
Snacking Behaviours of Australian Young Adults: Secondary Analysis of the MYMeals Cross-Sectional Study

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Recruitment
2.3. Assessment of Dietary Intake
2.4. Demographic Classification
2.5. Data Cleaning
2.6. Food Categorisation
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Snack Consumers
3.2. Contribution of Snacking to Total Energy and Nutrient Intakes
3.3. Average Total Energy and Nutrient Intake from Snacking
3.4. The Proportion of Discretionary Food Consumed as Snacks
3.5. Top Ten Food Sources by Frequency and Energy Contribution
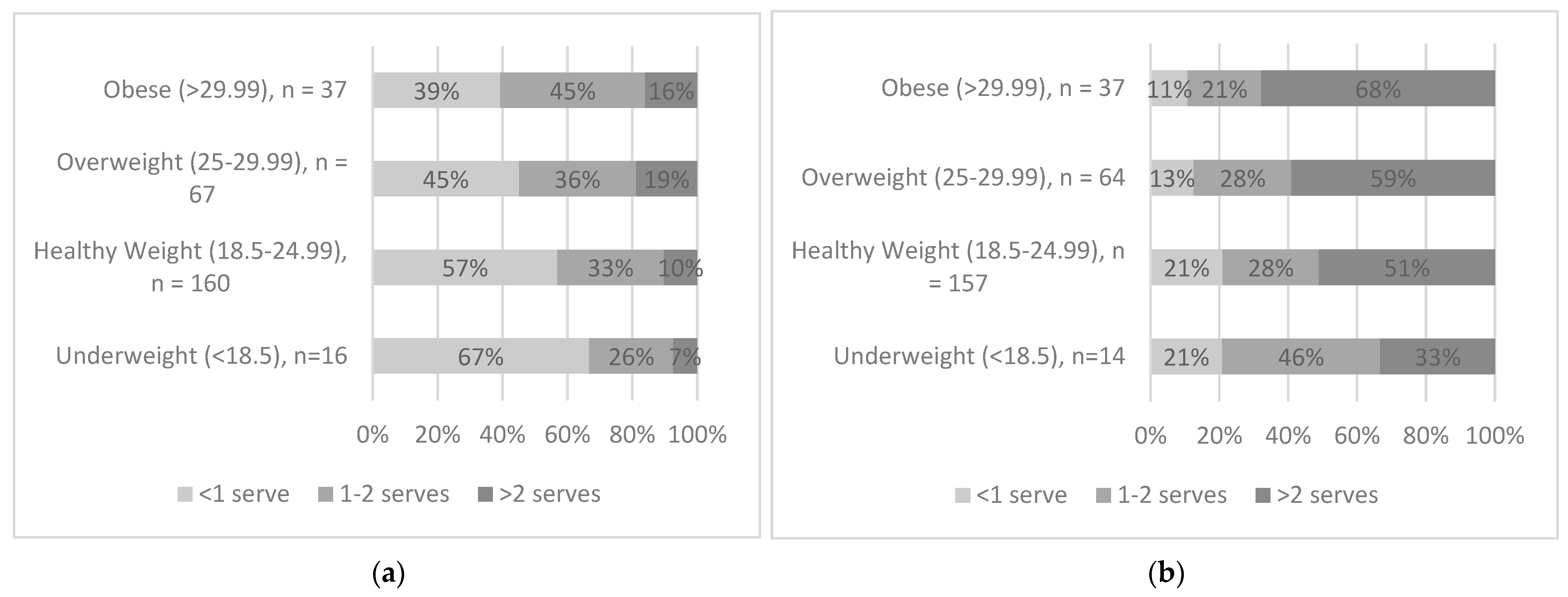
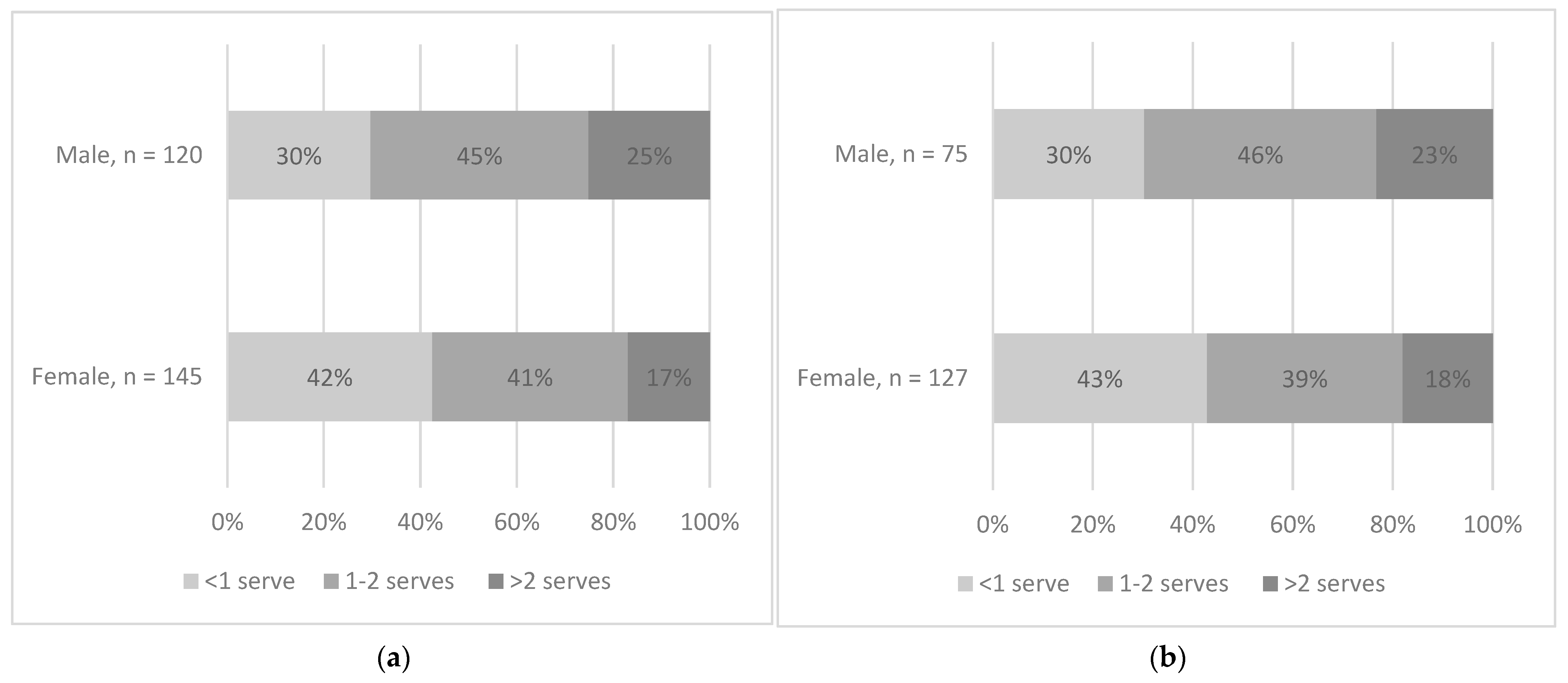
3.6. Portion Size (g) of Top Five Most Common Discretionary Foods Consumed as Snacks
3.7. Portion Sizes of Top Five Most Common Discretionary Foods Consumed as Snacks
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obesity and Overweight: World Health Organisation 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 August 2023).
- Australian Bureau of Statistics. National Health Survey: First Results 2017–2018. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-first-results/latest-release (accessed on 12 August 2023).
- Biro, F.M.; Wien, M. Childhood obesity and adult morbidities. Am. J. Clin. Nutr. 2010, 91, 1499S–1505S. [Google Scholar] [CrossRef]
- Singh, A.S.; Mulder, C.; Twisk, J.W.; Van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obesity Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.; Gearon, E.; Backholer, K.; Bauman, A.; Peeters, A. Age-specific changes in BMI and BMI distribution among Australian adults using cross-sectional surveys from 1980 to 2008. Int. J. Obes. 2015, 39, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Australian Government National Health and Medical Research Council. Australian Dietary Guidelines 2013; National Health and Medical Research Council: Canberra, Australia, 2013.
- Laska, M.N.; Hearst, M.O.; Lust, K.; Lytle, L.A.; Story, M. How we eat what we eat: Identifying meal routines and practices most strongly associated with healthy and unhealthy dietary factors among young adults. Public Health Nutr. 2015, 18, 2135–2145. [Google Scholar] [CrossRef]
- Powell, P.K.; Durham, J.; Lawler, S. Food Choices of Young Adults in the United States of America: A Scoping Review. Adv. Nutr. 2019, 10, 479–488. [Google Scholar] [CrossRef]
- Almoraie, N.M.; Saqaan, R.; Alharthi, R.; Alamoudi, A.; Badh, L.; Shatwan, I.M. Snacking patterns throughout the life span: Potential implications on health. Nutr. Res. 2021, 91, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Pendergast, F.J.; Livingstone, K.M.; Worsley, A.; McNaughton, S.A. Correlates of meal skipping in young adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 125. [Google Scholar] [CrossRef]
- Smith-Jackson, T.; Reel, J.J. Freshmen women and the “Freshman 15”: Perspectives on prevalence and causes of college weight gain. J. Amer Coll. Health 2012, 60, 14–20. [Google Scholar] [CrossRef]
- Arouchon, K.; Rubino, A.; Edelstein, S. Revisiting the freshman 15: Female freshman weight status, dietary habits, and exercise habits. J. Foodserv. Bus. Res. 2016, 19, 1–10. [Google Scholar] [CrossRef]
- Lopes, T.D.; Mello, A.V.D.; Nogueira, L.R.; Leme, A.C.B.; Fisberg, R.M. Energy, nutrients and food sources in snacks for adolescents and young adults. Rev. Paul. Pediatr. 2021, 40, E2020148. [Google Scholar] [CrossRef]
- Rebuli, M.A.; Williams, G.; James-Martin, G.; Hendrie, G.A. Food group intake at self-reported eating occasions across the day: Secondary analysis of the Australian National Nutrition Survey 2011–2012. Public Health Nutr. 2020, 23, 3067–3080. [Google Scholar] [CrossRef] [PubMed]
- Kirk, T.R. Role of dietary carbohydrate and frequent eating in body-weight control. Proc. Nutr. Soc. 2000, 59, 349–358. [Google Scholar] [CrossRef]
- Zizza, C.A.; Xu, B. Snacking is associated with overall diet quality among adults. J. Acad. Nutr. Diet. 2012, 112, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Marangoni, F.; Martini, D.; Scaglioni, S.; Sculati, M.; Donini, L.M.; Leonardi, F.; Agostoni, C.; Castelnuovo, G.; Ferrara, N.; Ghiselli, A.; et al. Snacking in nutrition and health. Int. J. Food Sci. Nutr. 2019, 70, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Wellard-Cole, L.; Davies, A.; Chen, J.; Jung, J.; Bente, K.B.; Kay, J.; Watson, W.L.; Hughes, C.; Rangan, A.; Yacef, K.; et al. The contribution of foods prepared outside the home to the diets of 18-to 30-year-old Australians: The MYMeals study. Nutrients 2021, 13, 1761. [Google Scholar] [CrossRef]
- Wellard-Cole, L.; Chen, J.; Davies, A.; Wong, A.; Huynh, S.; Rangan, A.; Allman-Farinelli, M. Relative Validity of the Eat and Track (EaT) Smartphone App for Collection of Dietary Intake Data in 18-to-30-Year Olds. Nutrients 2019, 11, 621. [Google Scholar] [CrossRef]
- Duncan, A.; Rangan, A.; Ho, P.Y.; Chan, V.; Davies, A.J.; Wellard-Cole, L.; Allman-Farinelli, M. High Consumption of Discretionary Beverages in Young Australian Adults Aged 18–30 Years: A Cross-Sectional Study. Dietetics 2022, 1, 105–113. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics—Australian Health Survey: Users’ Guide, 2011–2013. Catalogue Number 4363.0.55.001, ABS Canberra. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/mf/4363.0.55.001 (accessed on 12 August 2023).
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. S1), 5–41. [Google Scholar]
- Wolfenden, L.; Barnes, C.; Lane, C.; McCrabb, S.; Brown, H.M.; Gerritsen, S.; Baquera, S.; Vejar, L.S.; Munguia, A.; Yoong, S.L. Consolidating evidence on the effectiveness of interventions promoting fruit and vegetable consumption: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 11. [Google Scholar] [CrossRef]
- Veldhorst, M.; Smeets, A.; Soenen, S.; Hochstenbach-Waelen, R.; Hursel, K.; Diepvens, M.; Lejeune, N.; Luscombe-Marsh, M.; Westerterp-Plantenga, M. Protein-induced satiety: Effects and mechanisms of different proteins. Physiol. Behav. 2008, 94, 300–307. [Google Scholar] [CrossRef]
- Zheng, M.; Rangan, A.; Meertens, B.; Wu, J.H.Y. Changes in Typical Portion Sizes of Commonly Consumed Discretionary Foods among Australian Adults from 1995 to 2011–2012. Nutrients 2017, 9, 577. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Patel, Z.; Jones, A. Downsizing food: A systematic review and meta-analysis examining the effect of reducing served food portion sizes on daily energy intake and body weight. Br. J. Nutr. 2023, 129, 888–903. [Google Scholar] [CrossRef]
- Higgins, K.; Hudson, J.L.; Hayes, A.M.; Braun, E.; Cheon, E.; Couture, S.C.; Gunaratna, N.S.; Hill, E.R.; Hunter, S.R.; McGowan, B.S.; et al. Systematic review and meta-analysis on the effect of portion size and ingestive frequency on energy intake and body weight among adults in Randomized Controlled feeding trials. Adv. Nutr. 2022, 13, 248–268. [Google Scholar] [CrossRef] [PubMed]
- Njike, V.Y.; Smith, T.M.; Shuval, O.; Shuval, K.; Edshteyn, I.; Kalantari, V.; Yaroch, A.L. Snack Food, Satiety, and Weight. Adv. Nutr. 2016, 7, 866–878. [Google Scholar] [CrossRef]
- Grech, A.; Rangan, A.; Allman-Farinelli, M. Social Determinants and Poor Diet Quality of Energy-Dense Diets of Australian Young Adults. Healthcare 2017, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Savige, G.; Macfarlane, A.; Ball, K.; Worsley, A.; Crawford, D. Snacking behaviours of adolescents and their association with skipping meals. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Vandevijvere, S.; Kraak, V.; Sacks, G.; Snowdon, W.; Hawkes, C.; Barquera, S.; Friel, S.; Kelly, B.; Kumanyika, S. Monitoring public sector policies and actions. Obes. Rev. 2013, 14, 24–37. [Google Scholar] [CrossRef]
- Chan, V.; Wellard-Cole, L.; Davies, A.; Watson, W.; Hughes, C.; Chapman, K.; Signal, L.; Ni Mhurchu, C.; Wang, L.; D’Souza, D.; et al. The Association of Social and Food Preparation Location Context with the Quality of Meals and Snacks Consumed by Young Adults: Findings from the MYMeals Wearable Camera Study. Eur. J. Nutr. 2022, 61, 3407–3422. [Google Scholar] [CrossRef]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Total Sample n = 889 (%) | |
|---|---|---|
| Total sample | 889 | |
| Gender | Female | 520 (58) |
| Male | 369 (42) | |
| Age group (years) | 18–24 | 479 (54) |
| 25–30 | 410 (46) | |
| Body Mass Index (kg/m2) | Underweight (<18.5) | 47 (5) |
| Healthy weight (18.5–24.99) | 501 (56) | |
| Overweight (25–29.99) | 224 (25) | |
| Obese (>29.99) | 117 (13) | |
| Socioeconomic status a | Low | 363 (41) |
| High | 526 (59) | |
| Sample Size, n | Energy | Protein | Total Sugars | Sodium | Saturated Fat | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (%) | IQR | Median (%) | IQR | Median (%) | IQR | Median (%) | IQR | Median (%) | IQR | ||
| Consumers | 889 | 13.2 | 13 | 6.2 | 8.4 | 23.4 | 25.1 | 7.3 | 11.7 | 16.2 | 20.2 |
| Age (years) | |||||||||||
| 18–24 | 479 | 13.5 | 12.6 | 6.2 | 8.2 | 23.4 | 25.6 | 7.4 | 11.1 | 16.6 | 20.7 |
| 25–30 | 410 | 12.9 | 13.4 | 6.4 | 8.9 | 23.2 | 24.9 | 7.3 | 12.5 | 15.7 | 19.8 |
| p-Value | 0.852 | 0.674 | 0.492 | 0.913 | 0.828 | ||||||
| Gender | |||||||||||
| Male | 369 | 12.2 | 12.8 | 5.7 | 9 | 20.7 | 21.6 | 6.8 | 12 | 15.3 | 19 |
| Female | 520 | 13.8 | 13.3 | 6.5 | 8 | 25.8 | 26.3 | 7.6 | 11.4 | 17 | 22.1 |
| p-Value | 0.007 | 0.082 | 0.009 | 0.167 | 0.111 | ||||||
| SES a | |||||||||||
| Low | 363 | 13.5 | 14.4 | 6.5 | 8.8 | 22.9 | 25.9 | 7.9 | 12.8 | 16.5 | 20.6 |
| High | 526 | 12.9 | 12.4 | 5.9 | 8.2 | 23.9 | 24.5 | 7 | 11.1 | 15.8 | 19.7 |
| p-Value | 0.344 | 0.359 | 0.389 | 0.144 | 0.531 | ||||||
| BMI | |||||||||||
| Underweight (<18.5) | 47 | 12.8 | 11.9 | 5.7 | 7.7 | 24.8 | 23.5 | 6.8 | 10.4 | 13.5 | 14.2 |
| Healthy weight (18.5–24.99) | 501 | 13.6 | 13.3 | 6.4 | 8.7 | 23.8 | 25.1 | 7.6 | 11.7 | 16.6 | 22.2 |
| Overweight (25–29.99) | 224 | 12.8 | 12.2 | 6.5 | 8.9 | 22.9 | 23.8 | 7.3 | 12.4 | 16.6 | 17.7 |
| Obese (>29.99) | 117 | 12.5 | 13.7 | 5.4 | 7.8 | 22.2 | 26.4 | 6.1 | 11.9 | 14.7 | 17 |
| p-Value | 0.619 | 0.254 | 0.795 | 0.468 | 0.463 | ||||||
| Characteristics | Sample Size, n | Total Energy (kJ) | Total Protein (g) | Total Sugars (g) | Total Sodium (mg) | Total Saturated Fat (g) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | ||
| Consumers (total) | 889 | 993 | 1192 | 4.8 | 7.5 | 15.1 | 20.3 | 164 | 295 | 4.1 | 6.1 |
| Age (years) | |||||||||||
| 18–24 | 479 | 994 | 1173 | 4.7 | 7.0 | 15.7 | 19.9 | 164 | 293 | 4.2 | 6.2 |
| 25–30 | 410 | 985 | 1206 | 5.0 | 8.1 | 14.2 | 20.0 | 164 | 309 | 4.0 | 6.2 |
| p-Value | 0.97 | 0.24 | 0.33 | 0.97 | 0.66 | ||||||
| Gender | |||||||||||
| Male | 369 | 1043 | 1327 | 5.0 | 8.7 | 15.2 | 20.2 | 176 | 380 | 4.5 | 6.7 |
| Female | 520 | 975 | 1100 | 4.7 | 6.7 | 14.8 | 20.4 | 156 | 259 | 3.8 | 5.9 |
| p-Value | 0.40 | 0.48 | 0.87 | 0.48 | 0.07 | ||||||
| SES a | |||||||||||
| Low | 363 | 1033 | 1259 | 5.0 | 7.0 | 15.5 | 20.5 | 177 | 313 | 4.1 | 6.8 |
| High | 526 | 983 | 1151 | 4.7 | 7.9 | 14.8 | 20.0 | 156 | 275 | 4.0 | 5.9 |
| p-Value | 0.48 | 0.26 | 0.66 | 0.16 | 0.98 | ||||||
| BMI | |||||||||||
| Underweight | 47 | 922 | 946 | 3.8 | 5.8 | 14.3 | 21.0 | 123 | 199 | 3.6 | 4.8 |
| Healthy weight | 501 | 1023 | 1168 | 4.8 | 7.7 | 15.2 | 19.9 | 166 | 281 | 4.2 | 6.1 |
| Overweight | 224 | 1030 | 1203 | 5.3 | 7.5 | 15.0 | 20.0 | 183 | 337 | 4.2 | 6.9 |
| Obese | 117 | 925 | 1333 | 3.9 | 7.2 | 14.3 | 23.6 | 117 | 310 | 3.7 | 6.8 |
| p-Value | 0.69 | 0.19 | 0.96 | 0.64 | 0.82 | ||||||
| Characteristics | Total Snacks, n | Discretionary, n (%) | Five Food Groups, n (%) | p-Value |
|---|---|---|---|---|
| Age | ||||
| 18–24 yrs., n = 479 | 2448 | 1415 (58) | 1033 (42) | 0.253 |
| 25–30 yrs., n = 410 | 2237 | 1256 (56) | 981 (44) | |
| Gender | ||||
| Male, n = 369 | 1830 | 1058 (58) | 772 (42) | 0.374 |
| Female, n = 520 | 2855 | 1613 (56) | 1242 (44) | |
| SES | ||||
| Low, n = 363 | 1790 | 1097 (61) | 693 (39) | <0.001 |
| High, n = 526 | 2895 | 1574 (54) | 1321 (46) | |
| BMI | ||||
| Underweight, n = 47 | 260 | 138 (53) | 122 (47) | <0.001 |
| Healthy weight, n = 501 | 2813 | 1523 (54) | 1290 (46) | |
| Overweight, n = 224 | 1108 | 664 (60) | 444 (40) | |
| Obese, n = 117 | 504 | 346 (69) | 158 (31) |
| Snack Food | Frequency of Consumption (%) | Rank | Snack Food | Energy Contribution (%) | |
|---|---|---|---|---|---|
| 1 | Fruit (fresh and dried) | 20.2% | 1 | Cakes, doughnuts, muffins, pastries, slices, sugar desserts | 17.6% |
| 2 | Chocolate | 9.9% | 2 | Chocolate | 11.1% |
| 3 | Cakes, doughnuts, muffins, pastries, slices, sugar desserts | 8.4% | 3 | Fruit (fresh and dried) | 7.8% |
| 4 | Sweet biscuits | 6.1% | 4 | Crisps, extruded snacks | 7.2% |
| 5 | Ice cream, cream, soft serve, frozen yoghurt | 5.6% | 5 | Ice cream, cream, soft serve, frozen yoghurt | 6.7% |
| 6 | Crisps, extruded snacks | 5.6% | 6 | Sweet biscuits | 5.9% |
| 7 | Nuts and seeds | 4.6% | 7 | Nuts and seeds | 5.3% |
| 8 | Vegetables | 3.6% | 8 | Muesli bars, nut- and seed-based confectionary | 2.7% |
| 9 | Lollies | 3.1% | 9 | Potato products | 2.5% |
| 10 | Muesli bars, nut- and seed-based confectionary | 3.0% | 10 | Sweet breads | 2.4% |
| Food Category | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cakes, Muffins, Sweet Pastries, Sugar-Type Desserts | Chocolate | Fruit (Fresh and Dried) | Crisps, Extruded Snacks | Ice Cream and Frozen Yoghurt | ||||||||||||
| n | Median (g) | IQR | n | Median (g) | IQR | n | Median (g) | IQR | n | Median (g) | IQR | n | Median (g) | IQR | ||
| Consumers a | 272 | 95 | 88 | 280 | 26 | 36 | 437 | 106 | 73 | 202 | 45 | 28 | 265 | 75 | 42 | |
| Gender | Female | 170 | 95 | 92 | 164 | 26 | 34 | 275 | 95 | 72 | 127 | 40 | 30 | 145 | 74 | 41 |
| Male | 102 | 95 | 82 | 116 | 26 | 36 | 162 | 117 | 69 | 75 | 45 | 25 | 120 | 89 | 59 | |
| p-Value | 0.794 | 0.621 | 0.057 | 0.048 | 0.002 | |||||||||||
| BMI | Obese | 37 | 117 | 105 | 37 | 42 | 33 | 44 | 99 | 103 | 29 | 47 | 29 | 37 | 90 | 74 |
| Overweight | 64 | 101 | 88 | 67 | 30 | 35 | 98 | 111 | 77 | 53 | 40 | 29 | 71 | 75 | 41 | |
| Healthy weight | 157 | 90 | 89 | 160 | 25 | 27 | 269 | 104 | 70 | 110 | 45 | 29 | 144 | 74 | 42 | |
| Underweight | 14 | 76 | 70 | 16 | 25 | 24 | 26 | 109 | 77 | 10 | 45 | 25 | 13 | 75 | 66 | |
| p-Value | 0.021 | <0.01 | 0.656 | 0.899 | 0.090 | |||||||||||
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Trend | |
|---|---|---|---|---|---|
| <524 kJ | 524–992 kJ | 993–1709 kJ | >1709 kJ | ||
| n | 223 | 222 | 222 | 222 | |
| Total energy (%) | 4.9 (0.2) | 11.2 (0.3) | 16.7 (0.3) | 28.3 (0.6) | <0.001 |
| Total energy (kJ) | 6714 (188) | 7651 (179) | 8420 (149) | 10243 (221) | <0.001 |
| Protein (g) | 80.3 (2.6) | 84.6 (2.2) | 89.9 (2.2) | 103.2 (3.4) | <0.001 |
| Total sugars (g) | 51.2 (2.0) | 68.4 (2.4) | 76.0 (2.3) | 105.5 (3.2) | <0.001 |
| Saturated fat (g) | 21.6 (0.9) | 25.2 (0.9) | 29.0 (0.7) | 38.6 (1.2) | <0.001 |
| Sodium (mg) | 2244 (67) | 2336 (72) | 2682 (72) | 3014 (88) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.Y.; Morris, K.; Wellard-Cole, L.; Davies, A.; Rangan, A.; Allman-Farinelli, M. Snacking Behaviours of Australian Young Adults: Secondary Analysis of the MYMeals Cross-Sectional Study. Nutrients 2023, 15, 4471. https://doi.org/10.3390/nu15204471
Han JY, Morris K, Wellard-Cole L, Davies A, Rangan A, Allman-Farinelli M. Snacking Behaviours of Australian Young Adults: Secondary Analysis of the MYMeals Cross-Sectional Study. Nutrients. 2023; 15(20):4471. https://doi.org/10.3390/nu15204471
Chicago/Turabian StyleHan, Jae Youn (Lisa), Katrina Morris, Lyndal Wellard-Cole, Alyse Davies, Anna Rangan, and Margaret Allman-Farinelli. 2023. "Snacking Behaviours of Australian Young Adults: Secondary Analysis of the MYMeals Cross-Sectional Study" Nutrients 15, no. 20: 4471. https://doi.org/10.3390/nu15204471
APA StyleHan, J. Y., Morris, K., Wellard-Cole, L., Davies, A., Rangan, A., & Allman-Farinelli, M. (2023). Snacking Behaviours of Australian Young Adults: Secondary Analysis of the MYMeals Cross-Sectional Study. Nutrients, 15(20), 4471. https://doi.org/10.3390/nu15204471