
Perinatal Plasma Carotenoids and Vitamin E Concentrations with Glycemia and Insulin Resistance in Women during and after Pregnancy

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
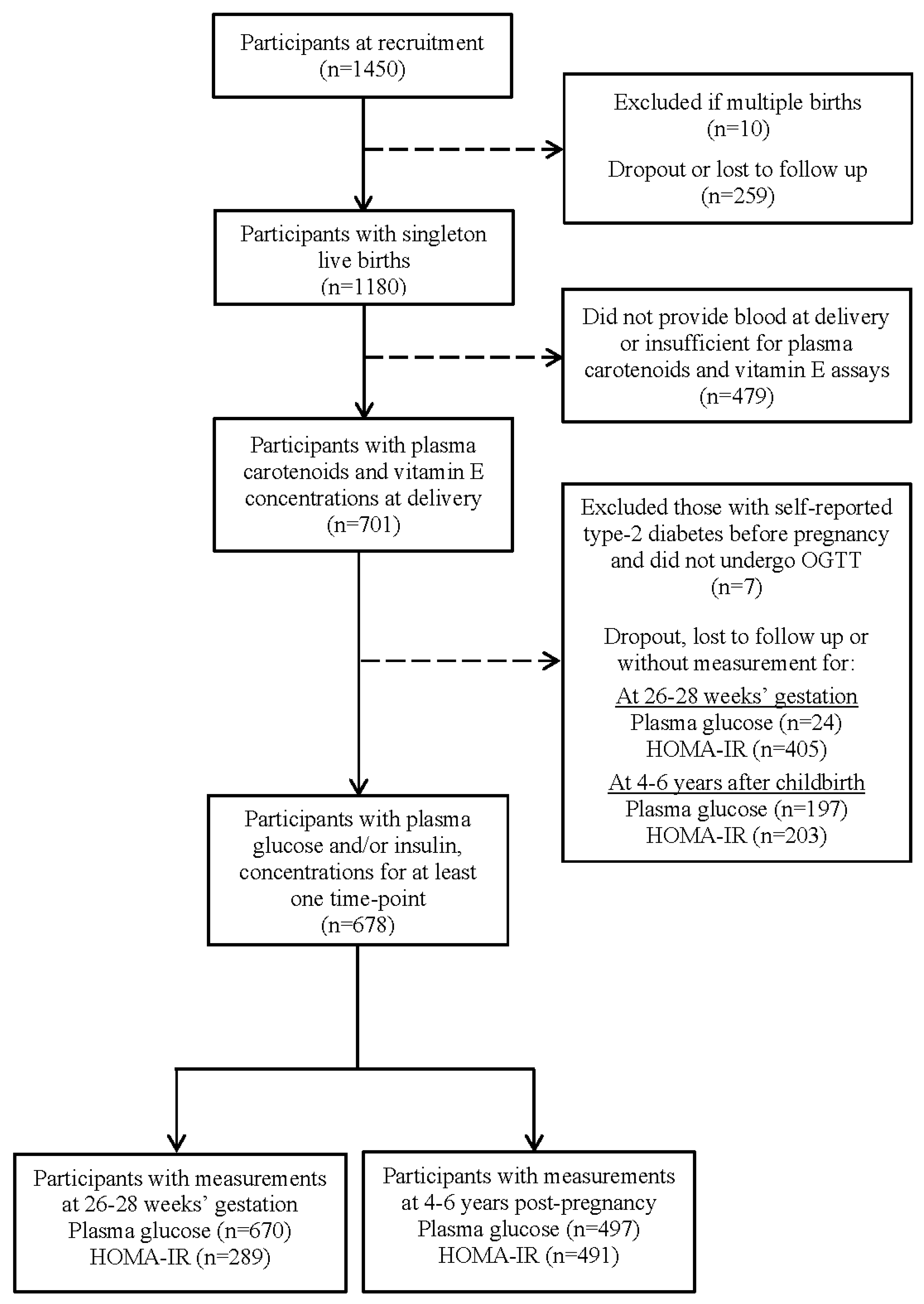
2.1. Study Sample
2.2. Plasma Concentrations of Carotenoids and E Vitamers
2.3. Plasma Glucose and Insulin Concentrations, GDM, and T2DM
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Study Sample Characteristics
3.2. Patterns of Carotenoid and E Vitamers
3.3. Carotenoid and E Vitamers with Gestational Plasma Glucose, HOMA-IR, and GDM
3.4. Carotenoid and E Vitamers with Post-Pregnancy Plasma Glucose, HOMA-IR, and T2DM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Myatt, L.; Cui, X. Oxidative stress in the placenta. Histochem. Cell Biol. 2004, 122, 369–382. [Google Scholar] [CrossRef]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The pathophysiology of gestational diabetes mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-W.; Soh, S.E.; Tint, M.-T.; Loy, S.L.; Yap, F.; Tan, K.H.; Lee, Y.S.; Shek, L.P.-C.; Godfrey, K.M.; Gluckman, P.D.; et al. Combined analysis of gestational diabetes and maternal weight status from pre-pregnancy through post-delivery in future development of type 2 diabetes. Sci. Rep. 2021, 11, 5021. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes: A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Chan, J.C.; Malik, V.; Jia, W.; Kadowaki, T.; Yajnik, C.S.; Yoon, K.H.; Hu, F.B. Diabetes in Asia: Epidemiology, risk factors, and pathophysiology. JAMA 2009, 301, 2129–2140. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019; Available online: https://www.diabetesatlas.org (accessed on 1 April 2021).
- Phelan, S. Windows of opportunity for lifestyle interventions to prevent gestational diabetes mellitus. Am. J. Perinatol. 2016, 33, 1291–1299. [Google Scholar] [CrossRef]
- Bohn, T. Carotenoids and markers of oxidative stress in human observational studies and intervention trials: Implications for chronic diseases. Antioxidants 2019, 8, 179. [Google Scholar] [CrossRef]
- Winklhofer-Roob, B.M.; Rock, E.; Ribalta, J.; Shmerling, D.H.; Roob, J.M. Effects of vitamin E and carotenoid status on oxidative stress in health and disease. Evidence obtained from human intervention studies. Mol. Asp. Med. 2003, 24, 391–402. [Google Scholar] [CrossRef]
- Cerf, M.E. Beta cell dysfunction and insulin resistance. Front. Endocrinol. 2013, 4, 37. [Google Scholar] [CrossRef]
- Hekmat, K.; Bagheri, R.; Abedi, P.; Tabesh, H. The relationship of fat soluble antioxidants with gestational diabetes in Iran: A case-control study. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obs. 2014, 27, 1676–1679. [Google Scholar] [CrossRef] [PubMed]
- Parast, V.M.; Paknahad, Z. Antioxidant status and risk of gestational diabetes mellitus: A case-control study. Clin. Nutr. Res. 2017, 6, 81–88. [Google Scholar] [CrossRef]
- Jacobs, D.R., Jr.; Gross, M.D.; Tapsell, L.C. Food synergy: An operational concept for understanding nutrition. Am. J. Clin. Nutr. 2009, 89, 1543S–1548S. [Google Scholar] [CrossRef] [PubMed]
- Soh, S.-E.; Tint, M.T.; Gluckman, P.D.; Godfrey, K.M.; Rifkin-Graboi, A.; Chan, Y.H.; Stünkel, W.; Holbrook, J.D.; Kwek, K.; Chong, Y.-S.; et al. Cohort profile: Growing Up in Singapore Towards healthy Outcomes (GUSTO) birth cohort study. Int. J. Epidemiol. 2014, 43, 1401–1409. [Google Scholar] [CrossRef]
- Lee, B.L.; Ong, C.N. Comprehensive high-performance liquid chromatographic method for the measurements of lipophilic antioxidants in human plasma. J. Chromatogr. A 2009, 1216, 3131–3137. [Google Scholar] [CrossRef]
- Burri, B.J.; Neidlinger, T.R.; Clifford, A.J. Serum carotenoid depletion follows first-order kinetics in healthy adult women fed naturally low carotenoid diets. J. Nutr. 2001, 131, 2096–2100. [Google Scholar] [CrossRef]
- Moran, N.E.; Cichon, M.J.; Riedl, K.M.; Grainger, E.M.; Schwartz, S.J.; Novotny, J.A.; Erdman, J.W., Jr.; Clinton, S.K. Compartmental and noncompartmental modeling of 13C-lycopene absorption, isomerization, and distribution kinetics in healthy adults. Am. J. Clin. Nutr. 2015, 102, 1436–1449. [Google Scholar] [CrossRef]
- Thurmann, P.A.; Schalch, W.; Aebischer, J.C.; Tenter, U.; Cohn, W. Plasma kinetics of lutein, zeaxanthin, and 3-dehydro-lutein after multiple oral doses of a lutein supplement. Am. J. Clin. Nutr. 2005, 82, 88–97. [Google Scholar] [CrossRef]
- Chuang, J.C.; Matel, H.D.; Nambiar, K.P.; Kim, S.-H.; Fadel, J.G.; Holstege, D.M.; Clifford, A.J. Quantitation of [5-CH3]-(2R, 4′R, 8′R)-α-Tocopherol in Humans. J. Nutr. 2011, 141, 1482–1488. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- WHO Consultation. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications: Report of A WHO Consultation; Part 1: Diagnosis and Classification of Diabetes Mellitus; WHO: Geneva, Switzerland, 1999. [Google Scholar]
- World Health Organisation (WHO). Classification of Diabetes Mellitus; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Hozawa, A.; Jacobs, D.R., Jr.; Steffes, M.W.; Gross, M.D.; Steffen, L.M.; Lee, D.H. Associations of serum carotenoid concentrations with the development of diabetes and with insulin concentration: Interaction with smoking: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am. J. Epidemiol. 2006, 163, 929–937. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Costacou, T.; King, I.; Zaccaro, D.J.; Bell, R.A.; Insulin Resistance Atherosclerosis Study (IRAS). Plasma and dietary vitamin E in relation to incidence of type 2 diabetes: The Insulin Resistance and Atherosclerosis Study (IRAS). Diabetes Care 2002, 25, 2172–2177. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.; Soh, S.E.; Loy, S.L.; Colega, M.; Kramer, M.S.; Chan, J.K.Y.; Tan, T.C.; Shek, L.P.C.; Yap, F.K.P.; Tan, K.H.; et al. Macronutrient composition and food groups associated with gestational weight gain: The GUSTO study. Eur. J. Nutr. 2019, 58, 1081–1094. [Google Scholar] [CrossRef] [PubMed]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Coyne, T.; Ibiebele, T.I.; Baade, P.D.; Dobson, A.; McClintock, C.; Dunn, S.; Leonard, D.; Shaw, J. Diabetes mellitus and serum carotenoids: Findings of a population-based study in Queensland, Australia. Am. J. Clin. Nutr. 2005, 82, 685–693. [Google Scholar] [CrossRef]
- Ylonen, K.; Alfthan, G.; Groop, L.; Saloranta, C.; Aro, A.; Virtanen, S.M. Dietary intakes and plasma concentrations of carotenoids and tocopherols in relation to glucose metabolism in subjects at high risk of type 2 diabetes: The Botnia Dietary Study. Am. J. Clin. Nutr. 2003, 77, 1434–1441. [Google Scholar] [CrossRef]
- Alperet, D.J.; Butler, L.M.; Koh, W.-P.; Yuan, J.-M.; van Dam, R.M. Influence of temperate, subtropical, and tropical fruit consumption on risk of type 2 diabetes in an Asian population. Am. J. Clin. Nutr. 2017, 105, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Burri, B.J.; La Frano, M.R.; Zhu, C. Absorption, metabolism, and functions of β-cryptoxanthin. Nutr. Rev. 2016, 74, 69–82. [Google Scholar] [CrossRef]
- The HAPO Study Cooperative Research Group. Hyperglycemia and adverse pregnancy outcomes. New Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef]
- Lai, J.S.; Cai, S.; Lee, B.L.; Godfrey, K.M.; Gluckman, P.D.; Shek, L.P.; Yap, F.; Tan, K.H.; Chong, Y.S.; Ong, C.N.; et al. Higher maternal plasma β-cryptoxanthin concentration is associated with better cognitive and motor development in offspring at 2 years of age. Eur. J. Nutr. 2021, 60, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.; Yuan, W.L.; Ong, C.N.; Tan, K.H.; Yap, F.; Chong, Y.S.; Gluckman, P.D.; Godfrey, K.M.; Lee, Y.S.; Chan, J.K.Y.; et al. Perinatal plasma carotenoid and vitamin E concentrations with maternal blood pressure during and after pregnancy. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2811–2821. [Google Scholar] [CrossRef] [PubMed]
- Ha, V.; Bonner, A.J.; Jadoo, J.K.; Beyene, J.; Anand, S.S.; de Souza, R.J. The effects of various diets on glycemic outcomes during pregnancy: A systematic review and network meta-analysis. PLoS ONE 2017, 12, e0182095. [Google Scholar] [CrossRef] [PubMed]
- Bates, C.J.; Mishra, G.D.; Prentice, A. γ-Tocopherol as a possible marker for nutrition-related risk: Results from four National Diet and Nutrition Surveys in Britain. Br. J. Nutr. 2007, 92, 137–150. [Google Scholar] [CrossRef]
- Lowe, L.P.; Metzger, B.E.; Lowe, W.L., Jr.; Dyer, A.R.; McDade, T.W.; McIntyre, H.D.; Group, H.S.C.R. Inflammatory mediators and glucose in pregnancy: Results from a subset of the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. J. Clin. Endocrinol. Metab. 2010, 95, 5427–5434. [Google Scholar] [CrossRef]
- McLaughlin, P.J.; Weihrauch, J.L. Vitamin E content of foods. J. Am. Diet. Assoc. 1979, 75, 647–665. [Google Scholar] [CrossRef]
- Zhuang, P.; Mao, L.; Wu, F.; Wang, J.; Jiao, J.; Zhang, Y. Cooking oil consumption is positively associated with risk of type 2 diabetes in a Chinese nationwide cohort study. J. Nutr. 2020, 150, 1799–1807. [Google Scholar] [CrossRef]
- Brown, T.J.; Brainard, J.; Song, F.; Wang, X.; Abdelhamid, A.; Hooper, L. Omega-3, omega-6, and total dietary polyunsaturated fat for prevention and treatment of type 2 diabetes mellitus: Systematic review and meta-analysis of randomised controlled trials. BMJ 2019, 366, l4697. [Google Scholar] [CrossRef]
- Oostenbrug, G.S.; Mensink, R.P.; Al, M.D.; van Houwelingen, A.C.; Hornstra, G. Maternal and neonatal plasma antioxidant levels in normal pregnancy, and the relationship with fatty acid unsaturation. Br. J. Nutr. 1998, 80, 67–73. [Google Scholar] [CrossRef]
- Herrera, E.; Ortega, H.; Alvino, G.; Giovannini, N.; Amusquivar, E.; Cetin, I. Relationship between plasma fatty acid profile and antioxidant vitamins during normal pregnancy. Eur. J. Clin. Nutr. 2004, 58, 1231–1238. [Google Scholar] [CrossRef]
- Dalrymple, K.V.; Vogel, C.; Godfrey, K.M.; Baird, J.; Harvey, N.C.; Hanson, M.A.; Cooper, C.; Inskip, H.M.; Crozier, S.R. Longitudinal dietary trajectories from preconception to mid-childhood in women and children in the Southampton Women’s Survey and their relation to offspring adiposity: A group-based trajectory modelling approach. Int. J. Obes. 2022, 46, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Cucó, G.; Fernández-Ballart, J.; Sala, J.; Viladrich, C.; Iranzo, R.; Vila, J.; Arija, V. Dietary patterns and associated lifestyles in preconception, pregnancy and postpartum. Eur. J. Clin. Nutr. 2006, 60, 364–371. [Google Scholar] [CrossRef]
- Mejía, L.A.; Pineda, O.; Noriega, J.F.; Benítez, J.; Falla, G. Significance of postprandial blood concentrations of retinol, retinol-binding protein, and carotenoids when assessing the vitamin A status of children. Am. J. Clin. Nutr. 1984, 39, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.D.; Rose, A.; Craft, N.; Seidel, K.E.; Smith, J.C. Concentrations of carotenoids, retinol, and tocopherol in plasma, in response to ingestion of a meal. Clin. Chem. 1989, 35, 310–312. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | n (%) |
|---|---|
| Pre-pregnancy overweight/obese (BMI ≥ 23.0 kg/m2), n (%) | 246 (39.6) |
| During pregnancy | |
| Age at delivery, year, mean ± SD | 31.4 ± 5.0 |
| Ethnicity, n (%) | |
| Chinese | 400 (59.0) |
| Malay | 158 (23.3) |
| Indian | 120 (17.7) |
| Highest education, n (%) | |
| ≤Secondary | 203 (30.2) |
| Post-secondary | 218 (32.4) |
| Tertiary | 252 (37.4) |
| Parity, n (%) | |
| Nulliparous | 297 (43.8) |
| Primi-/Multiparous | 381 (56.2) |
| Smoking, n (%) | 13 (1.9) |
| Alcohol intake, n (%) | 15 (2.3) |
| Moderate–vigorous physical activity, n (%) | |
| Never | 472 (70.0) |
| <150 min/week | 135 (20.0) |
| ≥150 min/week | 67 (9.9) |
| Total fat intake, g/day, mean ± SD | 69.6 ± 29.1 |
| Intake of supplements, n (%), containing | |
| Vitamin A/carotenoids | 462 (73.5) |
| Vitamin E | 169 (26.8) |
| Plasma carotenoids concentrations, μmol/L, mean ± SD | |
| α-Carotene | 0.12 ± 0.09 |
| β-Carotene | 0.45 ± 0.36 |
| β-Cryptoxanthin | 0.45 ± 0.33 |
| Lutein | 0.46 ± 0.26 |
| Zeaxanthin | 0.30 ± 0.12 |
| Lycopene | 0.23 ± 0.13 |
| Plasma vitamin E concentrations, μmol/L, mean ± SD | |
| α-tocopherol | 52.45 ± 13.09 |
| γ-tocopherol | 1.47 ± 0.77 |
| δ-tocopherol | 0.47 ± 0.29 |
| Family history of diabetes mellitus, n (%) | 204 (30.5) |
| Fasting plasma glucose, mmol/L, mean ± SD | 4.35 ± 0.49 |
| 2 h plasma glucose, mmol/L, mean ± SD | 6.56 ± 1.54 |
| HOMA-IR, median (IQR) | 1.18 (0.80, 1.70) |
| Gestational diabetes, n (%) | 130 (19.4 b) |
| At 4–6 years post-pregnancy | |
| Fasting plasma glucose, mmol/L, mean ± SD | 4.94 ± 0.73 |
| 2 h plasma glucose, mmol/L, mean ± SD | 6.36 ± 1.89 |
| HOMA-IR, median (IQR) | 1.22 (0.81, 1.97) |
| Type 2 diabetes, n (%) | 11 (2.2 c) |
| Carotenoid/E Vitamers | Carotenoid Pattern 1 (CP1) | Vitamin E (VE) Pattern | Carotenoid Pattern 2 (CP2) |
|---|---|---|---|
| α-carotene | 0.56 | ||
| β-carotene | 0.51 | ||
| lutein | 0.48 | ||
| γ-tocopherol | 0.61 | ||
| δ-tocopherol | 0.60 | ||
| α-tocopherol | 0.42 | ||
| zeaxanthin | 0.59 | ||
| lycopene | 0.55 | ||
| β-cryptoxanthin | 0.46 | ||
| % variance explained by each pattern | 21.9 | 20.5 | 17.1 |
| Cumulative % of variance explained | 21.9 | 42.4 | 39 |
| Carotenoid Pattern 1 (CP1) | p | Vitamin E (VE) Pattern | p | Carotenoid Pattern 2 (CP2) | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Tertile 1 | Tertile 3 | Tertile 1 | Tertile 3 | Tertile 1 | Tertile 3 | ||||
| Total fruit intake, g/day, mean ± SD | 63.7 ± 119.4 | 163.1 ± 189.7 | <0.001 | 122.1 ± 171.1 | 104.2 ± 165.4 | 0.091 | 99.0 ± 144.6 | 127.6 ± 185.9 | 0.379 |
| Total vegetables intake, g/day, mean ± SD | 56.0 ± 64.2 | 80.6 ± 74.9 | 0.001 | 66.7 ± 69.5 | 67.6 ± 70.6 | 0.095 | 59.0 ± 67.8 | 73.7 ± 69.7 | 0.029 |
| Total fat intake, g/day, mean ± SD | 67.3 ± 29.3 | 72.5 ± 28.2 | 0.157 | 68.3 ± 30.6 | 73.8 ± 28.9 | 0.020 | 68.1 ± 26.7 | 71.4 ± 30.5 | 0.574 |
| Supplements containing Vitamin A, n (%) | 167 (75.9) | 146 (70.9) | 0.499 | 164 (76.3) | 150 (69.4) | 0.233 | 161 (75.2) | 156 (74.3) | 0.599 |
| Supplements containing Vitamin E, n (%) | 49 (22.3) | 65 (31.6) | 0.097 | 63 (29.3) | 47 (21.8) | 0.107 | 61 (28.5) | 52 (24.8) | 0.669 |
| Fasting Glucose (n = 670) | 2 h Glucose (n = 670) | HOMA-IR (n = 289) | GDM (n = 130) vs. non-GDM (n = 540) | |||||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | OR (95% CI) | p | |
| Carotenoids d | ||||||||
| Individual concentrations | ||||||||
| α-Carotene | −0.05 (−0.09, −0.01) | 0.005 | −0.13 (−0.24, 0.01) | 0.05 | −0.05 (−0.41, 0.32) | 0.18 | 0.89 (0.71, 1.12) | 0.33 |
| β-Carotene | −0.06 (−0.08, −0.01) | 0.018 | −0.03 (−0.15, 0.10) | 0.68 | −0.12 (−0.46, 0.01) | 0.07 | 1.11 (0.90, 1.35) | 0.32 |
| Lutein | −0.05 (−0.09, −0.01) | 0.019 | 0.02 (−0.11, 0.15) | 0.76 | −0.01 (−0.26, 0.24) | 0.95 | 1.07 (0.85, 1.34) | 0.56 |
| CP 1 | −0.06 (−0.10, −0.02) | 0.004 | −0.04 (−0.17, 0.08) | 0.50 | −0.17 (−0.82, 0.01) | 0.06 | 1.05 (0.84, 1.33) | 0.65 |
| Individual concentrations | ||||||||
| Zeaxanthin | −0.02 (−0.06, 0.01) | 0.22 | −0.08 (−0.20, 0.03) | 0.17 | −0.08 (−0.35, 0.12) | 0.10 | 0.94 (0.74, 1.18) | 0.59 |
| Lycopene | −0.02 (−0.05, 0.02) | 0.42 | −0.05 (−0.16, 0.06) | 0.39 | 0.03 (−0.08, 0.15) | 0.58 | 1.09 (0.89, 1.33) | 0.41 |
| β-Cryptoxanthin | −0.04 (−0.05, 0.01) | 0.05 | 0.02 (−0.10, 0.13) | 0.80 | −0.09 (−0.72, 0.01) | 0.06 | 1.01 (0.81, 1.26) | 0.91 |
| CP 2 | −0.04 (−0.06, 0.01) | 0.05 | −0.07 (−0.19, 0.05) | 0.23 | −0.01 (−0.43, 0.20) | 0.11 | 1.02 (0.82, 1.27) | 0.86 |
| Vitamin E e | ||||||||
| Individual concentrations | ||||||||
| γ-Tocopherol | 0.05 (0.02, 0.09) | 0.004 | 0.10 (0.02, 0.17) | 0.010 | 0.09 (−0.24, 0.43) | 0.57 | 1.20 (1.00, 1.50) | 0.06 |
| δ-Tocopherol | 0.05 (0.02, 0.09) | 0.006 | 0.07 (−0.01, 0.15) | 0.07 | 0.03 (−0.34, 0.23) | 0.11 | 1.22 (0.99, 1.49) | 0.06 |
| α-Tocopherol | −0.001 (−0.04, 0.04) | 0.94 | 0.02 (−0.06, 0.10) | 0.55 | −0.05 (−0.58, 0.02) | 0.07 | 1.21 (0.99, 1.49) | 0.07 |
| VE pattern | 0.05 (0.01, 0.08) | 0.015 | 0.08 (0.01, 0.16) | 0.033 | 0.03 (−0.26, 0.34) | 0.80 | 1.19 (0.99, 1.58) | 0.06 |
| Fasting Glucose (n = 497) | 2 h Glucose (n = 497) | HOMA-IR (n = 491) | T2DM (n = 11) vs. non-T2DM (n = 486) | |||||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | OR (95% CI) | p | |
| Carotenoids d | ||||||||
| Individual concentrations | ||||||||
| α-carotene | −0.02 (−0.09, 0.05) | 0.60 | −0.03 (−0.21, 0.16) | 0.77 | −0.06 (−0.13, 0.01) | 0.08 | 0.29 (0.07, 1.20) | 0.09 |
| β-carotene | −0.03 (−0.10, 0.04) | 0.40 | −0.04 (−0.22, 0.14) | 0.68 | −0.05 (−0.07, −0.04) | 0.001 | 0.41 (0.09, 1.78) | 0.23 |
| Lutein | −0.01 (−0.10, 0.07) | 0.76 | 0.01 (−0.20, 0.21) | 0.94 | −0.05 (−0.11, 0.01) | 0.11 | 0.53 (0.17, 1.65) | 0.28 |
| CP 1 | −0.02 (−0.10, 0.06) | 0.64 | −0.08 (−0.27, 0.12) | 0.42 | −0.11 (−0.15, −0.08) | 0.001 | 0.32 (0.10, 1.00) | 0.05 |
| Individual concentrations | ||||||||
| Zeaxanthin | −0.04 (−0.07, 0.01) | 0.06 | −0.17 (−0.33, 0.01) | 0.06 | −0.07 (−0.14, 0.01) | 0.06 | 0.35 (0.19, 1.31) | 0.06 |
| Lycopene | −0.04 (−0.12, 0.06) | 0.56 | 0.01 (−0.19, 0.21) | 0.91 | −0.07 (−0.15, 0.01) | 0.10 | 0.81 (0.38, 1.74) | 0.60 |
| β-cryptoxanthin | −0.02 (−0.10, 0.05) | 0.55 | −0.10 (−0.28, 0.07) | 0.25 | −0.07 (−0.13, −0.02) | 0.009 | 0.36 (0.10, 1.26) | 0.11 |
| CP 2 | −0.04 (−0.08, 0.01) | 0.06 | −0.08 (−0.26, 0.11) | 0.41 | −0.09 (−0.16, 0.02) | 0.10 | 0.42 (0.17, 1.02) | 0.06 |
| Vitamin E e | ||||||||
| Individual concentrations | ||||||||
| γ-Tocopherol | 0.21 (0.09, 0.33) | 0.001 | 0.17 (−0.01, 0.34) | 0.06 | −0.02 (−0.11, 0.06) | 0.62 | 1.16 (0.65, 2.10) | 0.62 |
| δ-Tocopherol | 0.15 (0.03, 0.27) | 0.015 | 0.26 (0.08, 0.44) | 0.006 | 0.01 (−0.06, 0.15) | 0.34 | 1.47 (0.85, 2.54) | 0.17 |
| α-Tocopherol | 0.10 (−0.02, 0.22) | 0.10 | 0.08 (−0.12, 0.27) | 0.43 | 0.05 (−0.04, 0.15) | 0.24 | 0.73 (0.35, 1.50) | 0.39 |
| VE pattern | 0.19 (0.07, 0.31) | 0.002 | 0.24 (0.06, 0.42) | 0.009 | 0.10 (−0.03, 0.24) | 0.13 | 1.25 (0.67, 2.34) | 0.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, J.S.; Godfrey, K.M.; Ong, C.N.; Tan, K.H.; Yap, F.; Chong, Y.S.; Chan, J.K.Y.; Chan, S.-Y.; Chong, M.F.-F. Perinatal Plasma Carotenoids and Vitamin E Concentrations with Glycemia and Insulin Resistance in Women during and after Pregnancy. Nutrients 2023, 15, 4421. https://doi.org/10.3390/nu15204421
Lai JS, Godfrey KM, Ong CN, Tan KH, Yap F, Chong YS, Chan JKY, Chan S-Y, Chong MF-F. Perinatal Plasma Carotenoids and Vitamin E Concentrations with Glycemia and Insulin Resistance in Women during and after Pregnancy. Nutrients. 2023; 15(20):4421. https://doi.org/10.3390/nu15204421
Chicago/Turabian StyleLai, Jun S., Keith M. Godfrey, Choon Nam Ong, Kok Hian Tan, Fabian Yap, Yap Seng Chong, Jerry K. Y. Chan, Shiao-Yng Chan, and Mary F.-F. Chong. 2023. "Perinatal Plasma Carotenoids and Vitamin E Concentrations with Glycemia and Insulin Resistance in Women during and after Pregnancy" Nutrients 15, no. 20: 4421. https://doi.org/10.3390/nu15204421
APA StyleLai, J. S., Godfrey, K. M., Ong, C. N., Tan, K. H., Yap, F., Chong, Y. S., Chan, J. K. Y., Chan, S.-Y., & Chong, M. F.-F. (2023). Perinatal Plasma Carotenoids and Vitamin E Concentrations with Glycemia and Insulin Resistance in Women during and after Pregnancy. Nutrients, 15(20), 4421. https://doi.org/10.3390/nu15204421