
Very Low and High Levels of Vitamin D Are Associated with Shorter Leukocyte Telomere Length in 148,321 UK Biobank Participants

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. UK Biobank
2.2. Data
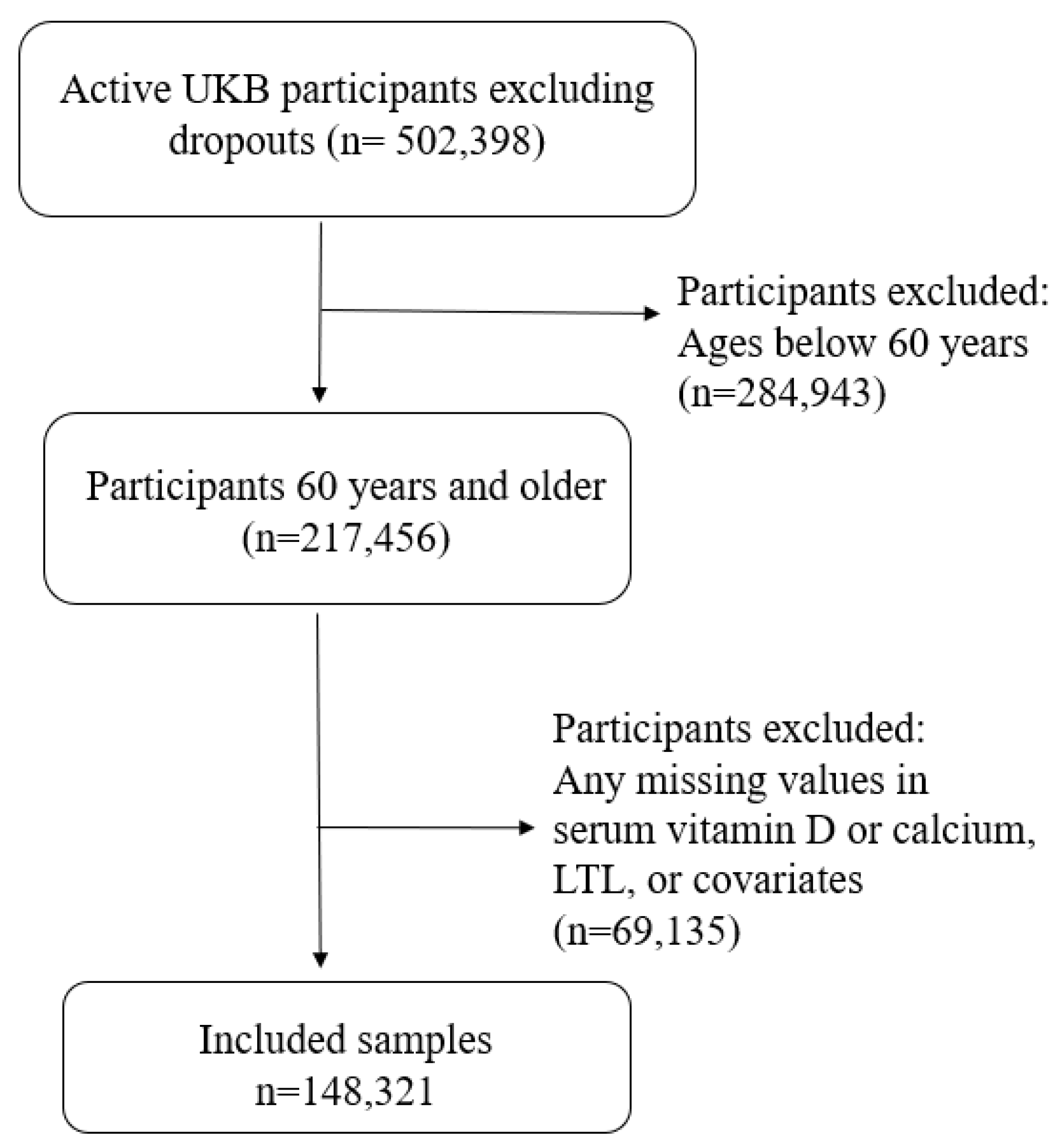
2.3. Inclusion and Exclusion Criteria
2.4. Leukocyte Telomere Length
2.5. Defining Serum Vitamin D Status
2.6. Covariates
2.7. Statistical Methods
3. Results
3.1. Population Characteristics
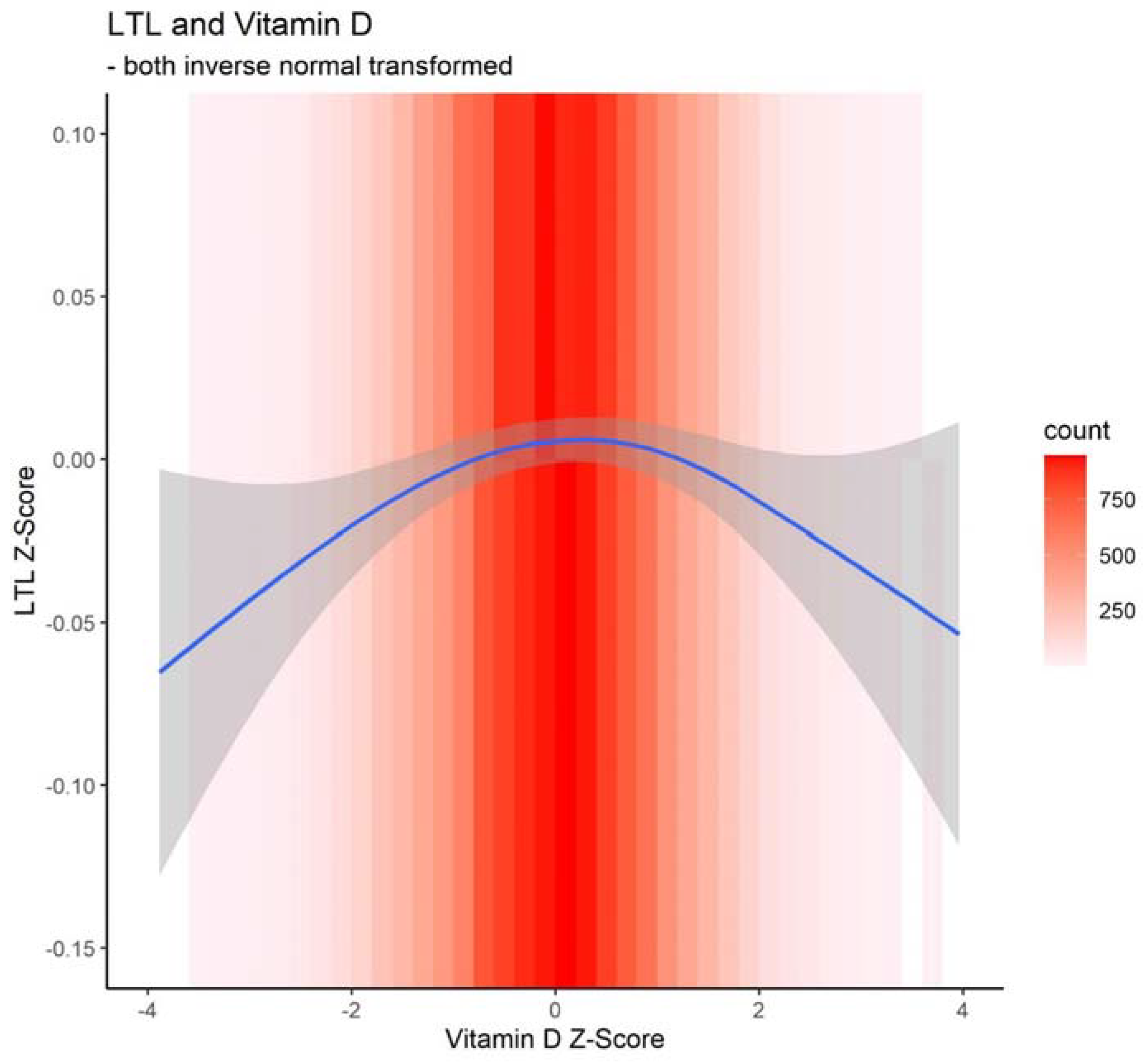
3.2. Associations between Telomere Length and Serum 25OHD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. Hallmarks of aging: An expanding universe. Cell 2023, 186, 243–278. [Google Scholar] [CrossRef] [PubMed]
- Gruber, H.J.; Semeraro, M.D.; Renner, W.; Herrmann, M. Telomeres and Age-Related Diseases. Biomedicines 2021, 9, 1335. [Google Scholar] [CrossRef]
- Kirk, B.; Al Saedi, A.; Duque, G. Osteosarcopenia: A case of geroscience. Aging Med. 2019, 2, 147–156. [Google Scholar] [CrossRef]
- Lorenzi, M.; Bonassi, S.; Lorenzi, T.; Giovannini, S.; Bernabei, R.; Onder, G. A review of telomere length in sarcopenia and frailty. Biogerontology 2018, 19, 209–221. [Google Scholar] [CrossRef]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef]
- Berridge, M.J. Vitamin D deficiency accelerates ageing and age-related diseases: A novel hypothesis. J. Physiol. 2017, 595, 6825–6836. [Google Scholar] [CrossRef]
- Zarei, M.; Zarezadeh, M.; Hamedi Kalajahi, F.; Javanbakht, M.H. The Relationship Between Vitamin D and Telomere/Telomerase: A Comprehensive Review. J. Frailty Aging 2021, 10, 2–9. [Google Scholar] [CrossRef]
- Mazidi, M.; Mikhailidis, D.P.; Banach, M.; Dehghan, A. Impact of serum 25-hydroxyvitamin D 25(OH) on telomere attrition: A Mendelian Randomization study. Clin. Nutr. 2020, 39, 2730–2733. [Google Scholar] [CrossRef] [PubMed]
- Beilfuss, J.; Camargo, C.A., Jr.; Kamycheva, E. Serum 25-Hydroxyvitamin D Has a Modest Positive Association with Leukocyte Telomere Length in Middle-Aged US Adults. J. Nutr. 2017, 147, 514–520. [Google Scholar] [CrossRef]
- Liu, J.J.; Cahoon, E.K.; Linet, M.S.; Little, M.P.; Dagnall, C.L.; Higson, H.; Savage, S.A.; Freedman, D.M. Relationship between plasma 25-hydroxyvitamin D and leucocyte telomere length by sex and race in a US study. Br. J. Nutr. 2016, 116, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Karras, S.N.; Bischoff-Ferrari, H.A.; Annweiler, C.; Boucher, B.J.; Juzeniene, A.; Garland, C.F.; Holick, M.F. Do studies reporting ‘U’-shaped serum 25-hydroxyvitamin D-health outcome relationships reflect adverse effects? Dermato-Endocrinology 2016, 8, e1187349. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.D. Vitamin D and health: Can too much be harmful? Am. J. Lifestyle Med. 2009, 3, 407–408. [Google Scholar] [CrossRef]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Peakman, T.C.; UK Biobank. The UK Biobank sample handling and storage protocol for the collection, processing and archiving of human blood and urine. Int. J. Epidemiol. 2008, 37, 234–244. [Google Scholar] [CrossRef] [PubMed]
- CDC. CDC Vitamin D Standardization-Certification Program (CDC VDSCP). Available online: https://www.cdc.gov/labstandards/csp/vdscp.html (accessed on 16 March 2023).
- UK Biobank. Biomarker Assay Quality Procedures: Approaches Used to Minimise Systematic and Random Errors, 1.2 ed.; 2019; Available online: https://biobank.ctsu.ox.ac.uk/crystal/crystal/docs/biomarker_issues.pdf (accessed on 16 March 2023).
- UK Biobank. Companion Document for Serum Biomarker Data, 1st ed.; 2019; Available online: https://biobank.ndph.ox.ac.uk/showcase/showcase/docs/serum_biochemistry.pdf (accessed on 16 March 2023).
- Cassidy, S.; Chau, J.Y.; Catt, M.; Bauman, A.; Trenell, M.I. Cross-sectional study of diet, physical activity, television viewing and sleep duration in 233,110 adults from the UK Biobank; the behavioural phenotype of cardiovascular disease and type 2 diabetes. BMJ Open 2016, 6, e010038. [Google Scholar] [CrossRef]
- Bruyère, O.; Cavalier, E.; Reginster, J.Y. Vitamin D and osteosarcopenia: An update from epidemiological studies. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 498–503. [Google Scholar] [CrossRef]
- Charoenngam, N. Vitamin D and Rheumatic Diseases: A Review of Clinical Evidence. Int. J. Mol. Sci. 2021, 22, 10659. [Google Scholar] [CrossRef]
- Giudici, K.V. Nutrition and the Hallmarks of Aging. J. Nutr. Health Aging 2021, 25, 1039–1041. [Google Scholar] [CrossRef]
- Pusceddu, I.; Farrell, C.J.; Di Pierro, A.M.; Jani, E.; Herrmann, W.; Herrmann, M. The role of telomeres and vitamin D in cellular aging and age-related diseases. Clin. Chem. Lab. Med. 2015, 53, 1661–1678. [Google Scholar] [CrossRef]
- Yang, T.; Wang, H.; Xiong, Y.; Chen, C.; Duan, K.; Jia, J.; Ma, F. Vitamin D Supplementation Improves Cognitive Function Through Reducing Oxidative Stress Regulated by Telomere Length in Older Adults with Mild Cognitive Impairment: A 12-Month Randomized Controlled Trial. J. Alzheimer’s Dis. 2020, 78, 1509–1518. [Google Scholar] [CrossRef]
- Agirbasli, D.; Kalyoncu, M.; Muftuoglu, M.; Aksungar, F.B.; Agirbasli, M. Leukocyte telomere length as a compensatory mechanism in vitamin D metabolism. PLoS ONE 2022, 17, e0264337. [Google Scholar] [CrossRef]
- Tuohimaa, P. Vitamin D and aging. J. Steroid Biochem. Mol. Biol. 2009, 114, 78–84. [Google Scholar] [CrossRef]
- Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual high-dose oral vitamin D and falls and fractures in older women: A randomized controlled trial. JAMA 2010, 303, 1815–1822. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Tanabe, M. Vitamin D supplementation as a potential cause of U-shaped associations between vitamin D levels and negative health outcomes: A decision tree analysis for risk of frailty. BMC Geriatr. 2017, 17, 236. [Google Scholar] [CrossRef] [PubMed]
- Sanders, K.M.; Nicholson, G.C.; Ebeling, P.R. Is high dose vitamin D harmful? Calcif. Tissue Int. 2013, 92, 191–206. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.K.; Ima-Nirwana, S.; Chin, K.Y. Can telomere length predict bone health? A review of current evidence. Bosn. J. Basic Med. Sci. 2020, 20, 423–429. [Google Scholar] [CrossRef]
- Rippberger, P.L.; Emeny, R.T.; Mackenzie, T.A.; Bartels, S.J.; Batsis, J.A. The association of sarcopenia, telomere length, and mortality: Data from the NHANES 1999–2002. Eur. J. Clin. Nutr. 2018, 72, 255–263. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Harris, S.S. High-dose vitamin D supplementation: Too much of a good thing? JAMA 2010, 303, 1861–1862. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Luttmann-Gibson, H.; Mora, S.; Danik, J.; Bubes, V.; Copeland, T.; LeBoff, M.S.; Cook, N.R.; Lee, I.M.; Buring, J.E.; et al. Association of Body Weight With Response to Vitamin D Supplementation and Metabolism. JAMA Netw. Open 2023, 6, e2250681. [Google Scholar] [CrossRef] [PubMed]
- Fry, A.; Littlejohns, T.J.; Sudlow, C.; Doherty, N.; Adamska, L.; Sprosen, T.; Collins, R.; Allen, N.E. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants With Those of the General Population. Am. J. Epidemiol. 2017, 186, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Staley, J.R.; Burgess, S. Semiparametric methods for estimation of a nonlinear exposure-outcome relationship using instrumental variables with application to Mendelian randomization. Genet. Epidemiol. 2017, 41, 341–352. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | UK Biobank Data Field |
|---|---|
| Leukocyte telomere length (T/S ratio), adjusted for the influence of technical parameters | 22,191 |
| 25OHD (nmol/L) | 30,890 |
| Calcium (mmol/L) | 30,680 |
| Age | 21,003 |
| Sex | 31 |
| Ethnicity | 21,000 |
| Education | 6138 |
| Townsend deprivation index at recruitment | 189 |
| Whole body fat mass | 23,100 |
| Smoking status | 20,116 |
| Alcohol intake frequency | 1558 |
| International Physical Activity Questionnaire (IPAQ) activity group | 22,032 |
| Variable | Mean ± SD (Min, Max) or Frequency (%) |
|---|---|
| Leukocyte telomere length (T/S ratio), adjusted for the influence of technical parameters | 0.81 ± 0.12; (0.08, 3.72) |
| Calcium (mmol/L) | 2.38 ± 0.09; (1.19, 3.57) |
| Vitamin D (nmol/L) | 51.34 ± 20.65; (10, 276) |
| Extremely low 1 | 3333 (2.2%) |
| Low 2 | 20,191 (13.6%) |
| Medium 3 (reference) | 101,195 (68.2%) |
| Moderately high 4 | 20,215 (13.6%) |
| High 5 | 3387 (2.3%) |
| Age (years) | 64.13 ± 2.85; (60, 70) |
| Sex | |
| Female | 74,549 (50.3%) |
| Male | 73,772 (49.7%) |
| Ethnicity | |
| White | 144,292 (97.3%) |
| Black | 1048 (0.7%) |
| South Asian | 1655 (1.1%) |
| Other | 1326 (0.9%) |
| Townsend deprivation index | −1.62 ± 2.92; (−6.26, 10.59) |
| Education | |
| None | 37,779 (25.5%) |
| CSEs | 2677 (1.8%) |
| GCSEs/O-levels | 20,977 (14.1%) |
| A-levels/NVQ/HND/HNC | 22,521 (15.2%) |
| Prof. qualification (e.g., nursing, teaching) | 23,632 (15.9%) |
| College or University degree | 40,735 (27.5%) |
| Whole body fat mass (kg) | 24.9 ± 8.84; (5, 108.1) |
| Smoking status | |
| Never | 73,929 (49.8%) |
| Current | 11,739 (7.9%) |
| Previous | 62,653 (42.2%) |
| Alcohol intake frequency | |
| Never | 11,865 (8%) |
| Special occasions only | 16,934 (11.4%) |
| One to three times a month | 14,470 (9.8%) |
| Once or twice a week | 35,499 (23.9%) |
| Three or four times a week | 33,689 (22.7%) |
| Daily or almost daily | 35,864 (24.2%) |
| IPAQ group | |
| Low | 20,213 (13.6%) |
| Moderate | 67,683 (45.6%) |
| High | 60,425 (40.7%) |
| Season of assessment | |
| Spring | 43,634 (29.4%) |
| Summer | 39,583 (26.7%) |
| Fall | 35,501 (23.9%) |
| Winter | 29,603 (20.0%) |
| 95% CI | |||||
|---|---|---|---|---|---|
| Model | Beta | Lower | Upper | p-Value | Overall p-Value |
| Unadjusted | |||||
| Vitamin D | <0.001 | ||||
| Extremely low 1 | −0.053 | −0.088 | −0.019 | 0.002 | |
| Low 2 | −0.018 | −0.033 | −0.003 | 0.021 | |
| Medium 3 (reference) | |||||
| Moderately high 4 | −0.003 | −0.018 | 0.012 | 0.663 | |
| High 5 | −0.051 | −0.086 | −0.017 | 0.003 | |
| Adjusted | |||||
| Vitamin D | 0.004 | ||||
| Extremely low 1 | −0.048 | −0.083 | −0.014 | 0.006 | |
| Low 2 | −0.018 | −0.033 | −0.003 | 0.022 | |
| Medium 3 (reference) | |||||
| Moderately high 4 | −0.002 | −0.017 | 0.013 | 0.778 | |
| High 5 | −0.038 | −0.072 | −0.004 | 0.030 | |
| Serum calcium (z score) | −0.0004 | −0.006 | 0.005 | 0.869 | 0.869 |
| Age (years) | −0.030 | −0.032 | −0.028 | 1.44 × 10−234 | <0.001 |
| Sex | <0.001 | ||||
| Female | Ref | Ref | Ref | Ref | |
| Male | −0.220 | −0.231 | −0.209 | <2.2 × 10−16 | |
| Ethnicity | <0.001 | ||||
| White | Ref | Ref | Ref | Ref | |
| Black | 0.363 | 0.302 | 0.424 | 1.23 × 10−31 | |
| South Asian | −0.010 | −0.059 | 0.039 | 0.695 | |
| Other | 0.182 | 0.129 | 0.236 | 3.01 × 10−11 | |
| Townsend deprivation index | −0.001 | −0.003 | 0.001 | 0.344 | 0.344 |
| Education | <0.001 | ||||
| None | Ref | Ref | Ref | Ref | |
| CSEs | 0.012 | −0.027 | 0.051 | 0.555 | |
| GCSEs/O-levels | 0.035 | 0.018 | 0.052 | 5.02 × 10−5 | |
| A-levels/NVQ/HND/HNC | 0.032 | 0.015 | 0.048 | 1.80 × 10−4 | |
| Prof. qualification (e.g., nursing, teaching) | 0.058 | 0.042 | 0.075 | 3.35 × 10−12 | |
| College or University degree | 0.097 | 0.082 | 0.111 | 6.49 × 10−39 | |
| Whole body fat mass | −0.026 | −0.032 | −0.021 | 1.65 × 10−21 | <0.001 |
| Smoking status | <0.001 | ||||
| Never | Ref | Ref | Ref | Ref | |
| Current | −0.095 | −0.115 | −0.075 | 3.32 × 10−21 | |
| Previous | −0.024 | −0.035 | −0.013 | 1.72 × 10−5 | |
| Alcohol intake frequency | 0.714 | ||||
| Never | Ref | Ref | Ref | Ref | |
| Special occasions only | 0.002 | −0.021 | 0.025 | 0.856 | |
| One to three times a month | 0.006 | −0.018 | 0.031 | 0.602 | |
| Once or twice a week | 0.000 | −0.021 | 0.021 | 0.982 | |
| Three or four times a week | −0.007 | −0.028 | 0.014 | 0.518 | |
| Daily or almost daily | −0.007 | −0.028 | 0.015 | 0.550 | |
| IPAQ group | 0.010 | ||||
| Low | Ref | Ref | Ref | Ref | |
| Moderate | 0.024 | 0.008 | 0.039 | 0.003 | |
| High | 0.021 | 0.005 | 0.037 | 0.009 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, C.-L.; Kirk, B.; Xiang, M.; Pilling, L.C.; Kuchel, G.A.; Kremer, R.; Duque, G. Very Low and High Levels of Vitamin D Are Associated with Shorter Leukocyte Telomere Length in 148,321 UK Biobank Participants. Nutrients 2023, 15, 1474. https://doi.org/10.3390/nu15061474
Kuo C-L, Kirk B, Xiang M, Pilling LC, Kuchel GA, Kremer R, Duque G. Very Low and High Levels of Vitamin D Are Associated with Shorter Leukocyte Telomere Length in 148,321 UK Biobank Participants. Nutrients. 2023; 15(6):1474. https://doi.org/10.3390/nu15061474
Chicago/Turabian StyleKuo, Chia-Ling, Ben Kirk, Meiruo Xiang, Luke C. Pilling, George A. Kuchel, Richard Kremer, and Gustavo Duque. 2023. "Very Low and High Levels of Vitamin D Are Associated with Shorter Leukocyte Telomere Length in 148,321 UK Biobank Participants" Nutrients 15, no. 6: 1474. https://doi.org/10.3390/nu15061474
APA StyleKuo, C.-L., Kirk, B., Xiang, M., Pilling, L. C., Kuchel, G. A., Kremer, R., & Duque, G. (2023). Very Low and High Levels of Vitamin D Are Associated with Shorter Leukocyte Telomere Length in 148,321 UK Biobank Participants. Nutrients, 15(6), 1474. https://doi.org/10.3390/nu15061474