


Iron Levels and Markers of Inflammation in a Population of Adults with Severe Obesity, a Cross-Sectional Study
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Population Study
2.3. Anthropometric Measurements
2.4. Bioelectrical Impedance Analysis
2.5. Assay Methods
2.6. Statistical Analysis
3. Results
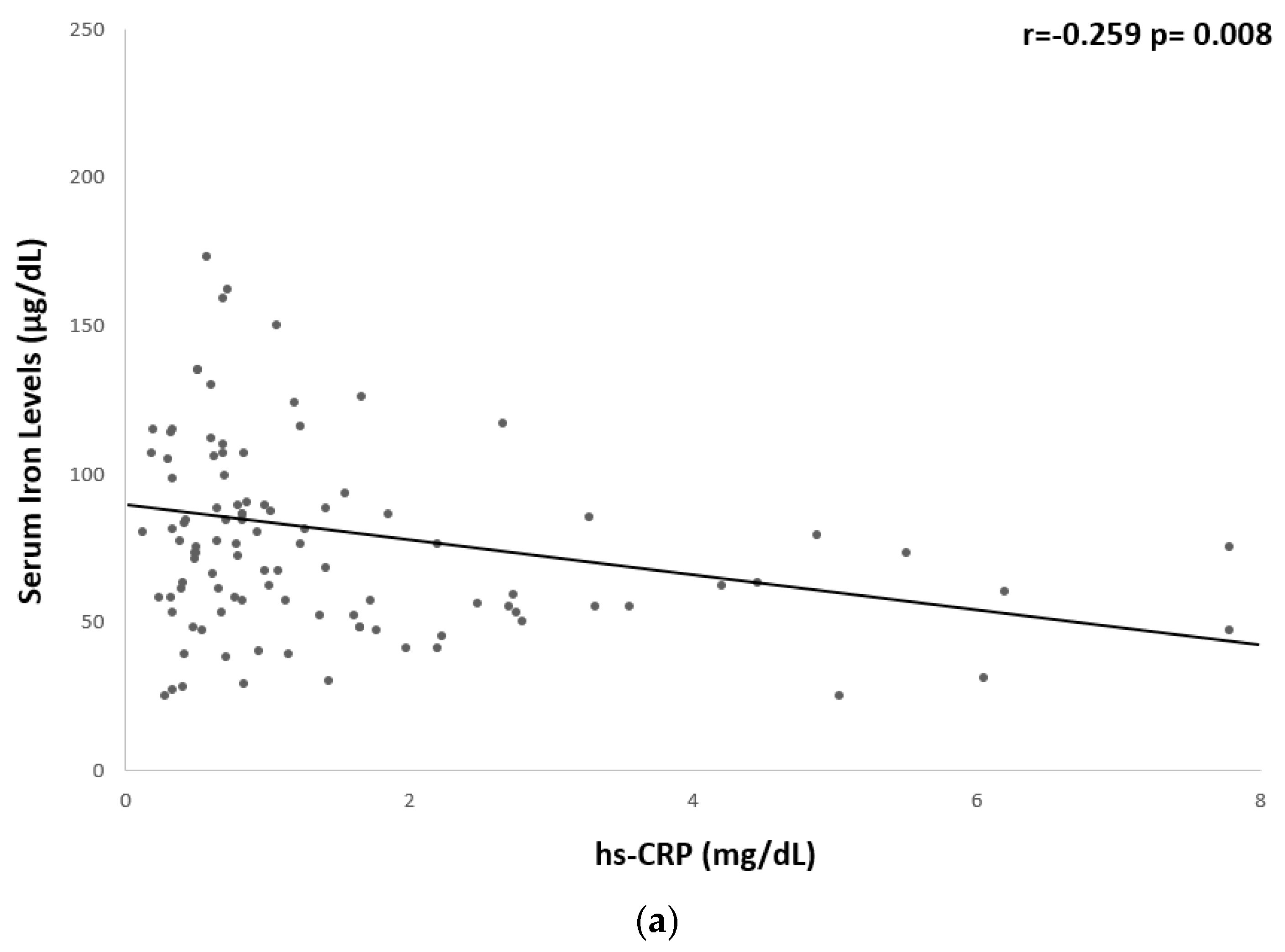
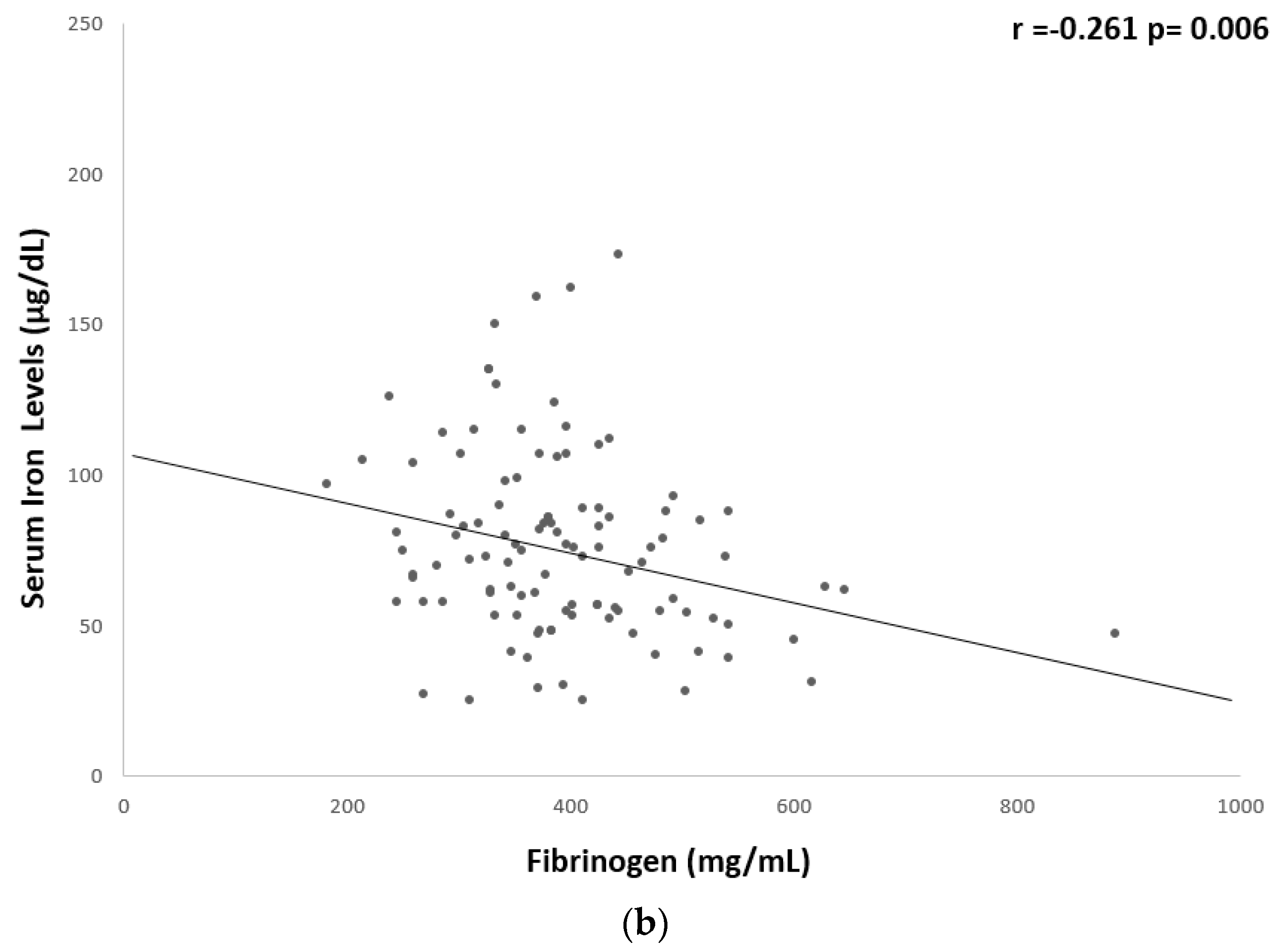
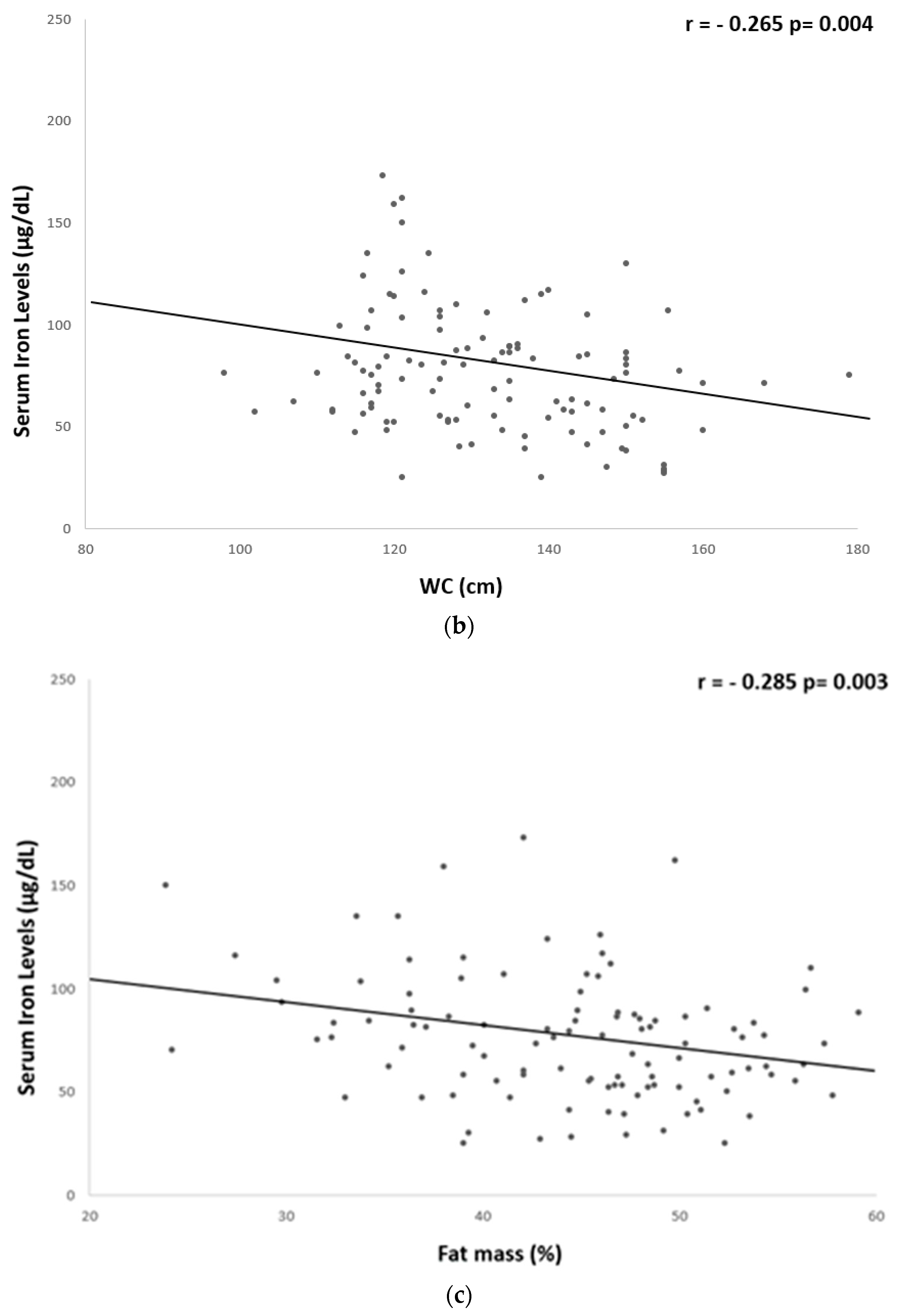
Correlation Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- WHO (World Health Organization). Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 4 April 2023).
- Cheng, H.L.; Bryant, C.; Cook, R.; O’Connor, H.; Rooney, K.; Steinbeck, K. The relationship between obesity and hypoferraemia in adults: A systematic review. Obes. Rev. 2012, 13, 150–161. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, X.; Shen, Y.; Fang, X.; Wang, Y.; Wang, F. Obesity and iron deficiency: A quantitative meta-analysis. Obes. Rev. 2015, 16, 1081–1093. [Google Scholar] [CrossRef]
- Kerkadi, A.; Mohsen Ali, R.; Shehada, A.A.H.; Abdelnasser AbouHassanein, E.; Moawad, J.; Bawadi, H.; Shi, Z. Association between central obesity indices and iron status indicators among Qatari adults. PLoS ONE 2021, 16, e0250759. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Khan, W.M.; Ayub, M.; Humayun, M.; Haroon, M. Ferritin Is a Marker of Inflammation rather than Iron Deficiency in Overweight and Obese People. J. Obes. 2016, 2016, 1937320. [Google Scholar] [CrossRef]
- Flancbaum, L.; Belsley, S.; Drake, V.; Colarusso, T.; Tayler, E. Preoperative nutritional status of patients undergoing Roux-en-Y gastric bypass for morbid obesity. J. Gastrointest. Surg. 2006, 10, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Alshwaiyat, N.M.; Ahmad, A.; Wan Hassan, W.M.R.; Al-Jamal, H.A.N. Association between obesity and iron deficiency (Review). Exp. Ther. Med. 2021, 22, 1268. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Rosato, E.; Gigante, A.; Gasperini, M.L.; Proietti, L.; Muscaritoli, M. Assessing Malnutrition in Systemic Sclerosis With Global Leadership Initiative on Malnutrition and European Society of Clinical Nutrition and Metabolism Criteria. JPEN J. Parenter Enteral Nutr. 2021, 45, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Laudisio, D.; Di Somma, C.; Pugliese, G.; Salzano, C.; Colao, A.; Savastano, S. Somatotropic Axis and Obesity: Is There Any Role for the Mediterranean Diet? Nutrients 2019, 11, 2228. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Muscogiuri, G.; Laudisio, D.; Pugliese, G.; de Alteriis, G.; Colao, A.; Savastano, S. Influence of the Mediterranean Diet on 25- Hydroxyvitamin D Levels in Adults. Nutrients 2020, 12, 1439. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. NCHS Data Brief 2020, 360, 1–8. [Google Scholar]
- Pellegrini, M.; Rahimi, F.; Boschetti, S.; Devecchi, A.; De Francesco, A.; Mancino, M.V.; Toppino, M.; Morino, M.; Fanni, G.; Ponzo, V.; et al. Pre-operative micronutrient deficiencies in patients with severe obesity candidates for bariatric surgery. J. Endocrinol. Investig. 2021, 44, 1413–1423. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Bixler, E.O.; Papanicolaou, D.A.; Chrousos, G.P. Chronic systemic inflammation in overweight and obese adults. JAMA 2000, 283, 2235; author reply 2236. [Google Scholar] [CrossRef]
- Fontana, L.; Eagon, J.C.; Trujillo, M.E.; Scherer, P.E.; Klein, S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes 2007, 56, 1010–1013. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, E.; Rivera, S.; Gabayan, V.; Keller, C.; Taudorf, S.; Pedersen, B.K.; Ganz, T. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J. Clin. Investig. 2004, 113, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, N.U.; El-Mallah, C.; Herter-Aeberli, I.; Bissani, N.; Wehbe, N.; Obeid, O.; Zimmermann, M.B. The effect of central obesity on inflammation, hepcidin, and iron metabolism in young women. Int. J. Obes. 2020, 44, 1291–1300. [Google Scholar] [CrossRef]
- Hilton, C.; Sabaratnam, R.; Drakesmith, H.; Karpe, F. Iron, glucose and fat metabolism and obesity: An intertwined relationship. Int. J. Obes. 2023, 47, 554–563. [Google Scholar] [CrossRef]
- Iwasaki, T.; Nakajima, A.; Yoneda, M.; Yamada, Y.; Mukasa, K.; Fujita, K.; Fujisawa, N.; Wada, K.; Terauchi, Y. Serum ferritin is associated with visceral fat area and subcutaneous fat area. Diabetes Care 2005, 28, 2486–2491. [Google Scholar] [CrossRef] [PubMed]
- Camaschella, C. Iron deficiency. Blood 2019, 133, 30–39. [Google Scholar] [CrossRef]
- Urbanski, G.; Chabrun, F.; Lavigne, C.; Lacout, C.; Delattre, E.; Reynier, P.; Requin, J. Serum ferritin/C-reactive protein ratio is a simple and effective biomarker for diagnosing iron deficiency in the context of systemic inflammation. QJM 2023, hcad218. [Google Scholar] [CrossRef]
- Wang, W.; Knovich, M.A.; Coffman, L.G.; Torti, F.M.; Torti, S.V. Serum ferritin: Past, present and future. Biochim. Biophys. Acta 2010, 1800, 760–769. [Google Scholar] [CrossRef]
- Dao, M.C.; Meydani, S.N. Iron biology, immunology, aging, and obesity: Four fields connected by the small peptide hormone hepcidin. Adv. Nutr. 2013, 4, 602–617. [Google Scholar] [CrossRef]
- Andrews, M.; Soto, N.; Arredondo-Olguin, M. Association between ferritin and hepcidin levels and inflammatory status in patients with type 2 diabetes mellitus and obesity. Nutrition 2015, 31, 51–57. [Google Scholar] [CrossRef]
- Chambers, E.C.; Heshka, S.; Gallagher, D.; Wang, J.; Pi-Sunyer, F.X.; Pierson, R.N., Jr. Serum iron and body fat distribution in a multiethnic cohort of adults living in New York City. J. Am. Diet. Assoc. 2006, 106, 680–684. [Google Scholar] [CrossRef] [PubMed]
- Senkus, K.E.; Crowe-White, K.M.; Locher, J.L.; Ard, J.D. Relative fat mass assessment estimates changes in adiposity among female older adults with obesity after a 12-month exercise and diet intervention. Ann. Med. 2022, 54, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Muscogiuri, G.; Pugliese, G.; Laudisio, D.; de Alteriis, G.; Graziadio, C.; Colao, A.; Savastano, S. Phase Angle as an Easy Diagnostic Tool of Meta-Inflammation for the Nutritionist. Nutrients 2021, 13, 1446. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Feng, Y.; Long, Q.; Chen, F.; Chen, Y.; Ma, M.; Mao, S. A comparative analysis of body composition assessment by BIA and DXA in children with type II and III spinal muscular atrophy. Front. Neurol. 2022, 13, 1034894. [Google Scholar] [CrossRef] [PubMed]
- Moschonis, G.; Chrousos, G.P.; Lionis, C.; Mougios, V.; Manios, Y.; Healthy Growth Study, g. Association of total body and visceral fat mass with iron deficiency in preadolescents: The Healthy Growth Study. Br. J. Nutr. 2012, 108, 710–719. [Google Scholar] [CrossRef]
- Kochkodan, J.; Telem, D.A.; Ghaferi, A.A. Physiologic and psychological gender differences in bariatric surgery. Surg. Endosc. 2018, 32, 1382–1388. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Mean ± SD or Number (%) n = 114 |
|---|---|
| Males n. (%) | 30 (26.3%) |
| Females n. (%) | 84 (73.7%) |
| Age (years) | 40.96 ± 12.54 |
| BMI (Kg/m2) | 44.94 ± 7.29 |
| Grade II obesity n. (%) | 34 (29.8%) |
| Grade III obesity n. (%) | 80 (70.2%) |
| WC (cm) | 132.20 ± 14.98 |
| HP (cm) | 138.36 ± 13.63 |
| WHR | 0.96 ± 0.09 |
| Fat mass (%) | 44.49 ± 7.60 |
| Fat mass (kg) | 53.38 ± 14.01 |
| Free fat mass (%) | 55.51 ± 7.60 |
| Free fat mass (kg) | 65.77 ± 12.55 |
| Parameters | Mean ± SD n = 114 |
|---|---|
| Glucose (mg/dL) | 97.18 ± 23.77 |
| Insulin (mIU/mL) | 21.44 ± 11.86 |
| HOMA-index | 4.56 ± 3.04 |
| HbA1c (%) | 5.31 ± 1.53 |
| Total cholesterol (mg/dL) | 191.32 ± 37.20 |
| LDL cholesterol (mg/dL) | 133.17 ± 36.72 |
| TG (mg/dL) | 132.25 ± 67.66 |
| Albumin (g/dL) | 4.35 ± 0.30 |
| Iron (μg/dL) | 76.30 ± 30.37 |
| Haemoglobin (g/dL) | 13.65 ± 2.31 |
| Vitamin B12 (pg/mL) | 343.72 ± 118.52 |
| Folic acid (ng/mL) | 4.45 ± 2.83 |
| 25(OH)D (ng/mL) hs-CRP (mg/dL) Fibrinogen (mg/mL) | 17.16 ± 9.81 1.47 ± 1.58 393.28 ± 102.19 |
| Parameters | Values | |
|---|---|---|
| 25(OH)D deficiency a | n. (%) | 67 (58.8%) |
| Folate deficiency b | n. (%) | 25 (21.9%) |
| Vitamin B12 deficiency c | n. (%) | 11 (9.6%) |
| Anaemia d | n. (%) | 10 (8.8%) |
| Low serum iron e | n. (%) | 23 (20.2%) |
| Parameters | Grade-II Obesity | Grade-III Obesity | p-Value |
|---|---|---|---|
| Serum iron levels (μg/dL) | 86.38 ± 37.71 | 72.01 ± 25.74 | 0.02 |
| Haemoglobin (g/dL) | 13.41 ± 3.67 | 13.75 ± 1.38 | 0.159 |
| hs-CRP (mg/dL) | 0.76 ± 0.53266 | 1.73 ± 1.75 | 0.005 |
| Fibrinogen (mg/mL) | 338.44 ± 72.27 | 416.37 ± 104.48 | <0.0001 |
| Glucose (mg/dL) | 92.18 ± 19.32 | 99.31 ± 25.24 | 0.143 |
| HbA1c (%) | 5.52 ± 0.98 | 5.22 ± 1.69 | 0.398 |
| Insulin (mIU/mL) | 17.07 ± 8.03 | 23.28 ± 12.75 | 0.015 |
| HOMA-index | 3.89 ± 2.14 | 5.49 ± 2.93 | 0.008 |
| Total cholesterol (mg/dL) | 191.09 ± 33.65 | 191.41 ± 146.7 | 0.955 |
| LDL cholesterol (mg/dL) | 130.34 ± 30.05 | 134.16 ± 38.7 | 0.861 |
| Triglycerides (mg/dL) | 132.68 ± 70.97 | 132.06 ± 66.64 | 0.965 |
| Vitamin B12 (pg/mL) | 358.22 ± 130.33 | 335.56 ± 111.94 | 0.502 |
| Folic acid (ng/mL) | 5.20 ± 3.6 | 4.01 ± 2.21 | 0.082 |
| 25(OH)D (ng/mL) | 19.06 ± 9.75 | 16.27 ± 9.78 | 0.193 |
| Parameters | Serum Iron (μg/dL) | |
|---|---|---|
| r | p-Value | |
| hs-CRP(mg/dL) | −0.259 | 0.008 |
| Fibrinogen (mg/mL) | −0.261 | 0.006 |
| BMI (kg/m2) | −0.186 | 0.04 |
| WC (cm) | −0.265 | 0.004 |
| Fat mass (%) | −0.285 | 0.003 |
| Parameters | hs-CRP (mg/dL) | |
|---|---|---|
| r | p-Value | |
| BMI (Kg/m2) | 0.362 | 0.001 |
| WC (cm) | 0.283 | 0.004 |
| Parameters | Multiple Regression Analysis | |||
|---|---|---|---|---|
| Model 1 | R2 | β | t | p Value |
| WC (cm) | −0.772 | −0.357 | −0.328 | 0.001 |
| Fat mass (%) | −1.090 | −0.251 | −2.272 | 0.02 |
| hs-CRP (mg/dL) | −4.974 | −0.237 | −2.018 | 0.04 |
| Variables excluded: Fibrinogen and BMI | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laudisio, D.; de Alteriis, G.; Vetrani, C.; Aprano, S.; Pugliese, G.; Zumbolo, F.; Colao, A.; Savastano, S. Iron Levels and Markers of Inflammation in a Population of Adults with Severe Obesity, a Cross-Sectional Study. Nutrients 2023, 15, 4702. https://doi.org/10.3390/nu15214702
Laudisio D, de Alteriis G, Vetrani C, Aprano S, Pugliese G, Zumbolo F, Colao A, Savastano S. Iron Levels and Markers of Inflammation in a Population of Adults with Severe Obesity, a Cross-Sectional Study. Nutrients. 2023; 15(21):4702. https://doi.org/10.3390/nu15214702
Chicago/Turabian StyleLaudisio, Daniela, Giulia de Alteriis, Claudia Vetrani, Sara Aprano, Gabriella Pugliese, Francesca Zumbolo, Annamaria Colao, and Silvia Savastano. 2023. "Iron Levels and Markers of Inflammation in a Population of Adults with Severe Obesity, a Cross-Sectional Study" Nutrients 15, no. 21: 4702. https://doi.org/10.3390/nu15214702
APA StyleLaudisio, D., de Alteriis, G., Vetrani, C., Aprano, S., Pugliese, G., Zumbolo, F., Colao, A., & Savastano, S. (2023). Iron Levels and Markers of Inflammation in a Population of Adults with Severe Obesity, a Cross-Sectional Study. Nutrients, 15(21), 4702. https://doi.org/10.3390/nu15214702