
The Effect of Vitamin K2 Supplementation on PIVKA-II Levels in Patients with Severe Motor and Intellectual Disabilities Undergoing Long-Term Tube Feeding
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Blood Sampling and Laboratory Examinations
2.3. Assessment of Dietary Vitamin K Intake
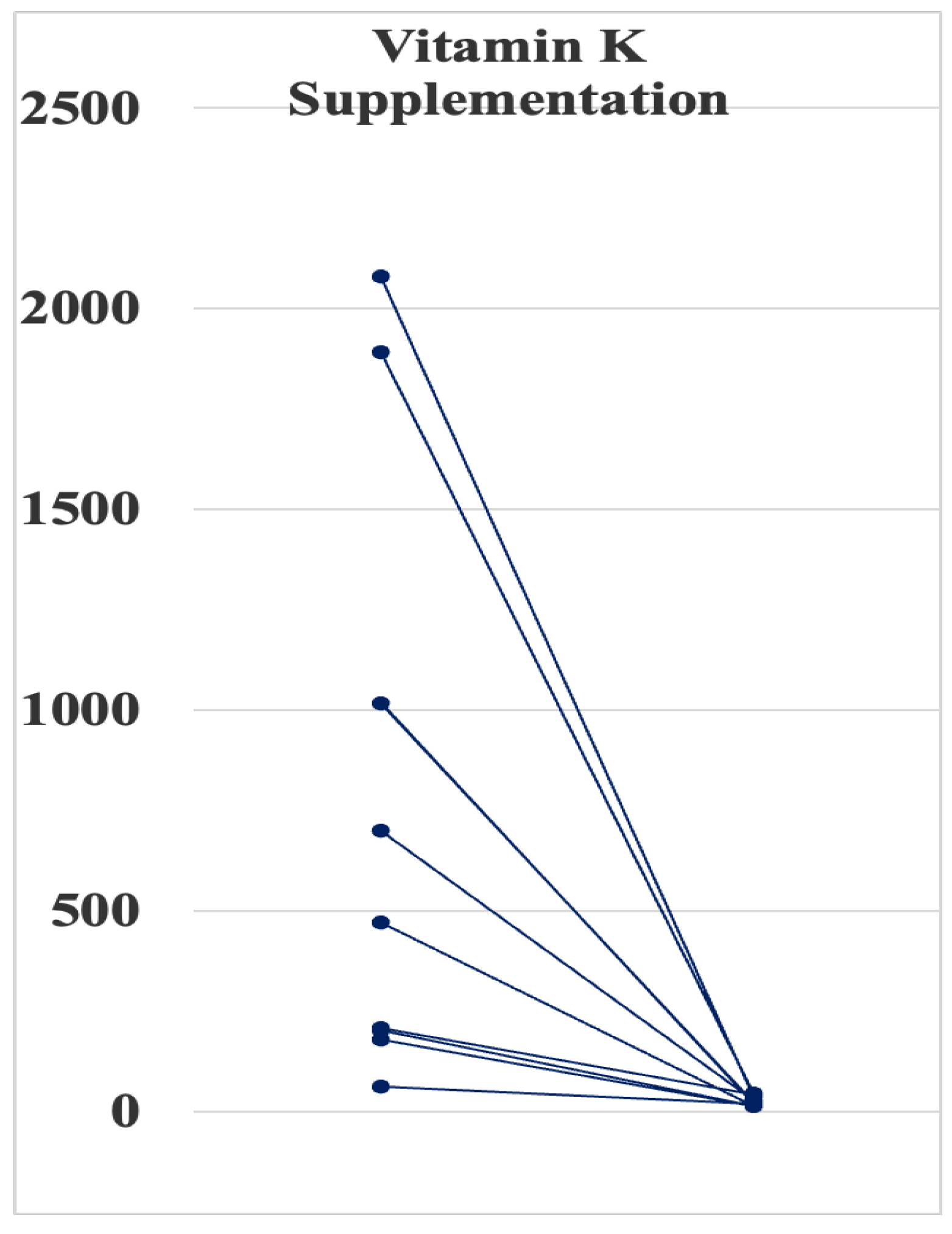
2.4. Supplementation of Vitamin K
2.5. Assessment of Bone Quality at the Calcaneus
2.6. Statistical Analyses
2.7. Ethics Statement
3. Results
3.1. Patients’ Characteristics
3.2. Enteral Tube Feeding
3.3. Vitamin K Status
3.4. Effect of Vitamin K Supplementation on PIVKA-II Levels
3.5. Effect of Vitamin K Supplementation on BMD Parameters at the Calcaneus
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nagae, A.; Kuwabara, A.; Tozawa, K.; Kumode, M.; Takeuchi, Y.; Tanaka, K. Enteral nutrition and antibiotic use increase the risk for vitamin K deficiency in patients with severe motor and intellectual disabilities. e-SPEN J. 2013, 8, e31–e36. [Google Scholar] [CrossRef]
- Konishi, T. SMID and epilepsy. Epilepsy 2013, 17, 113–117. [Google Scholar]
- Morimoto, M.; Satomura, S.; Hashimoto, T.; Kyotani, S. A study of oxidative stress and the newer antiepileptic drugs in epilepsy associated with severe motor and intellectual disabilities. J. Chin. Med. Assoc. 2017, 80, 19–28. [Google Scholar] [CrossRef][Green Version]
- Ohshima, K. Fundamental issues for severe motor and intellectual disabilities. Jap. J. Public Health 1971, 35, 648–655. (In Japanese) [Google Scholar]
- Kuwabara, A.; Nagae, A.; Kitagawa, M.; Tozawa, K.; Kumode, M.; Tanaka, K. Nutritional therapy with vitamin K1 is effective in the improvement of vitamin K status and bone turnover markers in patients with severe motor and intellectual disabilities. J. Nutr. Sci. Vitaminol. 2020, 66, 278–283. [Google Scholar] [CrossRef]
- Ohmori, H.; Kada, A.; Nakamura, M.; Saito, A.M.; Sanayama, Y.; Shinagawa, T.; Fujita, H.; Wakisaka, A.; Maruhashi, K.; Mizukami, A.; et al. Deep vein thrombosis in severe motor and intellectual disabilities patients and its treatment by anticoagulants of warfarin versus edoxaban. Ann. Vasc. Dis. 2019, 12, 372–378. [Google Scholar] [CrossRef]
- Hasegawa, M.; Tomiwa, K.; Higashiyama, Y.; Kawaguchi, C.; Kin, H.; Kubota, M.; Shima, M.; Nogami, K. Risk factors of malnutrition in children with severe motor and intellectual disabilities. Brain Dev. 2020, 42, 738–746. [Google Scholar] [CrossRef]
- Lauriti, G.; Lisi, G.; Chiesa, P.L.; Zani, A.; Pierro, A. Gastroesophageal reflux in children with neurological impairment: A systematic review and meta-analysis. Pediatr. Surg. Int. 2018, 34, 1139–1149. [Google Scholar] [CrossRef]
- Wales, P.W.; Diamond, I.R.; Dutta, S.; Muraca, S.; Chait, P.; Connolly, B.; Langer, J.C. Fundoplication and gastrostomy versus image-guided gastrojejunal tube for enteral feeding in neurologically impaired children with gastroesophageal reflux. J. Pediatr. Surg. 2002, 37, 407–412. [Google Scholar] [CrossRef]
- King, M.; Barnhart, D.C.; O’Gorman, M.; Downey, E.C.; Jackson, D.; Mundorff, M.; Holubkov, R.; Peter, F.; Rajendu, S. Effect of gastrojejunal feedings on visits and costs in children with neurologic impairment. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 518–524. [Google Scholar] [CrossRef]
- Ohmori, H.; Kodama, H.; Takemoto, M.; Yamasaki, M.; Matsumoto, T.; Kumode, M.; Miyachi, T.; Sumimoto, R. Isolated neutropenia caused by copper deficiency due to jejunal feeding and excessive zinc intake: A case report. World J. Clin. Cases 2021, 9, 8825–8830. [Google Scholar] [CrossRef]
- Sakai, T.; Shirai, T.; Oishi, T. Vitamin K and D deficiency in severe motor and intellectual disabled patients. Brain Dev. 2021, 43, 200–207. [Google Scholar] [CrossRef]
- Mergler, S.; Evenhuis, H.M.; Boot, A.M.; De Man, S.A.; Bindels-De Heus, K.G.C.B.; Huijbers, W.A.R.; Penning, C. Epidemiology of low bone mineral density and fractures in children with severe cerebral palsy: A systematic review. Dev. Med. Child. Neurol. 2009, 51, 773–778. [Google Scholar] [CrossRef]
- Maruyama, K.; Kurahashi, H.; Suzuki, M.; Miura, K.; Kumagai, T. Survival analysis for patients with severe motor and intellectual disabilities following tracheotomy. No To Hattatsu 2012, 44, 25–28. [Google Scholar]
- Shea, M.K.; Booth, L.S. Concepts and controversies in evaluating vitamin K status in population-based studies. Nutrients 2016, 8, 8. [Google Scholar] [CrossRef]
- Japanese Ministry of Health, Labour, and Welfare. Dietary Reference Intakes for Japanese 2020. Available online: https://www.mhlw.go.jp/stf/newpage_08517.html (accessed on 20 December 2021).
- Iwamoto, J. Vitamin K₂ therapy for postmenopausal osteoporosis. Nutrients 2014, 6, 1971–1980. [Google Scholar] [CrossRef]
- Asakura, H.; Myou, S.; Ontachi, Y.; Mizutani, T.; Kato, M.; Saito, M.; Morishita, E.; Yamazaki, M.; Nakao, S. Vitamin K administration to elderly patients with osteoporosis induces no hemostatic activation, even in those with suspected vitamin K deficiency. Osteoporos. Int. 2001, 12, 996–1000. [Google Scholar] [CrossRef]
- Hashizume, N.; Tanaka, Y.; Yoshida, M.; Fukahori, S.; Ishii, S.; Saikusa, N.; Masui, D.; Higashidate, N.; Sakamoto, S.; Tsuruhisa, S.; et al. Resting energy expenditure prediction using bioelectrical impedance analysis in patients with severe motor and intellectual disabilities. Brain Dev. 2019, 41, 352–358. [Google Scholar] [CrossRef]
- Ohwada, H.; Nakayama, T.; Ishikawa-Takata, K.; Iwasaki, N.; Kanaya, Y.; Tanaka, S. Total energy expenditure among children with motor, intellectual, visual, and hearing disabilities: A doubly labeled water method. Eur. J. Clin. Nutr. 2021, 75, 1607–1617. [Google Scholar] [CrossRef]
- Yoshikawa, H.; Yamazaki, S.; Watanabe, T.; Abe, T. Vitamin K deficiency in severely disabled children. J. Clin. Neurol. 2003, 18, 93–97. [Google Scholar] [CrossRef]
- Tanaka, Y.; Shibata, R. Effects of vitamin K2 administration in the patients with severely motor and intellectual disabilities: Assessment of bone metabolic marker and bone mineral density. No To Hattatsu 2000, 32, 491–496. [Google Scholar] [PubMed]
- Binkley, N.C.; Krueger, D.C.; Kawahara, T.N.; Engelke, J.A.; Chappell, R.J.; Suttie, J.W. A high phylloquinone intake is required to achieve maximal osteocalcin gamma-carboxylation. Am. J. Clin. Nutr. 2002, 76, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Shearer, M.J.; Hamulyák, K.; Stöcklin, E.; Vermeer, C. Effect of vitamin K intake on the stability of oral anticoagulant treatment: Dose-response relationships in healthy subjects. Blood 2004, 104, 2682–2689. [Google Scholar] [CrossRef][Green Version]
- Cheung, A.M.; Tile, L.; Lee, Y.; Tomlinson, G.; Hawker, G.; Scher, J.; Hu, H.; Vieth, R.; Thompson, L.; Jamal, S.; et al. Vitamin K supplementation in postmenopausal women with osteopenia (ECKO trial): A randomized controlled trial. PLoS Med. 2008, 5, e196. [Google Scholar] [CrossRef] [PubMed]
- Hanaoka, T.; Mita, K.; Hiramoto, A.; Suzuki, Y.; Maruyama, S.; Nakadate, T.; Kishi, R.; Okada, K.; Egusa, Y. Survival prognosis of Japanese with severe motor and intellectual disabilities living in public and private institutions between 1961 and 2003. J. Epidemiol. 2010, 20, 77–81. [Google Scholar] [CrossRef]


{kind=link}
| Elevated (n = 13) | Normal (n = 7) | |
|---|---|---|
| PIVKA-II (mAU/mL) (Normal Range < 40) | 616 ± 194 (44–2080) | 28 ± 3 (21–39) |
| Blood coagulation test | ||
| Prothrombin time (s) (normal range: 10.0–13.0) | 13.9 ± 1.4 | 11.9 ± 0.3 |
| PT (%) (normal range: 80–120) | 78 ± 5 | 91 ± 5 |
| PT-INR (normal range: 1.00–1.40) | 1.25 ± 0.14 | 1.10 ± 0.05 |
| aPTT (s) (normal range: 24.5–33.5) | 35.9 ± 1.7 | 35.8 ± 1.6 |
| Fibrinogen (mg/dL) (normal range: 200–400) | 316 ± 27 | 332 ± 19 |
| AT-III (%) (normal range: 5–125) | 109 ± 4 | 113 ± 4 |
| Duration of tube feeding (years) | 10 ± 2 | 11.9 ± 0.3 |
| Daily nutritional intake | ||
| Vitamin K intake (µg/day) | 53 ± 5 | 70 ± 9 |
| Percentile of recommended daily vitamin K intake (%) | 36.7 ± 2.6 | 46.5 ± 6.2 |
| Energy intake (kcal/day) | 950 ± 50 | 970 ± 102 |
| Percentile of recommended daily energy intake (%) | 43.0 ± 3.1 | 44.1 ± 5.3 |
| Protein (g/day) | 45 ± 3 | 45 ± 4 |
| Fat (g/day) | 29 ± 10 | 29 ± 4 |
| Carbohydrate (g/day) | 133 ± 10 | 127 ± 15 |
| Nutritional parameters | ||
| Albumin (g/dL) | 3.6 ± 0.1 * | 3.8 ± 0.2 |
| Transferrin (mg/dL) | 225 ± 10 | 220 ± 9 |
| Transthyretin (mg/dL) | 29 ± 2 | 31 ± 3 |
| Retinol binding protein (mg/dL) | 7.0 ± 0.9 | 6.4 ± 1.0 |
| Ceruloplasmin (mg/dL) | 32.7 ± 1.9 | 33.5 ± 2.6 |
| Total cholesterol (mg/dL) | 164 ± 7 | 175 ± 9 |
| Triglyceride (mg/dL) | 124 ± 21 | 79 ± 13 |
| HDL cholesterol (mg/dL) | 58 ± 6 | 66 ± 6 |
| LDL cholesterol (mg/dL) | 81 ± 6 | 92 ± 8 |
| Cholinesterase (U/L) | 312 ± 13 | 360 ± 19 |
| Total lymphocyte count (/μL) | 2003 ± 356 | 2064 ± 399 |
| C-reactive protein (mg/dL) | 0.56 ± 0.14 | 0.48 ± 0.17 |
| Liver and kidney functions | ||
| AST (IU/L) | 23 ± 2 | 17 ± 2 |
| ALT (IU/L) | 21 ± 3 | 16 ± 1 |
| γ-GTP (IU/L) | 81 ± 14 | 56 ± 13 |
| ALP (IU/mL) | 136 ± 15 | 99 ± 8 |
| LDH (U/L) | 159 ± 11 | 145 ± 20 |
| CPK (U/L) | 57 ± 12 | 72 ± 20 |
| Creatinine (mg/dL) | 0.58 ± 0.16 | 0.56 ± 0.12 |
| Blood urea nitrogen (mg/dL) | 17.3 ± 6.2 | 17.4 ± 4.0 |
| Elevated (n = 9) | Normal (n = 11) | |
|---|---|---|
| Osteocalcin (ng/mL) | 30.2 ± 11.7 | 22.1 ± 9.9 |
| ucOC (ng/mL) (normal range < 4.5 ng/mL) | 7.59 ± 3.12 | 2.44 ± 1.08 |
| Blood coagulation test | ||
| Prothrombin time (s) (normal range: 10.0–13.0) | 14.0 ± 6.4 | 12.2 ± 0.8 |
| PT (%) (normal range: 80–120) | 82 ± 25 | 86 ± 14 |
| PT-INR (normal range: 1.00–1.40) | 1.28 ± 0.64 | 1.08 ± 0.08 |
| aPTT (s) (normal range: 24.5–33.5) | 35.5 ± 7.9 | 35.1 ± 3.2 |
| Fibrinogen (mg/dL) (normal range: 200–400) | 344 ± 76 | 309 ± 93 |
| AT-III (%) (normal range: 5–125) | 113 ± 13 | 110 ± 12 |
| Duration of tube feeding (years) | 12 ± 8 | 13 ± 7 |
| Daily nutritional intake | ||
| Vitamin K intake (µg/day) | 55 ± 25 | 61 ± 18 |
| Percentile of recommended daily vitamin K intake (%) | 39.0 ± 14.2 | 41.0 ± 12.2 |
| Energy intake (kcal/day) | 947 ± 205 | 970 ± 220 |
| Protein (g/day) | 48 ± 12 | 43 ± 12 |
| Fat (g/day) | 22 ± 12 | 36 ± 39 |
| Carbohydrate (g/day) | 136 ± 29 | 132 ± 37 |
| Nutritional parameters | ||
| Albumin (g/dL) | 3.7 ± 0.4 | 3.6 ± 0.4 |
| Transferrin (mg/dL) | 221 ± 36 | 225 ± 31 |
| Transthyretin (mg/dL) | 31 ± 8 | 31 ± 3 |
| Retinol binding protein (mg/dL) | 7.4 ± 4.2 | 6.2 ± 1.9 |
| Ceruloplasmin (mg/dL) | 34.8 ± 8.0 | 30.8 ± 4.7 |
| Total cholesterol (mg/dL) | 157 ± 12 | 175 ± 9 |
| Triglyceride (mg/dL) | 136 ± 83 | 85 ± 36 |
| HDL cholesterol (mg/dL) | 55 ± 22 | 66 ± 14 |
| LDL cholesterol (mg/dL) | 75 ± 12 | 93 ± 24 |
| Cholinesterase (U/L) | 352 ± 62 | 310 ± 35 |
| Total lymphocyte count (/μL) | 2376 ± 1277 | 1737 ± 1010 |
| C-reactive protein (mg/dL) | 0.60 ± 0.60 | 0.47 ± 0.35 |
| Liver and kidney functions | ||
| AST (IU/L) | 21 ± 10 | 21 ± 6 |
| ALT (IU/L) | 20 ± 10 | 19 ± 7 |
| γ-GTP (IU/L) | 72 ± 57 | 72 ± 35 |
| ALP (IU/mL) | 124 ± 67 | 112 ± 32 |
| LDH (U/L) | 150 ± 42 | 154 ± 42 |
| CPK (U/L) | 53 ± 48 | 59 ± 39 |
| Creatinine (mg/dL) | 0.64 ± 0.69 | 0.51 ± 0.28 |
| Blood urea nitrogen (mg/dL) | 18.7 ± 18.1 | 16.3 ± 13.6 |
| MK-4 Treatment | T-Score | Z-Score | ||
|---|---|---|---|---|
| Before | After | Before | After | |
| Yes (n = 4) | −5.5 ± 1.0 | −6.1 ± 0.9 | −3.9 ± 1.3 | −5.0 ± 2.1 |
| No (n = 6) | −6.3 ± 1.0 | −6.4 ± 0.8 | −4.6 ± 1.2 | −4.6 ± 1.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohmori, H.; Kato, A.; Shirai, Y.; Fukano, R.; Nagae, A.; Yamasaki, M.; Komenaka, J.; Imamura, E.; Kumode, M.; Miyachi, T. The Effect of Vitamin K2 Supplementation on PIVKA-II Levels in Patients with Severe Motor and Intellectual Disabilities Undergoing Long-Term Tube Feeding. Nutrients 2023, 15, 4525. https://doi.org/10.3390/nu15214525
Ohmori H, Kato A, Shirai Y, Fukano R, Nagae A, Yamasaki M, Komenaka J, Imamura E, Kumode M, Miyachi T. The Effect of Vitamin K2 Supplementation on PIVKA-II Levels in Patients with Severe Motor and Intellectual Disabilities Undergoing Long-Term Tube Feeding. Nutrients. 2023; 15(21):4525. https://doi.org/10.3390/nu15214525
Chicago/Turabian StyleOhmori, Hiromitsu, Akihiko Kato, Yuka Shirai, Reiji Fukano, Akiko Nagae, Masami Yamasaki, Junko Komenaka, Eiji Imamura, Masao Kumode, and Takafumi Miyachi. 2023. "The Effect of Vitamin K2 Supplementation on PIVKA-II Levels in Patients with Severe Motor and Intellectual Disabilities Undergoing Long-Term Tube Feeding" Nutrients 15, no. 21: 4525. https://doi.org/10.3390/nu15214525
APA StyleOhmori, H., Kato, A., Shirai, Y., Fukano, R., Nagae, A., Yamasaki, M., Komenaka, J., Imamura, E., Kumode, M., & Miyachi, T. (2023). The Effect of Vitamin K2 Supplementation on PIVKA-II Levels in Patients with Severe Motor and Intellectual Disabilities Undergoing Long-Term Tube Feeding. Nutrients, 15(21), 4525. https://doi.org/10.3390/nu15214525