
Associations between Timing and Duration of Eating and Glucose Metabolism: A Nationally Representative Study in the U.S.


Abstract
1. Introduction
2. Materials & Methods
2.1. Sample
2.2. Measurements
2.3. Statistical Analysis
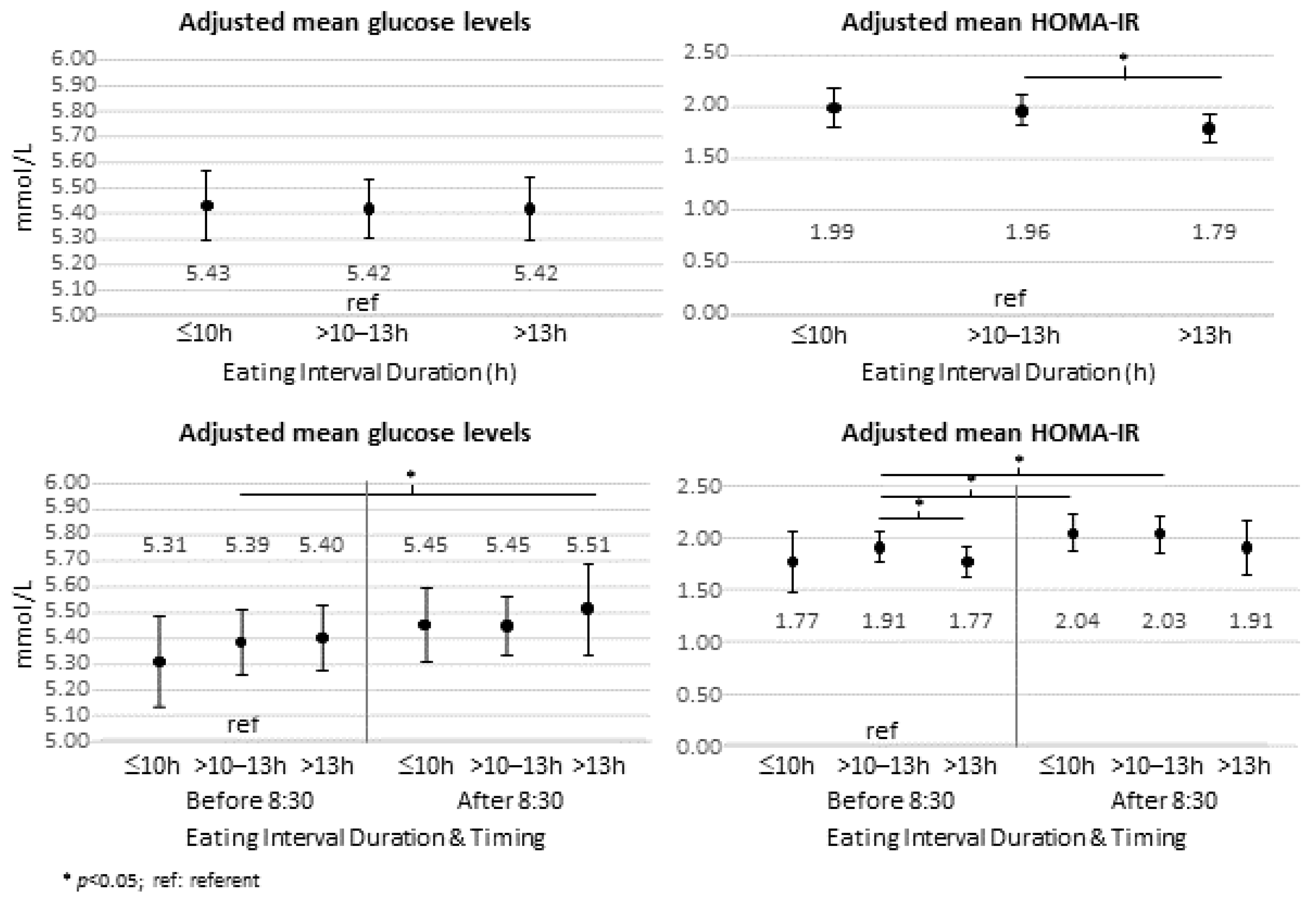
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef] [PubMed]
- Stenvers, D.J.; Scheer, F.; Schrauwen, P.; la Fleur, S.E.; Kalsbeek, A. Circadian clocks and insulin resistance. Nat. Rev. Endocrinol. 2019, 15, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.J.; Yang, J.N.; Garcia, J.I.; Myers, S.; Bozzi, I.; Wang, W.; Buxton, O.M.; Shea, S.A.; Scheer, F.A. Endogenous circadian system and circadian misalignment impact glucose tolerance via separate mechanisms in humans. Proc. Natl. Acad. Sci. USA 2015, 112, E2225–E2234. [Google Scholar] [CrossRef]
- Bass, J.; Takahashi, J.S. Circadian integration of metabolism and energetics. Science 2010, 330, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Dashti, H.S.; Gomez-Abellan, P.; Qian, J.; Esteban, A.; Morales, E.; Scheer, F.; Garaulet, M. Late eating is associated with cardiometabolic risk traits, obesogenic behaviors, and impaired weight loss. Am. J. Clin. Nutr. 2020, 113, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Garaulet, M.; Gomez-Abellan, P. Timing of food intake and obesity: A novel association. Physiol. Behav. 2014, 134, 44–50. [Google Scholar] [CrossRef]
- Sakai, R.; Hashimoto, Y.; Ushigome, E.; Miki, A.; Okamura, T.; Matsugasumi, M.; Fukuda, T.; Majima, S.; Matsumoto, S.; Senmaru, T.; et al. Late-night-dinner is associated with poor glycemic control in people with type 2 diabetes: The KAMOGAWA-DM cohort study. Endocr. J. 2018, 65, 395–402. [Google Scholar] [CrossRef]
- Chaix, A.; Zarrinpar, A.; Miu, P.; Panda, S. Time-restricted feeding is a preventative and therapeutic intervention against diverse nutritional challenges. Cell. Metab. 2014, 20, 991–1005. [Google Scholar] [CrossRef]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell. Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef]
- Liu, D.; Huang, Y.; Huang, C.; Yang, S.; Wei, X.; Zhang, P.; Guo, D.; Lin, J.; Xu, B.; Li, C.; et al. Calorie Restriction with or without Time-Restricted Eating in Weight Loss. N. Engl. J. Med. 2022, 386, 1495–1504. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021.
- Basner, M.; Fomberstein, K.; Razavi, F.; Banks, S.; William, J.; Rosa, R.; Dinges, D. American Time Use Survey: Sleep Time and Its Relationship to Waking Activities. Sleep 2007, 30, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Xun, P.; Iribarren, C.; Van Horn, L.; Steffen, L.; Daviglus, M.L.; Siscovick, D.; Liu, K.; He, K. Intake of fish and long-chain omega-3 polyunsaturated fatty acids and incidence of metabolic syndrome among American young adults: A 25-year follow-up study. Eur. J. Nutr. 2016, 55, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Gill, S.; Panda, S. A Smartphone App Reveals Erratic Diurnal Eating Patterns in Humans that Can Be Modulated for Health Benefits. Cell. Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef]
- Scheer, F.A.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Hsiao, T.J.; Chen, P.C. Persistent rotating shift-work exposure accelerates development of metabolic syndrome among middle-aged female employees: A five-year follow-up. Chronobiol. Int. 2009, 26, 740–755. [Google Scholar] [CrossRef] [PubMed]
- Patikorn, C.; Roubal, K.; Veettil, S.K.; Chandran, V.; Pham, T.; Lee, Y.Y.; Giovannucci, E.L.; Varady, K.A.; Chaiyakunapruk, N. Intermittent Fasting and Obesity-Related Health Outcomes: An Umbrella Review of Meta-analyses of Randomized Clinical Trials. JAMA Netw. Open 2021, 4, e2139558. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell. Metab. 2018, 27, 1212–1221.e3. [Google Scholar] [CrossRef]
- Manoogian, E.N.C.; Zadourian, A.; Lo, H.C.; Gutierrez, N.R.; Shoghi, A.; Rosander, A.; Pazargadi, A.; Ormiston, C.K.; Wang, X.; Sui, J.; et al. Feasibility of time-restricted eating and impacts on cardiometabolic health in 24-h shift workers: The Healthy Heroes randomized control trial. Cell. Metab. 2022, 34, 1442–1456.e7. [Google Scholar] [CrossRef]
- Wirth, M.D.; Zhao, L.; Turner-McGrievy, G.M.; Ortaglia, A. Associations between Fasting Duration, Timing of First and Last Meal, and Cardiometabolic Endpoints in the National Health and Nutrition Examination Survey. Nutrients 2021, 13, 2686. [Google Scholar] [CrossRef]
- Lowe, D.A.; Wu, N.; Rohdin-Bibby, L.; Moore, A.H.; Kelly, N.; Liu, Y.E.; Philip, E.; Vittinghoff, E.; Heymsfield, S.B.; Olgin, J.E.; et al. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men With Overweight and Obesity: The TREAT Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1491–1499. [Google Scholar] [CrossRef] [PubMed]
- Phillips, N.E.; Mareschal, J.; Schwab, N.; Manoogian, E.N.C.; Borloz, S.; Ostinelli, G.; Gauthier-Jaques, A.; Umwali, S.; Gonzalez Rodriguez, E.; Aeberli, D.; et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients 2021, 13, 1042. [Google Scholar] [CrossRef] [PubMed]
- Chia, C.W.; Egan, J.M.; Ferrucci, L. Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk. Circ. Res. 2018, 123, 886–904. [Google Scholar] [CrossRef] [PubMed]
- Rangaraj, V.R.; Siddula, A.; Burgess, H.J.; Pannain, S.; Knutson, K.L. Association between Timing of Energy Intake and Insulin Sensitivity: A Cross-Sectional Study. Nutrients 2020, 12, 503. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, M.; Hatamoto, Y.; Tajiri, E.; Matsumoto, N.; Tanaka, S.; Yoshimura, E. An Earlier First Meal Timing Associates with Weight Loss Effectiveness in A 12-Week Weight Loss Support Program. Nutrients 2022, 14, 249. [Google Scholar] [CrossRef]
- Nakamura, K.; Tajiri, E.; Hatamoto, Y.; Ando, T.; Shimoda, S.; Yoshimura, E. Eating Dinner Early Improves 24-h Blood Glucose Levels and Boosts Lipid Metabolism after Breakfast the Next Day: A Randomized Cross-Over Trial. Nutrients 2021, 13, 2424. [Google Scholar] [CrossRef]
- Bandin, C.; Scheer, F.A.; Luque, A.J.; Avila-Gandia, V.; Zamora, S.; Madrid, J.A.; Gomez-Abellan, P.; Garaulet, M. Meal timing affects glucose tolerance, substrate oxidation and circadian-related variables: A randomized, crossover trial. Int. J. Obes. 2015, 39, 828–833. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Wainstein, J.; Ahren, B.; Landau, Z.; Bar-Dayan, Y.; Froy, O. Fasting until noon triggers increased postprandial hyperglycemia and impaired insulin response after lunch and dinner in individuals with type 2 diabetes: A randomized clinical trial. Diabetes Care 2015, 38, 1820–1826. [Google Scholar] [CrossRef]
- Jamshed, H.; Steger, F.L.; Bryan, D.R.; Richman, J.S.; Warriner, A.H.; Hanick, C.J.; Martin, C.K.; Salvy, S.J.; Peterson, C.M. Effectiveness of Early Time-Restricted Eating for Weight Loss, Fat Loss, and Cardiometabolic Health in Adults With Obesity: A Randomized Clinical Trial. JAMA Intern. Med. 2022, 182, 953–962. [Google Scholar] [CrossRef]
- Van Cauter, E.; Blackman, J.D.; Roland, D.; Spire, J.P.; Refetoff, S.; Polonsky, K.S. Modulation of glucose regulation and insulin secretion by circadian rhythmicity and sleep. J. Clin. Investig. 1991, 88, 934–942. [Google Scholar] [CrossRef]
- Froy, O.; Garaulet, M. The Circadian Clock in White and Brown Adipose Tissue: Mechanistic, Endocrine, and Clinical Aspects. Endocr. Rev. 2018, 39, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Allison, K.C.; Goel, N. Timing of eating in adults across the weight spectrum: Metabolic factors and potential circadian mechanisms. Physiol. Behav. 2018, 192, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S.; Aronne, L.J.; Astrup, A.; de Cabo, R.; Cantley, L.C.; Friedman, M.I.; Heymsfield, S.B.; Johnson, J.D.; King, J.C.; Krauss, R.M.; et al. The carbohydrate-insulin model: A physiological perspective on the obesity pandemic. Am. J. Clin. Nutr. 2021, 114, 1873–1885. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Unweighted Mean (SD) or No. (%) | Weighted Mean or % (95% CI) * | |
|---|---|---|
| Age (years) | 49.8 (17.9) | 47.5 (46.7–48.2) |
| Women | 3920 (51.5%) | 51.9% (50.6–53.2) |
| Race and ethnicity | ||
| Mexican American | 1228 (16.1%) | 7.6% (6.2–9.2) |
| Non-Hispanic Black | 1466 (19.2%) | 10.3% (8.7–12.1) |
| Non-Hispanic White | 3755 (49.2%) | 72.1% (68.8–75.1) |
| Other Hispanic | 680 (8.9%) | 4.6% (36–5.9) |
| Other Race | 490 (6.4%) | 5.5% (4.7–6.5) |
| Education level | ||
| <9th grade | 796 (10.5%) | 5.4% (4.7–6.1) |
| 9–11th grade | 1144 (15.0%) | 11.0% (9.8–12.5) |
| High school degree/GED | 1776 (23.3%) | 23.3% (21.5–25.2) |
| Some College or AA degree | 2170 (28.5%) | 30.6% (29.0–32.3) |
| College graduate or above | 1733 (22.7%) | 29.7% (27.3–32.3) |
| Current Smoker | 1518 (19.9%) | 20.0% (18.5–21.6) |
| Alcohol Use (drinks/week) | 1.0 (1.8) | 1.2 (1.1–1.3) |
| Self-reported sleep duration (hours) | 6.8 (1.4) | 6.9 (6.8–6.9) |
| BMI (kg/m2) | 29.0 (6.7) | 28.8 (28.6–29.1) |
| Underweight (BMI < 18.5 kg/m2) | 112 (1.5%) | 1.4% (1.1–1.8) |
| Ideal weight (BMI 18.5– < 25 kg/m2) | 2095 (27.5%) | 29.7% (28.0–31.4) |
| Overweight (BMI 25– < 30 kg/m2) | 2596 (34.1%) | 33.7% (32.3–35.0) |
| Obese (BMI ≥ 30 kg/m2) | 2816 (37.0%) | 35.3% (33.6–37.0) |
| Diabetes | 1111 (14.5%) | 10.8% (9.8–11.8) |
| Fasting Glucose (mmol/L) | 6.0 (1.9) | 5.8 (5.7–5.9) |
| HOMA-IR | 3.8 (5.3) | 3.4 (3.2–3.5) |
| Total kcal/day | 2046 (788) | 2118 (2090–2146) |
| Eating Interval Duration (h) | 11.8 (2.2) | 12.0 (11.9–12.0) |
| <10 | 1491 (19.6%) | 18.0% (16.8–19.3) |
| 10–13 | 4083 (53.6%) | 52.1% (50.4–53.8) |
| >13 | 2045 (26.8%) | 30.0% (28.5–31.4) |
| Eating Interval Start Time (hh:mm) | 8:29 (1:52) | 8:21 (8:15–8:26) |
| At or before 8:30 | 4536 (59.5%) | 62.5% (60.1–64.8) |
| After 8:30 | 3083 (40.5%) | 37.5% (35.2–40.0) |
| Eating Interval Duration + Start Time | ||
| At/before 8:30 + <10 h | 294 (3.9%) | 3.3% (2.8–3.9) |
| At/before 8:30 + 10–13 h | 2420 (31.8%) | 32.4% (30.3–34.5) |
| At/before 8:30 + >13 h | 1822 (23.9%) | 26.8% (25.3–28.4) |
| After 8:30 + <10 h | 1197 (15.7%) | 14.7% (13.5–16.0) |
| After 8:30 + 10–13 h | 1663 (21.8%) | 19.7% (18.4–21.2) |
| After 8:30 + >13 h | 223 (2.9%) | 3.1% (2.7–3.7) |
| (ln) Fasting Glucose | (ln) HOMA-IR | |||
|---|---|---|---|---|
| Regression Coeff | 95% CI | Regression Coeff | 95% CI | |
| Eating Duration (hours) | 0.002 | −0.001, 0.005 | −0.005 | −0.017, 0.007 |
| Eating Start Time (hours) | 0.006 | 0.003, 0.008 | 0.030 | 0.016, 0.044 |
| Total Kcal | Protein (g) | Total Carbohydrates (g) | Total Sugars (g) | Total Fat (g) | Total Saturated Fatty Acids (g) | Total Mono-Unsaturated Fatty Acids (g) | Total Poly-Unsaturated Fatty Acids (g) | Dietary Fiber (g) | |
|---|---|---|---|---|---|---|---|---|---|
| Eating Duration Groups | |||||||||
| <10 h | 1846.1 * | 74.1 * | 225.2 * | 97.9 * | 70.1 * | 22.3 * | 25.4 * | 15.5 * | 14.2 * |
| 10–13 h (ref) | 2086.4 | 82.3 | 253.6 | 111.6 | 79.0 | 25.8 | 28.6 | 17.7 | 17.2 |
| >13 h | 2332.3 * | 91.2 * | 280.8 * | 128.7 * | 89.1 * | 29.5 * | 32.4 * | 19.6 * | 18.5 * |
| Eating Duration + Start Time Groups | |||||||||
| At/before 8:30 and: | |||||||||
| <10 h | 1747.5 * | 72.0 * | 215.9 * | 92.2 * | 64.9 * | 21.3 * | 23.5 * | 14.2 * | 16.3 |
| 10–13 h (ref) | 2044.5 | 82.2 | 245.9 | 106.7 | 78.0 | 25.3 | 28.3 | 17.6 | 17.4 |
| >13 h | 2306.8 * | 90.8 * | 277.6 * | 127.2 * | 88.3 * | 29.2 * | 32.1 * | 19.4 * | 18.5 * |
| After 8:30 and: | |||||||||
| <10 h | 1868.5 * | 74.6 * | 227.3 * | 99.1 * | 71.2 * | 22.6 * | 25.9 * | 15.8 * | 13.8 * |
| 10–13 h | 2156.0 | 82.4 | 266.4 * | 119.7 * | 80.8 | 26.7 * | 29.2 | 17.9 | 16.9 |
| >13 h | 2562.5 * | 95.3 * | 309.0 * | 142.7 * | 96.5 * | 32.4 * | 34.8 * | 21.1 * | 18.3 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, M.; Reutrakul, S.; Petersen, G.; Knutson, K.L. Associations between Timing and Duration of Eating and Glucose Metabolism: A Nationally Representative Study in the U.S. Nutrients 2023, 15, 729. https://doi.org/10.3390/nu15030729
Ali M, Reutrakul S, Petersen G, Knutson KL. Associations between Timing and Duration of Eating and Glucose Metabolism: A Nationally Representative Study in the U.S. Nutrients. 2023; 15(3):729. https://doi.org/10.3390/nu15030729
Chicago/Turabian StyleAli, Marriam, Sirimon Reutrakul, Gregory Petersen, and Kristen L. Knutson. 2023. "Associations between Timing and Duration of Eating and Glucose Metabolism: A Nationally Representative Study in the U.S." Nutrients 15, no. 3: 729. https://doi.org/10.3390/nu15030729
APA StyleAli, M., Reutrakul, S., Petersen, G., & Knutson, K. L. (2023). Associations between Timing and Duration of Eating and Glucose Metabolism: A Nationally Representative Study in the U.S. Nutrients, 15(3), 729. https://doi.org/10.3390/nu15030729