
Enablers and Barriers Related to Preconception Physical Activity: Insights from Women of Reproductive Age Using Mixed Methods

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Quantitative Study
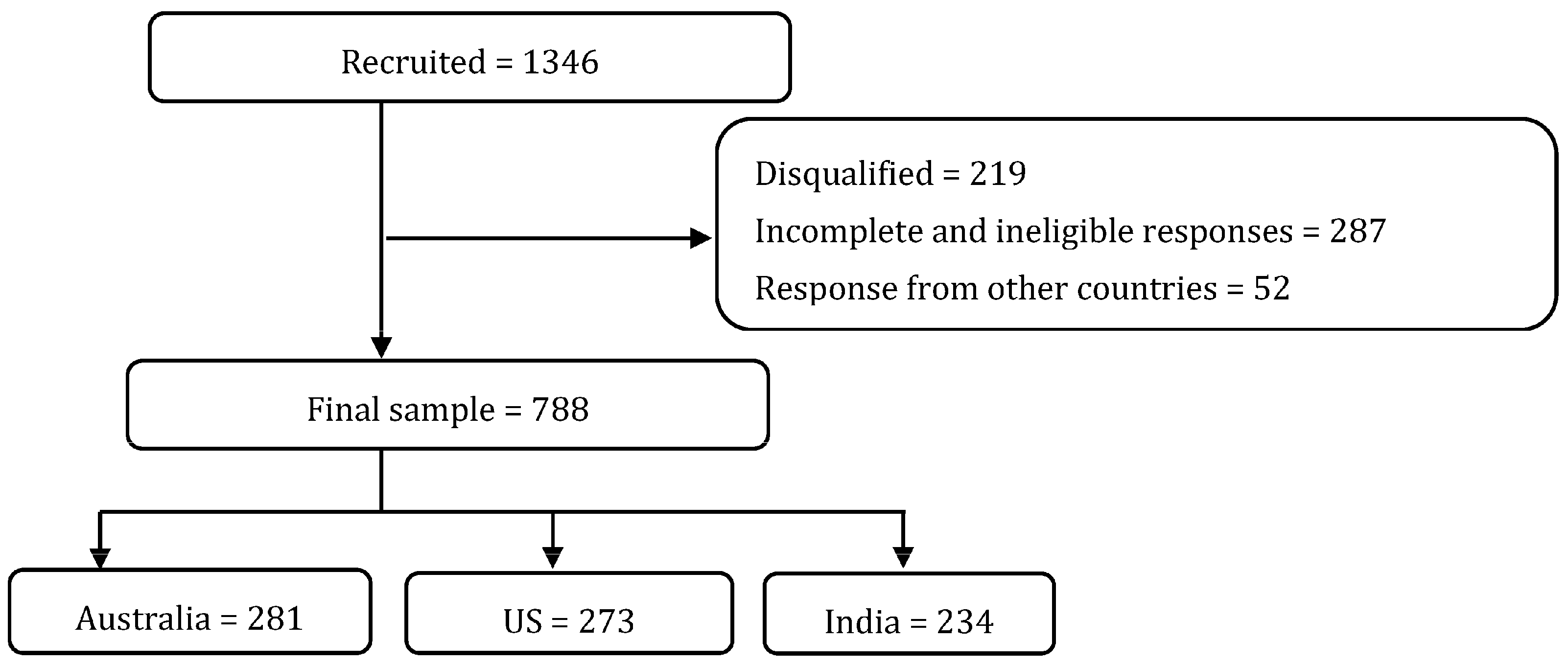
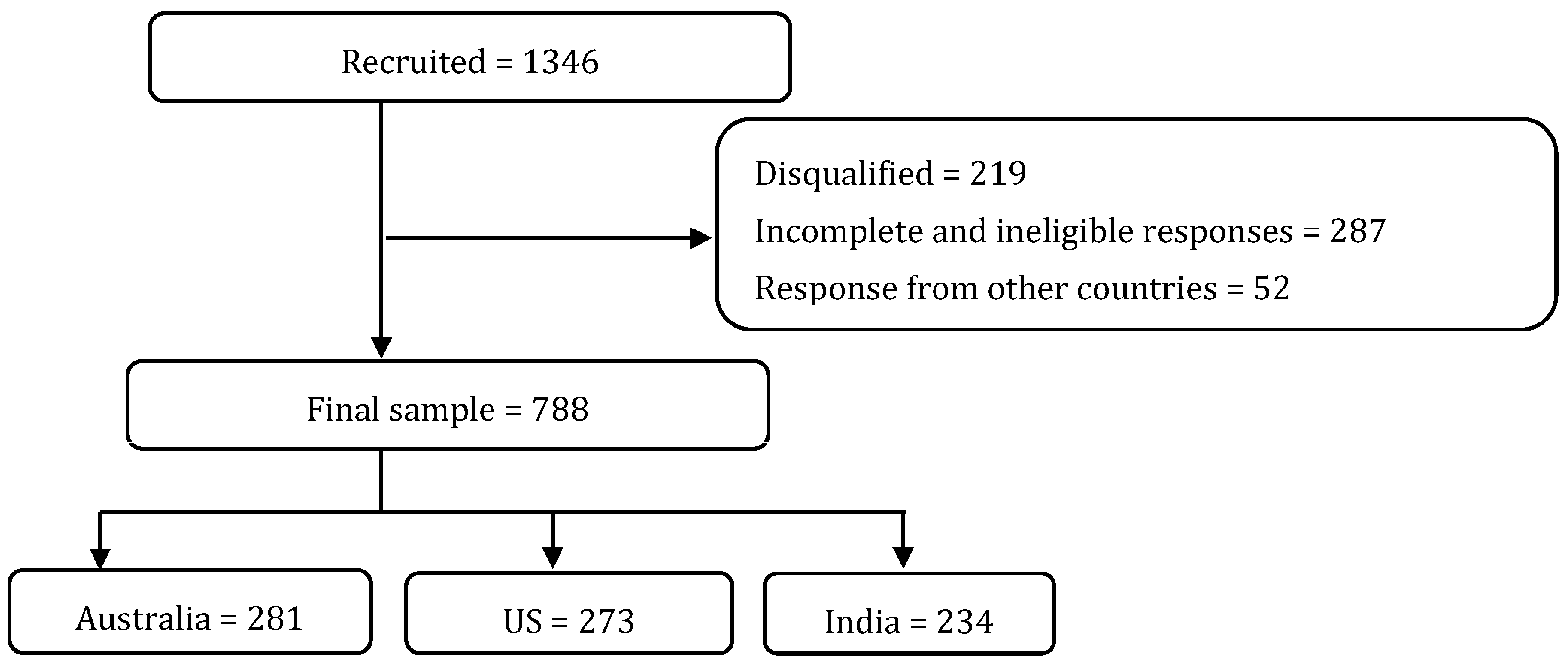
2.1.1. Study Population
2.1.2. Measures and Data Collection
2.1.3. Sample Size Calculation and Data Analysis
2.2. Qualitative Study
2.2.1. Study Population
2.2.2. Measures and Data Collection
2.2.3. Qualitative Analysis
2.3. Mixed Methods Integration and Analysis
3. Results
3.1. Quantitative Study
3.1.1. Participant Characteristics
3.1.2. Associations between PA Levels and Enablers and Barriers Related to PA
3.2. Qualitative Study
3.2.1. Demographic Characteristics
3.2.2. Integration of Quantitative and Qualitative Study Findings Mapped to the COM-B Model
3.3. Capability
3.4. Motivation
3.5. Opportunity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, B.; Hall, J.; Skouteris, H.; Currie, S. Defining preconception: Exploring the concept of a preconception population. BMC Pregnancy Childbirth 2020, 20, 280. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the beginning: Nutrition and lifestyle in the preconception period and its importance for future health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Chandranipapongse, W.; Koren, G. Preconception counseling for preventable risks. Can. Fam. Physician 2013, 59, 737–739. [Google Scholar] [PubMed]
- Tobias, D.K.; Zhang, C.; van Dam, R.M.; Bowers, K.; Hu, F.B. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: A meta-analysis. Diabetes Care 2011, 34, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Kruszewski, A.; Przybysz, P.; Kacperczyk-Bartnik, J.; Dobrowolska-Redo, A.; Romejko-Wolniewicz, E. Physical Activity during Preconception Impacts Some Maternal Outcomes-A Cross-Sectional Study on a Population of Polish Women. Int. J. Environ. Res. Public Health 2023, 20, 3581. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Saugstad, O.D.; Henriksen, T.; Tonstad, S. Physical activity and the risk of preeclampsia: A systematic review and meta-analysis. Epidemiology 2014, 25, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.L.; Brown, W.J.; Hayman, M.; Moran, L.J.; Redman, L.M. The Role of Physical Activity in Preconception, Pregnancy and Postpartum Health. Semin. Reprod. Med. 2016, 34, e28–e37. [Google Scholar] [CrossRef]
- Tosh, C.; Kavanagh, K.; Flynn, A.C.; Stephenson, J.; White, S.L.; Catalao, R.; Wilson, C.A. The physical-mental health interface in the preconception period: Analysis of 131 182 women planning pregnancy in the UK. BJOG 2023, 130, 1028–1037. [Google Scholar] [CrossRef]
- Owe, K.M.; Nystad, W.; Bø, K. Correlates of regular exercise during pregnancy: The Norwegian Mother and Child Cohort Study. Scand. J. Med. Sci. Sports 2009, 19, 637–645. [Google Scholar] [CrossRef]
- Tornquist, L.; Tornquist, D.; Mielke, G.I.; da Silveira, M.F.; Hallal, P.C.; Domingues, M.R. Maternal Physical Activity Patterns in the 2015 Pelotas Birth Cohort: From Preconception to Postpartum. J. Phys. Act. Health 2023, 20, 868–877. [Google Scholar] [CrossRef]
- Pan, K.; Bazzano, L.A.; Betha, K.; Charlton, B.M.; Chavarro, J.E.; Cordero, C.; Gunderson, E.P.; Haggerty, C.L.; Hart, J.E.; Jukic, A.M.; et al. Large-scale data harmonization across prospective studies: The Preconception Period Analysis of Risks and Exposures Influencing health and Development (PrePARED) consortium. Am. J. Epidemiol. 2023. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Physical Activity. Available online: https://www.aihw.gov.au/reports/physical-activity/physical-activity (accessed on 5 October 2023).
- Chuang, C.H.; Weisman, C.S.; Hillemeier, M.M.; Schwarz, E.B.; Camacho, F.T.; Dyer, A.M. Pregnancy intention and health behaviors: Results from the Central Pennsylvania Women’s Health Study cohort. Matern. Child Health J. 2010, 14, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef] [PubMed]
- Santo, E.C.; Forbes, P.W.; Oken, E.; Belfort, M.B. Determinants of physical activity frequency and provider advice during pregnancy. BMC Pregnancy Childbirth 2017, 17, 286. [Google Scholar] [CrossRef] [PubMed]
- St-Laurent, A.; Savard, C.; Plante, A.S.; Gagnon, M.; Robitaille, J.; Lemieux, S.; Ruchat, S.M.; Morisset, A.S. Health-Related Preconception Factors: Adherence to Guidelines and Associations with Weight Status. J. Acad. Nutr. Diet. 2022, 122, 1911–1921. [Google Scholar] [CrossRef]
- Hill, B.; Ling, M.; Mishra, G.; Moran, L.J.; Teede, H.J.; Bruce, L.; Skouteris, H. Lifestyle and Psychological Factors Associated with Pregnancy Intentions: Findings from a Longitudinal Cohort Study of Australian Women. Int. J. Environ. Res. Public Health 2019, 16, 5094. [Google Scholar] [CrossRef]
- Xie, Y.; Madkour, A.S.; Harville, E.W. Preconception Nutrition, Physical Activity, and Birth Outcomes in Adolescent Girls. J. Pediatr. Adolesc. Gynecol. 2015, 28, 471–476. [Google Scholar] [CrossRef]
- Kandel, P.; Lim, S.; Pirotta, S.; Skouteris, H.; Moran, L.J.; Hill, B. Enablers and barriers to women’s lifestyle behavior change during the preconception period: A systematic review. Obes. Rev. 2021, 22, e13235. [Google Scholar] [CrossRef]
- Nkrumah, I.; North, M.; Kothe, E.; Chai, T.L.; Pirotta, S.; Lim, S.; Hill, B. The Relationship Between Pregnancy Intentions and Diet or Physical Activity Behaviors in the Preconception and Antenatal Periods: A Systematic Review and Meta-Analysis. J. Midwifery Womens Health 2020, 65, 660–680. [Google Scholar] [CrossRef]
- Pico, M.L.; Grunnet, L.G.; Vinter, C.A.; Aagaard-Hansen, J.; Kragelund Nielsen, K. Barriers and facilitators for sustainable weight loss in the pre-conception period among Danish women with overweight or obesity—A qualitative study. BMC Public Health 2023, 23, 1778. [Google Scholar] [CrossRef]
- Hui, S.S.; Hui, G.P.; Xie, Y.J. Association between Physical Activity Knowledge and Levels of Physical Activity in Chinese Adults with Type 2 Diabetes. PLoS ONE 2014, 9, e115098. [Google Scholar] [CrossRef]
- Abula, K.; Gröpel, P.; Chen, K.; Beckmann, J. Does knowledge of physical activity recommendations increase physical activity among Chinese college students? Empirical investigations based on the transtheoretical model. J. Sport Health Sci. 2018, 7, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Ogunwole, S.M.; Chen, X.; Mitta, S.; Minhas, A.; Sharma, G.; Zakaria, S.; Vaught, A.J.; Toth-Manikowski, S.M.; Smith, G. Interconception Care for Primary Care Providers: Consensus Recommendations on Preconception and Postpartum Management of Reproductive-Age Patients With Medical Comorbidities. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 872–890. [Google Scholar] [CrossRef]
- Hill, B. Expanding our understanding and use of the ecological systems theory model for the prevention of maternal obesity: A new socioecological framework. Obes. Rev. 2021, 22, e13147. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2017; ISBN 978-150-639-467-1. [Google Scholar]
- Johnson, R.B.; Onwuegbuzie, A.J.; Turner, L.A. Toward a Definition of Mixed Methods Research. J. Mix. Methods Res. 2007, 1, 112–133. [Google Scholar] [CrossRef]
- Curry, L.; Nunez-Smith, M. Mixed Methods in Health Sciences Research: A Practical Primer; Sage Publications: Thousand Oaks, CA, USA, 2014; Volume 1, ISBN 978-148-335-455-2. [Google Scholar]
- Qualtrics. Available online: https://www.qualtrics.com/au/ (accessed on 12 April 2021).
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Physiopedia, Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short Form. Available online: https://www.physio-pedia.com/images/c/c7/Quidelines_for_interpreting_the_IPAQ.pdf (accessed on 15 April 2022).
- Brancato, G.; Macchia, S.; Murgia, M.; Signore, M.; Simeoni, G.; Blanke, K.; Körner, T.; Nimmergut, A.; Lima, P.; Paulino, R.; et al. Handbook of Recommended Practices for Questionnaire Development and Testing in the European Statistical System. 2006. European Commission Grant Agreement 2004103000002. Available online: https://www.istat.it/it/files/2013/12/Handbook_questionnaire_development_2006.pdf (accessed on 3 March 2020).
- Benton, M.R.; Tape, N.; Deussen, A.R.; Turnbull, D.; Dodd, J.M. Barriers to and facilitators for addressing overweight and obesity before conception: A qualitative study. Women Birth 2021, 34, e493–e497. [Google Scholar] [CrossRef]
- Fischhoff, B.; Slovic, P.; Lichtenstein, S. Knowing with certainty: The appropriateness of extreme confidence. J. Exp. Psychol. Hum. Percept. Perform. 1977, 3, 552–564. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Birkimer, J.C.; Brown, J.H. Back to basics: Percentage agreement measures are adequate, but there are easier ways. J. Appl. Behav. Anal. 1979, 12, 535–543. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs-principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [PubMed]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research Through Joint Displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Clark, V.L.P.; Sanders, K. The use of visual displays in mixed methods research. In Use of Visual Displays in Research and Testing: Coding, Interpreting, and Reporting Data; Information Age Publishing: Charlotte, NC, USA, 2015; pp. 177–206. ISBN 978-1-68123-101-3. [Google Scholar]
- McCluskey, A.; Lovarini, M. Providing education on evidence-based practice improved knowledge but did not change behaviour: A before and after study. BMC Med. Educ. 2005, 5, 40. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Kraus, W.E.; Powell, K.E.; Campbell, W.W.; Janz, K.F.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L. Association between Bout Duration of Physical Activity and Health: Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1213–1219. [Google Scholar] [CrossRef]
- Jacobs, E.J.A.; van Steijn, M.E.; van Pampus, M.G. Internet usage of women attempting pregnancy and pregnant women in the Netherlands. Sex. Reprod. Healthc. 2019, 21, 9–14. [Google Scholar] [CrossRef]
- Narasimhulu, D.M.; Karakash, S.; Weedon, J.; Minkoff, H. Patterns of Internet Use by Pregnant Women, and Reliability of Pregnancy-Related Searches. Matern. Child Health J. 2016, 20, 2502–2509. [Google Scholar] [CrossRef]
- Green, E.C.; Murphy, E.M.; Gryboski, K. The Health Belief Model. In The Wiley Encyclopedia of Health Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2020; pp. 211–214. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986; ISBN 978-0-13-815614-5. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Peng, B.; Ng, J.Y.Y.; Ha, A.S. Barriers and facilitators to physical activity for young adult women: A systematic review and thematic synthesis of qualitative literature. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 23. [Google Scholar] [CrossRef]
- King, A.C.; Castro, C.; Wilcox, S.; Eyler, A.A.; Sallis, J.F.; Brownson, R.C. Personal and environmental factors associated with physical inactivity among different racial-ethnic groups of U.S. middle-aged and older-aged women. Health Psychol. 2000, 19, 354–364. [Google Scholar] [CrossRef]
- Ware, L.J.; Prioreschi, A.; Bosire, E.; Cohen, E.; Draper, C.E.; Lye, S.J.; Norris, S.A. Environmental, Social, and Structural Constraints for Health Behavior: Perceptions of Young Urban Black Women during the Preconception Period-A Healthy Life Trajectories Initiative. J. Nutr. Educ. Behav. 2019, 51, 946–957. [Google Scholar] [CrossRef]
- House, J.S. Social support and social structure. Sociol. Forum 1987, 2, 135–146. [Google Scholar] [CrossRef]
- Garriguet, D.; Colley, R.; Bushnik, T. Parent-Child association in physical activity and sedentary behaviour. Health Rep. 2017, 28, 3–11. [Google Scholar]
- Mailey, E.L.; Huberty, J.; Dinkel, D.; McAuley, E. Physical activity barriers and facilitators among working mothers and fathers. BMC Public Health 2014, 14, 657. [Google Scholar] [CrossRef]
- Pickett, K.E.; Wilkinson, R.G. Income inequality and health: A causal review. Soc. Sci. Med. 2015, 128, 316–326. [Google Scholar] [CrossRef]
- Addy, C.L.; Wilson, D.K.; Kirtland, K.A.; Ainsworth, B.E.; Sharpe, P.; Kimsey, D. Associations of perceived social and physical environmental supports with physical activity and walking behavior. Am. J. Public Health 2004, 94, 440–443. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Donovan, R.J. Relative influences of individual, social environmental, and physical environmental correlates of walking. Am. J. Public Health 2003, 93, 1583–1589. [Google Scholar] [CrossRef]
- Humpel, N.; Owen, N.; Leslie, E. Environmental factors associated with adults’ participation in physical activity: A review. Am. J. Prev. Med. 2002, 22, 188–199. [Google Scholar] [CrossRef]

{kind=link}
| Demographic Characteristic | Total Sample (n = 788) | Australia (n = 281) | US (n = 273) | India (n = 234) |
|---|---|---|---|---|
| Age in years (n = 768), n (%) | ||||
| 18–24 | 141 (18.4) | 14 (5.0) | 58 (21.8) | 69 (30.8) |
| 25–34 | 313 (40.8) | 113 (40.7) | 102 (38.4) | 98 (43.8) |
| 35–45 | 314(40.9) | 151 (54.3) | 106 (39.9) | 57 (25.5) |
| Marital Status, n (%) | ||||
| Single/Never Married | 332 (42.1) | 79 (28.1) | 144 (52.8) | 109 (46.6) |
| Married/De facto | 416 (52.8) | 194 (69.0) | 99 (36.3) | 123 (52.6) |
| Divorced/Separated/Widowed | 40 (5.1) | 8 (2.6) | 30 (11.0) | 2 (0.9) |
| Household Composition (n = 786), n (%) | ||||
| Couple family with children | 383 (48.7) | 131(46.6) | 106 (39.1) | 146 (62.4) |
| Couple family without children | 133 (16.9) | 71 (25.3) | 43 (15.9) | 19 (8.1) |
| Group household | 113 (14.4) | 31 (11.0) | 42 (15.5) | 40 (17.1) |
| One parent family | 67 (8.5) | 16 (5.7) | 35 (12.9) | 16 (6.8) |
| Single person household | 90 (11.5) | 32 (11.4) | 45 (16.6) | 13 (5.6) |
| Educational Status (n = 786), n (%) | ||||
| High School not completed | 98 (12.5) | 8 (2.9) | 77 (28.3) | 13 (5.7) |
| High school graduate/Diploma | 100 (12.7) | 25 (8.9) | 61 (22.4) | 14 (6.0) |
| Trade/Vocational/Associate degree | 100 (12.7) | 58 (20.7) | 37 (13.6) | 5 (2.1) |
| Bachelor’s degree | 302 (38.4) | 109 (38.9) | 70 (25.7) | 123 (52.6) |
| Masters and above | 186 (23.7) | 80 (28.6) | 27 (10.0) | 79 (33.8) |
| Paid employment, n (%) | ||||
| Yes | 563 (71.5) | 230 (81.9) | 163 (59.7) | 170 (72.7) |
| No | 225 (28.6) | 51 (18.2) | 110 (40.3) | 64 (27.4) |
| Pregnancy plans for future (n = 787), n (%) | ||||
| Considering in next 1 or 2 years | 131 (16.7) | 51 (18.2) | 40 (14.7) | 40 (17.1) |
| Considering in next 3 to 5 years | 100 (12.7) | 31 (11.0) | 39 (14.3) | 30 (12.8) |
| Currently trying to conceive | 54 (6.9) | 21 (7.5) | 15 (5.5) | 18 (7.7) |
| Have completed my family | 76 (9.7) | 43 (15.3) | 22 (8.1) | 11 (4.7) |
| Tried and unable to get pregnant | 20 (2.5) | 4 (1.4) | 12 (4.4) | 4 (1.7) |
| No plans/Not sure/Prefer not to answer | 406 (51.6) | 131 (46.6) | 144 (52.9) | 131 (56.0) |
| Smoking Habit (n = 786), n (%) | ||||
| Never smoked cigarettes | 541 (68.8) | 200 (71.2) | 152 (56.1) | 189 (80.8) |
| Currently smoking | 113 (14.4) | 26 (9.3) | 72 (26.6) | 15 (6.4) |
| Smoked in past | 132 (16.8) | 55 (19.6) | 47 (17.3) | 30 (12.8) |
| Drinking habit (n = 787), n (%) | ||||
| 1–3 times a week | 194 (24.7) | 81 (28.8) | 82 (30.2) | 31 (13.3) |
| 2–4 times a month | 95 (12.1) | 37 (13.2) | 33 (12.1) | 25 (10.7) |
| 4 or more times a week | 40 (5.1) | 13 (4.6) | 25 (9.2) | 2 (0.9) |
| Monthly or less | 168 (21.4) | 76 (27.1) | 56 (20.6) | 36 (15.9) |
| Never | 290 (36.9) | 74 (26.3) | 76 (27.9) | 140 (59.8) |
| BMI (n = 771), n (%) | ||||
| Underweight | 73 (9.5) | 12 (4.4) | 31 (11.6) | 30 (13.2) |
| Normal | 309 (40.1) | 130 (47.3) | 74 (27.6) | 105 (46.1) |
| Overweight | 199 (25.8) | 76 (27.6) | 54 (20.2) | 69 (30.3) |
| Obesity | 190 (24.6) | 57 (20.7) | 109 (40.7) | 24 (10.5) |
| PA level, n (%) | ||||
| Low | 12 (1.5) | 9 (3.2) | 1 (0.4) | 2 (0.9) |
| Moderate | 492 (62.4) | 183 (65.1) | 167 (61.2) | 142 (60.7) |
| High | 284 (36) | 89 (31.7) | 105 (38.5) | 90 (38.5) |
| PPEBS | High PA Level | |||
|---|---|---|---|---|
| UOR (95% CI) | p-Value | aOR (95% CI) | p-Value | |
| PA during the preconception period is important. | 1.5 (1.04–2.1) | 0.027 | 1.29 (0.86–1.95) | 0.209 |
| PA during the preconception period is important for a healthy pregnancy. | 1.27 (0.89–1.82) | 0.179 | 1.15 (0.78–1.69) | 0.477 |
| PA during the preconception period is important for a healthy baby. | 1.29 (0.92–1.80) | 0.145 | 1.06 (0.73–1.52) | 0.774 |
| I believe in the benefits of PA during the preconception period for my own general health. | 1.29 (0.89–1.89) | 0.181 | 1.09 (0.72–1.67) | 0.659 |
| I believe in the benefits of PA during the preconception period for any potential babies I have in future. | 1.37 (0.97–1.95) | 0.077 | 1.18 (0.81–1.72) | 0.392 |
| I cannot understand the PA information available on the Internet/social media related to the preconception period. | 1.07 (0.76–1.52) | 0.695 | 0.92 (0.63–1.35) | 0.663 |
| I have enough time to be physically active even though I have other commitments. | 2.43 (1.75–3.41) | <0.01 | 2.1 (1.47–2.99) | <0.01 |
| I do not have my partner’s support for regular PA. | 0.69 (0.45–1.04) | 0.076 | 0.62 (0.39–0.99) | 0.044 |
| I do not have my family’s support for regular PA. | 0.67 (0.45–1.04) | 0.078 | 0.65 (0.414–1.03) | 0.067 |
| I do not have my friends’ support for regular PA. | 0.65 (0.42–1.02) | 0.064 | 0.55 (0.33–0.90) | 0.017 |
| I find doing regular exercise expensive. | 0.81 (0.57–1.15) | 0.237 | 0.79 (0.53–1.17) | 0.236 |
| I want to be physically active to become a healthy person. | 1.81 (1.17–2.78) | 0.007 | 1.63 (1.01–2.62) | 0.045 |
| I want to be physically active to lose weight. | 1.04 (0.76–1.50) | 0.774 | 1.04 (0.73–1.47) | 0.848 |
| I want to be physically active to attract/maintain a partner. | 1.11 (0.83–1.48) | 0.503 | 1 (0.72–1.38) | 0.99 |
| I am physically active to improve body image. | 1.84 (1.33–2.56) | <0.01 | 1.59 (1.12–2.27) | 0.01 |
| I am doing PA and will continue doing regular PA. | 4.09 (2.78–6.01) | <0.01 | 3.73(2.45–5.68) | <0.01 |
| I want to be a role model for my children/future children by exercising daily. | 2.06 (1.43–3.01) | <0.01 | 1.70 (1.12–2.56) | 0.012 |
| Demographic Characteristic (N = 13) | Value n (%) |
|---|---|
| Age in years | |
| 25–29 | 2 (15.4) |
| 30–34 | 3 (23.1) |
| 35–39 | 2 (15.4) |
| 40–45 | 6 (46.2) |
| Ever been pregnant | |
| Yes | 10 (76.9) |
| No | 3 (23.1) |
| Planned their previous pregnancy | |
| Yes | 9 (69.2) |
| No | 1 (7.7) |
| Pregnancy plans for future | |
| No plans/Not sure | 8 (61.5) |
| Currently trying to conceive | 2 (15.4) |
| Considering in future | 3 (23.1) |
| COM-B Component | Themed groups of Enablers/Barriers | Categories of Enablers/Barriers | Joint Display of Quantitative and Qualitative Findings * | Integrated Summation of Findings |
|---|---|---|---|---|
| Capability | Knowledge | Awareness of the importance of preconception PA PA information available on social media/internet Misconceptions | Approximately three-quarters of women expressed that physical activity during the preconception period is essential for general health (78.6%), a healthy pregnancy (77.7%) and a healthy baby (74.3%). Agreement with the statement that “Physical activity during the preconception period is important” was significantly associated with higher levels of PA (univariable analysis; Table 2). “…you know, pregnancy takes a huge toll on the body a huge toll on the body……. the healthier you are, you know, the better chance your body can, can tolerate the extra weight of the baby and, and then childbirth…” Over three-quarters (77.6%) of women in the quantitative study reported that they can understand the PA information available on the internet or social media related to the preconception period. “So I don’t quite know whether to trust that or not. However, it is hard to filter through what is kind of, you know, well informed and non-biased information.” “we when you say physical activity in [sic] the stereotypical things that come to mind of like intense exercise isn’t really something I do.” | Awareness of the importance of preconception PA and understanding PA information available on internet/social media acted as enabler to PA. Misconceptions that only vigorous activity counts as PA and feeling overwhelmed by the information available on social media/internet acted as barriers to PA. |
| Motivation | Beliefs about consequences Goals Emotions Belief about capabilities | Believing in the benefits of preconception PA Positive feelings associated with regular PA Having goals Physical exhaustion and fatigue Lack of confidence No priority given to oneself | Over three-quarters of participants expressed a strong belief in the benefits of preconception PA, with 81.1% agreeing it can have a positive impact on their own general health and 75.9% perceiving benefits for the health of potential future offspring. “Yeah, I mean, I believe, but on top of that for your future babies.” “What is fun, like, I love, I love movement.” 84.7% of participants expressed a desire to be physically active to attain general health, while 69.9% aimed to lose weight, and 67.5% sought to enhance their body image. “I would like to be super fit.” “So the idea now of working all day, and you’re completely exhausted. And then going actually physical exhaustion, like as I know that I need to.” “I think I’ve lost a lot of confidence to even just get out and do anything.” “There’s a kid sport something. So usually I’m running around between all of them. By the time I actually get time to sit, I want to rest, not run around or engage in exercise, so I don’t prioritise it as much as I should.” “I don’t go to the gym because I’ve got children. And you know, with my husband working, it’s really hard for me to find, find somewhere I can go.” “I don’t mean that in any sort of, I’m a supermom, or I’m a master or nothing like that. I just, yeah, I just want to try and help them succeed in the best way they can. So, where I can facilitate that I do, but it doesn’t leave a lot of time left for me.” | Belief in the benefits of preconception PA, positive feelings associated with regular PA and having goals acted as enabler to PA. Lack of confidence, no priority given to oneself, and physical exertion acted as barriers to PA. |
| Opportunity | Social Influences Environmental context and resources | Presence of social support Lack of social support Aspiring to be role model Time Restrictions Financial constraints Lack of accessibility | The majority of women agreed that that they received support from their partners (84.2%), families (84.7%), and friends (86.5%). “So, my husband built me a little gym here at the home, which is amazing. And I do that every morning.” “So I could like [sic] a supportive friend or partner or family member or something would be helpful.” 75.5% of women expressed their agreement with the statement that they aspire to be role models for their children or future children through daily exercise. 35% of women agreed with the statement that they lacked sufficient time for physical activity due to competing commitments. Women who reported they had enough time to participate in PA were more than twice as likely to be moderately to vigorously active (multivariable analyses, Table 2). Only 22% of women agreed that they find doing regular exercise expensive. “After having my second child, I did try to go to a gym, that had they advertised that they had childcare available at the gym. And I tried that. However, the tricky thing with that was that you had to book in time slots. And it was really pricey.” “You can imagine having a baby in a stroller, I know you’re walking down the road. And the place is just bumpy, bumpy.” | Presence of social support and aspiring to be role model acted as enabler to PA. Time restrictions, lack of social support, financial constraints and lack of accessibility acted as barriers to PA. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kandel, P.; Lim, S.; Dever, M.; Lamichhane, P.; Skouteris, H.; Currie, S.; Hill, B. Enablers and Barriers Related to Preconception Physical Activity: Insights from Women of Reproductive Age Using Mixed Methods. Nutrients 2023, 15, 4939. https://doi.org/10.3390/nu15234939
Kandel P, Lim S, Dever M, Lamichhane P, Skouteris H, Currie S, Hill B. Enablers and Barriers Related to Preconception Physical Activity: Insights from Women of Reproductive Age Using Mixed Methods. Nutrients. 2023; 15(23):4939. https://doi.org/10.3390/nu15234939
Chicago/Turabian StyleKandel, Pragya, Siew Lim, Michelle Dever, Prabhat Lamichhane, Helen Skouteris, Sinead Currie, and Briony Hill. 2023. "Enablers and Barriers Related to Preconception Physical Activity: Insights from Women of Reproductive Age Using Mixed Methods" Nutrients 15, no. 23: 4939. https://doi.org/10.3390/nu15234939
APA StyleKandel, P., Lim, S., Dever, M., Lamichhane, P., Skouteris, H., Currie, S., & Hill, B. (2023). Enablers and Barriers Related to Preconception Physical Activity: Insights from Women of Reproductive Age Using Mixed Methods. Nutrients, 15(23), 4939. https://doi.org/10.3390/nu15234939