Vitamin D Supplementation and Vitamin D Status during Pregnancy and the Risk of Congenital Anomalies—A Systematic Review and Meta-Analysis

 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Alterations to Protocol
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search
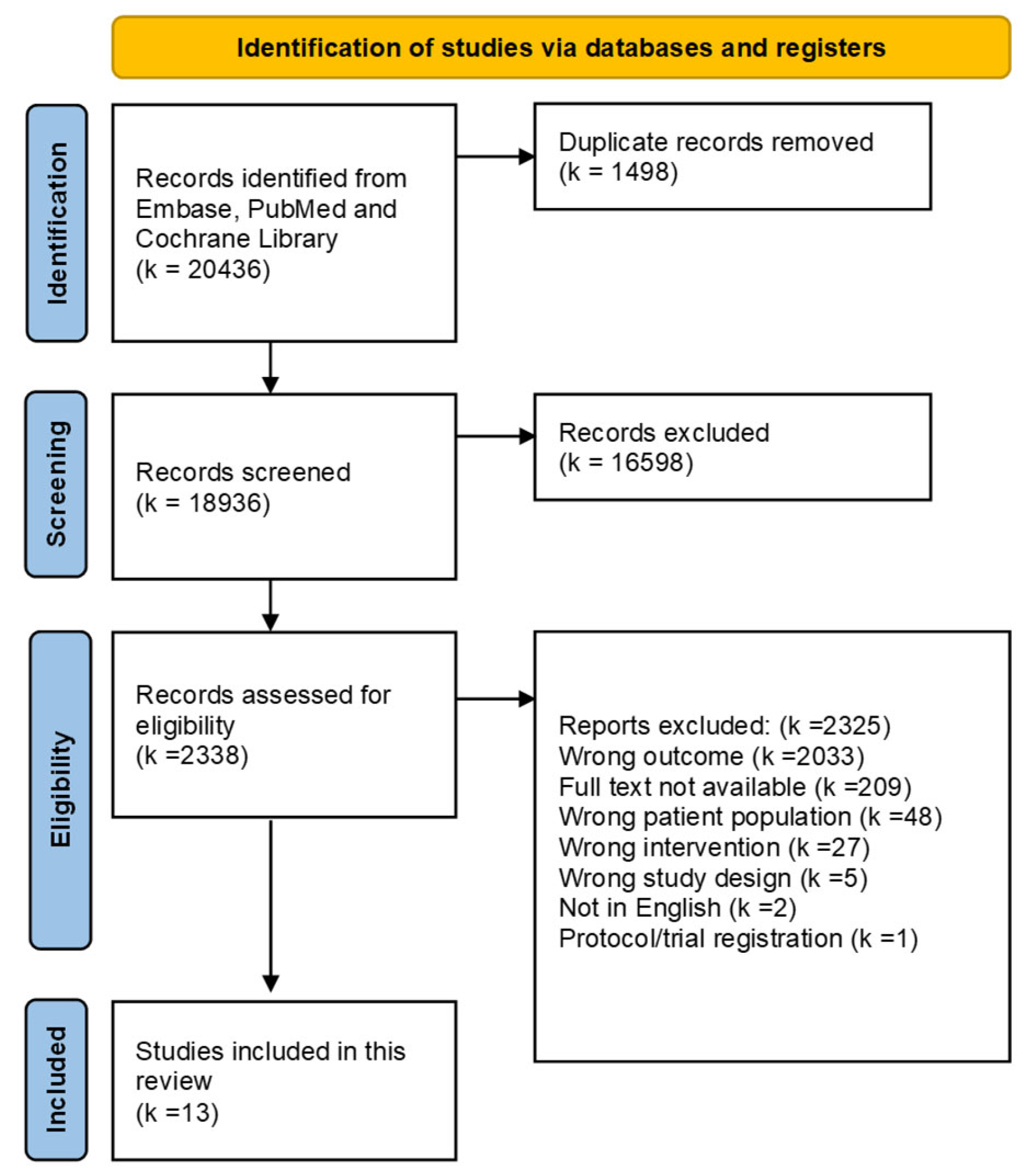
2.5. Study Selection
2.6. Data Collection
2.7. Data Items
2.8. Summary Measures and Synthesis of Results
2.9. Certainty Assessment (GRADE)
2.10. Risk of Bias in Individual Studies
3. Results
3.1. Study Characteristics
3.2. Risk of Bias within Studies
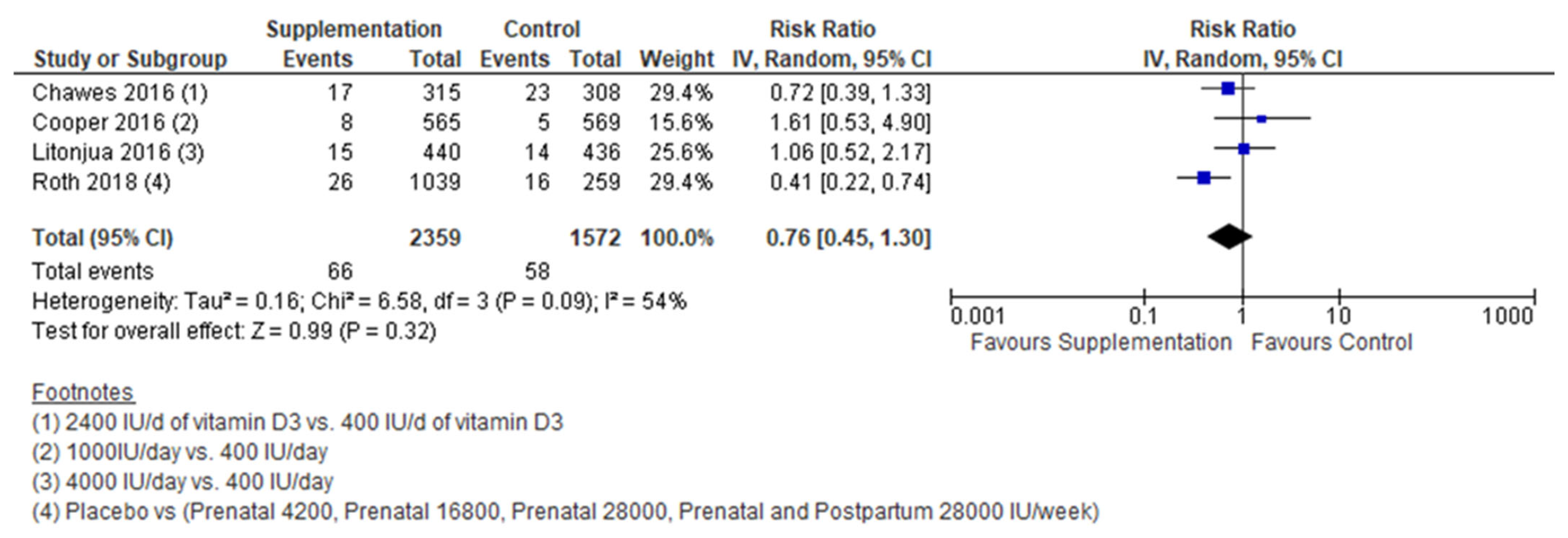
3.3. Vitamin D and Congenital Anomalies
4. Discussion
4.1. Summary of the Evidence
4.2. Strengths and Limitations of the Included Studies
4.3. Strengths and Limitations of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Congenital Anomalies. Available online: https://www.who.int/health-topics/congenital-anomalies#tab=tab_1 (accessed on 16 February 2022).
- Sarmah, S.; Muralidharan, P.; Marrs, J.A. Common congenital anomalies: Environmental causes and prevention with folic acid containing multivitamins. Birth Defects Res. C Embryo Today 2016, 108, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Botto, L.D.; Krikov, S.; Carmichae, S.L.; Munger, R.G.; Shaw, G.M.; Feldkamp, M.L. Lower rate of selected congenital heart defects with better maternal diet quality: A population-based study. Arch. Dis. Child Fetal Neonatal Ed. 2016, 101, F43–F49. [Google Scholar] [CrossRef] [PubMed]
- Imbard, A.; Benoist, J.F.; Blom, H.J. Neural Tube Defects, Folic Acid and Methylation. Int. J. Environ. Res. Public Health 2013, 10, 4352. [Google Scholar] [CrossRef] [PubMed]
- Koster, M.P.H.; van Duijn, L.; Krul-Poel, Y.H.M.; Laven, J.S.; Helbing, W.A.; Simsek, S.; Steegers-Theunissen, R.P.M. A compromised maternal vitamin D status is associated with congenital heart defects in offspring. Early Hum. Dev. 2018, 117, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Wagner, C.L.; Castracane, V.D. Understanding vitamin D metabolism in pregnancy: From physiology to pathophysiology and clinical outcomes. Metabolism 2018, 86, 112–123. [Google Scholar] [CrossRef]
- Rabbani, S.; Afaq, S.; Fazid, S.; Khattak, M.I.; Yousafzai, Y.M.; Habib, S.H.; Lowe, N.; Ul-Haq, Z. Correlation between maternal and neonatal blood Vitamin D level: Study from Pakistan. Matern. Child Nutr. 2021, 17, e13028. [Google Scholar] [CrossRef]
- VioStreym, S.; Kristine Moller, U.; Rejnmark, L.; Heickendorff, L.; Mosekilde, L.; Vestergaard, P. Maternal and infant vitamin D status during the first 9 months of infant life-a cohort study. Eur. J. Clin. Nutr. 2013, 67, 1022–1028. [Google Scholar] [CrossRef]
- Donovan, M.F.; Cascella, M. Embryology, Weeks 6–8. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2021; Bookshelf ID: NBK563181. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Risk of Bias Tools-Current Version of RoB 2. Available online: https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool/current-version-of-rob-2 (accessed on 29 April 2022).
- Chawes, B.L.; Bønnelykke, K.; Stokholm, J.; Vissing, N.H.; Bjarnadóttir, E.; Schoos, A.-M.M.; Wolsk, H.M.; Pedersen, T.M.; Vinding, R.K.; Thorsteinsdóttir, S.; et al. Effect of Vitamin D 3 Supplementation During Pregnancy on Risk of Persistent Wheeze in the Offspring A Randomized Clinical Trial. JAMA 2016, 315, 353–361. [Google Scholar] [CrossRef]
- Cooper, C.; Harvey, N.C.; Bishop, N.J.; Kennedy, S.; Papageorghiou, A.T.; Schoenmakers, I.; Fraser, R.; Gandhi, S.V.; Carr, A.; D’Angelo, S.; et al. Maternal gestational vitamin D supplementation and off spring bone health (MAVIDOS): A multicentre, double-blind, randomised placebo-controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 393–402. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Harshfield, B.J.; Mcelrath, T.F.; O’Connor, G.T.; Sandel, M.; Iverson, R.E., Jr.; Lee-Paritz, A.; Strunk, R.C.; et al. Effect of Prenatal Supplementation with Vitamin D on Asthma or Recurrent Wheezing in Offspring by Age 3 Years The VDAART Randomized Clinical Trial. JAMA 2016, 315, 362–370. [Google Scholar] [CrossRef]
- Roth, D.E.; Morris, S.K.; Zlotkin, S.; Gernand, A.D.; Ahmed, T.; Shanta, S.S.; Papp, E.; Korsiak, J.; Shi, J.; Islam, M.M.; et al. Vitamin D Supplementation in Pregnancy and Lactation and Infant Growth. N. Engl. J. Med. 2018, 379, 1174–1177. [Google Scholar] [CrossRef]
- Fernández-Alonso, A.M.; Dionis-Sánchez, E.C.; Chedraui, P.; González-Salmerón, M.D.; Pérez-López, F.R. First-trimester maternal serum 25-hydroxyvitamin D3 status and pregnancy outcome. Int. J. Gynecol. Obstet. 2012, 116, 6–9. [Google Scholar] [CrossRef]
- Zhou, J.; Su, L.; Liu, M.; Liu, Y.; Cao, X.; Wang, Z.; Xiao, H. Associations between 25-hydroxyvitamin D levels and pregnancy outcomes: A prospective observational study in southern China. Eur. J. Clin. Nutr. 2014, 68, 925–930. [Google Scholar] [CrossRef]
- Daglar, K.; Tokmak, A.; Kirbas, A.; Guzel, A.I.; Erkenekli, K.; Yucel, A.; Uygur, D. Maternal serum vitamin D levels in pregnancies complicated by neural tube defects. J. Matern. Fetal Neonatal Med. 2016, 29, 298–302. [Google Scholar] [CrossRef]
- Nasri, K.; Ben Fradj, M.K.; Feki, M.; Kaabechi, N.; Sahraoui, M.; Masmoudi, A.; Marrakchi, R.; Gaigi, S.S. Maternal 25-hydroxyvitamin D level and the occurrence of neural tube defects in Tunisia. Int. J. Gynecol. Obstet. 2016, 134, 131–134. [Google Scholar] [CrossRef]
- Ates, S.; Sevket, O.; Ozcan, P.; Ozkal, F.; Kaya, M.O.; Dane, B. Vitamin D status in the first-trimester: Effects of Vitamin D deficiency on pregnancy outcomes. Afr. Health Sci. 2016, 16, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Turkmen, G.G.; Timur, H.; Tokmak, A.; Yilmaz, Z.; Kirbas, A.; Daglar, K.; Sanhal, C.Y.; Uygur, D. Levels of serum vitamin D and calcium in pregnancies complicated with fetal congenital diaphragmatic hernia and normal pregnancies. J. Matern. Fetal Neonatal Med. 2017, 30, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Dilli, D.; Doğan, N.N.; Örün, U.A.; Koç, M.; Zenciroğlu, A.; Karademir, S.; Akduman, H. Maternal and neonatal micronutrient levels in newborns with CHD. Cardiol. Young 2018, 28, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, W.A.; Fawzy, A.; Allam, R.M.; Amer, R.M.; Hamed, M.S. Maternal vitamin D level and vitamin D receptor gene polymorphism as a risk factor for congenital heart diseases in offspring; An Egyptian case-control study. Genes Dis. 2018, 6, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Sirinoglu, H.A.; Pakay, K.; Aksoy, M.; Turan Bakırci, I.; Ozkaya, E.; Sanverdi, I. Comparison of serum folate, 25-OH vitamin D, and calcium levels between pregnants with and without fetal anomaly of neural tube origin. J. Matern. Fetal Neonatal Med. 2018, 31, 1490–1493. [Google Scholar] [CrossRef] [PubMed]
- Wald, N.; Sneddon, J.; Densem, J.; Frost, C.; Stone, R. Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar] [CrossRef]
- Giustina, A.; Bouillon, R.; Binkley, N.; Sempos, C.; Adler, R.A.; Bollerslev, J.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Heijboer, A.; et al. Controversies in Vitamin D: A Statement from the Third International Conference. JBMR Plus 2020, 4, e10417. [Google Scholar] [CrossRef]
- Wolsk, H.M.; Harshfield, B.J.; Laranjo, N.; Carey, V.J.; O’Connor, G.; Sandel, M.; Strunk, R.C.; Bacharier, L.B.; Zeiger, R.S.; Schatz, M.; et al. Vitamin D supplementation in pregnancy, prenatal 25(OH)D levels, race, and subsequent asthma or recurrent wheeze in offspring: Secondary analyses from the Vitamin D Antenatal Asthma Reduction Trial. J. Allergy Clin. Immunol. 2017, 140, 1423–1429.e5. [Google Scholar] [CrossRef]
- Bi, W.G.; Nuyt, A.M.; Weiler, H.; Leduc, L.; Santamaria, C.; Wei, S.Q. Association between Vitamin D Supplementation during Pregnancy and Offspring Growth, Morbidity, and Mortality: A Systematic Review and Meta-analysis. JAMA Pediatr. 2018, 172, 635–645. [Google Scholar] [CrossRef]
- Liu, Y.; Ding, C.; Xu, R.; Wang, K.; Zhang, D.; Pang, W.; Tu, W.; Chen, Y. Effects of vitamin D supplementation during pregnancy on offspring health at birth: A meta-analysis of randomized controlled trails. Clin. Nutr. 2022, 41, 1532–1540. [Google Scholar] [CrossRef]
- Peryer, G.; Golder, S.; Junqueira, D.R.; Vohra, S.; Loke, Y.K. Chapter 19: Adverse effects | Cochrane Training. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Version 6.3; Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 20 April 2022).
- Goldring, S.T.; Griffiths, C.J.; Martineau, A.R.; Robinson, S.; Yu, C.; Poulton, S.; Kirkby, J.C.; Stocks, J.; Hooper, R.; Shaheen, S.O.; et al. Prenatal Vitamin D Supplementation and Child Respiratory Health: A Randomised Controlled Trial. PLoS ONE 2013, 8, e66627. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Sample Size | Maternal Baseline Characteristics (Age, Body Mass Index (BMI), Smoking, Socio-Economic Status (SES), Ethnicity, Parity, and Alcohol Consumption) | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|
| Chawes, 2016 [16] | Intervention group: 295 Control group: 286 | Age (years), mean (SD) 32.3 (4.3) Smoking n (%) 46 (8) SES, educational level, n (%) Low: 45 (8) Medium: 375 (65) High: 160 (27) Parity, n (%) Primiparity: 263 (45) Remaining baseline characteristics not reported | Healthy pregnant women | Gestational age > week 26, any endocrine, cardiovascular, or nephrological disorders; or vitamin D3 (cholecalciferol) intake more than 600 IU/d. |
| Cooper, 2016 [17] | Intervention group: 565 Control group: 569 | Age (years), mean (SD) Intervention group: 30.5 (5.2) Control group: 30.5 (5.2) BMI (kg/m2), median (IQR) Intervention group: 24.7 (22.3–28.6) Control group: 25.7 (23.0–30.0) Smoking (yes), n (%) Intervention group: 44/533 (8%) Control group: 43/526 (8%) SES, educational attainment ≥A level Intervention group: 414/531 (78%) Control group: 393/522 (75%) Ethnicity, white ethnic origin, n (%) Intervention group: 499/531 (94%) Control group: 497/527 (94%) Parity, Nulliparous, n (%) Intervention group: 232/532 (44%) Control group: 230/524 (44%) Alcohol consumption not reported | Women older than 18 years, had a singleton pregnancy, had gestation of less than 17 weeks based on last menstrual period and ultrasound measurements, and were aiming to give birth at the local maternity hospital. Women with a serum 25-hydroxyvitamin D (25[OH]D) concentration of 25–100 nmol/L and serum calcium of less than 2.75 mmol/L. | Metabolic bone disease, renal stones, hyper parathyroidism, or hypercalciuria, diagnosed with cancer in the previous 10 years, unable to give informed consent or comply with the protocol, taking drugs known to interfere with foetal growth, foetal anomalies on ultrasonography, or taking more than 400 IU/day vitamin D supplementation. |
| Litonjua 2016 [18] | Intervention group: 440 Control group: 436 | Age, mean (SD) Intervention group: 27.5 (5.5) Control group: 27.3 (5.6) BMI (kg/m2) not reported Smoking All non-smokers SES, educational status, n (%) Intervention group: <High school: 66 (15) High School or technical school: 123 (28) Some college: 108 (25) College graduate or graduate school: 143 (33) Control group: <High school: 42 (10) High School or technical school: 142 (33) Some college: 105 (24) College graduate or graduate school: 147 (34) Ethnicity Intervention group: Black: 190 (43) White Hispanic: 59 (13) White non-Hispanic: 114 (26) Other: 77 (18) Control group: Black: 190 (44) White Hispanic: 61 (14) White non-Hispanic: 116 (27) Other: 69 (16) Parity not reported Alcohol consumption not reported | Women between 18 and 39 years, with estimated gestational ages of 10 and 18 weeks; who had a history of asthma, eczema, or allergic rhinitis, or whose partner (biologic father of the child) had a history of asthma, eczema, or allergic rhinitis; who was a nonsmoker; and who was English or Spanish speaking, with intent to participate for 4 years (up to the third birthday of the child). | Not reported |
| Roth, 2018 [19] | Placebo group: 259 Prenatal 4200 group: 260 Prenatal 16,800 group: 259 Prenatal 28,000 group: 260 Prenatal and Postpartum 28,000 group: 260 | Age, median (range) Placebo group: 23 (18–38) Prenatal 4200 group: 22.5 (18–40) Prenatal 16,800 group: 22 (18–35) Prenatal 28,000 group: 22 (18–38) Prenatal and Postpartum 28,000 group: 23 (18–38) Smoking not reported SES, Secondary school education complete or higher, n (%) Placebo group: 52 (20.1) Prenatal 4200 group: 70 (26.9) Prenatal 16,800 group: 51 (19.7) Prenatal 28,000 group: 58 (22.3) Prenatal and Postpartum 28,000 group: 55 (21.2) Ethnicity not reported Parity, median (range) Placebo group: 2 (0–6) Prenatal 4200 group: 2 (0–5) Prenatal 16,800 group: 2 (0–5) Prenatal 28,000 group: 2 (0–5) Prenatal and Postpartum 28,000 group: 2 (0–4) Alcohol consumption not reported | Women at 18 years or above, 17 to 24 completed weeks of gestation (i.e., 17 weeks +0 days to 24 weeks + 0 days, inclusive) based on recalled last menstrual period and/or ultrasound. Intends to reside in the trial catchment area (including Hazaribag, Azimpur, Lalbag, and Kamrangirchar) for at least 18 months. Provides written informed consent. | History of any medical condition or medications that may predispose to vitamin D sensitivity, altered vitamin D metabolism, and/or hypercalcemia, including active tuberculosis or current therapy for tuberculosis, sarcoidosis, history of renal/ureteral stones, parathyroid disease, renal or liver failure, or current use of anti-convulsants. High-risk pregnancy based on one or more of the following findings by point-of-care testing:
Currently prescribed vitamin D supplements as part of a physician’s treatment plan for vitamin D deficiency. Previous enrolment in the trial during a previous pregnancy. |
| Author, Year | Sample Size | Maternal Baseline Characteristics (Age, Body Mass Index (BMI), Smoking, Socio-Economic Status (SES), Ethnicity, Parity, and Alcohol Consumption) | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|
| Fernández-Alonso, 2012 [20] | n = 466 | Maternal baseline characteristics not reported for those who were included in the second phase analysis | Pregnant women attending their first prenatal (week 11–14 of pregnancy) visit at the Torrecárdenas Hospital, Almería, Spain. | Women with an increased risk for intrauterine foetal growth restriction, specifically hereditary or acquired thrombophilias. |
| Zhou, 2014 [21] | n = 1923 (Group A: n = 364 Group B: n = 932 Group C: n = 627) | Age (years), mean (SD) Group A: 29.2 (3.5) Group B: 29.5 (3.6) Group C: 30.3 (3.9) BMI (kg/m2), mean (SD) Group A: 20.28 (2.52) Group B: 20.44 (2.51) Group C: 20.67 (2.64) Remaining baseline characteristics not reported | Pregnant women ≥18 years of age, recruited at the hospital. Included delivery methods were normal delivery, abortion, and induced labour | Women were excluded if they did not provide informed consent; had increased liver enzymes by a factor of two or more above upper normal limits; chronic disease and tumor; if the women presented with severe infections or trauma before 13 weeks of gestation, including 13 weeks; pregnant women accompanied by severe infections, trauma, or perioperatively. Before 13 weeks of gestation, including 13 weeks, pregnant women taking corticosteroids, drug abuse (including alcohol) |
| Daglar, 2014 [22] | n = 60 (Case group: n = 30 Control group: n = 30) | Age (years), mean (SD) Case group: 26.1 (5.4) Control group: 27.9 (5.3) BMI (kg/m2), mean (SD) Case group: 26.3 (5.5) Control group: 26.1 (5.2) Smoking (yes), n (%) Case group: 4 (13.3) Control group: 3 (10) Remaining baseline characteristics not reported | Women were recruited from a referral hospital for high-risk pregnancies. The patient profile of the hospital were low–middle income socio-economic groups | Women with a known history or evidence of rheumatological or adrenal diseases, hepatic or renal failure, gestational diabetes, hypertensive disorders, and previous history of childbirth with neural tube defect were excluded from the study |
| Nasri, 2016 [23] | n = 132 (Case group: n = 68 Control group: n = 64) | Age, >30 years, n (%) Case group: 41 (60) Control group: 41 (64) Parity ≥1, n (%) Case group: 37 (54) Control group: 54 (84) Remaining baseline characteristics not reported | Pregnant women were recruited from a unit receiving all referrals of women carrying a foetus with severe neural tube defect between January 2012 and December 2013. A healthy pregnant woman with normal ultrasonography and normal obstetric history was matched to every woman presenting with a foetus with neural tube defect by date/month of conception and use of folate supplementation. | Women with hypertension, cardiac disease, atherosclerosis. |
| Ates, 2016 [24] | n = 229 | Age (years), mean (SD): 29.49 (4.879) BMI (kg/m2): 25.3 ± 4.5 Smoking (yes), n (%): 15 (6.6) SES, Education, n (%) 0–5 years: 75 (35.2) 6–8 years: 38 (17.8) =9 years: 100 (46.9) Parity Nulliparous, %: 35.5 Remaining baseline characteristics not reported | Pregnant women attending their first antenatal visit at an outpatient clinic. | Multiple pregnancies and women with a history of thyroid, parathyroid, or adrenal disease; hepatic or renal failure; metabolic bone diseases and those taking medications that might affect vitamin D metabolism. |
| Turkmen, 2017 [25] | Case group: 24 Control group: 53 | Age, mean (SD) Case group: 26.4 ± 5.7 Control group: 27.0 ± 5.1 BMI (kg/m2) Case group: 26.3 ± 4.8 Control group: 26.3 ± 3.9 Smoking n (%) Case group: 3 (12.5) Control group: 5 (9.4) SES not reported Ethnicity not reported Parity unclearly reported Alcohol consumption: exclusion criteria | Pregnant women were recruited from the high-risk pregnancy and antenatal clinics | Patients with a known history or evidence of rheumatologic or adrenal disease, hepatic or renal failure, gestational diabetes, hypertensive disorders, drug abuse, alcohol consumption, steroid use, or vitamin D supplementation were excluded from the study. |
| Dilli, 2018 [26] | Case group: 108 Control group: 103 | Age Case group: 27.4 ± 5.8 Control group: 27.3 ± 5.8 BMI (kg/m2) ≥25, n (%) Case group: 34 (31.5) Control group: 39 (37.9) Smoking n (%) Case group: 59 (54.6) Control: 54 (52.4) SES Case group: Low 58 (53.7) Medium 42 (38.8) High 8 (7.4) Control group: Low 57 (55.3) Medium 42 (40.7) High 4 (3.8) Ethnicity not reported Parity, Nulliparous, n (%) Case group: 45 (41.6) Control group: 47 (45.6) Alcohol consumption not reported | Cases born between 35–42 weeks of gestation and diagnosed with congenital heart disease within the first month of life at the tertiary neonatal intensive care unit between May 2013 and May 2015. Healthy controls were matched on gestational week, postnatal age, and sex. | Not reported |
| Mokhtar, 2018 [27] | Case group: 50 Control group: 50 | Age, median (min-max) Case group: 28 (17–38) Control group: 28 (19–37) BMI not reported Smoking not reported SES, Educational level; n (%) Case group: High: 3 (6) Medium: 19 (38) Low: 28 (56) Control group: High: 6 (12) Medium: 20 (40) Low: 24 (48) Ethnicity not reported Parity not reported Alcohol consumption not reported | Mothers giving birth to term neonates diagnosed with a congenital heart disease within the first two weeks of life recruited from a tertiary neonatal intensive care unit. Recruitment took place at Zagazig University Children’s Hospital in Egypt between January 2016 and May 2018. Control mothers were age-comparable and gave birth to age and sex harmonised term neonates with congenital heart disease. | Mothers of neonates suffering from sepsis, congenital infection, genetic syndromes, multiple congenital malformations, and mothers with a history of certain diseases, drug intake, or who experienced an infection during pregnancy. |
| Sirinoglu, 2018 [28] | Case group: 79 Control group: 99 | Age, mean (SD) Case group: 27.4 (6.03) Control group: 31.02 (6.07) BMI not reported Smoking not reported SES not reported Ethnicity not reported Parity not reported Alcohol consumption not reported | This case control study was conducted between January 2014 and April 2016 at a tertiary referral hospital. The control group were selected among gestational age-matched women who had a normal targeted ultrasound during the second trimester (during the 16th week of gestation) | Not reported |
| 1st Author, Year, Country | Vitamin D Assessment (Timing) | Analysis Method | Confounding Factors | Outcome | Key Findings | Authors’ Conclusion |
|---|---|---|---|---|---|---|
| Dilli, 2018, Turkey [26] | Maternal and infant blood (<30 days of life) | Multivariate analysis | Maternal age, multivitamin use, maternal education, socio-economic levels, maternal chronic diseases, maternal homocysteine, zinc, folate levels (ng/mL), gender of the infant. | Congenital heart disease | Odds ratio not reported for vitamin D | The authors found no significant association between vitamin D and congenital heart disease. |
| Nasri, 2016, Tunisia [23] | Maternal blood (Vitamin D was assessed ≤20 weeks of gestation for 43% of the neural tube defect group and for 42% of the control group and after 20 weeks of gestation for the remaining women) | Multivariate analysis | Odds ratios adjusted for maternal age, season of blood draw, pregnancy duration, foetal weight, gravidity, parity, and consanguinity | Neural tube defect | Odds ratio 2.34 95% CI (1.07; 5.07) p-value 0.035 | The authors found that s-25OHD < 30 nmol/L in the mother was associated with an increased risk of having a foetus with neural tube defect. |
| Zhou, 2014, China [21] | Maternal blood (16–20-weeks of gestation) | Logistic regression analysis | Odds ratios adjusted for maternal age, systolic/diastolic pressure, pre-pregnancy body mass index, and serum calcium | Malformations | Odds ratio 1.016 * 95% CI (0.984; 1.049) p-value 0.338 | The authors found no significant difference in malformations between the three groups *. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walker, K.C.; Thorsteinsdottir, F.; Christesen, H.T.; Hjortdal, V.E.; Heitmann, B.L.; Specht, I.O.; Händel, M.N. Vitamin D Supplementation and Vitamin D Status during Pregnancy and the Risk of Congenital Anomalies—A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2125. https://doi.org/10.3390/nu15092125
Walker KC, Thorsteinsdottir F, Christesen HT, Hjortdal VE, Heitmann BL, Specht IO, Händel MN. Vitamin D Supplementation and Vitamin D Status during Pregnancy and the Risk of Congenital Anomalies—A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(9):2125. https://doi.org/10.3390/nu15092125
Chicago/Turabian StyleWalker, Karen Christina, Fanney Thorsteinsdottir, Henrik Thybo Christesen, Vibeke Elisabeth Hjortdal, Berit Lilienthal Heitmann, Ina Olmer Specht, and Mina Nicole Händel. 2023. "Vitamin D Supplementation and Vitamin D Status during Pregnancy and the Risk of Congenital Anomalies—A Systematic Review and Meta-Analysis" Nutrients 15, no. 9: 2125. https://doi.org/10.3390/nu15092125
APA StyleWalker, K. C., Thorsteinsdottir, F., Christesen, H. T., Hjortdal, V. E., Heitmann, B. L., Specht, I. O., & Händel, M. N. (2023). Vitamin D Supplementation and Vitamin D Status during Pregnancy and the Risk of Congenital Anomalies—A Systematic Review and Meta-Analysis. Nutrients, 15(9), 2125. https://doi.org/10.3390/nu15092125