
Malnutrition Screening Tools Are Not Sensitive Enough to Identify Older Hospital Patients with Malnutrition

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
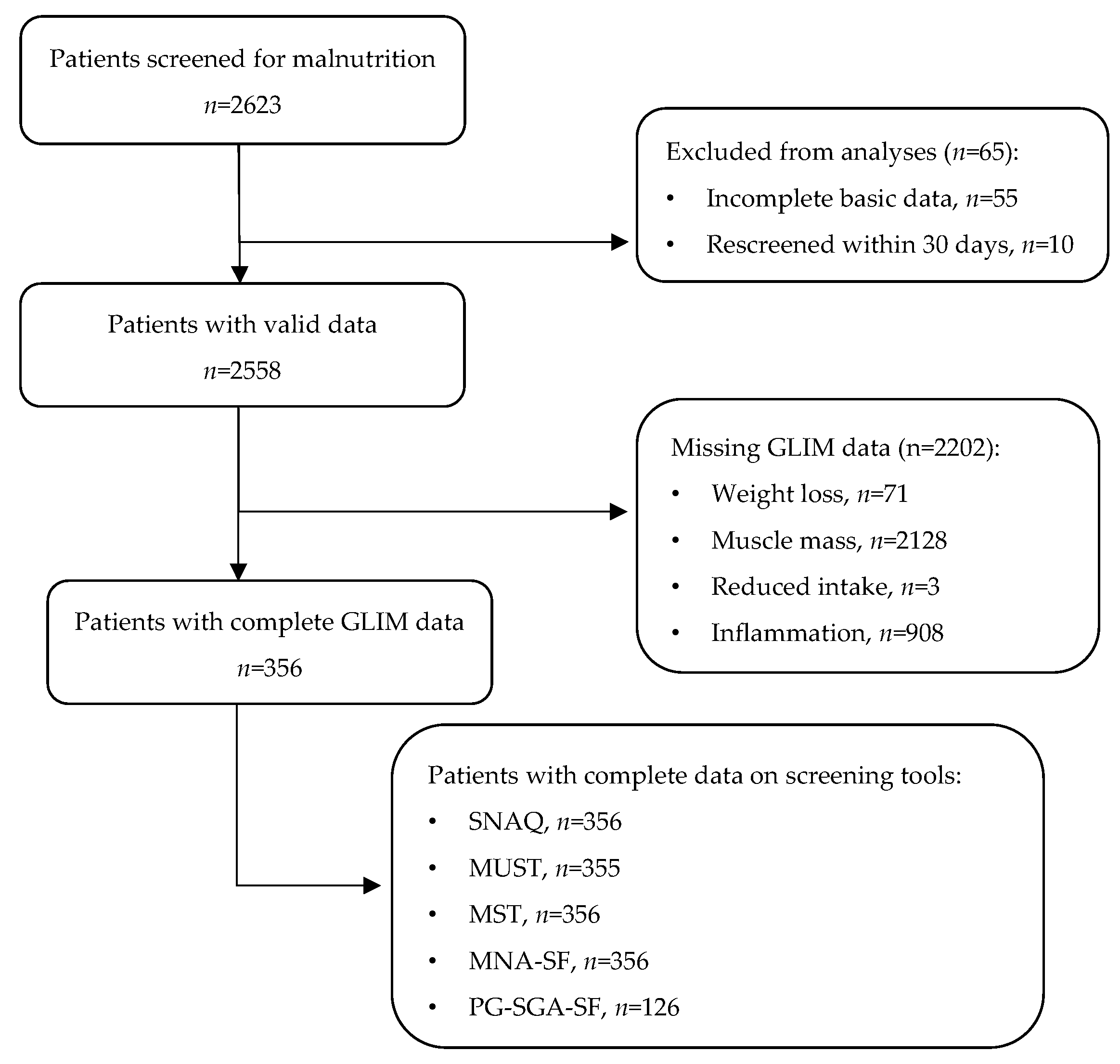
2.1. Study Design and Participants
2.2. Screening Tools
2.3. GLIM Criteria
- Reduced food intake or assimilation: having a severely decreased appetite or having answered ‘yes’ on the malabsorption question, ‘Did you suffer from dysphagia, nausea, vomiting, diarrhea, constipation, or abdominal pain?’ [10];
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Prevalence of Malnutrition
3.3. Concurrent Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellanti, F.; Lo Buglio, A.; Quiete, S.; Vendemiale, G. Malnutrition in Hospitalized Old Patients: Screening and Diagnosis, Clinical Outcomes, and Management. Nutrients 2022, 14, 910. [Google Scholar] [CrossRef]
- Dent, E.; Wright, O.R.L.; Woo, J.; Hoogendijk, E.O. Malnutrition in older adults. Lancet 2023, 401, 951–966. [Google Scholar] [CrossRef] [PubMed]
- Meyer, F.; Valentini, L. Disease-Related Malnutrition and Sarcopenia as Determinants of Clinical Outcome. Visc. Med. 2019, 35, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Brito, J.E.; Burgel, C.F.; Lima, J.; Chites, V.S.; Saragiotto, C.B.; Rabito, E.I.; Silva, F.M. GLIM criteria for malnutrition diagnosis of hospitalized patients presents satisfactory criterion validity: A prospective cohort study. Clin. Nutr. 2021, 40, 4366–4372. [Google Scholar] [CrossRef] [PubMed]
- Pourhassan, M.; Rommersbach, N.; Lueg, G.; Klimek, C.; Schnatmann, M.; Liermann, D.; Janssen, G.; Wirth, R. The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients. Nutrients 2020, 12, 1387. [Google Scholar] [CrossRef] [PubMed]
- Kaegi-Braun, N.; Kilchoer, F.; Dragusha, S.; Gressies, C.; Faessli, M.; Gomes, F.; Deutz, N.E.; Stanga, Z.; Mueller, B.; Schuetz, P. Nutritional support after hospital discharge improves long-term mortality in malnourished adult medical patients: Systematic review and meta-analysis. Clin. Nutr. 2022, 41, 2431–2441. [Google Scholar] [CrossRef] [PubMed]
- Power, L.; Mullally, D.; Gibney, E.R.; Clarke, M.; Visser, M.; Volkert, D.; Bardon, L.; de van der Schueren, M.A.E.; Corish, C.A.; MaNu, E.L.C. A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clin. Nutr. ESPEN 2018, 24, 1–13. [Google Scholar] [CrossRef]
- Kruizenga, H.M.; Seidell, J.C.; de Vet, H.C.W.; Wierdsma, N.J.; van Bokhorst–de van der Schueren, M.A.E. Development and validation of a hospital screening tool for malnutrition: The short nutritional assessment questionnaire (SNAQ). Clin. Nutr. 2004, 24, 75–82. [Google Scholar] [CrossRef]
- Kruizenga, H.M.; Schager, M.; van Dronkelaar, C.; Naumann, E. Protein intake during hospital admission; Dutch national data on protein intake in 339,720 malnourished patients from 2009–2019. Clin. Nutr. Open Sci. 2022, 41, 74–81. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Huo, Z.; Chong, F.; Yin, L.; Lu, Z.; Liu, J.; Xu, H. Accuracy of the GLIM criteria for diagnosing malnutrition: A systematic review and meta-analysis. Clin. Nutr. 2022, 41, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Correia, M.; Tappenden, K.A.; Malone, A.; Prado, C.M.; Evans, D.C.; Sauer, A.C.; Hegazi, R.; Gramlich, L. Utilization and validation of the Global Leadership Initiative on Malnutrition (GLIM): A scoping review. Clin. Nutr. 2022, 41, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Barazzoni, R. Validity and feasibility of the global leadership initiative on malnutrition diagnostic concept in older people: A literature review from August 2021 to August 2022. Curr. Opin. Clin. Nutr. Metab. Care 2023, 26, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Jobim Milanez, D.S.; Razzera, E.L.; da Silveira Knobloch, I.; Lima, J.; Bernardes, S.; Silva, F.M. A scoping review on the GLIM criteria for malnutrition diagnosis: Understanding how and for which purpose it has been applied in studies on hospital settings. Clin. Nutr. 2023, 42, 29–44. [Google Scholar] [CrossRef] [PubMed]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ’malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, M.; Capra, S.; Bauer, J.; Banks, M. Development of a valid and reliable malnutrition screening tool for adult acute hospital patients. Nutrition 1999, 15, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Harker, J.O.; Salva, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Ottery, F.D. Rethinking nutritional support of the cancer patient: The new field of nutritional oncology. Semin. Oncol. 1994, 21, 770–778. [Google Scholar]
- Korzilius, J.W.; Oppenheimer, S.E.; de Roos, N.M.; Wanten, G.J.A.; Zweers, H. Having breakfast has no clinically relevant effect on bioelectrical impedance measurements in healthy adults. Nutr. J. 2023, 22, 55. [Google Scholar] [CrossRef]
- Artero, A.; Saez Ramirez, T.; Muresan, B.T.; Ruiz-Berjaga, Y.; Jimenez-Portilla, A.; Sanchez-Juan, C.J. The Effect of Fasting on Body Composition Assessment in Hospitalized Cancer Patients. Nutr. Cancer 2023, 75, 1610–1618. [Google Scholar] [CrossRef]
- Nutritional Assessment Platform. Standard Operating Procedure (SOP). Available online: https://nutritionalassessment.nl/standard-operating-procedures-sops (accessed on 21 January 2021).
- Rutten, E.P.; Spruit, M.A.; Wouters, E.F. Critical view on diagnosing muscle wasting by single-frequency bio-electrical impedance in COPD. Respir. Med. 2010, 104, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Kruizenga, H.; Beijer, S.; Huisman-de Waal, G.; Jonkers-Schuitema, C.; Klos, M.; Remijnse-Meester, W.; Thijs, A.; Tieland, M.; Vasse, E.; Witteman, B. Richtlijn Ondervoeding. Stuurgroep Ondervoeding 2019, 39. [Google Scholar]
- Pourhassan, M.; Cederholm, T.; Trampisch, U.; Volkert, D.; Wirth, R. Inflammation as a diagnostic criterion in the GLIM definition of malnutrition-what CRP-threshold relates to reduced food intake in older patients with acute disease? Eur. J. Clin. Nutr. 2022, 76, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef]
- Clark, A.B.; Reijnierse, E.M.; Lim, W.K.; Maier, A.B. Prevalence of malnutrition comparing the GLIM criteria, ESPEN definition and MST malnutrition risk in geriatric rehabilitation patients: RESORT. Clin. Nutr. 2020, 39, 3504–3511. [Google Scholar] [CrossRef]
- Masson, L.F.; McNeill, G.; Tomany, J.O.; Simpson, J.A.; Peace, H.S.; Wei, L.; Grubb, D.A.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire: Use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Munoz Fernandez, S.S.; Garcez, F.B.; Alencar, J.C.G.; Cederholm, T.; Aprahamian, I.; Morley, J.E.; de Souza, H.P.; Avelino da Silva, T.J.; Ribeiro, S.M.L. Applicability of the GLIM criteria for the diagnosis of malnutrition in older adults in the emergency ward: A pilot validation study. Clin. Nutr. 2021, 40, 5447–5456. [Google Scholar] [CrossRef]
- Lima, J.; Brizola Dias, A.J.; Burgel, C.F.; Bernardes, S.; Gonzalez, M.C.; Silva, F.M. Complementarity of nutritional screening tools to GLIM criteria on malnutrition diagnosis in hospitalised patients: A secondary analysis of a longitudinal study. Clin. Nutr. 2022, 41, 2325–2332. [Google Scholar] [CrossRef] [PubMed]
- Bellanti, F.; Lo Buglio, A.; Quiete, S.; Pellegrino, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. J. Clin. Med. 2020, 9, 1898. [Google Scholar] [CrossRef] [PubMed]
- IJmker-Hemink, V.; Heerschop, S.; Wanten, G.; van den Berg, M. Evaluation of the Validity and Feasibility of the GLIM Criteria Compared with PG-SGA to Diagnose Malnutrition in Relation to One-Year Mortality in Hospitalized Patients. J. Acad. Nutr. Diet. 2022, 122, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Allard, J.P.; Keller, H.; Gramlich, L.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R. GLIM criteria has fair sensitivity and specificity for diagnosing malnutrition when using SGA as comparator. Clin. Nutr. 2020, 39, 2771–2777. [Google Scholar] [CrossRef]
- Swan, I.; Nyulasi, I.; Collins, K.; Weir-Phyland, J.; Bolster, D.; Burgell, R.; Fineberg, D.; Johnson, W.; King, S.; Leong, R.; et al. Identification and management of malnutrition in hospitalised patients: A survey of staff knowledge and attitudes. Clin. Nutr. Exp. 2020, 31, 8–18. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Barazzoni, R.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Higashiguchi, T.; Shi, H.P.; Bischoff, S.C.; Boirie, Y.; Carrasco, F.; Cruz-Jentoft, A.; et al. Guidance for assessment of the muscle mass phenotypic criterion for the Global Leadership Initiative on Malnutrition (GLIM) diagnosis of malnutrition. Clin. Nutr. 2022, 41, 1425–1433. [Google Scholar] [CrossRef]


{kind=link}
| Patients | n = 356 |
|---|---|
| Sex, males, n (%) | 192 (54) |
| Age in years, median (IQR) | 70 (63–77) |
| BMI in kg/m2, median (IQR) | 24.8 (22.6–28.1) |
| Hospital, n (%) | |
| Amsterdam UMC, location AMC | 22 (6) |
| Amsterdam UMC, location VUmc | 152 (43) |
| OLVG, location East | 110 (31) |
| OLVG, location West | 43 (12) |
| BovenIJ Hospital | 29 (8) |
| Ward, n (%) | |
| Acute admission | 257 (72) |
| Internal medicine | 18 (5) |
| Cardiology | 27 (8) |
| Neurology | 18 (5) |
| Pulmonary | 13 (4) |
| Gastroenterology | 10 (3) |
| Geriatric | 3 (<1) |
| Other | 14 (4) |
| n | Prevalence, n (%) | |
|---|---|---|
| SNAQ | 356 | |
| Malnutrition (≥3) | 88 (25) | |
| Moderate malnutrition (≥2) | 115 (32) | |
| MUST | 355 | |
| Malnutrition (≥2) | 65 (18) | |
| Risk of malnutrition (≥1) | 126 (36) | |
| MST | 356 | |
| Malnutrition (≥2) | 111 (31) | |
| MNA-SF | 356 | |
| Malnutrition (≤7) | 52 (15) | |
| Risk of malnutrition (≤11) | 206 (60) | |
| PGSGA-SF | 126 | |
| Malnutrition (≥9) | 65 (52) | |
| Risk of malnutrition (≥4) | 88 (70) |
| n | Prevalence, n (%) | |
|---|---|---|
| GLIM | 356 | 148 (42) |
| Phenotypic criteria | 356 | 156 (44) |
| Weight loss | 356 | 113 (32) |
| Low BMI | 356 | 59 (17) |
| Low muscle mass | 356 | 83 (23) |
| Etiologic criteria | 356 | 330 (93) |
| Reduced intake | 356 | 251 (71) |
| Inflammation | 356 | 294 (83) |
| SNAQ (n = 356) | MUST (n = 356) | MST (n = 356) | MNA-SF (n = 356) | PG-SGA-SF (n = 126) | |||||
|---|---|---|---|---|---|---|---|---|---|
| A (≥3) | B (≥2) | A (≥2) | B (≥1) | A (≥2) | A (≤7) | B (≤11) | A (≥9) | B (≥4) | |
| False positive, n | 5 | 17 | 7 | 11 | 16 | 5 | 79 | 27 | 38 |
| False negative, n | 65 | 50 | 89 | 32 | 53 | 203 | 21 | 18 | 6 |
| Sensitivity, % | 56 | 66 | 40 | 78 | 64 | 32 | 86 | 68 | 89 |
| Specificity, % | 98 | 92 | 97 | 95 | 92 | 98 | 62 | 61 | 46 |
| PPV, % | 94 | 85 | 90 | 91 | 86 | 90 | 62 | 59 | 57 |
| NPV, % | 76 | 79 | 70 | 86 | 78 | 67 | 86 | 71 | 84 |
| Cohen’s kappa | 0.57 | 0.60 | 0.39 | 0.75 | 0.59 | 0.21 | 0.45 | 0.29 | 0.33 |
| McNemar | p < 0.001 | p < 0.001 | p < 0.001 | p = 0.002 | p < 0.001 | p < 0.001 | p < 0.001 | p = 0.233 | p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Dronkelaar, C.; Tieland, M.; Cederholm, T.; Reijnierse, E.M.; Weijs, P.J.M.; Kruizenga, H. Malnutrition Screening Tools Are Not Sensitive Enough to Identify Older Hospital Patients with Malnutrition. Nutrients 2023, 15, 5126. https://doi.org/10.3390/nu15245126
van Dronkelaar C, Tieland M, Cederholm T, Reijnierse EM, Weijs PJM, Kruizenga H. Malnutrition Screening Tools Are Not Sensitive Enough to Identify Older Hospital Patients with Malnutrition. Nutrients. 2023; 15(24):5126. https://doi.org/10.3390/nu15245126
Chicago/Turabian Stylevan Dronkelaar, Carliene, Michael Tieland, Tommy Cederholm, Esmee M. Reijnierse, Peter J. M. Weijs, and Hinke Kruizenga. 2023. "Malnutrition Screening Tools Are Not Sensitive Enough to Identify Older Hospital Patients with Malnutrition" Nutrients 15, no. 24: 5126. https://doi.org/10.3390/nu15245126
APA Stylevan Dronkelaar, C., Tieland, M., Cederholm, T., Reijnierse, E. M., Weijs, P. J. M., & Kruizenga, H. (2023). Malnutrition Screening Tools Are Not Sensitive Enough to Identify Older Hospital Patients with Malnutrition. Nutrients, 15(24), 5126. https://doi.org/10.3390/nu15245126