
Factors That Influence Children’s Exits from the Special Supplemental Nutrition Program for Women, Infants, and Children: A Systematic Review


Abstract
1. Introduction
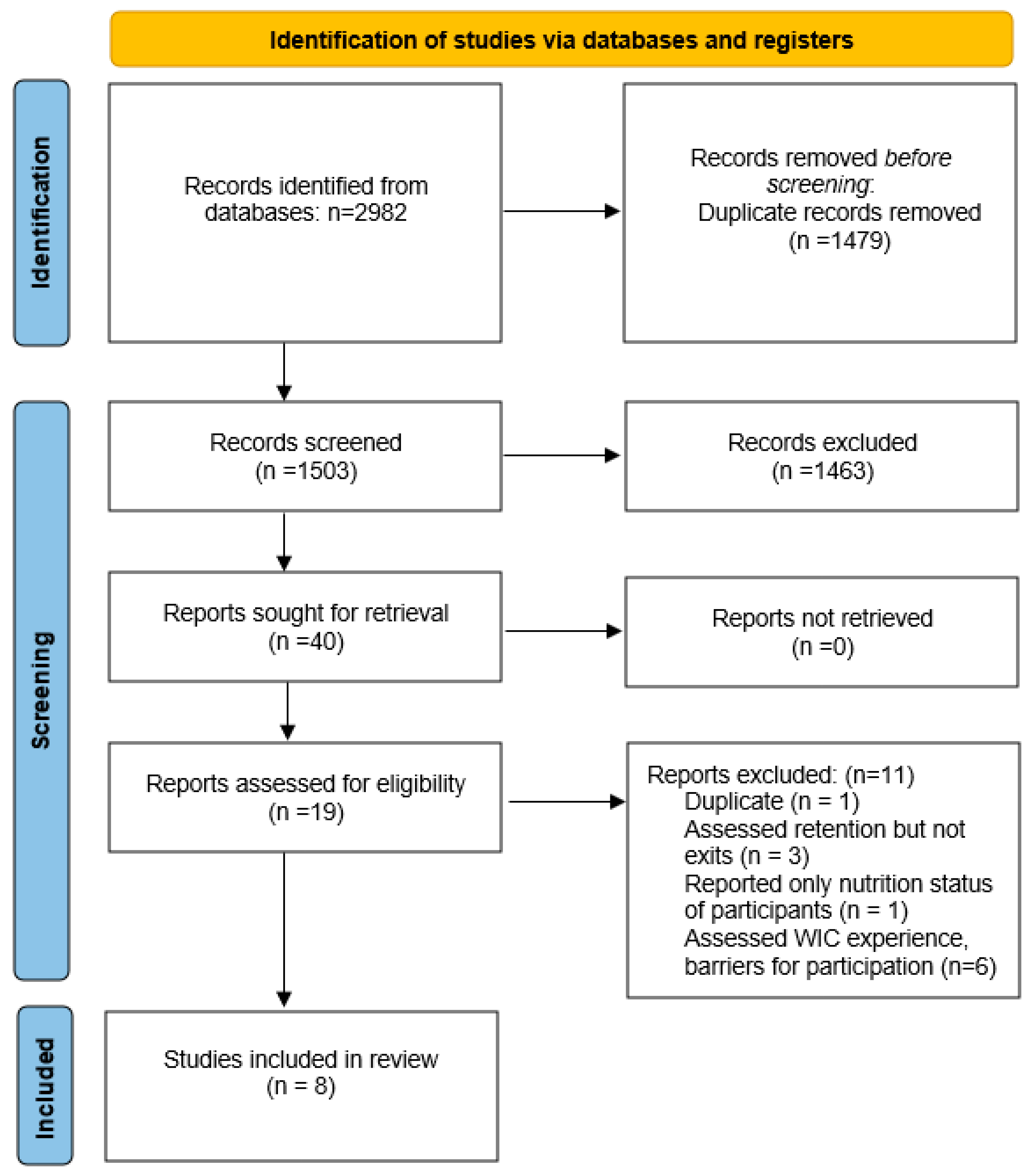
2. Materials and Methods
3. Results
3.1. Criteria Used to Assess WIC Exits
3.2. Demographic Characteristics of Study Samples
3.3. Main Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Archives and Records Administration. Title 7, Part 246. Special Supplemental Nutrition Program for Women, Infants and Children. Available online: https://www.govinfo.gov/app/details/CFR-2022-title7-vol4/CFR-2022-title7-vol4-part246 (accessed on 29 November 2022).
- WIC Frequently Asked Questions (FAQs). Available online: https://www.fns.usda.gov/wic/frequently-asked-questions (accessed on 29 November 2022).
- WIC Program. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/wic-program/#:~:text=This%20amounts%20to%20the%20cost,to%20apply%20for%20the%20program (accessed on 16 November 2022).
- Weinfield, N.S.; Borger, C.; Au, L.E.; Whaley, S.E.; Berman, D.; Ritchie, L.D. Longer participation in WIC Is associated with better diet quality in 24-month-old children. J. Acad. Nutr. Diet. 2020, 120, 963–971. [Google Scholar] [CrossRef]
- Anderson, C.E.; Martinez, C.E.; Ritchie, L.D.; Paolicelli, C.; Reat, A.; Borger, C.; Whaley, S.E. Longer Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) participation duration is associated with higher diet quality at age 5 years. J. Nutr. 2022, 152, 1974–1982. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, J.F.; Anater, A.S.; Hampton, J.C.; Catellier, D.J.; Eldridge, A.L.; Johnson, W.L.; Quann, E.E. The Special Supplemental Nutrition Program for Women, Infants, and Children is associated with several changes in nutrient intakes and food consumption patterns of participating infants and young children, 2008 compared with 2016. J. Nutr. 2020, 150, 2985–2993. [Google Scholar] [CrossRef]
- Caulfield, L.E.; Bennett, W.L.; Gross, S.M.; Hurley, K.M.; Ogunwole, S.M.; Venkataramani, M.; Lerman, J.L.; Zhang, A.; Sharma, R.; Bass, E.B. Maternal and Child Outcomes Associated With the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC); Comparative Effectiveness Review No. 253. (Prepared by the Johns Hopkins University Evidence-Based Practice Center under Contract No. 75Q80120D00003.) AHRQ Publication No. 22-EHC019; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2022; Posted final reports are located on the Effective Health Care Program. [CrossRef]
- Toossi, S.; Jones, J.W.; Hodges, L. The Food and Nutrition Assistance Landscape: Fiscal Year 2020 Annual Report. 2021. Available online: https://www.ers.usda.gov/webdocs/publications/101909/eib-227.pdf?v=5724.2 (accessed on 1 December 2022).
- Farson Gray, K.B.-C.E.; Giannarelli, L.; Johnson, P. Estimates of WIC Eligibility and WIC Program Reach in 2019. 2022. Available online: https://www.fns.usda.gov/wic/national-state-level-estimates-eligibility-program-reach-2019 (accessed on 2 December 2022).
- Modernizing WIC. Available online: https://www.fns.usda.gov/infographic/modernizing-wic (accessed on 17 November 2022).
- Borger, C.; Paolicelli, C.; Sun, B.; Zimmerman, T.P.; Dixit-Joshi, S. Duration of WIC Participation and Early Feeding Practices Are Associated With Meeting the Added Sugars Recommendation at Age 3 Years. J. Nutr. Educ. Behav. 2022, 54, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Borger, C.; Paolicelli, C.P.; Sun, B. Duration of Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) Participation is Associated With Children’s Diet Quality at Age 3 Years. Am. J. Prev. Med. 2022, 62, e343–e350. [Google Scholar] [CrossRef]
- Gago, C.M.; Wynne, J.O.; Moore, M.J.; Cantu-Aldana, A.; Vercammen, K.; Zatz, L.Y.; May, K.; Andrade, T.; Mendoza, T.; Stone, S.L.; et al. Caregiver perspectives on underutilization of WIC: A qualitative study. Pediatrics 2022, 149, e2021053889. [Google Scholar] [CrossRef] [PubMed]
- Gundersen, C. A dynamic analysis of the well-being of WIC recipients and eligible non-recipients. Child. Youth Serv. Rev. 2005, 27, 99–114. [Google Scholar] [CrossRef]
- Hammad, T.A.; Havas, S.; Damron, D.; Langenberg, P. Withdrawal rates for infants and children participating in WIC in Maryland. J. Am. Diet. Assoc. 1997, 97, 893–895. [Google Scholar] [CrossRef]
- Jacknowitz, A.; Tiehen, L. Transitions into and out of the WIC program: A cause for concern? Soc. Serv. Rev. 2009, 83, 151–183. [Google Scholar] [CrossRef]
- Panzera, A.D.; Bryant, C.A.; Hawkins, F.; Goff, R.; Napier, A.; Schneider, T.; Kirby, R.S.; Coulter, M.L.; Sappenfield, W.M.; Baldwin, J. Mapping a WIC mother’s journey: A preliminary analysis. Soc. Mark. Q. 2017, 23, 137–154. [Google Scholar] [CrossRef]
- Rosenberg, T.J.; Alperen, J.K.; Chiasson, M.A. Why do WIC participants fail to pick up their checks? An urban study in the wake of welfare reform. Am. J. Public Health 2003, 93, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Whaley, S.E.; Whaley, M.; Au, L.E.; Gurzo, K.; Ritchie, L.D. Breastfeeding is associated with higher retention in WIC after age 1. J. Nutr. Educ. Behav. 2017, 49, 810–816.e811. [Google Scholar] [CrossRef]
- Woelfel, M.L.; Abusabha, R.; Pruzek, R.; Stratton, H.; Chen, S.G.; Edmunds, L.S. Barriers to the use of WIC services. J. Am. Diet. Assoc. 2004, 104, 736–743. [Google Scholar] [CrossRef]
- Gray, C. Why Leave Benefits on the Table? Evidence from SNAP. Soc. Mark. Q. 2018, 23, 137–154. [Google Scholar] [CrossRef]
- Gray, C.; O’Leary, C. Increasing beneficiary retention in food assistance programs. Policy Res. Briefs 2019, 6, 4. [Google Scholar] [CrossRef]
- Breastfeeding Data Local Agency Report. FY 2021 Report. Available online: https://www.fns.usda.gov/wic/wic-breastfeeding-data-local-agency-report (accessed on 16 November 2022).
- WIC Food Packages—Maximum Monthly Allowances. Available online: https://www.fns.usda.gov/wic/wic-food-packages-maximum-monthly-allowances (accessed on 28 October 2022).
- Almeida, R.; Alvarez Gutierrez, S.; Whaley, S.E.; Ventura, A.K. A qualitative study of breastfeeding and formula-feeding mothers’ perceptions of and experiences in WIC. J. Nutr. Educ. Behav. 2020, 52, 615–625. [Google Scholar] [CrossRef] [PubMed]
- The Impact of In-Person Benefit Reloading on WIC Participation During the COVID-19 Pandemic. Available online: https://policylab.chop.edu/blog/impact-person-benefit-reloading-wic-participation-during-covid-19-pandemic (accessed on 4 November 2022).
- Congress. Gov. H.R.6201—Families First Coronavirus Response Act. 2020. Available online: https://www.congress.gov/bill/116th-congress/house-bill/6201 (accessed on 17 November 2022).
- WIC COVID-19 Waivers. Available online: https://www.fns.usda.gov/programs/fns-disaster-assistance/fns-responds-covid-19/wic-covid-19-waivers (accessed on 4 November 2022).
- Food Research and Action Center. One Year of WIC During COVID-19: Waivers are Vital to Participation and Benefit Redemption. 2021. Available online: https://frac.org/wp-content/uploads/One-Year-of-WIC-During-COVID-19.pdf (accessed on 7 November 2022).
- The Network for Public Health Law. WIC: Lessons Learned from COVID-19. Available online: https://www.networkforphl.org/wp-content/uploads/2022/05/WIC-COVID-Issue-Brief-Final.pdf (accessed on 7 November 2022).
- Bess, S.; Odoms-Young, A.; Uesugi, K.; Brooks, T. Retention of Participants Through the First Five Years; University of Illinois at Chicago: Chicago, IL, USA. Available online: https://drive.google.com/drive/folders/1uf4xLp6iJuKAkKi_2gghGfjSUfdvdmw3 (accessed on 7 November 2022).
- Scott, C.; Padilla, V.; Markides, B.; Biediger-Friedman, L.; Crixell, S. O47 Chat with Maya: Assessing the usability of the Texas WIC chatbot. J. Nutr. Educ. Behav. 2021, 53, S22–S23. [Google Scholar] [CrossRef]
- Hanks, A.S.; Gunther, C.; Lillard, D.; Scharff, R.L. From paper to plastic: Understanding the impact of eWIC on WIC recipient behavior. Food Policy 2019, 83, 83–91. [Google Scholar] [CrossRef]
- Chauvenet, C.; De Marco, M.; Barnes, C.; Ammerman, A.S. WIC recipients in the retail environment: A qualitative study assessing customer experience and satisfaction. J. Acad. Nutr. Diet. 2019, 119, 416–424.e412. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, S.E.; Shriver, L.; Haldeman, L. Qualitative analysis of maternal barriers and perceptions to participation in a federal supplemental nutrition program in rural appalachian north carolina. J. Appalach. Health 2020, 2, 37–52. [Google Scholar]
- Weber, S.J.; Wichelecki, J.; Chavez, N.; Bess, S.; Reese, L.; Odoms-Young, A. Understanding the factors influencing low-income caregivers’ perceived value of a federal nutrition programme, the Special Supplemental Nutrition Program for Women, Infants and Children (WIC). Public Health Nutr. 2019, 22, 1056–1065. [Google Scholar] [CrossRef]
- WIC Online Ordering Grant. Available online: https://www.centerfornutrition.org/wic-online-ordering (accessed on 4 December 2022).
- Food Research and Action Center. Making WIC Work Better: Strategies to Reach More Women and Children and Strengthen Benefits Use. 2019. Available online: https://frac.org/wp-content/uploads/Making-WIC-Work-Better-Exec-Summary-FNL.pdf (accessed on 2 November 2022).
- Halverson, M.M.; Karpyn, A. WIC participants’ perceptions of the cash-value benefit increase during the COVID-19 pandemic. Nutrients 2022, 14, 3509. [Google Scholar] [CrossRef] [PubMed]
- USDA Proposes Science-Driven Updates to Foods Provided Through WIC. Available online: https://www.usda.gov/media/press-releases/2022/11/17/usda-proposes-science-driven-updates-foods-provided-through-wic (accessed on 2 December 2022).
- USDA. USDA Proposes Science Driven Updates to Foods Provided through WIC. What They’re Saying. Press Release No. 0256.22. 2022. Available online: https://www.usda.gov/media/press-releases/2022/11/29/usda-proposes-science-driven-updates-foods-provided-through-wic (accessed on 2 December 2022).
- Southern States Generally Have a Higher Share of Infants Participating in WIC. Available online: https://www.ers.usda.gov/data-products/chart-gallery/gallery/chart-detail/?chartId=78052 (accessed on 12 November 2022).
- Ma, X.; Liu, J.; Smith, M. WIC participation and breastfeeding in South Carolina: Updates from PRAMS 2009–2010. Matern. Child Health J. 2014, 18, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Marshall, C.; Gavin, L.; Bish, C.; Winter, A.; Williams, L.; Wesley, M.; Zhang, L. WIC participation and breastfeeding among White and Black mothers: Data from Mississippi. Matern. Child Health J. 2013, 17, 1784–1792. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhang, J.; Park, K.; Tang, C. Association between usage of an app to redeem prescribed food benefits and redemption behaviors among the Special Supplemental Nutrition Program for Women, Infants, and Children participants: Cross-sectional study. JMIR mHealth uHealth 2020, 8, e20720. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.A.; Leavitt, H.B.; Chau, M. A review of interventions to increase WIC enrollment and participation. J. Community Health 2022, 47, 990–1000. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Design/Data Collection/Data Analysis/Location | Participants | Criteria Used to Assess WIC Exit | Demographic Characteristics of Study Sample a | Main Findings |
|---|---|---|---|---|---|
| Hammad T et al., 1997 [15] | Retrospective/secondary data analysis of administrative records/Maryland, US | Caregivers of infants and children up to 3 years old (n = 12,749) | Child identification number absent from monthly participation record, or a new certification date was not present on monthly participation record for two consecutive months | 40% were non-Hispanic White, 53% were non-Hispanic Black, 5% were Hispanic of any race; 2% were non-Hispanic of another race | Children who enrolled in WIC at 7–12 months were more likely to exit WIC within a year than children who enrolled in WIC at ages 6 months and younger (RR b = 1.34; 95% CI c = 1.26, 1.43) Participants with military health care and those that received health care from a health maintenance organization were more likely to exit WIC than participants that received healthcare from a private physician (RR = 1.32; 95% CI = 1.21, 1.44, and RR = 1.26; 95% CI = 1.16, 1.37, respectively) Suburban residents were more likely (RR = 1.06; 95% CI = 1.02, 1.11) while rural residents were less likely (RR = 0.85; 95% CI = 0.81, 0.90) to exit WIC than urban residents Families with five or more members were less likely to exit WIC than those with two members (RR = 0.94; 95% CI = 0.89, 0.99) |
| Rosenberg T et al., 2003 [18] | Cross sectional/structured questionnaire with close and open-ended questions/New York, US | Former WIC participants who had withdrawn from the program (“leavers,” n = 188) and current WIC clients (“clients,” n= 280) | WIC records contained an entry of “void” or “void unclaimed” for check registry meaning that the participant did not pick up or redeem WIC food package benefits | 90% identified as Hispanic. 51.6% were between 15–29 years, 48.4% were ≥ 30 years. 90% were foreign born | Women who had received WIC themselves were more likely to exit the program compared to women who had not received WIC themselves (AOR d = 1.90; 95% confidence interval [CI] = 1.04, 3.46; p < 0.05) Women who received Medicaid for their child were less likely to exit WIC compared to those who had not received Medicaid for their children (AOR = 0.50; 95% CI = 0.30, 0.84; p < 0.01). Other factors associated with exits from WIC included: Transportation problems (AOR = 2.00; 95% CI = 1.08, 3.72; p < 0.05), family illnesses (AOR = 2.68; 95% CI = 1.48, 4.85; p < 0.01), and job conflicts (AOR = 1.87; 95% CI = 0.30, 0.84; p < 0.05) |
| Woelfel M et al., 2004 [20] | Cross sectional/survey (based on literature review, focus groups with caretakers of WIC participants, and expert panel input)/New York, US | Parents/caretakers of infants and children (n = 3167) on WIC | Did not redeem or pick up WIC food package benefits (paper checks) | 50% were non-Hispanic White, 30% were non-Hispanic Black, 15% were Hispanic of any race. The mean age of parent/caretaker was 29 years | Those that exited WIC reported difficulty rescheduling appointments (n = 309), difficulty recertifying (n = 267), or having to wait too long when picking up checks |
| Gundersen C, 2005 [14] | Retrospective/secondary data analysis from the 1996 panel of the Survey of Income and Program Participation/nationally representative, US | Infants and children income-eligible for WIC in month 12 of the 1996 panel of the Survey of Income and Program Participation (n = 3471) | WIC-eligible infants and children who received WIC in month 12 of the survey and then did not receive WIC in later survey months | 48% were non-Hispanic White, 24% were non-Hispanic Black, 24% were Hispanic of any race; 4% were non-Hispanic of another race or unknown | On average, families that exited WIC had incomes higher than those who continued receiving WIC (average monthly income = $2300 per month), were less likely to continue to participate in SNAP e (66%) and Medicaid (60%), and were less likely to be income-eligible for WIC f |
| Jacknowitz A and Tiehen L, 2009 [16] | Retrospective/secondary data analysis from the 9-month (n = 10,700) and 2-year (n = 9850) waves of the Early Childhood Longitudinal Study Birth Cohort/national, US | WIC participants (n = 4050) | Left the program (no longer reported WIC participation) when the child turned 1 year old | 39% non-Hispanic White; 22% were non-Hispanic Black; 34% were Hispanic of any race; 2% were non-Hispanic Asian, and 3% were non-Hispanic of another race. 13% of were <20 years old, 38% were between 20–24 years, 26% were between 25–29 years, 15% were between 30–34 years, and 9% were over the age of 35. 78% were U.S. citizens | Factors associated with exits from WIC included: higher household income, higher rates of maternal employment before and after the survey child’s birth, more household savings and assets, vehicle ownership, post- natal participation in other assistance programs, higher levels of maternal education, higher rates of maternal smoking, higher rates of never breastfeeding or breastfeeding for less than 6 months, and beliefs about not being eligible for WIC benefits, household location in the Southern region of the U.S., household location in towns with population <2500 |
| Panzera A et al., 2017 [17] | Cross sectional/focus groups, interviews, and direct observations at WIC clinic/Kentucky, US | WIC participants/former WIC participants. Focus groups (n = 19), individual interviews (n = 1), and observed at WIC clinic (n = 6) | Terminated from WIC due to non-participation (failure to attend appointments with food benefit issuance for 60 days) | Focus groups participants age range was 19–51 years, majority White, English speakers | Difficulty scheduling appointments, lack of transportation, childcare challenges, long waits, confusion about program eligibility criteria and procedures, negative interactions with program staff, problems redeeming program benefits, and stigma. |
| Whaley et al., 2017 [19] | Retrospective/secondary data analysis of administrative records/Los Angeles-Orange-San Bernardino counties, US | Infants receiving WIC benefits for at least 1 month between age 7 and 12 months (n = 9632) | Responded “no” to recertification question by when child was 14 months | 67.4% preferred English language, used by authors as a proxy for race and ethnicity | The non-recertified group was statistically significantly different from the recertified/participant group in the following metrics: Less likely to fully breastfeed (11.1% vs. 16.5%; p < 0.001); less likely to have prenatal intention to breastfeed (59.1% vs. 76.8%, p < 0.001); more likely to have missed at least one month of benefits between 6–12 months (48.4% vs. 14.4%; p < 0.001) and redeemed <75% of benefits (41.7% vs. 22.9%; p < 0.001) Had longer prenatal WIC participation (4.85 months vs. 6.23 months; p < 0.001); were less likely to have other family members receiving WIC (1.36 average family members vs. 1.41; p < 0.01); had greater household income (71.3% at or below 100% FPL vs. 76.4%; p < 0.001) g; were more educated (67.6% with high school degree or higher vs. 60.1; p < 0.001); prefer English (83.2% vs. 63.9%; p < 0.001); and less likely to participate in Medicaid (66.9% vs. 75.5%; p < 0.001) |
| Gago C et al., 2022 [13] | Cross sectional/semi structured interviews/Massachusetts, US | Caregivers of WIC eligible children under the age of 5 years who were currently enrolled in WIC or children who were 6–24 months before the date of the interview (total = 37, current = 18, early leavers = 17) | Chose to leave WIC for reasons other than ineligibility | 47% were White, 18% were Black, 35% were of another race 63% were Hispanic 29% were between 18 and 29 years; 32% between the ages of 30–34 and 38% were 35–44 years | Families reported exiting WIC because of: Insufficient fruit and vegetable benefits Food benefits’ inflexibility to allergies, cultural appropriateness, and individual preferences Embarrassment at checkout due to in-store item mislabeling Administrative barriers, including lack of clarity in requirements for certification; challenges rescheduling appointments; long wait times; challenges with transportation to and from appointments; and clinical requirements they felt were unnecessary, redundant, and/or burdensome Perceptions that they were taking benefits that others would need more |
| Demographic Factors | |
| Race & ethnicity | Non-Hispanic White [16] Non-Hispanic of any race [13] |
| Language | Preferred English language [19] |
| Child’ age | Later enrollment in WIC during infancy [15] |
| Parent’s age | Less than 30 years [13,16,18] |
| Family size | Smaller families [15] |
| Socioeconomic factors | |
| Educational attainment | High school completion [13,18,19] More than high school [16,19] |
| Income & assets | Higher household income [14,16,19] Household savings and assets [16] Vehicle ownership [16] |
| Health insurance | Military healthcare [15] Healthcare from health maintenance organization [15] Less likely to receive Medicaid [14,18,19] |
| Means-tested programs | Less likely to participate in SNAP [13,14,18] Less likely to participate in TANF [18] |
| Feeding Practices | |
| Breastfeeding | Less likely to fully breastfeed [19] Less likely to report prenatal intention to breastfeed [19] Never breastfeeding [16] Breastfeeding for less than 6 months [16] |
| Experience with WIC | |
| Prior | Mother received WIC themselves [18] |
| Current | Missed at least one month of benefits between 6–12 months [19] Redeemed less than 75% of benefits [19] Longer prenatal participation [19] |
| Ineligibility |
| Income ineligibility [13,14,16,17] Eligible but on waitlist due to lack of program funds [16] |
| Participant Experience |
| Administrative factors |
| Difficulties recertifying and rescheduling appointments [13,17,20] Long waiting lines to pick up checks [13,20] Negative interactions with program staff [17] Lack of clarity in requirements for certification and redundant requirements [13,16] Benefits not worth the time required to recertify [16] |
| Food benefits |
| Individual preference [13] Cultural appropriateness [13] Allergies [13] No longer needed food benefits [16] |
| Societal expectations |
| Stigma [17] Embarrassment [13] |
| Work & Family |
| Transportation problems [13,16,17,18] Family illnesses [18] Job conflicts [18] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lora, K.R.; Hodges, L.; Ryan, C.; Ver Ploeg, M.; Guthrie, J. Factors That Influence Children’s Exits from the Special Supplemental Nutrition Program for Women, Infants, and Children: A Systematic Review. Nutrients 2023, 15, 766. https://doi.org/10.3390/nu15030766
Lora KR, Hodges L, Ryan C, Ver Ploeg M, Guthrie J. Factors That Influence Children’s Exits from the Special Supplemental Nutrition Program for Women, Infants, and Children: A Systematic Review. Nutrients. 2023; 15(3):766. https://doi.org/10.3390/nu15030766
Chicago/Turabian StyleLora, Karina R., Leslie Hodges, Cayley Ryan, Michele Ver Ploeg, and Joanne Guthrie. 2023. "Factors That Influence Children’s Exits from the Special Supplemental Nutrition Program for Women, Infants, and Children: A Systematic Review" Nutrients 15, no. 3: 766. https://doi.org/10.3390/nu15030766
APA StyleLora, K. R., Hodges, L., Ryan, C., Ver Ploeg, M., & Guthrie, J. (2023). Factors That Influence Children’s Exits from the Special Supplemental Nutrition Program for Women, Infants, and Children: A Systematic Review. Nutrients, 15(3), 766. https://doi.org/10.3390/nu15030766