −1.815 | −0.837 | −0.793 | |
| p | 0.130 | 0.070 | 0.403 | 0.428 | |
| Educational Level | |||||
| High school and below | 47 | 10.00 (10.00–13.00) | 7.00 (6.00–13.00) | 5.00 (5.00–5.00) | 23.00 (21.00–31.50) |
| Bachelor’s degree | 420 | 10.00 (10.00–12.00) | 8.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.00–30.00) |
| MSc and PhD | 202 | 10.00 (10.00–12.00) | 7.50 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.25–29.00) |
| χ2 | 1.485 | 0.115 | 1.756 | 0.077 | |
| p | 0.476 | 0.944 | 0.416 | 0.962 | |
| Post hoc | - | - | - | - | |
| Occupation | |||||
| Student | 107 | 10.00 (10.00–12.00) | 9.00 (7.00–14.00) | 5.00 (5.00–5.00) | 26.00 (22.50–34.00) |
| Private sector employee | 233 | 10.00 (10.00–12.00) | 8.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (22.00–29.00) |
| Unemployed | 57 | 10.00 (10.00–13.00) | 8.00 (6.00–12.00) | 5.00 (5.00–5.00) | 24.00 (21.00–35.00) |
| Self-employed | 80 | 10.00 (10.00–11.25) | 7.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.00–28.25) |
| Civil servant | 136 | 10.00 (10.00–11.00) | 7.00 (6.00–10.00) | 5.00 (5.00–5.00) | 23.00 (21.00–26.25) |
| Housewife | 33 | 11.00 (10.00–12.00) | 7.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.00–30.00) |
| Retired | 23 | 10.00 (10.00–10.00) | 6.00 (6.00–8.50) | 5.00 (5.00–5.00) | 21.00 (21.00–23.50) |
| χ2 | 10.586 | 21.198 | 9.409 | 23.277 | |
| p | 0.102 | 0.002 ** | 0.152 | <0.001 *** | |
| Post hoc | - | a > b, c, d, e, f, g b > g | - | a, b, c, d, e, f > g a > b, d, e | |
| Marital Status | |||||
| Single | 305 | 10.00 (10.00–12.00) | 8.00 (6.00–13.00) | 5.00 (5.00–5.00) | 24.00 (21.00–32.00) |
| Married | 364 | 10.00 (10.00–12.00) | 7.00 (6.00–10.00) | 5.00 (5.00–5.00) | 23.00 (21.00–27.00) |
| z | −0.640 | −3.409 | −1.541 | −2.995 | |
| p | 0.522 | <0.001 *** | 0.123 | 0.003 ** | |
| Smoking Status | |||||
| Yes | 180 | 10.00 (10.00–13.00) | 8.00 (6.00–11.00) | 5.00 (5.00–5.00) | 24.00 (21.75–31.25) |
| No | 489 | 10.00 (10.00–11.00) | 8.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.00–29.00) |
| z | −2.495 | −0.506 | −0.541 | −1.450 | |
| p | 0.013 * | 0.613 | 0.589 | 0.147 | |
| 150 min exercise per week | |||||
| Yes | 407 | 10.00 (10.00–12.00) | 8.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.00–29.00) |
| No | 262 | 10.00 (10.00–12.00) | 7.00 (6.00–11.00) | 5.00 (5.00–5.00) | 23.00 (21.00–30.00) |
| z | −0.183 | −0.675 | −0.203 | −0.352 | |
| p | 0.855 | 0.500 | 0.839 | 0.725 | |
| Lifestyle | |||||
| I am not married and live with family members.a | 193 | 10.00 (10.00–11.00) | 8.00 (6.00–13.00) | 5.00 (5.00–5.00) | 24.00 (22.00–32.00) |
| I live with my roommates b | 23 | 10.00 (10.00–11.50) | 9.00 (6.00–15.50) | 5.00 (5.00–5.00) | 25.00 (21.00–36.50) |
| I live with a spouse/partner, and we have no children c | 103 | 10.00 (10.00–13.00) | 8.00 (6.00–11.50) | 5.00 (5.00–5.00) | 24.00 (22.00–30.50) |
| I live alone d | 64 | 10.00 (10.00–12.25) | 8.00 (6.00–12.25) | 5.00 (5.00–5.00) | 24.50 (21.00–32.00) |
| I live with a spouse/partner, and we have a child e | 266 | 10.00 (10.00–11.75) | 7.00 (6.00–9.75) | 5.00 (5.00–5.00) | 23.00 (21.00–27.00) |
| I am single and live with my child/children f | 20 | 10.00 (10.00–11.00) | 6.50 (6.00–8.00) | 5.00 (5.00–5.00) | 22.00 (21.00–23.00) |
| χ2 | 2.041 | 22.984 | 4.731 | 20.025 | |
| p | 0.844 | <0.001 *** | 0.450 | 0.001 ** | |
| Post hoc | - | a, b, c, d > e, f | - | a, c, d, e > f a, c > e |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kahriman, M.; Baş, M.; Yilmaz, S. Psychometric Properties of the Turkish Version of the Soft Drink Addiction Scale. Nutrients 2025, 17, 196. https://doi.org/10.3390/nu17010196
Kahriman M, Baş M, Yilmaz S. Psychometric Properties of the Turkish Version of the Soft Drink Addiction Scale. Nutrients. 2025; 17(1):196. https://doi.org/10.3390/nu17010196
Chicago/Turabian StyleKahriman, Meryem, Murat Baş, and Salim Yilmaz. 2025. "Psychometric Properties of the Turkish Version of the Soft Drink Addiction Scale" Nutrients 17, no. 1: 196. https://doi.org/10.3390/nu17010196
APA StyleKahriman, M., Baş, M., & Yilmaz, S. (2025). Psychometric Properties of the Turkish Version of the Soft Drink Addiction Scale. Nutrients, 17(1), 196. https://doi.org/10.3390/nu17010196