

Lower Intakes of Key Nutrients Are Associated with More School and Workplace Absenteeism in US Children and Adults: A Cross-Sectional Study of NHANES 2003–2008


Abstract
:1. Introduction
2. Materials and Methods
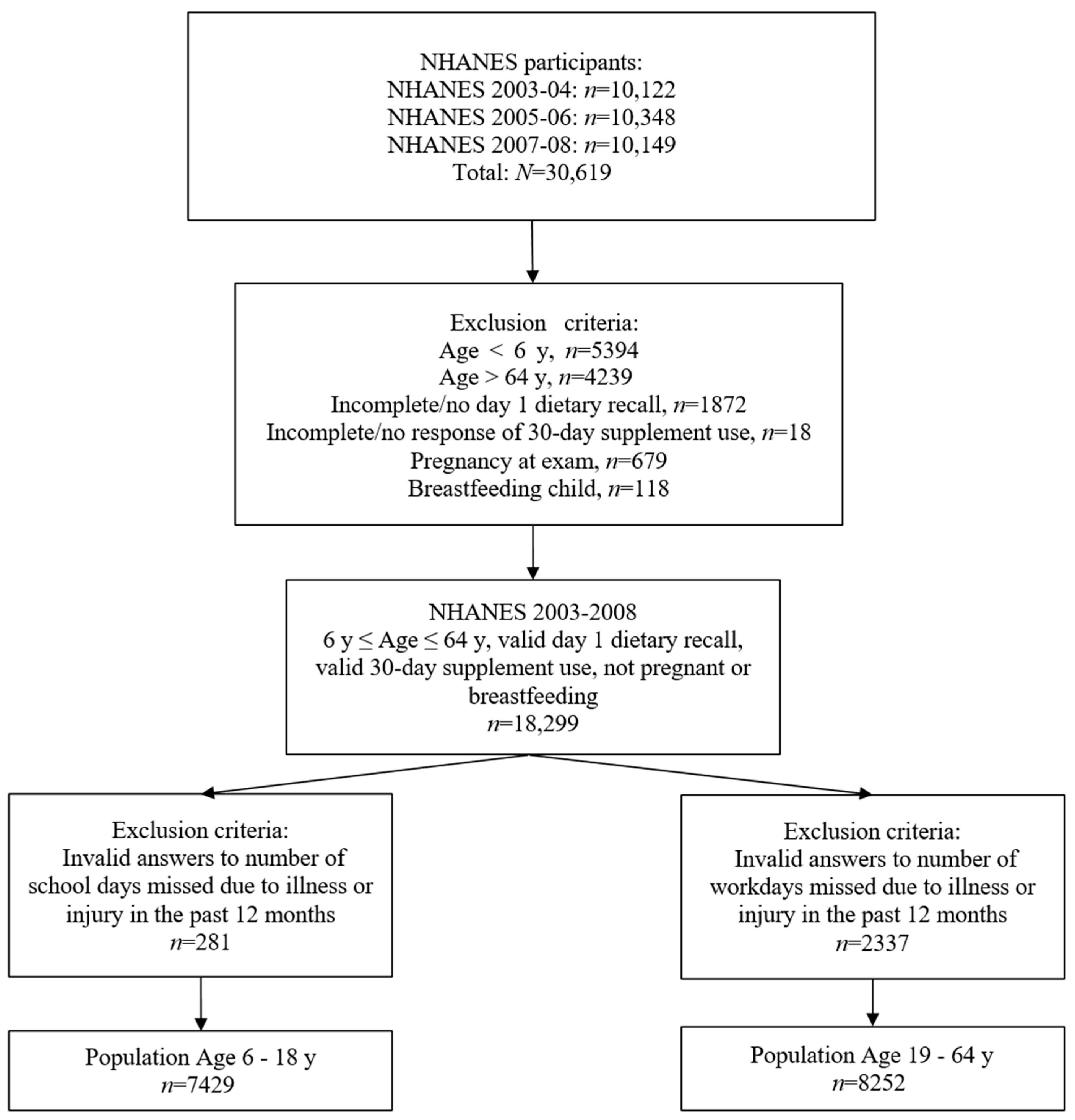
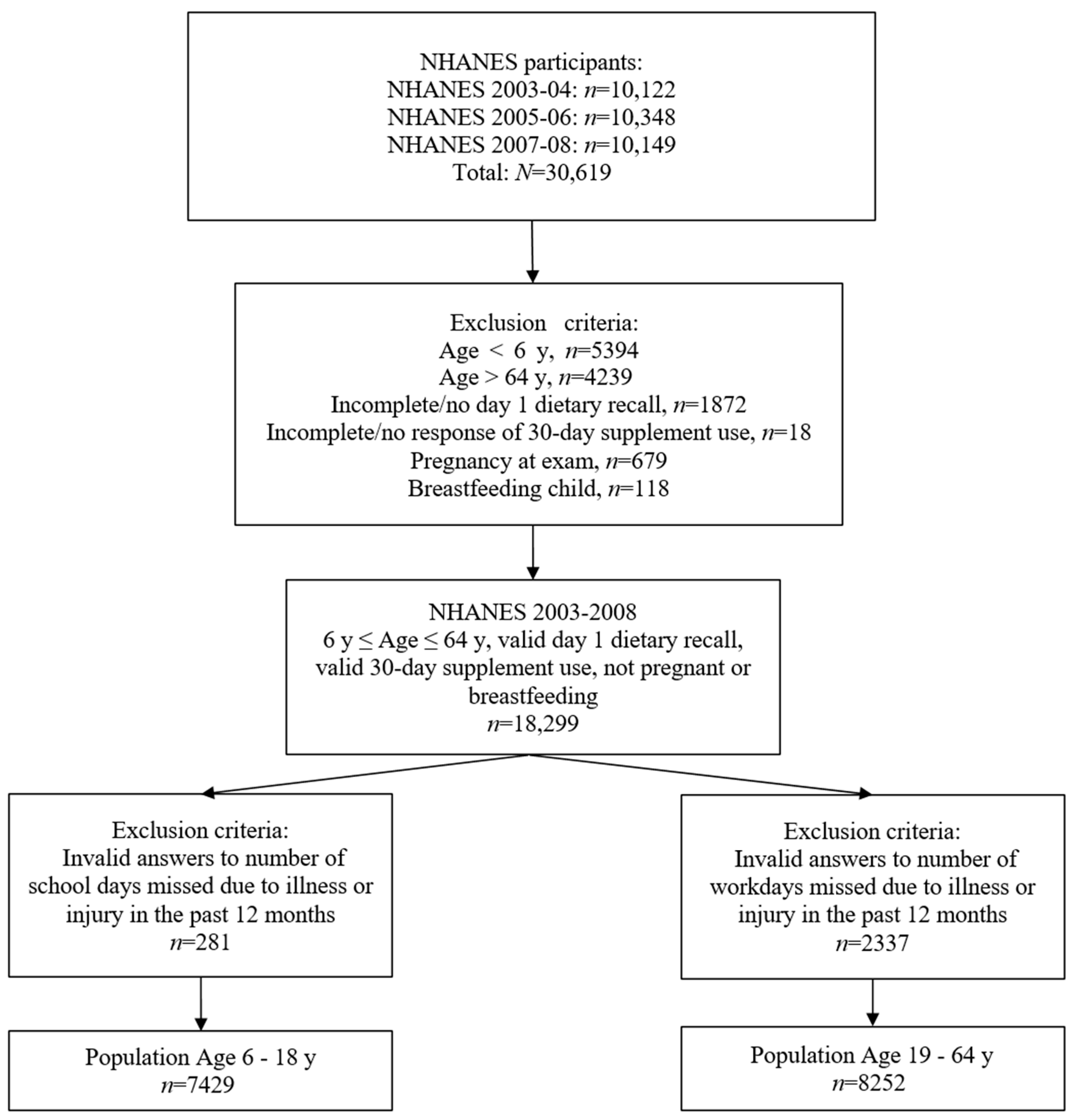
2.1. Database and Study Population
2.2. Absenteeism Data
2.3. Dietary Intake Data
2.4. Nutrient Biomarkers
2.5. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Nutrient Intake
3.3. Nutrient Biomarkers
4. Discussion
4.1. Absenteeism and Macronutrient Status
4.2. Absenteeism and Micronutrient Status
4.3. Absenteeism and Supplement Intake
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gottfried, M.A. Chronic absenteeism and its effects on students’ academic and socioemotional outcomes. J. Educ. Stud. Placed Risk 2014, 19, 53–75. [Google Scholar] [CrossRef]
- Ansari, A.; Gottfried, M.A. The grade-level and cumulative outcomes of absenteeism. Child Dev. 2021, 92, e548–e564. [Google Scholar] [CrossRef] [PubMed]
- Ansari, A.; Pianta, R.C. School absenteeism in the first decade of education and outcomes in adolescence. J. Sch. Psychol. 2019, 76, 48–61. [Google Scholar] [CrossRef]
- Mitchell, R.J.; Bates, P. Measuring health-related productivity loss. Popul. Health Manag. 2011, 14, 93–98. [Google Scholar] [CrossRef]
- Loeppke, R.; Taitel, M.; Haufle, V.; Parry, T.; Kessler, R.C.; Jinnett, K. Health and productivity as a business strategy: A multiemployer study. J. Occup. Environ. Med. 2009, 51, 411–428. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.W.; Diamond-Myrsten, S.; Rollins, L.K. School absenteeism in children and adolescents. Am. Fam. Physician 2018, 98, 738–744. [Google Scholar]
- Gubbels, J.; van der Put, C.E.; Assink, M. Risk factors for school absenteeism and dropout: A meta-analytic review. J. Youth Adolesc. 2019, 48, 1637–1667. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.M.; Aldana, S.G.; Pope, J.E.; Anderson, D.R.; Coberley, C.R.; Grossmeier, J.J.; Whitmer, R.W. Self-rated job performance and absenteeism according to employee engagement, health behaviors, and physical health. J. Occup. Environ. Med. 2013, 55, 10–18. [Google Scholar] [CrossRef]
- Gohar, B.; Lariviere, M.; Lightfoot, N.; Lariviere, C.; Wenghofer, E.; Nowrouzi-Kia, B. Demographic, Lifestyle, and Physical Health Predictors of Sickness Absenteeism in Nursing: A Meta-Analysis. Saf. Health Work 2021, 12, 536–543. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Frith, E. Accelerometer-assessed physical activity and school absenteeism due to illness or injury among children and adolescents: NHANES 2003 to 2006. Am. J. Health Promot. 2018, 32, 571–577. [Google Scholar] [CrossRef]
- Losina, E.; Yang, H.Y.; Deshpande, B.R.; Katz, J.N.; Collins, J.E. Physical activity and unplanned illness-related work absenteeism: Data from an employee wellness program. PLoS ONE 2017, 12, e0176872. [Google Scholar] [CrossRef] [PubMed]
- Andreyeva, T.; Luedicke, J.; Wang, Y.C. State-level estimates of obesity-attributable costs of absenteeism. J. Occup. Environ. Med./Am. Coll. Occup. Environ. Med. 2014, 56, 1120. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Raychowdhury, S.; Tedders, S.H.; Lyn, R.; Fede, L.-D.; Zhang, J. Association between increased BMI and severe school absenteeism among US children and adolescents: Findings from a national survey, 2005–2008. Int. J. Obes. 2012, 36, 517–523. [Google Scholar] [CrossRef]
- Kristjansson, B.; Petticrew, M.; MacDonald, B.; Krasevec, J.; Janzen, L.; Greenhalgh, T.; Wells, G.A.; MacGowan, J.; Farmer, A.P.; Shea, B. School feeding for improving the physical and psychosocial health of disadvantaged students. Cochrane Database Syst. Rev. 2007, 2, 1–189. [Google Scholar] [CrossRef]
- Kirksey, J.J.; Gottfried, M.A. The effect of serving “breakfast after-the-Bell” meals on school absenteeism: Comparing results from regression discontinuity designs. Educ. Eval. Policy Anal. 2021, 43, 305–328. [Google Scholar] [CrossRef]
- Drewnowski, A. Impact of nutrition interventions and dietary nutrient density on productivity in the workplace. Nutr. Rev. 2020, 78, 215–224. [Google Scholar] [CrossRef]
- Rongen, A.; Robroek, S.J.; van Lenthe, F.J.; Burdorf, A. Workplace health promotion: A meta-analysis of effectiveness. Am. J. Prev. Med. 2013, 44, 406–415. [Google Scholar] [CrossRef]
- Jensen, J.D. Can worksite nutritional interventions improve productivity and firm profitability? A literature review. Perspect. Public Health 2011, 131, 184–192. [Google Scholar] [CrossRef]
- Peltz, A.; Garg, A. Food insecurity and health care use. Pediatrics 2019, 144, e20190347. [Google Scholar] [CrossRef]
- Walingo, M.K.; Musamali, B. Nutrient intake and nutritional status indicators of participant and nonparticipant pupils of a parent-supported school lunch program in Kenya. J. Nutr. Educ. Behav. 2008, 40, 298–304. [Google Scholar] [CrossRef]
- Jacoby, E.R.; Cueto, S.; Pollitt, E. When science and politics listen to each other: Good prospects from a new school breakfast program in Peru. Am. J. Clin. Nutr. 1998, 67, 795S–797S. [Google Scholar] [CrossRef]
- Duong, M.-C.; Mora-Plazas, M.; Marín, C.; Villamor, E. Vitamin B-12 deficiency in children is associated with grade repetition and school absenteeism, independent of folate, iron, zinc, or vitamin a status biomarkers. J. Nutr. 2015, 145, 1541–1548. [Google Scholar] [CrossRef]
- Fitzgerald, S.; Kirby, A.; Murphy, A.; Geaney, F. Obesity, diet quality and absenteeism in a working population. Public Health Nutr. 2016, 19, 3287–3295. [Google Scholar] [CrossRef] [PubMed]
- Fulton, S.L.; McKinley, M.C.; Young, I.S.; Cardwell, C.R.; Woodside, J.V. The effect of increasing fruit and vegetable consumption on overall diet: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2016, 56, 802–816. [Google Scholar] [CrossRef]
- Panjwani, A.A.; Cowan, A.E.; Jun, S.; Bailey, R.L. Trends in Nutrient-and Non-Nutrient–Containing Dietary Supplement Use among US Children from 1999 to 2016. J. Pediatr. 2021, 231, 131–140. [Google Scholar] [CrossRef]
- Council for Responsible Nutrition. CRN Reveals Initial Data from 2021 Consumer Survey on Dietary Supplements. Available online: https://www.crnusa.org/newsroom/crn-reveals-initial-data-2021-consumer-survey-dietary-supplements (accessed on 24 February 2023).
- National Center for Health Statistics. National Health and Nutrition Examination Survey, NHANES 2003–2004; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?BeginYear=2003 (accessed on 29 April 2022).
- National Center for Health Statistics. National Health and Nutrition Examination Survey, NHANES 2005-2006; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?BeginYear=2005 (accessed on 29 April 2022).
- National Center for Health Statistics. National Health and Nutrition Examination Survey, NHANES 2007–2008; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?BeginYear=2007 (accessed on 29 April 2022).
- Curtin, L.R.; Mohadjer, L.K.; Dohrmann, S.M.; Kruszon-Moran, D.; Mirel, L.B.; Carroll, M.D.; Hirsch, R.; Burt, V.L.; Johnson, C.L. National Health and Nutrition Examination Survey: Sample design, 2007–2010. Vital Health Stat. 2013, 160, 1–23. [Google Scholar]
- Zipf, G.; Chiappa, M.; Porter, K.S.; Ostchega, Y.; Lewis, B.G.; Dostal, J. National health and nutrition examination survey: Plan and operations, 1999–2010. Vital. Health Stat. 2013, 1, 1–37. [Google Scholar]
- National Center for Health Statistics. NHANES 2003-2004 Questionnaire Data Overview; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/overviewquex.aspx?BeginYear=2003 (accessed on 6 September 2023).
- National Center for Health Statistics. NHANES 2005-2006 Questionnaire Data Overview; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/overviewquex.aspx?BeginYear=2005 (accessed on 6 September 2023).
- National Center for Health Statistics. NHANES 2007-2008 Questionnaire Data Overview; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/overviewquex.aspx?BeginYear=2007 (accessed on 6 September 2023).
- Blanton, C.A.; Moshfegh, A.J.; Baer, D.J.; Kretsch, M.J. The USDA Automated Multiple-Pass Method accurately estimates group total energy and nutrient intake. J. Nutr. 2006, 136, 2594–2599. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES): MEC In-Person Dietary Interviewers Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2007-2008/manuals/manual_dietarymec.pdf (accessed on 5 September 2023).
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES): Phone Follow-up Dietary Interviewer Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2007-2008/manuals/manual_dietarypfu.pdf (accessed on 5 September 2023).
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES): MEC In-Person Dietary Interviewers Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2005-2006/manuals/DIETARY_MEC.pdf (accessed on 5 September 2023).
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES): Phone Follow-up Dietary Interviewer Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2005-2006/manuals/DIETARY_PFU.pdf (accessed on 5 September 2023).
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES): MEC In-Person Dietary Interviewers Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2003-2004/manuals/DIETARY_MEC.pdf (accessed on 5 September 2023).
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES): Phone Follow-up Dietary Interviewer Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2003-2004/manuals/DIETARY_PFU.pdf (accessed on 5 September 2023).
- World Health Organization. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005: WHO Global Database on Vitamin A Deficiency; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Pfeiffer, C.M.; Lacher, D.A.; Schleicher, R.L.; Johnson, C.L.; Yetley, E.A. Challenges and lessons learned in generating and interpreting NHANES nutritional biomarker data. Adv. Nutr. 2017, 8, 290–307. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US). Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and its Panel on Folate, Other B Vitamins, and Choline. In Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B(6), Folate, Vitamin B(12), Pantothenic Acid, Biotin, and Choline; National Academies Press (US), National Academy of Sciences: Washington, DC, USA, 1998. [Google Scholar]
- Allen, L.H.; Miller, J.W.; De Groot, L.; Rosenberg, I.H.; Smith, A.D.; Refsum, H.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND): Vitamin B-12 review. J. Nutr. 2018, 148, 1995S–2027S. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Carmel, R.; Green, R.; Pfeiffer, C.M.; Cogswell, M.E.; Osterloh, J.D.; Sempos, C.T.; Yetley, E.A. Monitoring of vitamin B-12 nutritional status in the United States by using plasma methylmalonic acid and serum vitamin B-12. Am. J. Clin. Nutr. 2011, 94, 552–561. [Google Scholar] [CrossRef]
- Lynch, S.; Pfeiffer, C.M.; Georgieff, M.K.; Brittenham, G.; Fairweather-Tait, S.; Hurrell, R.F.; McArdle, H.J.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)—Iron Review. J. Nutr. 2018, 148, 1001S–1067S. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Serum Ferritin Concentrations for the Assessment of Iron Status and Iron Deficiency in Populations; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Pfeiffer, C.M.; Looker, A.C. Laboratory methodologies for indicators of iron status: Strengths, limitations, and analytical challenges. Am. J. Clin. Nutr. 2017, 106, 1606S–1614S. [Google Scholar] [CrossRef]
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Rohner, F.; Zimmermann, M.; Jooste, P.; Pandav, C.; Caldwell, K.; Raghavan, R.; Raiten, D.J. Biomarkers of nutrition for development—Iodine review. J. Nutr. 2014, 144, 1322S–1342S. [Google Scholar] [CrossRef]
- National Center for Health Statistics. NHANES 2007-2008: Ferritin Data Documentation, Codebook, and Frequencies. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2007-2008/FERTIN_E.htm (accessed on 25 July 2022).
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef]
- Lohner, S.; Jakobik, V.; Mihályi, K.; Soldi, S.; Vasileiadis, S.; Theis, S.; Sailer, M.; Sieland, C.; Berényi, K.; Boehm, G.; et al. Inulin-Type Fructan Supplementation of 3- to 6-Year-Old Children Is Associated with Higher Fecal Bifidobacterium Concentrations and Fewer Febrile Episodes Requiring Medical Attention. J. Nutr. 2018, 148, 1300–1308. [Google Scholar] [CrossRef]
- Lyon, P.; Strippoli, V.; Fang, B.; Cimmino, L. B vitamins and one-carbon metabolism: Implications in human health and disease. Nutrients 2020, 12, 2867. [Google Scholar] [CrossRef] [PubMed]
- Ducker, G.S.; Rabinowitz, J.D. One-carbon metabolism in health and disease. Cell Metab. 2017, 25, 27–42. [Google Scholar] [CrossRef]
- Tamura, J.; Kubota, K.; Murakami, H.; Sawamura, M.; Matsushima, T.; Tamura, T.; Saitoh, T.; Kurabayshi, H.; Naruse, T. Immunomodulation by vitamin B12: Augmentation of CD8+ T lymphocytes and natural killer (NK) cell activity in vitamin B12-deficient patients by methyl-B12 treatment. Clin. Exp. Immunol. 1999, 116, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Gombart, A.F.; Pierre, A.; Maggini, S. A review of micronutrients and the immune system–working in harmony to reduce the risk of infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef]
- Maggini, S.; Beveridge, S.; Sorbara, P.; Senatore, G. Feeding the immune system: The role of micronutrients in restoring resistance to infections. CAB Rev. Perspect. Agric. Vet. Sci. Nutr. Nat. Resour. 2008, 3, 1–21. [Google Scholar] [CrossRef]
- Wu, Y.; Li, S.; Wang, W.; Zhang, D. Associations of dietary B vitamins intakes with depression in adults. Int. J. Vitam. Nutr. Res. 2023, 93, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Esnafoglu, E.; Ozturan, D.D. The relationship of severity of depression with homocysteine, folate, vitamin B12, and vitamin D levels in children and adolescents. Child Adolesc. Ment. Health 2020, 25, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Kafeshani, M.; Feizi, A.; Esmaillzadeh, A.; Keshteli, A.H.; Afshar, H.; Roohafza, H.; Adibi, P. Higher vitamin B6 intake is associated with lower depression and anxiety risk in women but not in men: A large cross-sectional study. Int. J. Vitam. Nutr. Res. 2019, 90, 484–492. [Google Scholar] [CrossRef]
- Li, J.; Kang, X.; Zhang, L.; Luo, J.; Zhang, D. Dietary choline is inversely associated with depressive symptoms: A cross-sectional study of the National Health and Nutrition Examination Survey (NHANES) 2011 to 2018. J. Affect. Disord. 2022, 301, 23–29. [Google Scholar] [CrossRef]
- Nguyen, C.T.; Gracely, E.J.; Lee, B.K. Serum folate but not vitamin B-12 concentrations are positively associated with cognitive test scores in children aged 6–16 years. J. Nutr. 2013, 143, 500–504. [Google Scholar] [CrossRef]
- Puertollano, M.; Puertollano, E.; Alvarez de Cienfuegos, G.; de Pablo, A. Dietary antioxidants: Immunity and host defense. Curr. Top. Med. Chem. 2011, 11, 1752–1766. [Google Scholar] [CrossRef] [PubMed]
- Keya, T.A.; Leela, A.; Fernandez, K.; Habib, N.; Rashid, M. Effect of Vitamin C Supplements on Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Curr. Rev. Clin. Exp. Pharmacol. Former. Curr. Clin. Pharmacol. 2022, 17, 205–215. [Google Scholar] [CrossRef]
- Abioye, A.I.; Bromage, S.; Fawzi, W. Effect of micronutrient supplements on influenza and other respiratory tract infections among adults: A systematic review and meta-analysis. BMJ Glob. Health 2021, 6, e003176. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.; Arentz, S.; Goldenberg, J.; Yang, G.; Beardsley, J.; Myers, S.P.; Mertz, D.; Leeder, S. Zinc for the prevention or treatment of acute viral respiratory tract infections in adults: A rapid systematic review and meta-analysis of randomised controlled trials. BMJ Open 2021, 11, e047474. [Google Scholar] [CrossRef]
- Wang, M.X.; Win, S.S.; Pang, J. Zinc supplementation reduces common cold duration among healthy adults: A systematic review of randomized controlled trials with micronutrients supplementation. Am. J. Trop. Med. Hyg. 2020, 103, 86. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Das, R.R. Zinc for the common cold. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Bailey, L.B.; Stover, P.J.; McNulty, H.; Fenech, M.F.; Gregory III, J.F.; Mills, J.L.; Pfeiffer, C.M.; Fazili, Z.; Zhang, M.; Ueland, P.M. Biomarkers of nutrition for development—Folate review. J. Nutr. 2015, 145, 1636S–1680S. [Google Scholar] [CrossRef] [PubMed]
- National Center for Environmental Health, Division of Laboratory Sciences. Second National Report on Biochemical Indicators of Diet and Nutrition in the U.S; Population. Centers for Disease Control and Prevention: Atlanta, GA, USA, 2012. Available online: https://www.cdc.gov/nutritionreport/pdf/Nutrition_Book_complete508_final.pdf (accessed on 29 April 2022).
- Ueland, P.M.; Ulvik, A.; Rios-Avila, L.; Midttun, Ø.; Gregory, J.F. Direct and functional biomarkers of vitamin B6 status. Annu. Rev. Nutr. 2015, 35, 33–70. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.M.; Schleicher, R.L.; Caldwell, K.L. Biochemical indices. In Encyclopedia of Human Nutrition, 3rd ed.; Caballero, B., Ed.; Academic Press: Amsterdam, The Netherlands, 2013; pp. 156–174. [Google Scholar]
- Bailey, R.L.; Gahche, J.J.; Miller, P.E.; Thomas, P.R.; Dwyer, J.T. Why US adults use dietary supplements. JAMA Intern. Med. 2013, 173, 355–361. [Google Scholar] [CrossRef]
- Bailey, R.L.; Gahche, J.J.; Thomas, P.R.; Dwyer, J.T. Why US children use dietary supplements. Pediatr. Res. 2013, 74, 737–741. [Google Scholar] [CrossRef]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Zhang, F.F.; Bhupathiraju, S.N. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality Among US Adults, 1999–2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef]
- Cowan, A.E.; Tooze, J.A.; Gahche, J.J.; Eicher-Miller, H.A.; Guenther, P.M.; Dwyer, J.T.; Potischman, N.; Bhadra, A.; Carroll, R.J.; Bailey, R.L. Trends in Overall and Micronutrient-Containing Dietary Supplement Use in US Adults and Children, NHANES 2007–2018. J. Nutr. 2023, 152, 2789–2801. [Google Scholar] [CrossRef]
- Liu, J.; Micha, R.; Li, Y.; Mozaffarian, D. Trends in Food Sources and Diet Quality Among US Children and Adults, 2003-2018. JAMA Netw Open 2021, 4, e215262. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Foster, E.; Bradley, J. Methodological considerations and future insights for 24-h dietary recall assessment in children. Nutr. Res. 2018, 51, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Potischman, N.; Freudenheim, J.L. Biomarkers of nutritional exposure and nutritional status: An overview. J. Nutr. 2003, 133, 873S–874S. [Google Scholar] [CrossRef]

{kind=link}
| Age Group | ||||||
|---|---|---|---|---|---|---|
| 6 to 18 Years | 19 to 64 Years | |||||
| Demographic Characteristic | n | Mean | Standard Error | n | Mean | Standard Error |
| Age (years) | 7429 | 12.0 | 0.10 | 8252 | 39.7 | 0.24 |
| Gender (%) | 7429 | 8252 | ||||
| Males | 3724 | 51.1 | 0.95 | 4552 | 53.8 | 0.72 |
| Females | 3705 | 48.9 | 0.95 | 3700 | 46.2 | 0.72 |
| Race/ethnicity (%) | 7429 | 8252 | ||||
| Mexican American | 2154 | 12.2 | 1.16 | 1685 | 8.6 | 0.86 |
| Other Hispanic | 422 | 4.3 | 0.83 | 530 | 3.7 | 0.50 |
| Non-Hispanic white | 2091 | 62.5 | 2.20 | 3764 | 70.9 | 1.92 |
| Non-Hispanic black | 2399 | 14.8 | 1.37 | 1896 | 11.3 | 1.14 |
| Other race (including multiracial) | 363 | 6.2 | 0.82 | 377 | 5.6 | 0.54 |
| HH income (%) | 7066 | 7793 | ||||
| ≤1.35 of PIR | 2907 | 30.1 | 1.45 | 1948 | 16.8 | 0.85 |
| >1.35 to <1.85 of PIR | 832 | 9.4 | 0.75 | 818 | 7.9 | 0.41 |
| ≥1.85 of PIR | 3327 | 60.5 | 1.69 | 5027 | 75.3 | 1.01 |
| Education (%) b | 7154 | 7770 | ||||
| <High school | 2173 | 18.1 | 1.13 | 1651 | 13.2 | 0.72 |
| High school | 1791 | 26.0 | 1.23 | 1875 | 24.2 | 0.96 |
| >High school | 3190 | 55.9 | 1.41 | 4244 | 62.6 | 1.27 |
| Marital status (%) c | 7116 | 8141 | ||||
| Never been married | 4403 | 69.9 | 1.10 | 4135 | 54.1 | 1.21 |
| Divorced/Widowed | 1456 | 18.4 | 1.06 | 1168 | 14.0 | 0.63 |
| Currently married | 1257 | 11.7 | 0.84 | 2838 | 31.9 | 1.22 |
| BMI (%) d | 7370 | 8202 | ||||
| Underweight | 222 | 3.3 | 0.30 | 131 | 1.6 | 0.19 |
| Normal | 4404 | 63.1 | 1.41 | 2569 | 32.7 | 0.87 |
| Overweight | 1226 | 16.7 | 0.89 | 2720 | 33.1 | 0.75 |
| Obese | 1518 | 16.9 | 1.03 | 2782 | 32.6 | 1.08 |
| Dietary supplement use (%) | 7429 | 8252 | ||||
| Yes | 1663 | 29.4 | 1.26 | 3470 | 48.4 | 0.98 |
| No | 5766 | 70.6 | 1.26 | 4782 | 51.6 | 0.98 |
| Age Group | ||
|---|---|---|
| Age 6 to 18 Years | Age 19 to 64 Years | |
| n a | 7429 | 8252 |
| Reported missing school or work days due to illness/injury, n (%) b | 5131 (77) | 3919 (51) |
| Number of days missed, mean (SE) c | 4.00 (0.13) | 4.90 (0.33) |
| Predicted number of missed school or work days, mean d | 3.99 | 4.79 |
| Participants with lower absenteeism (missing days ≤ the predicted mean number of days missed), n (%) | 5162 (64) | 6930 (84) |
| Participants with higher absenteeism (missing days > the predicted mean number of days missed), n (%) | 2267 (36) | 1322 (16) |
| Food Alone | Food + Supplements | |||||||
|---|---|---|---|---|---|---|---|---|
| Nutrient | Lower Absenteeism n = 4534 | Higher Absenteeism n = 2002 | Lower Absenteeism n = 4534 | Higher Absenteeism n = 2002 | ||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
| Protein (g) | 76.3 | 0.9 | 72.1 * | 1.3 | 76.4 | 0.9 | 72.3 * | 1.3 |
| Carbohydrate (g) | 286 | 3 | 286 | 4 | 286 | 3 | 286 | 4 |
| Vitamin E as alpha-tocopherol (mg) | 6.3 | 0.1 | 6.2 | 0.1 | 9.9 | 0.9 | 10.5 | 0.8 |
| Vitamin A, RAE (μg) | 598 | 12 | 588 | 16 | 765 | 20 | 833 | 64 |
| Thiamin (Vitamin B1) (mg) | 1.67 | 0.02 | 1.62 | 0.03 | 1.99 | 0.05 | 2.31 | 0.2 |
| Riboflavin (Vitamin B2) (mg) | 2.24 | 0.03 | 2.2 | 0.04 | 2.59 | 0.07 | 2.79 | 0.16 |
| Niacin (mg) | 23.1 | 0.4 | 22.3 | 0.4 | 25.6 | 0.4 | 25.8 | 0.9 |
| Vitamin B6 (mg) | 1.84 | 0.03 | 1.75 * | 0.04 | 2.28 | 0.07 | 2.43 | 0.19 |
| Folate, DFE (μg) | 573 | 9 | 544 * | 12 | 667 | 12 | 672 | 27 |
| Vitamin B12 (μg) | 5.53 | 0.1 | 5.13 * | 0.14 | 6.81 | 0.19 | 6.86 | 0.34 |
| Vitamin D (D2 + D3) (μg) | 5.2 | 0.1 | 5 | 0.3 | 6.7 | 0.3 | 6.3 | 0.5 |
| Vitamin C (mg) | 82.4 | 2 | 77.6 | 3.1 | 107.6 | 3 | 105.5 | 4.9 |
| Calcium (mg) | 1040 | 16 | 1012 | 24 | 1068 | 17 | 1040 | 25 |
| Iron (mg) | 15.8 | 0.2 | 15.1 * | 0.3 | 17.6 | 0.3 | 17.1 | 0.4 |
| Magnesium (mg) | 241 | 3 | 236 | 4 | 246 | 3 | 241 | 4 |
| Phosphorus (mg) | 1317 | 15 | 1281 | 23 | 1325 | 15 | 1289 | 24 |
| Zinc (mg) | 11.8 | 0.2 | 11.1 * | 0.2 | 13.2 | 0.2 | 12.6 | 0.3 |
| Copper (mg) | 1.1 | 0.01 | 1.1 | 0.02 | 1.3 | 0.03 | 1.3 | 0.03 |
| Selenium (μg) | 101 | 1 | 96 * | 2 | 102 | 1 | 98 * | 2 |
| Vitamin K (μg) | 58.7 | 1.5 | 55.7 | 1.7 | 59.8 | 1.5 | 57.4 | 1.8 |
| Total choline (mg) | 266 | 5 | 248 * | 6 | 268 | 5 | 249 * | 6 |
| Potassium (mg) | 2297 | 33 | 2229 | 43 | 2301 | 33 | 2232 | 43 |
| Sodium (mg) | 3370 | 44 | 3275 | 56 | 3372 | 44 | 3276 | 56 |
| Dietary fiber (g) | 13.5 | 0.2 | 13.2 | 0.2 | 13.6 | 0.2 | 13.2 | 0.2 |
| PUFA 18:3 (Octadecatrienoic) (g) | 1.30 | 0.02 | 1.24 | 0.03 | 1.30 | 0.02 | 1.24 | 0.03 |
| Alpha-carotene (μg) | 350 | 40 | 315 | 38 | 350 | 40 | 315 | 38 |
| Beta-carotene (μg) | 1198 | 61 | 1109 | 79 | 1260 | 64 | 1209 | 84 |
| Beta-cryptoxanthin (μg) | 199 | 14 | 160 * | 15 | 199 | 14 | 160 * | 15 |
| Lycopene (μg) | 8324 | 425 | 7776 | 465 | 8331 | 425 | 7781 | 465 |
| Lutein + zeaxanthin (μg) | 765 | 29 | 719 | 33 | 770 | 29 | 723 | 32 |
| Total fat (g) | 80.7 | 1.1 | 79.1 | 1.1 | 80.7 | 1.1 | 79.2 | 1.1 |
| Total saturated fatty acids (g) | 28.3 | 0.4 | 27.7 | 0.5 | 28.3 | 0.4 | 27.7 | 0.5 |
| Total monounsaturated fatty acids (g) | 29.8 | 0.4 | 29.3 | 0.4 | 29.8 | 0.4 | 29.3 | 0.4 |
| Total polyunsaturated fatty acids (g) | 16 | 0.3 | 15.6 | 0.3 | 16 | 0.3 | 15.6 | 0.3 |
| PUFA 20:5 (Eicosapentaenoic) (g) | 0.01 | 0.001 | 0.01 | 0.001 | 0.01 | 0.001 | 0.01 | 0.002 |
| PUFA 22:6 (Docosahexaenoic) (g) | 0.05 | 0.003 | 0.04 * | 0.004 | 0.05 | 0.003 | 0.04 * | 0.004 |
| Food Alone | Food + Supplements | |||||||
|---|---|---|---|---|---|---|---|---|
| Nutrient | Lower Absenteeism n = 6086 | Higher Absenteeism n = 1213 | Lower Absenteeism n = 6086 | Higher Absenteeism n = 1213 | ||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | |
| Protein (g) | 89.8 | 0.9 | 86.3 * | 1.5 | 89.9 | 0.9 | 86.4 * | 1.5 |
| Carbohydrate (g) | 280 | 2 | 278 | 5 | 280 | 2 | 278 | 5 |
| Vitamin E as alpha-tocopherol (mg) | 7.8 | 0.1 | 7.4 * | 0.2 | 32.7 | 2.2 | 34.3 | 3.7 |
| Vitamin A, RAE (μg) | 618 | 11 | 596 | 18 | 1244 | 235 | 946 | 42 |
| Thiamin (Vitamin B1) (mg) | 1.76 | 0.02 | 1.69 * | 0.03 | 5.27 | 0.29 | 5.42 | 0.63 |
| Riboflavin (Vitamin B2) (mg) | 2.36 | 0.02 | 2.3 | 0.04 | 5.37 | 0.26 | 5.95 | 0.62 |
| Niacin (mg) | 27.1 | 0.3 | 25.7 * | 0.4 | 38 | 1.4 | 35.2 | 1.5 |
| Vitamin B6 (mg) | 2.08 | 0.02 | 1.95 * | 0.04 | 6.16 | 0.41 | 6.39 | 0.64 |
| Folate, DFE (μg) | 570 | 8 | 539 * | 9 | 799 | 16 | 770 | 25 |
| Vitamin B12 (μg) | 5.58 | 0.1 | 5.30 | 0.14 | 27.91 | 2.53 | 34.6 | 10.56 |
| Vitamin D (D2 + D3) (μg) | 4.6 | 0.2 | 4.2 | 0.3 | 8.5 | 0.3 | 8.9 | 1.4 |
| Vitamin C (mg) | 88.0 | 2 | 77.2 * | 3 | 192.1 | 11 | 178.8 | 13 |
| Calcium (mg) | 975 | 13 | 954 | 22 | 1126 | 17 | 1128 | 30 |
| Iron (mg) | 16.5 | 0.2 | 15.9 | 0.3 | 19.7 | 0.3 | 20.0 | 0.5 |
| Magnesium (mg) | 310 | 4 | 301 | 5 | 343 | 4 | 341 | 8 |
| Phosphorus (mg) | 1434 | 14 | 1389 | 25 | 1450 | 15 | 1403 | 26 |
| Zinc (mg) | 13.1 | 0.2 | 12.5 | 0.3 | 17.9 | 0.4 | 17.1 | 0.5 |
| Copper (mg) | 1.4 | 0.02 | 1.4 | 0.03 | 1.9 | 0.04 | 1.8 | 0.08 |
| Selenium (μg) | 119 | 1 | 113 * | 2 | 134 | 2 | 126 * | 3 |
| Vitamin K (μg) | 103.2 | 3.1 | 93.2 * | 3.2 | 109.8 | 3.1 | 99.1 * | 3.3 |
| Total choline (mg) | 351 | 4 | 328 * | 9 | 353 | 4 | 329 * | 9 |
| Potassium (mg) | 2824 | 27 | 2715 * | 41 | 2842 | 27 | 2730 * | 41 |
| Sodium (mg) | 3770 | 38 | 3733 | 62 | 3772 | 38 | 3735 | 62 |
| Dietary fiber (g) | 16.5 | 0.3 | 15.5 * | 0.3 | 16.5 | 0.3 | 15.6 * | 0.3 |
| PUFA 18:3 (Octadecatrienoic) (g) | 1.62 | 0.03 | 1.53 * | 0.04 | 1.64 | 0.03 | 1.54 * | 0.04 |
| Alpha-carotene (μg) | 788 | 46 | 629 * | 61 | 789 | 47 | 629 * | 61 |
| Beta-carotene (μg) | 1991 | 70 | 1815 | 95 | 2283 | 73 | 2049 * | 111 |
| Beta-cryptoxanthin (μg) | 187 | 11 | 158 | 15 | 187 | 11 | 158 | 15 |
| Lycopene (μg) | 9600 | 371 | 8335 * | 450 | 9683 | 371 | 8393 * | 450 |
| Lutein + zeaxanthin (μg) | 1369 | 45 | 1255 | 57 | 1453 | 46 | 1301 * | 58 |
| Total fat (g) | 89.2 | 1.1 | 88.2 | 1.8 | 89.4 | 1.1 | 88.3 | 1.7 |
| Total saturated fatty acids (g) | 29.6 | 0.4 | 29.6 | 0.6 | 29.6 | 0.4 | 29.7 | 0.6 |
| Total monounsaturated fatty acids (g) | 33.2 | 0.4 | 32.9 | 0.7 | 33.2 | 0.4 | 32.9 | 0.7 |
| Total polyunsaturated fatty acids (g) | 18.9 | 0.3 | 18.1 | 0.4 | 19 | 0.3 | 18.1 * | 0.4 |
| PUFA 20:5 (Eicosapentaenoic) (g) | 0.04 | 0.003 | 0.04 | 0.003 | 0.05 | 0.003 | 0.04 * | 0.003 |
| PUFA 22:6 (Docosahexaenoic) (g) | 0.1 | 0.005 | 0.09 | 0.008 | 0.11 | 0.005 | 0.09 * | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, Q.; Devarshi, P.P.; Grant, R.W.; Higgins, K.A.; Mitmesser, S.H. Lower Intakes of Key Nutrients Are Associated with More School and Workplace Absenteeism in US Children and Adults: A Cross-Sectional Study of NHANES 2003–2008. Nutrients 2023, 15, 4356. https://doi.org/10.3390/nu15204356
Ye Q, Devarshi PP, Grant RW, Higgins KA, Mitmesser SH. Lower Intakes of Key Nutrients Are Associated with More School and Workplace Absenteeism in US Children and Adults: A Cross-Sectional Study of NHANES 2003–2008. Nutrients. 2023; 15(20):4356. https://doi.org/10.3390/nu15204356
Chicago/Turabian StyleYe, Qian, Prasad P. Devarshi, Ryan W. Grant, Kelly A. Higgins, and Susan H. Mitmesser. 2023. "Lower Intakes of Key Nutrients Are Associated with More School and Workplace Absenteeism in US Children and Adults: A Cross-Sectional Study of NHANES 2003–2008" Nutrients 15, no. 20: 4356. https://doi.org/10.3390/nu15204356
APA StyleYe, Q., Devarshi, P. P., Grant, R. W., Higgins, K. A., & Mitmesser, S. H. (2023). Lower Intakes of Key Nutrients Are Associated with More School and Workplace Absenteeism in US Children and Adults: A Cross-Sectional Study of NHANES 2003–2008. Nutrients, 15(20), 4356. https://doi.org/10.3390/nu15204356