

Association of Maternal Plasma Manganese with the Risk of Spontaneous Preterm Birth: A Nested Case–Control Study Based on the Beijing Birth Cohort Study (BBCS) in China

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Definitions
2.3. Laboratory Analysis
2.4. Sample Size Estimation
2.5. Statistical Analysis
3. Results
3.1. Baseline Information
3.2. Mn Concentration in the First and Third Trimesters
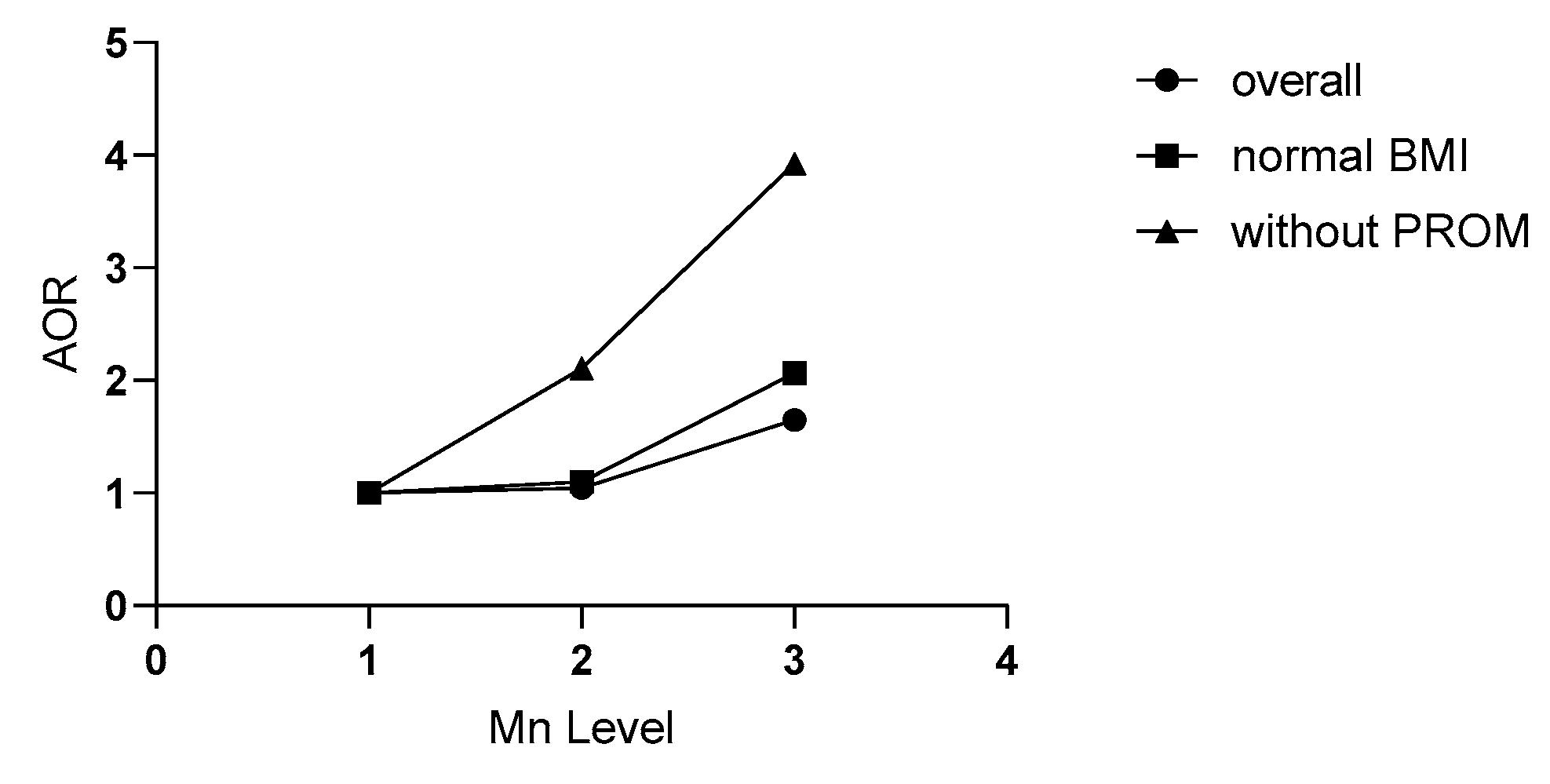
3.3. Relationship between Mn Level in the Third Trimester and SPB Risk
3.4. Relationship between Mn Level in the Third Trimester and SPB Risk Stratified by BMI Grade
3.5. Relationship between Mn Level in the Third Trimester and SPB Risk in Non-PROM Women
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deng, K.; Liang, J.; Mu, Y.; Liu, Z.; Wang, Y.; Li, M.; Li, X.; Dai, L.; Li, Q.; Chen, P.; et al. Preterm births in China between 2012 and 2018: An observational study of more than 9 million women. Lancet Glob. Health 2021, 9, e1226–e1241. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Sun, K.; Zhang, Y. The rising preterm birth rate in China: A cause for concern. Lancet Glob. Health 2021, 9, e1179–e1180. [Google Scholar] [CrossRef] [PubMed]
- Bermúdez, L.; García-Vicent, C.; López, J.; Torró, M.I.; Lurbe, E. Assessment of ten trace elements in umbilical cord blood and maternal blood: Association with birth weight. J. Transl. Med. 2015, 13, 291. [Google Scholar] [CrossRef]
- Mora, A.M.; Joode, B.V.W.D.; Mergler, D.; Córdoba, L.; Cano, C.; Quesada, R.; Smith, D.R.; Menezes-Filho, J.A.; Eskenazi, B. Maternal blood and hair manganese concentrations, fetal growth, and length of gestation in the ISA cohort in Costa Rica. Environ. Res. 2015, 136, 47–56. [Google Scholar] [CrossRef]
- Eum, J.-H.; Cheong, H.-K.; Ha, E.-H.; Ha, M.; Kim, Y.; Hong, Y.-C.; Park, H.; Chang, N. Maternal blood manganese level and birth weight: A MOCEH birth cohort study. Environ. Health 2014, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Zhang, J.; Qi, X.; Wang, Z.; Zheng, M.; Liu, P.; Jiang, S.; Guo, J.; Wu, C.; Zhou, Z. Cord Blood Manganese Concentrations in Relation to Birth Outcomes and Childhood Physical Growth: A Prospective Birth Cohort Study. Nutrients 2021, 13, 4304. [Google Scholar] [CrossRef]
- Oulhote, Y.; Mergler, D.; Bouchard, M.F. Sex- and age-differences in blood manganese levels in the U.S. general population: National health and nutrition examination survey 2011–2012. Environ. Health 2014, 13, 87. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press (US): Washington, DC, USA, 2001.
- WHO; FAO. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization: Geneva, Switzerland; FAO: Rome, Italy, 2004. [Google Scholar]
- Williams, M.; Todd, G.D.; Roney, N.; Crawford, J.; Coles, C.; McClure, P.R.; Garey, J.D.; Zaccaria, K.; Citra, M. Toxicological Profile for Manganese. Atlanta (GA): Agency for Toxic Substances and Disease Registry (US); Agency for Toxic Substances and Disease Registry (ATSDR): Atlanta, GA, USA, 2012; (PMID: 24049862; Bookshelf ID: NBK158872). Available online: https://www.atsdr.cdc.gov/ToxProfiles/tp151.pdf (accessed on 12 March 2023).
- Di Renzo, G.C.; Tosto, V.; Giardina, I. The biological basis and prevention of preterm birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 13–22. [Google Scholar] [CrossRef]
- Martinez-Finley, E.J.; Gavin, C.E.; Aschner, M.; Gunter, T.E. Manganese neurotoxicity and the role of reactive oxygen species. Free. Radic. Biol. Med. 2013, 62, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Ashrap, P.; Watkins, D.J.; Mukherjee, B.; Boss, J.; Richards, M.J.; Rosario, Z.; Velez-Vega, C.M.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Maternal blood metal and metalloid concentrations in association with birth outcomes in Northern Puerto Rico. Environ. Int. 2020, 138, 105606. [Google Scholar] [CrossRef]
- Hao, Y.; Yan, L.; Pang, Y.; Yan, H.; Zhang, L.; Liu, J.; Li, N.; Wang, B.; Zhang, Y.; Li, Z.; et al. Maternal serum level of manganese, single nucleotide polymorphisms, and risk of spontaneous preterm birth: A nested case-control study in China. Environ. Pollut. 2020, 262, 114187. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Meng, X.; Pang, Y.; An, H.; Wang, B.; Zhang, L.; Ye, R.; Ren, A.; Li, Z.; Gong, J. Associations of maternal exposure to 41 metals/metalloids during early pregnancy with the risk of spontaneous preterm birth: Does oxidative stress or DNA methylation play a crucial role? Environ. Int. 2022, 158, 106966. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, M.; Shibata, E.; Morokuma, S.; Tanaka, R.; Senju, A.; Araki, S.; Sanefuji, M.; Koriyama, C.; Yamamoto, M.; Ishihara, Y.; et al. The association between whole blood concentrations of heavy metals in pregnant women and premature births: The Japan Environment and Children’s Study (JECS). Environ. Res. 2018, 166, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wei, L.; Chen, X.; Zhang, R.; Su, L.; Rahman, M.; Mostofa, G.; Qamruzzaman, Q.; Zhao, Y.; Yu, H.; et al. Cord serum elementomics profiling of 56 elements depicts risk of preterm birth: Evidence from a prospective birth cohort in rural Bangladesh. Environ. Int. 2021, 156, 106731. [Google Scholar] [CrossRef]
- China Expert Panel of Medical Nutrition Therapy for Overweight/Obesity. Expert consensus on medical nutrition therapy for overweight/obesity in China. Chin. J. Diabetes Mellit. 2016, 8, 525–540. (In Chinese) [Google Scholar]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Chou, D.; Born Too Soon Preterm Birth Action Group. Born too soon: The global epidemiology of 15 million preterm births. Reprod. Health 2013, 10 (Suppl. 1), S2. [Google Scholar] [CrossRef]
- Peelen, M.J.C.S.; Kazemier, B.M.; Ravelli, A.C.J.; de Groot, C.J.M.; van der Post, J.A.M.; Mol, B.W.J.; Kok, M.; Hajenius, P.J. Ethnic differences in the impact of male fetal gender on the risk of spontaneous preterm birth. J. Perinatol. 2021, 41, 2165–2172. [Google Scholar] [CrossRef]
- Armstrong, R.A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef]
- Horning, K.J.; Caito, S.W.; Tipps, K.G.; Bowman, A.B.; Aschner, M. Manganese Is Essential for Neuronal Health. Annu. Rev. Nutr. 2015, 35, 71–108. [Google Scholar] [CrossRef] [PubMed]
- Roth, J.; Ponzoni, S.; Aschner, M. Manganese homeostasis and transport. Met. Ions Life Sci. 2013, 12, 169–201. [Google Scholar]
- Yoon, M.; Nong, A.; Clewell, H.J.; Taylor, M.D.; Dorman, D.C.; Andersen, M.E. Evaluating placental transfer and tissue concentrations of manganese in the pregnant rat and fetuses after inhalation exposures with a PBPK model. Toxicol. Sci. 2009, 112, 44–58. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.G.; Simpson, C.D.; Stover, B.; Sheppard, L.; Checkoway, H.; Racette, B.A.; Seixas, N.S. Blood manganese as an exposure biomarker: State of the evidence. J. Occup. Environ. Hyg. 2014, 11, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Hoet, P.; Vanmarcke, E.; Geens, T.; Deumer, G.; Haufroid, V.; Roels, H.A. Manganese in plasma: A promising biomarker of exposure to Mn in welders. A pilot study. Toxicol. Lett. 2012, 213, 69–74. [Google Scholar] [CrossRef]
- Ashrap, P.; Watkins, D.J.; Mukherjee, B.; Boss, J.; Richards, M.J.; Rosario, Z.; Vélez-Vega, C.M.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Predictors of urinary and blood Metal(loid) concentrations among pregnant women in Northern Puerto Rico. Environ. Res. 2020, 183, 109178. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.E.; Cheong, H.K.; Ha, E.H.; Kim, B.N.; Ha, M.; Kim, Y.; Hong, Y.C.; Park, H.; Oh, S.Y. Maternal Blood Manganese and Early Neurodevelopment: The Mothers and Children’s Environmental Health (MOCEH) Study. Environ. Health Perspect. 2015, 123, 717–722. [Google Scholar] [CrossRef]
- Gong, L.; Yang, Q.; Liu, C.-W.; Wang, X.; Zeng, H.-L. Assessment of 12 Essential and Toxic Elements in Whole Blood of Pregnant and Non-pregnant Women Living in Wuhan of China. Biol. Trace Elem. Res. 2021, 199, 2121–2130. [Google Scholar] [CrossRef]
- Yamamoto, M.; Sakurai, K.; Eguchi, A.; Yamazaki, S.; Nakayama, S.F.; Isobe, T.; Takeuchi, A.; Sato, T.; Hata, A.; Mori, C.; et al. Association between blood manganese level during pregnancy and birth size: The Japan environment and children’s study (JECS). Environ. Res. 2019, 172, 117–126. [Google Scholar] [CrossRef]
- Vigeh, M.; Yokoyama, K.; Ramezanzadeh, F.; Dahaghin, M.; Fakhriazad, E.; Seyedaghamiri, Z.; Araki, S. Blood manganese concentrations and intrauterine growth restriction. Reprod. Toxicol. 2008, 25, 219–223. [Google Scholar] [CrossRef]
- Bocca, B.; Ruggieri, F.; Pino, A.; Rovira, J.; Calamandrei, G.; Mirabella, F.; Martínez, M.Á.; Domingo, J.L.; Alimonti, A.; Schuhmacher, M. Human biomonitoring to evaluate exposure to toxic and essential trace elements during pregnancy. Part, A. concentrations in maternal blood, urine and cord blood. Environ. Res. 2019, 177, 108599. [Google Scholar] [CrossRef]
- Caspersen, I.H.; Thomsen, C.; Haug, L.S.; Knutsen, H.K.; Brantsæter, A.L.; Papadopoulou, E.; Erlund, I.; Lundh, T.; Alexander, J.; Meltzer, H.M. Patterns and dietary determinants of essential and toxic elements in blood measured in mid-pregnancy: The Norwegian Environmental Biobank. Sci. Total Environ. 2019, 671, 299–308. [Google Scholar] [CrossRef]
- Irwinda, R.; Wibowo, N.; Putri, A.S. The Concentration of Micronutrients and Heavy Metals in Maternal Serum, Placenta, and Cord Blood: A Cross-Sectional Study in Preterm Birth. J. Pregnancy 2019, 2019, 5062365. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Ali, I.; Rust, P.; Kundi, M.; Ekmekcioglu, C. Selenium, Zinc, and Manganese Status in Pregnant Women and Its Relation to Maternal and Child Complications. Nutrients 2020, 12, 725. [Google Scholar] [CrossRef]
- Liang, C.M.; Wu, X.Y.; Huang, K.; Yan, S.Q.; Li, Z.J.; Xia, X.; Pan, W.J.; Sheng, J.; Tao, Y.R.; Xiang, H.Y.; et al. Trace element profiles in pregnant women’s sera and umbilical cord sera and influencing factors: Repeated measurements. Chemosphere 2019, 218, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Yan, L.; Li, H.; Li, X.; Liu, Y.; Liu, J. Patterns and Determinants of Essential and Toxic Elements in Chinese Women at Mid-Pregnancy, Late Pregnancy, and Lactation. Nutrients 2021, 13, 668. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhang, Y.; Piao, J.; Mao, D.; Li, Y.; Li, W.; Yang, L.; Yang, X. Reference Values of 14 Serum Trace Elements for Pregnant Chinese Women: A Cross-Sectional Study in the China Nutrition and Health Survey 2010–2012. Nutrients 2017, 9, 309. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-S.; Liao, K.-W.; Chang, C.-H.; Chien, L.-C.; Mao, I.-F.; Tsai, Y.-A.; Chen, M.-L. The critical fetal stage for maternal manganese exposure. Environ. Res. 2015, 137, 215–221. [Google Scholar] [CrossRef]
- Alacios, C. The role of nutrients in bone health, from A to Z. Crit. Rev. Food Sci. Nutr. 2006, 46, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Couceiro, J.; Matos, I.; Mendes, J.J.; Baptista, P.V.; Fernandes, A.R.; Quintas, A. Inflammatory factors, genetic variants, and predisposition for preterm birth. Clin. Genet. 2021, 100, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Lien, Y.-C.; Zhang, Z.; Cheng, Y.; Polyak, E.; Sillers, L.; Falk, M.J.; Ischiropoulos, H.; Parry, S.; Simmons, R.A. Human Placental Transcriptome Reveals Critical Alterations in Inflammation and Energy Metabolism with Fetal Sex Differences in Spontaneous Preterm Birth. Int. J. Mol. Sci. 2021, 22, 7899. [Google Scholar] [CrossRef]
- Wang, P.; Pan, J.; Tian, X.; Dong, X.; Ju, W.; Wang, Y.; Zhong, N. Transcriptomics-determined chemokine-cytokine pathway presents a common pathogenic mechanism in pregnancy loss and spontaneous preterm birth. Am. J. Reprod. Immunol. 2021, 86, e13398. [Google Scholar] [CrossRef] [PubMed]
- Phillippe, M. Telomeres, oxidative stress, and timing for spontaneous term and preterm labor. Am. J. Obstet. Gynecol. 2022, 227, 148–162. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Yan, H.; Liu, Y.; Zhang, L.; Li, Z.; Ye, R. Research progress on the effect of essential trace elements on premature delivery. Chin. J. Reprod. Health 2020, 31, 174–176+183. (In Chinese) [Google Scholar]



{kind=link}
{kind=link}
| Characteristic | Total (N = 488) | SPB (N = 244) | TB (N = 244) | p |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Age (year) a | 31.51 ± 3.91 | 31.92 ± 3.95 | 31.09 ± 3.82 | 0.018 |
| <30 | 161 (33) | 76 (31.1) | 85 (34.8) | 0.128 |
| 30–34 | 212 (43.4) | 101 (41.4) | 111 (45.5) | |
| ≥35 | 115 (23.6) | 67 (27.5) | 48 (19.7) | |
| BMI (kg/m2) a | 21.67 ± 2.90 | 22.14 ± 3.25 | 21.21 ± 2.4 | <0.001 |
| Slim | 58 (11.9) | 29 (11.9) | 29 (11.9) | 0.003 |
| Normal | 337 (69.1) | 154 (63.1) | 183 (75) | |
| Overweight | 93 (19) | 61 (25) | 32 (13.1) | |
| Education | ||||
| Lower than bachelor’s | 116 (23.8) | 67 (27.5) | 49 (20.1) | 0.133 |
| Bachelor’s | 262 (53.7) | 122 (50) | 140 (57.4) | |
| Master’s or higher | 110 (22.5) | 55 (22.5) | 55 (22.5) | |
| Economy | ||||
| <5000 | 19 (3.9) | 11 (4.5) | 8 (3.3) | 0.513 |
| 5000–9999 | 92 (18.9) | 50 (20.5) | 42 (17.3) | |
| 10,000–19,999 | 188 (38.6) | 96 (39.3) | 92 (37.9) | |
| ≥20,000 | 188 (38.6) | 87 (35.7) | 101 (41.6) | |
| Nationality | ||||
| Han | 449 (92) | 223 (91.4) | 226 (92.6) | 0.617 |
| Others | 39 (8) | 21 (8.6) | 18 (7.4) | |
| Gravida | ||||
| 1 | 239 (49) | 111 (45.5) | 128 (52.5) | 0.124 |
| ≥2 | 249 (51) | 133 (54.5) | 116 (47.5) | |
| Parity | ||||
| Nulliparous | 343 (70.3) | 157 (64.3) | 186 (76.2) | 0.004 |
| Multiparous | 145 (29.7) | 87 (35.7) | 58 (23.8) | |
| GWG (kg) a | 13.82 ± 4.63 | 13.01 ± 4.70 | 14.63 ± 4.42 | <0.001 |
| Sampling time | ||||
| First trimester (week) b | 8 (1) | 8 (1) | 8 (1) | 0.892 |
| Third trimester (week) b | 34 (1) | 34 (1) | 34 (1) | 0.824 |
| Delivery way | ||||
| Natural birth | 325 (66.6) | 147 (60.2) | 178 (73) | 0.003 |
| cesarean section | 163 (33.4) | 97 (39.8) | 66 (27) | |
| Labor week (week) b | 37 (4) | 36 (1) | 40 (1) | <0.001 |
| Fetal gender | ||||
| Boy | 261 (53.5) | 136 (55.7) | 125 (51.2) | 0.318 |
| Girl | 227 (46.5) | 108 (44.3) | 119 (48.8) | |
| Birth weight (g) a | 3067 ± 487 | 2701 ± 341 | 3434 ± 297 | <0.001 |
| Median (IQR) (ng/mL) | p a | |||
|---|---|---|---|---|
| Total (n = 488) | SPB (n = 244) | TB (n = 244) | ||
| First Trimester | 0.81 (0.63) | 0.82 (0.73) | 0.79 (0.60) | 0.441 |
| Third Trimester | 1.23 (0.67) | 1.27 (0.66) | 1.20 (0.61) | 0.119 |
| p b | <0.001 | <0.001 | <0.001 | |
| Tertile Concentration of Mn (ng/mL) | Total | Cases | Controls | Crude OR | p | Adjusted OR a | p | Adjusted OR b | p | Adjusted OR c | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | |||||
| First trimester | |||||||||||
| <0.609 | 163 (33.4) | 77 (31.6) | 86 (35.2) | 1 | 1 | 1 | 1 | ||||
| 0.609–1.012 | 163 (33.4) | 82 (33.6) | 81 (33.2) | 1.13 (0.73–1.75) | 0.58 | 1.12 (0.72–1.77) | 0.612 | 1.09 (0.70–1.70) | 0.716 | 1.123 (0.71–1.79) | 0.614 |
| >1.012 | 162 (33.2) | 85 (34.8) | 77 (31.6) | 1.23 (0.80–1.91) | 0.346 | 1.19 (0.76–1.87) | 0.45 | 1.20 (0.76–1.87) | 0.434 | 1.16 (0.73–1.85) | 0.522 |
| p trend | 0.346 | 0.450 | 0.434 | 0.521 | |||||||
| Third Trimester | |||||||||||
| >1.061 | 163 (33.5) | 75 (30.7) | 88 (36.2) | 1 | 1 | 1 | 1 | ||||
| 1.061–1.470 | 162 (33.3) | 77 (31.6) | 85 (35) | 1.06 (0.69–1.64) | 0.784 | 1.08 (0.68–1.70) | 0.754 | 1.06 (0.68–1.65) | 0.804 | 1.04 (0.66–1.65) | 0.862 |
| >1.470 | 162 (33.3) | 92 (37.7) | 70 (28.8) | 1.54 (1.00–2.39) | 0.052 | 1.60 (1.02–2.53) | 0.043 | 1.63 (1.04–2.55) | 0.032 | 1.65 (1.04–2.62) | 0.035 |
| p trend | 0.053 | 0.042 | 0.033 | 0.035 | |||||||
| Median (IQR) (ng/mL) | ||||
|---|---|---|---|---|
| Total | SPB | TB | ||
| Slim | ||||
| n (%) | 58 (11.9) | 29 (11.9) | 29 (11.9) | |
| First Trimester | 0.77(0.63) | 0.68(0.65) | 0.95(0.66) | 0.27 |
| Third Trimester | 1.29(0.78) | 1.30(0.69) | 1.20(0.91) | 0.858 |
| Normal | ||||
| n (%) | 337 (69.1) | 154 (63.1) | 183 (75) | |
| First Trimester | 0.80(0.63) | 0.82(0.70) | 0.78(0.62) | 0.297 |
| Third Trimester | 1.22(0.68) | 1.30(0.67) | 1.15(0.59) | 0.043 |
| Overweight | ||||
| n (%) | 93 (19.1) | 61 (25) | 32 (13.1) | |
| First Trimester | 0.86(0.74) | 0.88(0.80) | 0.84(0.47) | 0.701 |
| Third Trimester | 1.27(0.54) | 1.26(0.67) | 1.30(0.61) | 0.282 |
| Tertile Concentration of Mn (ng/mL) | Total | Cases | Controls | Crude OR | p | Adjusted OR a | p | Adjusted OR b | p | Adjusted OR c | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | |||||
| Slim | 58 | ||||||||||
| First trimester | |||||||||||
| <0.609 | 23 (39.7) | 13 (44.8) | 10 (34.5) | 1 | 1 | 1 | 1 | ||||
| 0.609–1.012 | 15 (25.9) | 7 (24.1) | 8 (27.6) | 0.67 (0.18–2.49) | 0.553 | 0.54 (0.09–3.27) | 0.506 | 0.62 (0.16–2.48) | 0.498 | 0.51 (0.07–3.60) | 0.496 |
| >1.012 | 20 (34.5) | 9 (31) | 11 (37.9) | 0.63 (0.19–2.10) | 0.452 | 0.39 (0.07–2.13) | 0.279 | 0.81 (0.22–3.01) | 0.758 | 0.66 (0.08–5.37) | 0.699 |
| p trend | 0.446 | 0.280 | 0.736 | 0.699 | |||||||
| Third trimester | |||||||||||
| <1.061 | 17 (29.3) | 7 (24.1) | 10 (34.5) | 1 | 1 | 1 | 1 | ||||
| 1.061–1.470 | 19 (32.8) | 10 (34.5) | 9 (31) | 1.59 (0.42–5.95) | 0.493 | 3.87 (0.55–27.39) | 0.175 | 1.98 (0.47–8.37) | 0.352 | 5.28 (0.63–44.40) | 0.125 |
| >1.470 | 22 (37.9) | 12 (41.4) | 10 (34.5) | 1.71 (0.48–6.16) | 0.409 | 3.41 (0.65–17.92) | 0.147 | 2.50 (0.61–10.34) | 0.205 | 5.95 (0.84–42.20) | 0.075 |
| p trend | 0.422 | 0.179 | 0.212 | 0.090 | |||||||
| Normal | 337 | ||||||||||
| First trimester | |||||||||||
| <0.609 | 116 (34.4) | 48 (31.2) | 68 (37.2) | 1 | 1 | 1 | 1 | ||||
| 0.609–1.012 | 114 (33.8) | 53 (34.4) | 61 (33.3) | 1.21 (0.72–2.04) | 0.435 | 1.3 (0.76–2.23) | 0.320 | 1.24 (0.73–2.11) | 0.435 | 1.38 (0.79–2.41) | 0.260 |
| >1.012 | 107 (31.8) | 53 (34.4) | 54 (29.5) | 1.39 (0.82–2.36) | 0.222 | 1.33 (0.77–2.30) | 0.304 | 1.32 (0.77–2.28) | 0.318 | 1.27 (0.73–2.23) | 0.400 |
| p trend | 0.221 | 0.297 | 0.314 | 0.387 | |||||||
| Third trimester | |||||||||||
| <1.061 | 121 (36) | 48 (31.2) | 73 (40.1) | ||||||||
| 1.061–1.470 | 104 (31) | 44 (28.6) | 60 (33) | 1.12 (0.66–1.90) | 0.688 | 1.17 (0.67–2.06) | 0.572 | 1.09 (0.63–1.88) | 0.760 | 1.10 (0.62–1.95) | 0.747 |
| >1.470 | 111 (33) | 62 (40.3) | 49 (26.9) | 1.89 (1.12–3.20) | 0.014 | 1.96 (1.13–3.38) | 0.014 | 2.07 (1.20–3.54) | 0.008 | 2.07 (1.18–3.61) | 0.011 |
| p trend | 0.015 | 0.014 | 0.009 | 0.011 | |||||||
| Overweight | 93 | ||||||||||
| First trimester | |||||||||||
| <0.609 | 24 (25.8) | 16 (26.2) | 8 (25) | 1 | 1 | 1 | 1 | ||||
| 0.609–1.012 | 34 (36.6) | 22 (36.1) | 12 (37.5) | 0.92 (0.30–2.76) | 0.877 | 0.99 (0.26–3.72) | 0.984 | 0.79 (0.25–2.51) | 0.692 | 0.69 (0.17–2.80) | 0.604 |
| >1.012 | 35 (37.6) | 23 (37.7) | 12 (37.5) | 0.96 (0.32–2.88) | 0.939 | 1.25 (0.33–4.76) | 0.746 | 0.89 (0.28–2.78) | 0.835 | 1.08 (0.26–4.55) | 0.915 |
| p trend | 0.952 | 0.717 | 0.867 | 0.847 | |||||||
| Third trimester | |||||||||||
| <1.061 | 25 (26.9) | 20 (32.8) | 5 (15.6) | 1 | 1 | 1 | 1 | ||||
| 1.061–1.470 | 39 (41.9) | 23 (37.7) | 16 (50) | 0.36 (0.11–1.16) | 0.086 | 0.38 (0.10–1.41) | 0.148 | 0.34 (0.10–1.16) | 0.086 | 0.31 (0.08–1.26) | 0.101 |
| >1.470 | 29 (31.2) | 18 (29.5) | 11 (34.4) | 0.41 (0.12–1.41) | 0.156 | 0.32 (0.07–1.40) | 0.129 | 0.36 (0.10–1.32) | 0.123 | 0.18 (0.04–0.95) | 0.044 |
| p trend | 0.188 | 0.144 | 0.153 | 0.046 | |||||||
| Tertile Concentration of Mn (ng/mL) | Cases | Controls | Crude OR | p | Adjusted OR a | p | Adjusted OR b | p | Adjusted OR c | p |
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | |||||
| First Trimester | ||||||||||
| SPB with PROM | ||||||||||
| <0.609 | 52 (35.9) | 86 (35.2) | ||||||||
| 0.609–1.012 | 50 (34.5) | 81 (33.2) | 1.03 (0.63–1.69) | 0.895 | 1.04 (0.62–1.72) | 0.949 | 1.00 (0.61–1.65) | 0.990 | 1.04 (0.62–1.75) | 0.941 |
| >1.012 | 43 (29.7) | 77 (31.6) | 0.91 (0.55–1.51) | 0.721 | 0.91 (0.54–1.54) | 0.700 | 0.91 (0.54–1.51) | 0.702 | 0.90 (0.53–1.52) | 0.643 |
| P trend | 0.732 | 0.734 | 0.709 | 0.699 | ||||||
| SPB without PROM | ||||||||||
| <0.609 | 25 (25.3) | 86 (35.2) | ||||||||
| 0.609–1.012 | 32 (32.3) | 81 (33.2) | 1.38 (0.75–2.52) | 0.301 | 1.37 (0.73–2.57) | 0.327 | 1.31 (0.70–2.44) | 0.396 | 1.39 (0.72–2.66) | 0.347 |
| >1.012 | 42 (42.4) | 77 (31.6) | 1.85 (1.04–3.32) | 0.038 | 1.72 (0.94–3.14) | 0.084 | 1.80 (0.98–3.29) | 0.058 | 1.71 (0.91–3.20) | 0.098 |
| p trend | 0.036 | 0.077 | 0.056 | 0.092 | ||||||
| Third Trimester | ||||||||||
| SPB with PROM | ||||||||||
| <1.061 | 58 (40) | 88 (36.2) | ||||||||
| 1.061–1.470 | 42 (29) | 85 (35) | 0.75 (0.46–1.23) | 0.255 | 0.75 (0.45–1.26) | 0.319 | 0.76 (0.46–1.25) | 0.28 | 0.74 (0.44–1.25) | 0.303 |
| >1.470 | 45 (31) | 70 (28.8) | 0.98 (0.59–1.61) | 0.922 | 0.99 (0.59–1.67) | 0.986 | 1.03 (0.62–1.71) | 0.912 | 1.02 (0.60–1.73) | 0.925 |
| P trend | 0.855 | 0.922 | 0.986 | 0.993 | ||||||
| SPB without PROM | ||||||||||
| <1.061 | 17 (17.2) | 88 (36.2) | ||||||||
| 1.061–1.470 | 35 (35.4) | 85 (35) | 2.13 (1.11–4.09) | 0.023 | 2.22 (1.12–4.39) | 0.021 | 2.08 (1.07–4.05) | 0.031 | 2.11 (1.05–4.22) | 0.031 |
| >1.470 | 47 (47.5) | 70 (28.8) | 3.48 (1.84–6.57) | <0.001 | 3.81 (1.96–7.40) | <0.001 | 3.69 (1.92–7.08) | <0.001 | 3.93 (2.00–7.74) | <0.001 |
| p trend | <0.001 | <0.001 | <0.001 | <0.001 |
| Tertile Concentration of Mn (ng/mL) | Total (n = 463) | Cases (n = 235) | Controls (n = 228) | Crude OR | p | Adjusted OR a | p | Adjusted OR b | p | Adjusted OR c | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | |||||
| First Trimester | |||||||||||
| <0.609 | 156 (33.7) | 75 (31.9) | 81 (35.5) | ||||||||
| 0.609–1.012 | 153 (33) | 77 (32.8) | 76 (33.3) | 1.09 (0.70–1.71) | 0.692 | 1.10 (0.69–1.76) | 0.680 | 1.04 (0.66–1.64) | 0.879 | 1.10 (0.68–1.77) | 0.697 |
| >1.012 | 154 (33.3) | 83 (35.3) | 71 (31.1) | 1.26 (0.81–1.97) | 0.306 | 1.21 (0.76–1.92) | 0.422 | 1.23 (0.78–1.95) | 0.378 | 1.19 (0.74–1.92) | 0.477 |
| p trend | 0.306 | 0.422 | 0.380 | 0.477 | |||||||
| Third Trimester | |||||||||||
| <1.061 | 156 (33.8) | 72 (30.6) | 84 (37) | ||||||||
| 1.061–1.470 | 151 (32.7) | 74 (31.5) | 77 (33.9) | 1.12 (0.72–1.76) | 0.617 | 1.13 (0.71–1.80) | 0.615 | 1.10 (0.70–1.74) | 0.671 | 1.08 (0.67–1.75) | 0.738 |
| >1.470 | 155 (33.5) | 89 (19.3) | 66 (29.1) | 1.57 (1.01–2.46) | 0.047 | 1.62 (1.01–2.57) | 0.044 | 1.66 (1.05–2.63) | 0.030 | 1.68 (1.04–2.69) | 0.033 |
| p trend | 0.048 | 0.043 | 0.031 | 0.033 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, W.; Zheng, W.; Wang, A.; Chen, J.; Wang, J.; Huang, J.; An, H.; Ma, Y.; Zhang, K.; Yang, R.; et al. Association of Maternal Plasma Manganese with the Risk of Spontaneous Preterm Birth: A Nested Case–Control Study Based on the Beijing Birth Cohort Study (BBCS) in China. Nutrients 2023, 15, 1413. https://doi.org/10.3390/nu15061413
Han W, Zheng W, Wang A, Chen J, Wang J, Huang J, An H, Ma Y, Zhang K, Yang R, et al. Association of Maternal Plasma Manganese with the Risk of Spontaneous Preterm Birth: A Nested Case–Control Study Based on the Beijing Birth Cohort Study (BBCS) in China. Nutrients. 2023; 15(6):1413. https://doi.org/10.3390/nu15061413
Chicago/Turabian StyleHan, Weiling, Wei Zheng, Aili Wang, Junxi Chen, Jia Wang, Junhua Huang, Hang An, Yuru Ma, Kexin Zhang, Ruihua Yang, and et al. 2023. "Association of Maternal Plasma Manganese with the Risk of Spontaneous Preterm Birth: A Nested Case–Control Study Based on the Beijing Birth Cohort Study (BBCS) in China" Nutrients 15, no. 6: 1413. https://doi.org/10.3390/nu15061413
APA StyleHan, W., Zheng, W., Wang, A., Chen, J., Wang, J., Huang, J., An, H., Ma, Y., Zhang, K., Yang, R., Yan, L., Li, Z., & Li, G. (2023). Association of Maternal Plasma Manganese with the Risk of Spontaneous Preterm Birth: A Nested Case–Control Study Based on the Beijing Birth Cohort Study (BBCS) in China. Nutrients, 15(6), 1413. https://doi.org/10.3390/nu15061413