
Geriatric Nutritional Risk Index as a Prognostic Factor for Renal Progression in Patients with Type 2 Diabetes Mellitus

 ,
,
Abstract
:1. Introduction
2. Material and Methods
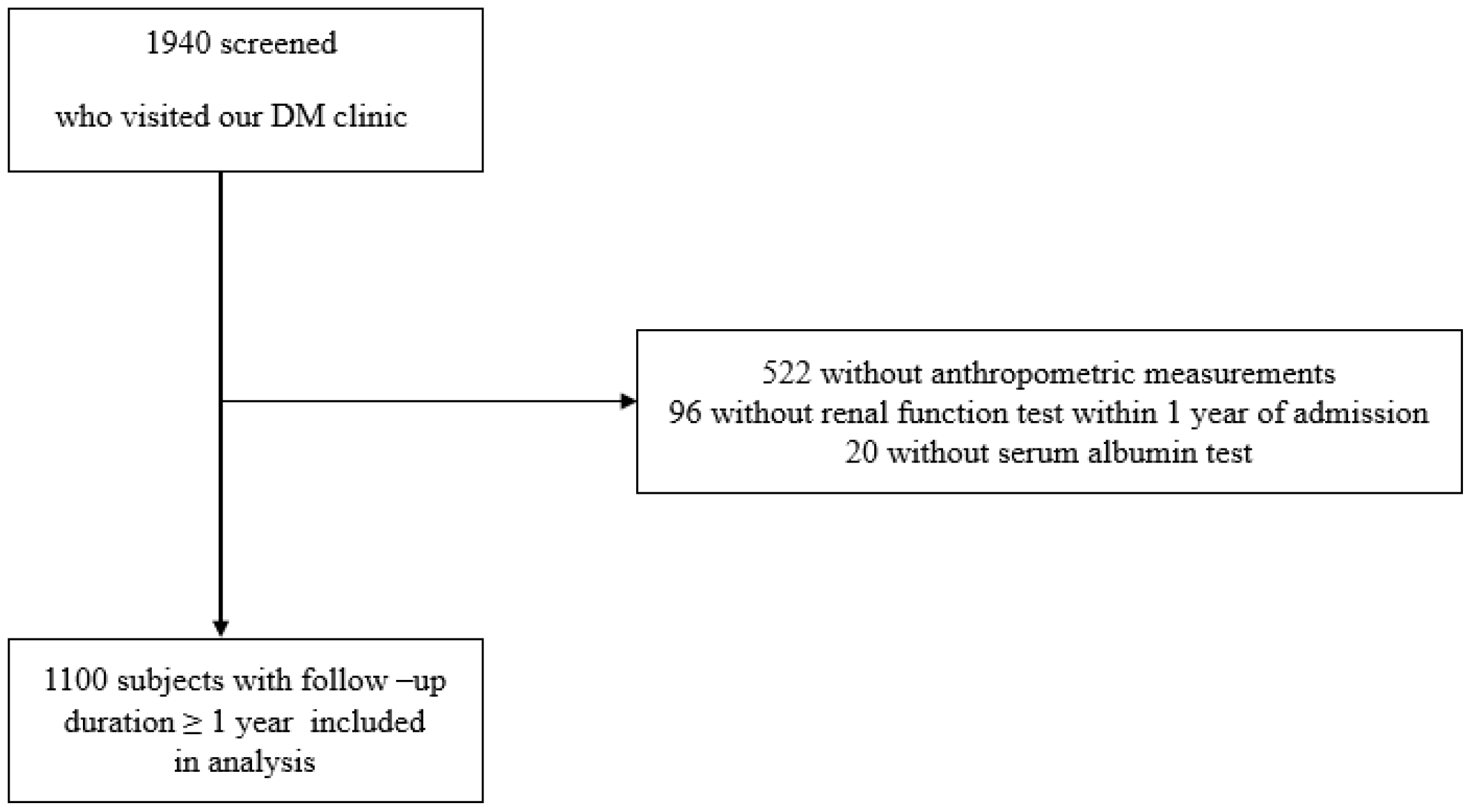
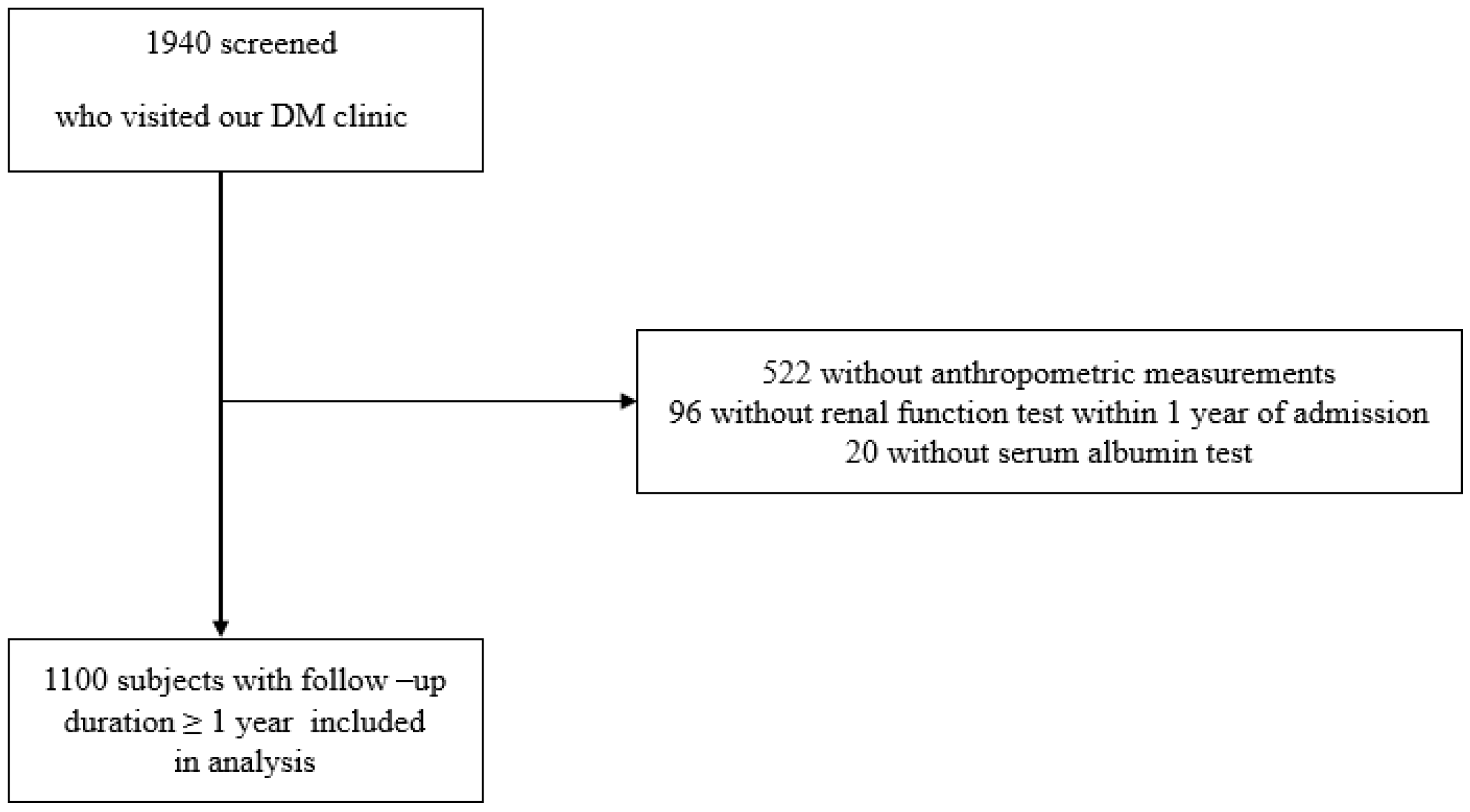
2.1. Study Design and Patients
2.2. GNRI Calculation
2.3. Definition of CKD Progression and Albuminuria Progression
2.4. Laboratory Data Measurement
2.5. Statistical Analysis
3. Results
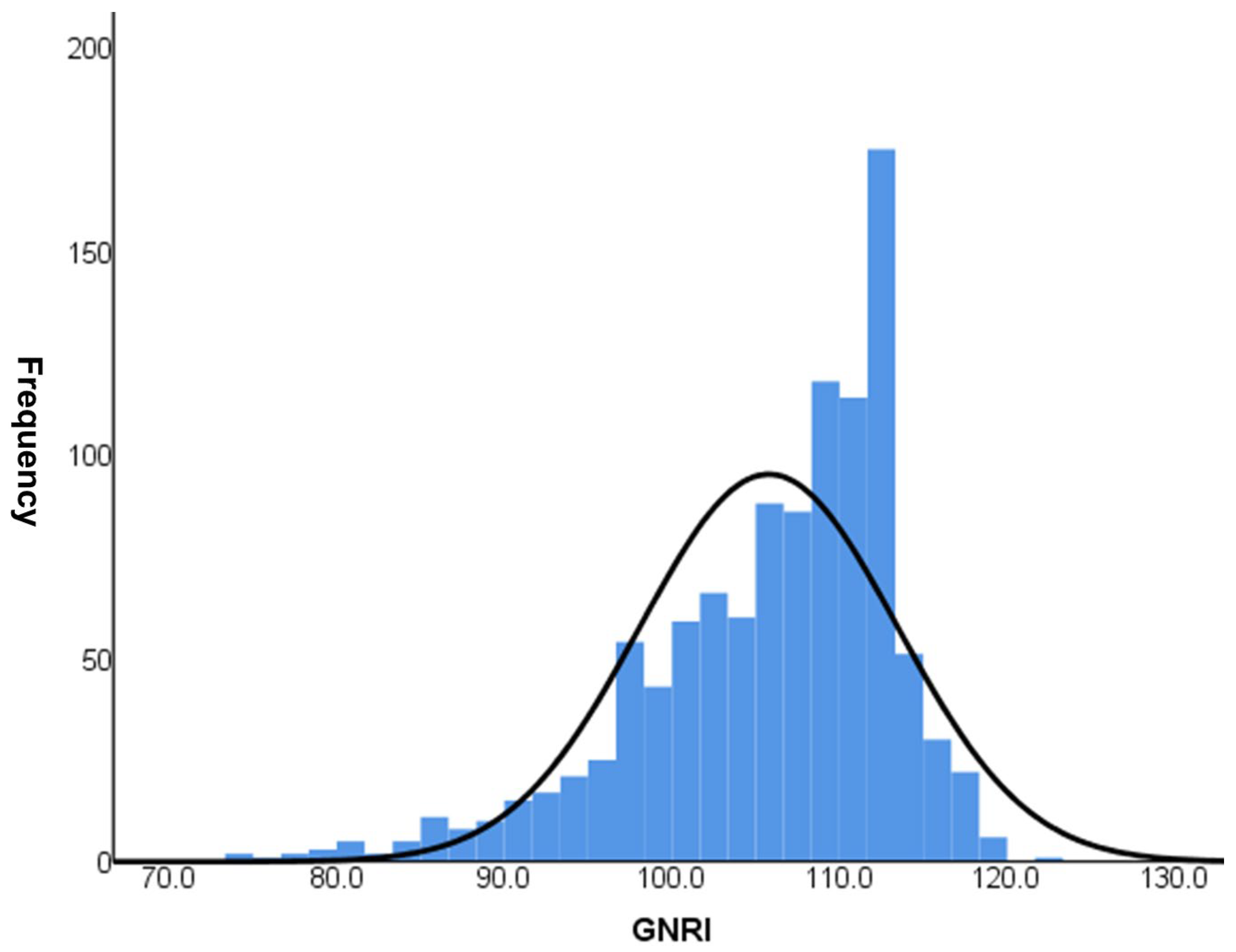
3.1. Baseline Characteristics of the Patients According to GNRI Quartiles
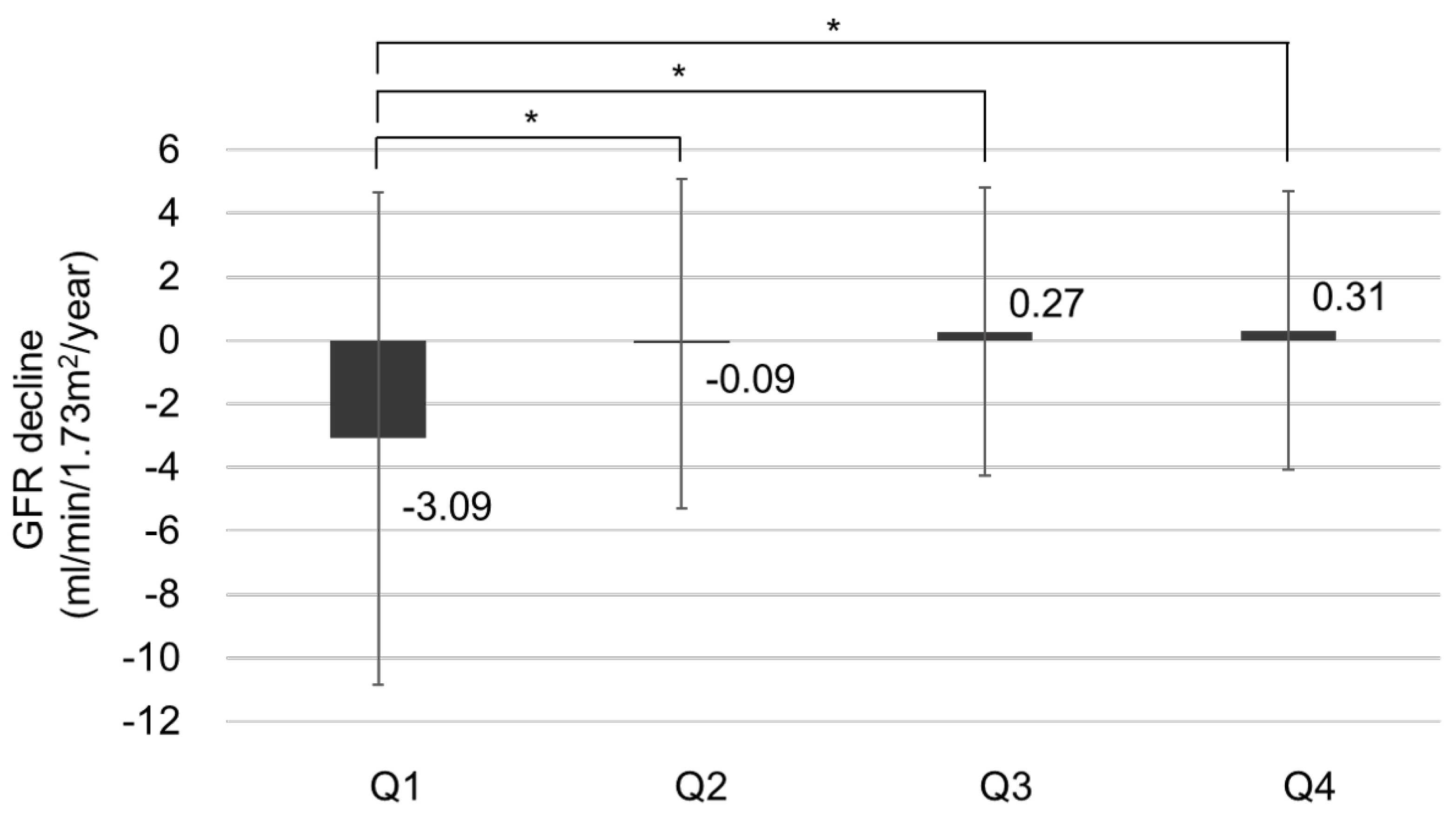
3.2. Effect of GNRI on the Rate of Renal Function Decline
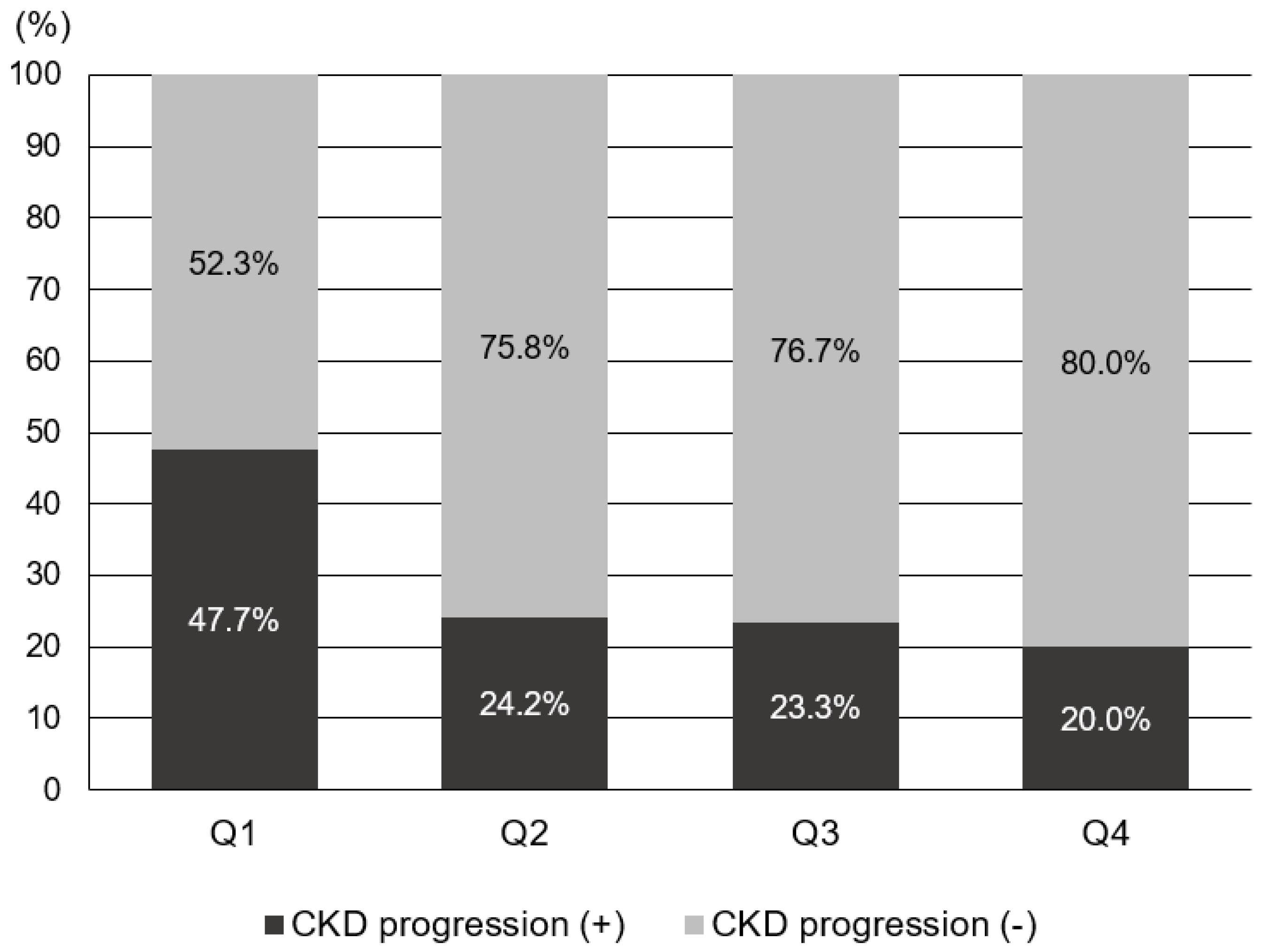
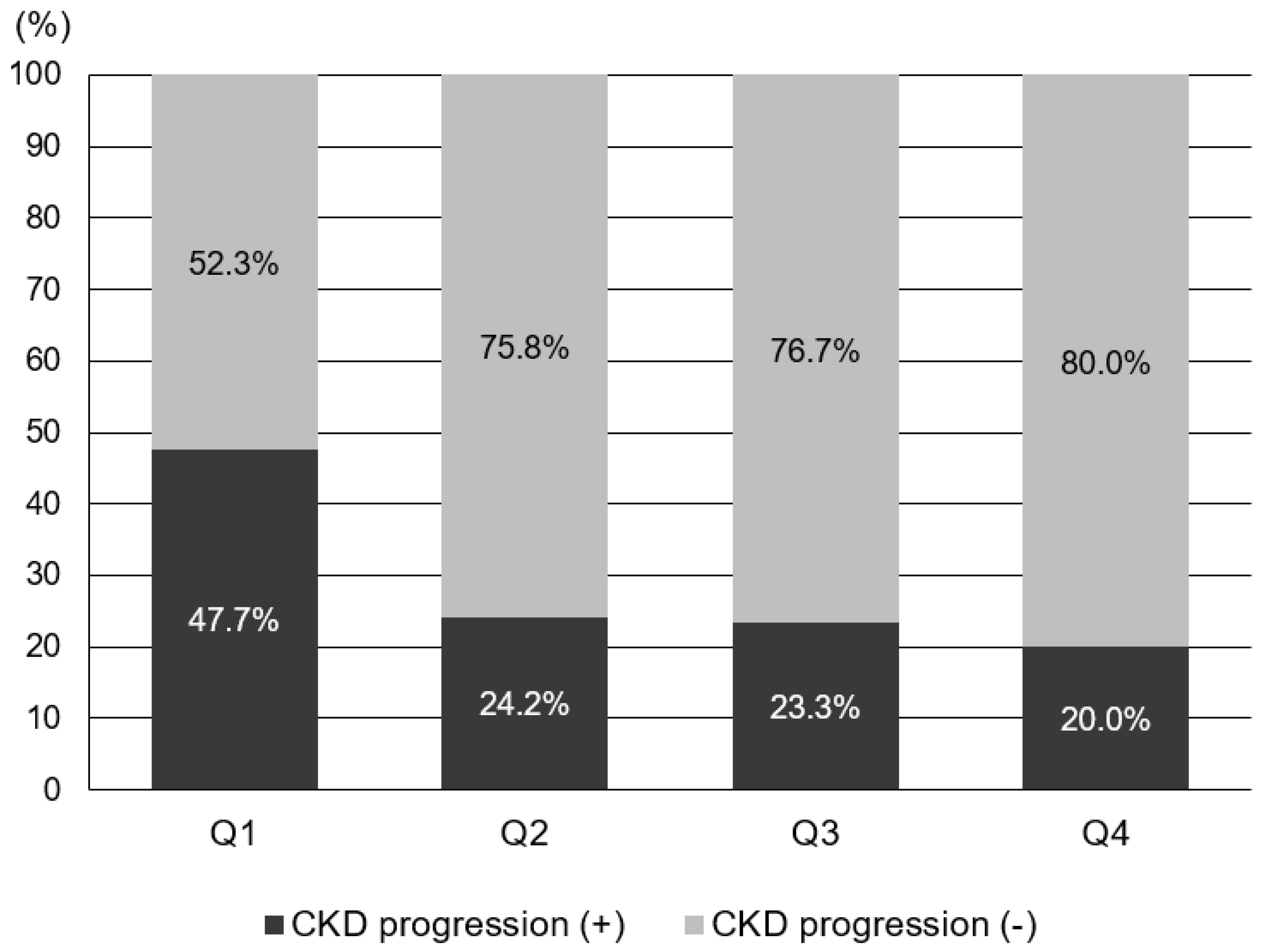
3.3. GNRI as a Risk Factor for CKD Progression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zha, Y.; Qian, Q. Protein Nutrition and Malnutrition in CKD and ESRD. Nutrients 2017, 9, 208. [Google Scholar] [CrossRef] [PubMed]
- Okamura, M.; Inoue, T.; Ogawa, M.; Shirado, K.; Shirai, N.; Yagi, T.; Momosaki, R.; Kokura, Y. Rehabilitation Nutrition in Patients with Chronic Kidney Disease and Cachexia. Nutrients 2022, 14, 4722. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, K.; Nakagawa, N.; Saito, E.; Matsuki, M.; Takehara, N.; Akasaka, K.; Sato, N.; Hasebe, N. Malnutrition, renal dysfunction and left ventricular hypertrophy synergistically increase the long-term incidence of cardiovascular events. Hypertens Res. 2016, 39, 633–639. [Google Scholar] [CrossRef]
- Schrauben, S.J.; Apple, B.J.; Chang, A.R. Modifiable Lifestyle Behaviors and CKD Progression: A Narrative Review. Kidney360 2022, 3, 752–778. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A. A patient with CKD and poor nutritional status. Clin. J. Am. Soc. Nephrol. 2013, 8, 2174–2182. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. K/DOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef] [PubMed]
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 8, 1065. [Google Scholar] [CrossRef]
- Lee, M.J.; Kwon, Y.E.; Park, K.S.; Park, J.T.; Han, S.H.; Kang, S.W.; Kim, H.J.; Yoo, T.H. Changes in geriatric nutritional risk index and risk of major adverse cardiac and cerebrovascular events in incident peritoneal dialysis patients. Kidney Res. Clin. Pract. 2017, 36, 377–386. [Google Scholar] [CrossRef]
- Xiong, J.; Wang, M.; Zhang, Y.; Nie, L.; He, T.; Wang, Y.; Huang, Y.; Feng, B.; Zhang, J.; Zhao, J. Association of Geriatric Nutritional Risk Index with Mortality in Hemodialysis Patients: A Meta-Analysis of Cohort Studies. Kidney Blood Press. Res. 2018, 43, 1878–1889. [Google Scholar] [CrossRef]
- Kuo, I.C.; Huang, J.C.; Wu, P.Y.; Chen, S.C.; Chang, J.M.; Chen, H.C. A Low Geriatric Nutrition Risk Index Is Associated with Progression to Dialysis in Patients with Chronic Kidney Disease. Nutrients 2017, 9, 1228. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P.; Kopple, J.D.; Kalantar-Zadeh, K. Management of protein-energy wasting in non-dialysis-dependent chronic kidney disease: Reconciling low protein intake with nutritional therapy. Am. J. Clin. Nutr. 2013, 97, 1163–1177. [Google Scholar] [CrossRef] [PubMed]
- Cano, N.J.; Roth, H.; Aparicio, M.; Aza, F.; Canaud, B.; Chauveau, P.; Combe, C.; Fouque, D.; Laville, M.; Leverve, X.M. Malnutrition in hemodialysis diabetic patients: Evaluation and prognostic influence. Kidney Int. 2002, 62, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. Chapter 2: Definition, identification, and prediction of CKD progression. Kidney Int. Suppl. 2013, 3, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Park, H.C.; Lee, Y.K.; Cho, A.; Han, C.H.; Noh, J.W.; Shin, Y.J.; Bae, S.H.; Kim, H. Diabetic retinopathy is a prognostic factor for progression of chronic kidney disease in the patients with type 2 diabetes mellitus. PLoS ONE 2019, 14, e0220506. [Google Scholar] [CrossRef]
- Iorember, F.M. Malnutrition in Chronic Kidney Disease. Front. Pediatr. 2018, 6, 161. [Google Scholar] [CrossRef]
- Becker, P.J.; Nieman, C.L.; Corkins, M.R.; Monczka, J.; Smith, E.; Smith, S.E.; Spear, B.A.; White, J.V. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: Indicators recommended for the identification and documentation of pediatric malnutrition (undernutrition). J. Acad. Nutr. Diet. 2014, 114, 1988–2000. [Google Scholar] [CrossRef]
- Grover, Z.; Ee, L.C. Protein energy malnutrition. Pediatr. Clin. North Am. 2009, 56, 1055–1068. [Google Scholar] [CrossRef]
- Friedman, A.N.; Fadem, S.Z. Reassessment of albumin as a nutritional marker in kidney disease. J. Am. Soc. Nephrol. 2010, 21, 223–230. [Google Scholar] [CrossRef]
- Dai, L.; Mukai, H.; Lindholm, B.; Heimbürger, O.; Barany, P.; Stenvinkel, P.; Qureshi, A.R. Clinical global assessment of nutritional status as predictor of mortality in chronic kidney disease patients. PLoS ONE 2017, 12, e0186659. [Google Scholar] [CrossRef] [PubMed]
- Kiuchi, A.; Ohashi, Y.; Tai, R.; Aoki, T.; Mizuiri, S.; Ogura, T.; Aikawa, A.; Sakai, K. Association between Low Dietary Protein Intake and Geriatric Nutrition Risk Index in Patients with Chronic Kidney Disease: A Retrospective Single-Center Cohort Study. Nutrients 2016, 8, 662. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.J.; Zheng, C.M.; Wu, M.Y.; Chen, T.T.; Wu, Y.C.; Wu, Y.L.; Lin, H.T.; Zheng, J.Q.; Chu, N.F.; Lin, Y.M.; et al. Relationship between body mass index and renal function deterioration among the Taiwanese chronic kidney disease population. Sci. Rep. 2018, 8, 6908. [Google Scholar] [CrossRef] [PubMed]
- Khedr, A.; Khedr, E.; House, A.A. Body mass index and the risk of progression of chronic kidney disease. J. Ren. Nutr. 2011, 21, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Li, W.C.; Chen, J.Y.; Lee, Y.Y.; Weng, Y.M.; Hsiao, C.T.; Loke, S.S. Association between waist-to-height ratio and chronic kidney disease in the Taiwanese population. Intern. Med. J. 2014, 44, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Iseki, K.; Ikemiya, Y.; Kinjo, K.; Inoue, T.; Iseki, C.; Takishita, S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int. 2004, 65, 1870–1876. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.W.; Tsai, C.H.; Chou, S.E.; Su, W.T.; Li, C.; Hsu, S.Y.; Hsieh, C.H. Geriatric nutritional risk index in screening malnutrition among young adult and elderly trauma patients. Formos. J. Surg. 2021, 54, 183–190. [Google Scholar] [CrossRef]
- Nakagawa, N.; Maruyama, K.; Hasebe, N. Utility of Geriatric Nutritional Risk Index in Patients with Chronic Kidney Disease: A Mini-Review. Nutrients 2021, 13, 3688. [Google Scholar] [CrossRef]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef]
- Xiong, J.; Wang, M.; Wang, J.; Yang, K.; Shi, Y.; Zhang, J.; Zhang, B.; Zhang, L.; Zhao, J. Geriatric nutrition risk index is associated with renal progression, cardiovascular events and all-cause mortality in chronic kidney disease. J. Nephrol. 2020, 33, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, M.K. Diabetic nephropathy: Recent advances in pathophysiology and challenges in dietary management. Diabetol. Metab. Syndr. 2019, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Retnakaran, R.; Cull, C.A.; Thorne, K.I.; Adler, A.I.; Holman, R.R.; UKPDS Study Group. Risk factors for renal dysfunction in type 2 diabetes: U.K. Prospective Diabetes Study 74. Diabetes 2006, 55, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Raile, K.; Galler, A.; Hofer, S.; Herbst, A.; Dunstheimer, D.; Busch, P.; Holl, R.W. Diabetic nephropathy in 27,805 children, adolescents, and adults with type 1 diabetes: Effect of diabetes duration, A1C, hypertension, dyslipidemia, diabetes onset, and sex. Diabetes Care 2007, 30, 2523–2528. [Google Scholar] [CrossRef]
- Ritz, E. Diabetic nephropathy. Saudi J. Kidney Dis. Transpl. 2006, 17, 481–490. [Google Scholar] [PubMed]
- Meloni, C.; Tatangelo, P.; Cipriani, S.; Rossi, V.; Suraci, C.; Tozzo, C.; Rossini, B.; Cecilia, A.; Franco, D.D.; Straccialano, E.; et al. Adequate protein dietary restriction in diabetic and nondiabetic patients with chronic renal failure. J. Ren. Nutr. 2004, 14, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Otoda, T.; Kanasaki, K.; Koya, D. Low-protein diet for diabetic nephropathy. Curr. Diab. Rep. 2014, 14, 523. [Google Scholar] [CrossRef]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Abebayo, O.M.; Afarideh, M.; Kumar Agarwal, S.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Carrero, J.J.; Stenvinkel, P.; Cuppari, L.; Ikizer, T.A.; Kalantar-Zadeh, K.; Kaysen, G.; Mitch, W.E.; Price, S.R.; Wanner, C.; Wang, A.Y.M.; et al. Etiology of the protein energy wasting syndrome in chronic kidney disease: A consensus statement from the International Society of Renal Nutrition and Metabolism (ISRNM). J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2013, 23, 77–90. [Google Scholar] [CrossRef]
- Cano, N.; Fiaccadori, E.; Tesinsky, P.; Toigo, G.; Druml, W.; Kuhlmann, M.; Mann, H.; Horl, W.H. ESPEN Guidelines on Enteral Nutrition: Adult renal failure. Clin. Nutr. 2006, 25, 295–331. [Google Scholar] [CrossRef]
- Dombros, N.; Dratwa, M.; Feriani, M.; Gokal, R.; Heimbürger, O.; Krediet, R.; Plum, J.; Rodrigues, A.; Selgas, R.; Struijk, D.; et al. European best practice guidelines for peritoneal dialysis. Nutrition in peritoneal dialysis. Nephrol. Dial. Transplant. 2005, 20, ix28–ix33. [Google Scholar]
- Chan, W. Chronic Kindey Disease and Nutritional Support. Nutr. Clin. Pract. 2021, 36, 312–330. [Google Scholar] [CrossRef]
- Campbell, K.L.; Ash, S.; Davies, P.S.; Bauer, J.D. Randomized controlled trial of nutritional counseling on body composition and dietary intake in severe CKD. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2008, 51, 748–758. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 1100) | Q1 (n = 281) | Q2 (n = 298) | Q3 (n = 236) | Q4 (n = 285) | p-Value |
|---|---|---|---|---|---|---|
| Age (years) | 57.3 ± 11.2 | 57.5 ± 12.6 | 59.0 ± 10.6 | 57.2 ± 10.1 | 55.6 ± 11.1 | 0.005 |
| Male (%) | 527 (47.9) | 132 (47.0) | 134 (45.0) | 107 (45.3) | 154 (54.0) | 0.11 |
| Hypertension (%) | 529 (49.7) | 131 (47.3) | 151 (52.1) | 117 (51.8) | 130 (47.8) | 0.557 |
| SBP (mmHg) | 130.0 (118.0–140.0) | 130.0 (112.0–140.0) | 130.0 (120.0–130.0) | 130.0 (117.0–140.0) | 123.5 (116.3–138.5) | 0.208 |
| DBP (mmHg) | 79.0 (70.0–85.0) | 80.0 (70.0–90.0) | 80.0 (70.0–87.0) | 78.0 (70.0–85.0) | 74.0 (68.0–80.0) | 0.096 |
| DM duration (years) | 10.0 (5.0–15.0) | 11.0 (5.0–17.0) | 10.0 (5.0–15.0) | 9.0 (4.0–15.0) | 9.0 (5.0–14.0) | 0.016 |
| HbA1c (%) | 7.3 (6.5–78.9) | 8.3 (6.78–10.2) | 7.1 (6.5–8.5) | 7.0 (6.4–8.2) | 7.2 (6.5–8.0) | <0.001 |
| FPG (mg/dL) | 134.0 (109.0–177.0) | 148.0 (108.5–209.0) | 131.0 (110.0–174.5) | 128.5 (108.0–166.3) | 131.0 (108.0–169.0) | <0.001 |
| ACEI or ARB (%) | 517 (47.0) | 137 (48.8) | 138 (46.3) | 106 (44.9) | 136 (47.7) | 0.831 |
| Hemoglobin (g/dL) | 7.3 (6.5–8.9) | 11.9 (10.6–13.4) | 13.2 (12.2–14.4) | 13.7 (12.7–14.7) | 13.8 (12.6–14.9) | <0.001 |
| Creatinine (mg/dL) | 0.91 (0.78–1.1) | 0.95 (0.78–1.15) | 0.89 (0.78–1.1) | 0.91 (0.77–1.08) | 0.91 (0.78–1.1) | 0.646 |
| eGFR (mL/min/1.73 m2) | 80.0 (66.0–95.3) | 77.5 (61.2–95.4) | 80.0 (65.9–96.0) | 80.4 (66.3–94.5) | 82.7 (68.7–96.0) | 0.114 |
| Calcium (mg/dL) | 8.9 (8.6–9.2) | 8.4 (8.0–8.7) | 8.9 (8.6–9.1) | 9.0 (8.8–9.4) | 9.2 (9.0–9.5) | <0.001 |
| Phosphorus (mg/dL) | 3.6 (3.2–4.0) | 3.6 (3.0–4.1) | 3.6 (3.2–4.0) | 3.6 (3.3–4.0) | 3.7 (3.3–4.0) | 0.062 |
| Total cholesterol (mg/dL) | 162.0 (140.0–189.0) | 153.0 (129.0–183.0) | 163.0 (141.0–186.0) | 165.0 (142.0–195.0) | 166.0 (146.0–191.0) | 0.011 |
| Albumin (g/dL) | 4.4 (4.1–4.7) | 3.8 (3.5–4.0) | 4.3 (4.2–4.4) | 4.6 (4.5–4.6) | 4.8 (4.7–4.9) | <0.001 |
| UACR (mg/g) | 15.2 (8.2–36.0) | 22.5 (9.3–114.4) | 16.3 (9.4–41.6) | 13.4 (7.0–25.2) | 13.8 (7.9–26.0) | <0.001 |
| BMI (kg/m2) | 24.7 (22.5–27.1) | 23.6 (20.8–26.2) | 25.1 (22.4–27.4) | 24.8 (22.8–27.4) | 25.2 (23.4–27.2) | <0.001 |
| GNRI | 107.2 (101.3–111.7) | 96.8 (92.3–99.8) | 105.7 (104.2–107.2) | 108.8 (108.7–110.2) | 113.2 (111.7–114.7) | <0.001 |
| Parameters | CKD Progression | p Value | |
|---|---|---|---|
| (−) (n = 782) | (+) (n = 318) | ||
| Age (years) | 57.1 ± 11.1 | 58.0 ± 11.4 | 0.216 |
| Male (%) | 363 (46.4%) | 164 (51.6%) | 0.121 |
| Hypertension (%) | 365 (48.5%) | 164 (52.4%) | 0.251 |
| SBP | 130.0 (118.0–140.0) | 130.0 (118.0–140.0) | 0.328 |
| DBP | 79.0 (70.0–83.8) | 80.0 (70.0–87.0) | 0.921 |
| DM duration (years) | 9.0 (4.0–14.0) | 13.0 (6.0–18.0) | <0.001 |
| HbA1c (%) | 7.1 (6.5–8.4) | 7.9 (6.7–9.7) | <0.001 |
| FPG (mg/dL) | 131.5 (109.0–170.0) | 144.0 (110.0–202.0) | 0.006 |
| ACEI or ARB (%) | 348 (44.5) | 169 (53.1) | 0.009 |
| Hemoglobin (g/dL) | 13.4 (12.4–14.4) | 12.3 (11.0–14.1) | <0.001 |
| Creatinine at baseline (mg/dL) | 0.9 (0.77–1.07) | 0.94 (0.8–1.2) | 0.004 |
| eGFR at baseline(mL/min/1.73 m2) | 80.7 (69.0–95.0) | 75.7 (59.6–95.4) | 0.006 |
| Calcium | 9.0 (8.6–9.3) | 8.8 (8.3–9.2) | <0.001 |
| Phosphorus | 3.6 (3.2–4.1) | 3.6 (3.2–4.0) | 0.082 |
| Total cholesterol (mg/dL) | 163.0 (141.0–189.0) | 162.0 (138.0–191.0) | 0.934 |
| Albumin (g/dL) | 4.5 (4.2–4.7) | 4.2 (3.8–4.6) | <0.001 |
| UACR at baseline (mg/g) | 13.7 (7.5–27.1) | 22.6 (10.2–129.2) | 0.004 |
| BMI (kg/m2) | 24.7 (22.5–27.0) | 24.8 (22.5–27.3) | 0.327 |
| GNRI score | 108.7 (103.7–111.7) | 104.2 (96.8–110.2) | <0.001 |
| GNRI Q1 | 147 (18.8) | 134 (42.1) | <0.001 |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age > 60 | 1.199 (0.921–1.559) | 0.177 | 2.320 (1.312–4.100) | 0.004 |
| Female gender | 1.229 (0.947–1.596) | 0.121 | 1.610 (00966–2.686) | 0.068 |
| DM duration ≥ 10 years | 2.041 (1.561–2.669) | <0.001 | 1.482 (0.780–2.523) | 0.148 |
| HbA1c ≥ 7.0% | 1.651 (1.247–2.186) | <0.001 | 0.986 (0.587–1.674) | 0.957 |
| Calcium | 0.570 (0.450–0.721) | <0.001 | 1.543 (0.864–2.754) | 0.142 |
| Phosphorus | 0.822 (0.667–1.014) | 0.068 | ||
| Total cholesterol (mg/dL) | 1.00 (0.997–1.003) | 0.928 | ||
| Hemoglobin < 10 g/dL | 3.101 (1.955–4.920) | <0.001 | 1.540 (0.424–5.595) | 0.512 |
| SBP | 1.004 (0.996–1.012) | 0.328 | ||
| DBP | 1.001 (0.998–1.013) | 0.921 | ||
| Baseline eGFR (mL/min/1.73 m2) | 0.991 (0.985–0.997) | 0.003 | 1.025 (1.010–1.040) | 0.001 |
| Presence of proteinuria | 15.958 (7.125–35.744) | <0.001 | 20.311 (6.904–59.750) | <0.001 |
| Use of ACEI or ARB | 1.781 (1.424–2.153) | <0.001 | 2.004 (1.171–3.428) | 0.011 |
| GNRI Q1 vs. Q2,3,4 | 3.146 (2.364–4.187) | <0.001 | 2.526 (1.156–5.521) | 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.J.; Cho, A.; Kim, D.H.; Park, H.C.; Yoon, J.Y.; Shon, K.; Kim, E.; Koo, J.-R.; Lee, Y.-K. Geriatric Nutritional Risk Index as a Prognostic Factor for Renal Progression in Patients with Type 2 Diabetes Mellitus. Nutrients 2023, 15, 4636. https://doi.org/10.3390/nu15214636
Kim EJ, Cho A, Kim DH, Park HC, Yoon JY, Shon K, Kim E, Koo J-R, Lee Y-K. Geriatric Nutritional Risk Index as a Prognostic Factor for Renal Progression in Patients with Type 2 Diabetes Mellitus. Nutrients. 2023; 15(21):4636. https://doi.org/10.3390/nu15214636
Chicago/Turabian StyleKim, Eun Jung, Ajin Cho, Do Hyoung Kim, Hayne Cho Park, Joo Yeon Yoon, Kyungjun Shon, Eunji Kim, Ja-Ryong Koo, and Young-Ki Lee. 2023. "Geriatric Nutritional Risk Index as a Prognostic Factor for Renal Progression in Patients with Type 2 Diabetes Mellitus" Nutrients 15, no. 21: 4636. https://doi.org/10.3390/nu15214636
APA StyleKim, E. J., Cho, A., Kim, D. H., Park, H. C., Yoon, J. Y., Shon, K., Kim, E., Koo, J.-R., & Lee, Y.-K. (2023). Geriatric Nutritional Risk Index as a Prognostic Factor for Renal Progression in Patients with Type 2 Diabetes Mellitus. Nutrients, 15(21), 4636. https://doi.org/10.3390/nu15214636