
The Effect of Three Different Ketogenic Diet Protocols on Migraine and Fatigue in Chronic and High-Frequency Episodic Migraine: A Pilot Study

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Participants, and Eligibility
2.2. Ethical Aspects
2.3. Ketogenic Diet Therapy
2.4. Fatigue Severity Scale
2.5. MIDAS and HIT-6 Scales
2.6. Primary Endpoint
2.7. Secondary Endpoint
2.8. Data and Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Silberstein, S.D. Migraine. Lancet 2004, 363, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Filler, K.; Lyon, D.; Bennett, J.; McCain, N.; Elswick, R.; Lukkahatai, N.; Saligan, L.N. Association of Mitochondrial Dysfunction and Fatigue: A Review of the Literature. BBA Clin. 2014, 1, 12–23. [Google Scholar] [CrossRef]
- Chaudhuri, A.; Behan, O.P. Fatigue in neurological disorders. Lancet 2004, 363, 978–988. [Google Scholar] [CrossRef]
- Seo, J.-G.; Park, S.-P. Significance of fatigue in patients with migraine. J. Clin. Neurosci. 2018, 50, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-W.; Chu, M.K.; Kim, J.-M.; Park, S.-G.; Cho, S.-J. Analysis of Trigger Factors in Episodic Migraineurs Using a Smartphone Headache Diary Applications. PLoS ONE 2016, 11, e0149577. [Google Scholar] [CrossRef]
- Peres, M.; Zukerman, E.; Young, W.; Silberstein, S. Fatigue in chronic migraine patients. Cephalalgia 2002, 22, 720–724. [Google Scholar] [CrossRef] [PubMed]
- Lucchesi, C.; Baldacci, F.; Cafalli, M.; Dini, E.; Giampietri, L.; Siciliano, G.; Gori, S. Fatigue, sleep-wake pattern, depressive and anxiety symptoms and body-mass index: Analysis in a sample of episodic and chronic migraine patients. Neurol. Sci. 2016, 37, 987–989. [Google Scholar] [CrossRef]
- Reynolds, K.J.; Vernon, S.D.; Bouchery, E.; Reeves, W.C. The economic impact of chronic fatigue syndrome. Cost Eff. Resour. Alloc. 2004, 2, 4. [Google Scholar] [CrossRef]
- Kaynak, H.; Altintaş, A.; Kaynak, D.; Uyanik, S.; Saip, S.; Ağaoğlu, J.; Önder, G.; Siva, A. Fatigue and sleep disturbance in multiple sclerosis. Eur. J. Neurol. 2006, 13, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- Aiyegbusi, O.L.; Hughes, E.S.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef] [PubMed]
- Yamato, M.; Kataoka, Y. Fatigue sensation following peripheral viral infection is triggered by neuroinflammation: Who will answer these questions? Neural. Regen. Res. 2015, 10, 203–204. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Lockwood, M.B.; Rhee, C.M.; Tantisattamo, E.; Andreoli, S.; Balducci, A.; Laffin, P.; Harris, T.; Knight, R.; Kumaraswami, L.; et al. Patient-centred approaches for the management of unpleasant symptoms in kidney disease. Nat. Rev. Nephrol. 2022, 18, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.I.; Cohen, S.I.; Alexander, M.P. Mild Traumatic Brain Injury, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Arnold, L.M.; Choy, E.; Clauw, D.J.; Goldenberg, D.L.; Harris, R.E.; Helfenstein, M.J.; Jensen, T.S.; Noguchi, K.; Silverman, S.L.; Ushida, T.; et al. Fibromyalgia and chronic pain syndromes: A white paper detailing current challenges in the field. Clin. J. Pain 2016, 32, 737–746. [Google Scholar] [CrossRef]
- Maged, A.M.; Abbassy, A.H.; Sakr, H.R.S.; Elsawah, H.; Wagih, H.; Ogila, A.I.; Kotb, A. Effect of swimming exercise on premenstrual syndrome. Arch. Gynecol. Obstet. 2018, 297, 951–959. [Google Scholar] [CrossRef]
- Wheless, J.W. History of the ketogenic diet. Epilepsia 2008, 49 (Suppl. S8), 3–5. [Google Scholar] [CrossRef]
- Arora, N.; Mehta, T.R. Role of the ketogenic diet in acute neurological diseases. Clin. Neurol. Neurosurg. 2020, 192, 105727. [Google Scholar] [CrossRef]
- Devivo, D.C.; Leckie, M.P.; Ferrendelli, J.S.; McDougal, D.B. Chronic ketosis and cerebral metabolism. Ann. Neurol. 1978, 3, 331–337. [Google Scholar] [CrossRef]
- Evcili, G.; Utku, U.; Oün, M.N.; Özdemir, G. Early and long period follow-up results of low-glycemic index diet for migraine prophylaxis. J. Turk. Soc. Algol. 2018, 30, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Tereshko, Y.; Dal Bello, S.; Di Lorenzo, C.; Pez, S.; Pittino, A.; Sartor, R.; Filippi, F.; Lettieri, C.; Belgrado, E.; Garbo, R.; et al. 2:1 ketogenic diet and low-glycemic-index diet for the treatment of chronic and episodic migraine: A single-center real-life retrospective study. J. Headache Pain 2023, 24, 95. [Google Scholar] [CrossRef]
- Bongiovanni, D.; Benedetto, C.; Corvisieri, S.; Del Favero, C.; Orlandi, F.; Allais, G.; Sinigaglia, S.; Fadda, M. Effectiveness of ketogenic diet in treatment of patients with refractory chronic migraine. Neurol. Sci. 2021, 42, 3865–3870. [Google Scholar] [CrossRef] [PubMed]
- Lovati, C.; D’alessandro, C.M.; Della Ventura, S.; Muzio, F.; Pantoni, L. Ketogenic diet in refractory migraine: Possible efficacy and role of ketone bodies—A pilot experience. Neurol. Sci. 2022, 43, 6479–6485. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Huffman, J.; Turner, Z.; Gladstein, J. Use of the modified Atkins diet for adolescents with chronic daily headache. Cephalalgia 2010, 30, 1014–1016. [Google Scholar] [PubMed]
- Valente, M.; Garbo, R.; Filippi, F.; Antonutti, A.; Ceccarini, V.; Tereshko, Y.; Di Lorenzo, C.; Gigli, G.L. Migraine Prevention through Ketogenic Diet: More than Body Mass Composition Changes. J. Clin. Med. 2022, 11, 4946. [Google Scholar] [CrossRef]
- Armutlu, K.; Korkmaz, N.C.; Keser, I.; Sumbuloglu, V.; Akbiyik, D.I.; Guney, Z.; Karabudak, R. The validity and reliability of the Fatigue Severity Scale in Turkish multiple sclerosis patients. Int. J. Rehabil. Res. 2007, 30, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Lipton, R.B.; Dowson, A.J.; Sawyer, J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology 2001, 56, S20–S28. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.E.; Park, J.W.; Kim, Y.I.; Lee, K.S. Headache impact test-6 (HIT-6) scores for migraine patients: Their relation to disability as measured from a headache diary. J. Clin. Neurol. 2008, 4, 158–163. [Google Scholar] [CrossRef]
- Karsan, N.; Goadsby, P.J. Migraine Is More Than Just Headache: Is the Link to Chronic Fatigue and Mood Disorders Simply Due to Shared Biological Systems? Front. Hum. Neurosci. 2021, 15, 646692. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Fofi, L.; Aurilia, C.; Egeo, G.; Caprio, M. Ketogenic diet in migraine: Rationale, findings and perspectives. Neurol. Sci. 2017, 38, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Fila, M.; Pawłowska, E.; Blasiak, J. Mitochondria in migraine pathophysiology—does epigenetics play a role? Arch. Med Sci. 2019, 15, 944–956. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Pierelli, F.; Coppola, G.; Grieco, G.S.; Rengo, C.; Ciccolella, M.; Magis, D.; Bolla, M.; Casali, C.; Santorelli, F.M.; et al. Mitochondrial DNA haplogroups influence the therapeutic response to riboflavin in migraineurs. Neurology 2009, 72, 1588–1594. [Google Scholar] [CrossRef] [PubMed]
- Maalouf, M.; Sullivan, P.G.; Davis, L.; Kim, D.Y.; Rho, J.M. Ketones inhibit mitochondrial production of reactive oxygen species production following glutamate excitotoxicity by increasing NADH oxidation. Neuroscience 2007, 145, 256–264. [Google Scholar] [CrossRef]
- Merlino, G.; Tereshko, Y.; Pez, S.; Dal Bello, S.; Pittino, A.; Di Lorenzo, C.; Filippi, F.; Lettieri, C.; Belgrado, E.; Gigli, G.L.; et al. Sleep of migraine patients is ameliorated by ketogenic diet, independently of pain control. Sleep Med. 2023, 107, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Lichstein, K.L.; Means, M.K.; Noe, S.L.; Aguillard, R.N. Fatigue and sleep disorders. Behav. Res. Ther. 1997, 35, 733–740. [Google Scholar] [CrossRef]
- Barrea, L.; Pugliese, G.; Frias-Toral, E.; Napolitano, B.; Laudisio, D.; Aprano, S.; Ceriani, F.; Savastano, S.; Colao, A.; Muscogiuri, G. Is there a relationship between the ketogenic diet and sleep disorders? Int. J. Food Sci. Nutr. 2021, 73, 285–295. [Google Scholar] [CrossRef]
- Seidel, S.; Hartl, T.; Weber, M.; Matterey, S.; Paul, A.; Riederer, F.; Gharabaghi, M.; Wöber-Bingöl, Ç.; Wöber, C.; PAMINA Study Group. Quality of sleep, fatigue and daytime sleepiness in migraine—A controlled study. Cephalalgia 2009, 29, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Lucchesi, C.; Sassi, A.N.; Siciliano, G.; Gori, S. Fatigue is increased in episodic migraine without aura patients. Headache 2013, 53, 1163–1165. [Google Scholar] [CrossRef] [PubMed]
- Snetselaar, L.G.; Cheek, J.J.; Fox, S.S.; Healy, H.S.; Schweizer, M.L.; Bao, W.; Kamholz, J.; Titcomb, T.J. Efficacy of Diet on Fatigue and Quality of Life in Multiple Sclerosis: A Systematic Review and Network Meta-Analysis of Randomized Trials. Neurology 2022, 100, e357–e366. [Google Scholar] [CrossRef]

{kind=link}
| During the Past Week, I Have Found That | Disagree ←→ Agree |
|---|---|
| 1. My motivation is lower when I am fatigued | 1 2 3 4 5 6 7 |
| 2. Exercise brings on my fatigue | 1 2 3 4 5 6 7 |
| 3. I am easily fatigued | 1 2 3 4 5 6 7 |
| 4. Fatigue interferes with my physical functioning | 1 2 3 4 5 6 7 |
| 5. Fatigue causes frequent problems for me | 1 2 3 4 5 6 7 |
| 6. My fatigue prevents sustained physical functioning | 1 2 3 4 5 6 7 |
| 7. Fatigue interferes with carrying out certain duties and responsibilities | 1 2 3 4 5 6 7 |
| 8. Fatigue is among my three most disabling symptoms | 1 2 3 4 5 6 7 |
| 9. Fatigue interferes with my work, family, or social life | 1 2 3 4 5 6 7 |
| Variable | Mean ± SD or N° (%) |
|---|---|
| Number of patients | 76 |
| Age | 45.895 ± 14.773 |
| Female sex | 58/70 (84.21%) |
| Smoking | 13/76 (17.11%) |
| Chronic migraine | 45/76 (59.21%) |
| Migraine duration (years) | 22.461 ± 17.364 |
| N° previous prophylaxes | 2.474 ± 2.069 |
| Concomitant prophylaxis | 42/76 (55.26%) |
| MOH | 37/76 (40.79%) |
| Depression | 7/76 (9.21%) |
| T0 | T1 | p-Value | |
|---|---|---|---|
| MIDAS | 76.079 ± 74.257 | 37.079 ± 59.076 | <0.001 |
| HIT-6 | 65.092 ± 6.575 | 54.105 ± 13.241 | <0.001 |
| Frequency (days/month) | 18.197 ± 8.408 | 8.750 ± 9.436 | <0.001 |
| Intensity (NRS) | 8.145 ± 1.055 | 5.355 ± 2.779 | <0.001 |
| FM (Kg) | 24.262 ± 11.338 | 18.328 ± 10.118 | <0.001 |
| FFM (Kg) | 49.822 ± 8.565 | 49.288 ± 8.196 | 0.136 |
| BMI (Kg/m2) | 26.715 ± 5.961 | 24.372 ± 5.044 | <0.001 |
| T0 | T1 | p-Value | |
|---|---|---|---|
| Item 1 | 6.263 ± 1.310 | 4.947 ± 2.052 | <0.001 |
| Item 2 | 5.289 ± 1.486 | 4.184 ± 1.853 | <0.001 |
| Item 3 | 4.697 ± 2.142 | 3.763 ± 2.103 | <0.001 |
| Item 4 | 5.408 ± 1.798 | 4.263 ± 2.043 | <0.001 |
| Item 5 | 4.526 ± 2.043 | 3.592 ± 2.054 | <0.001 |
| Item 6 | 4.987 ± 1.851 | 3.921 ± 2.140 | <0.001 |
| Item 7 | 4.842 ± 1.960 | 3.500 ± 2.030 | <0.001 |
| Item 8 | 4.461 ± 2.484 | 3.632 ± 2.214 | <0.001 |
| Item 9 | 4.316 ± 2.276 | 3.395 ± 2.123 | 0.003 |
| Total score | 4.977 ± 1.644 | 3.911 ± 1.779 | <0.001 |
| Total score: LGID | 5.030 ± 1.614 | 4.051 ± 1.740 | <0.001 |
| Total score: 2:1 | 5.016 ± 1.794 | 3.958 ± 1.945 | 0.034 |
| Total score: VLCKD | 4.762 ± 1.604 | 3.429 ± 1.678 | 0.006 |
| Total score: chronic migraine | 5.038 ± 1.643 | 3.944 ± 1.729 | <0.001 |
| Total score: high-frequency episodic migraine | 4.892 ± 1.669 | 3.856 ± 1.874 | 0.002 |
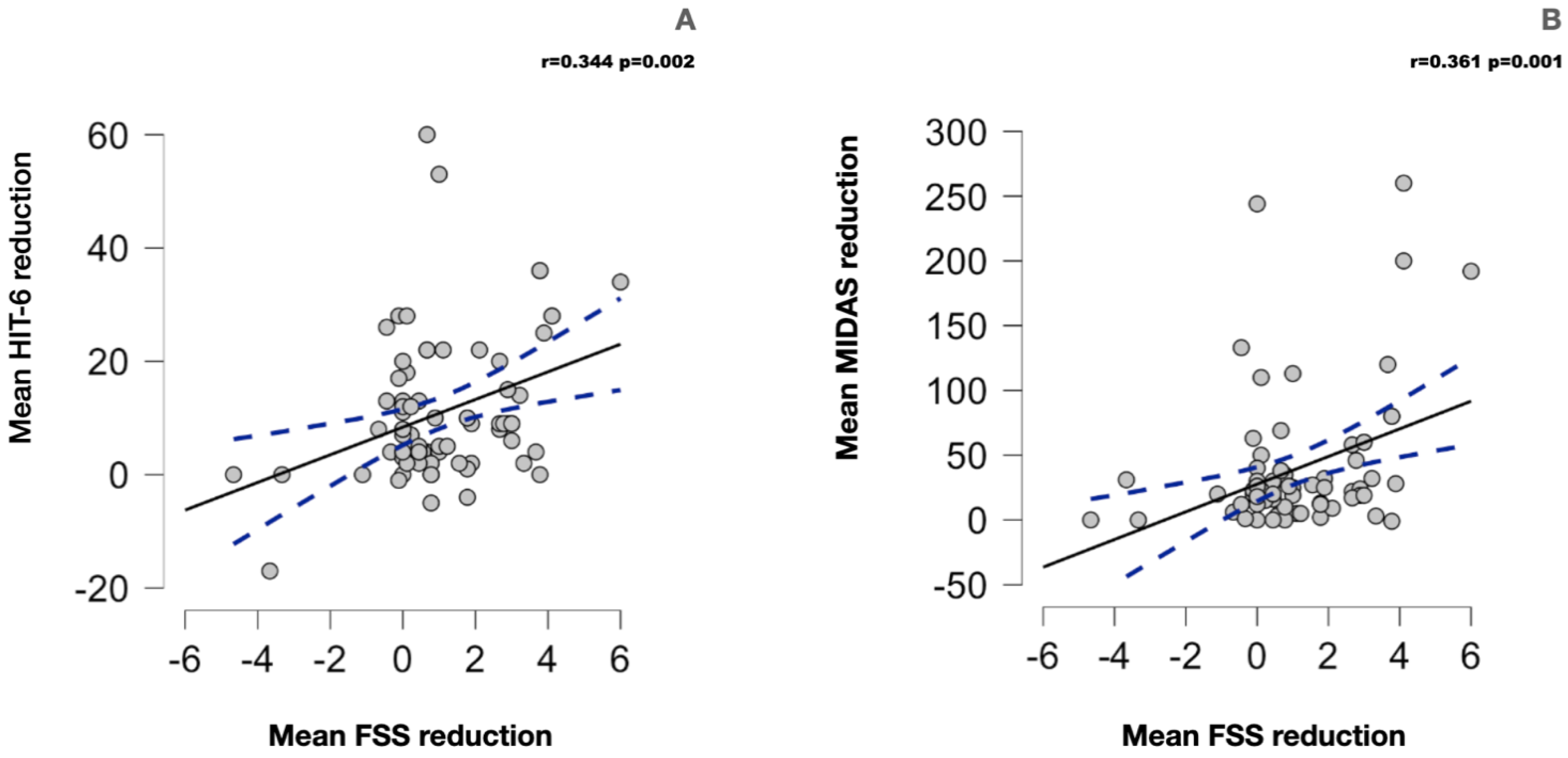
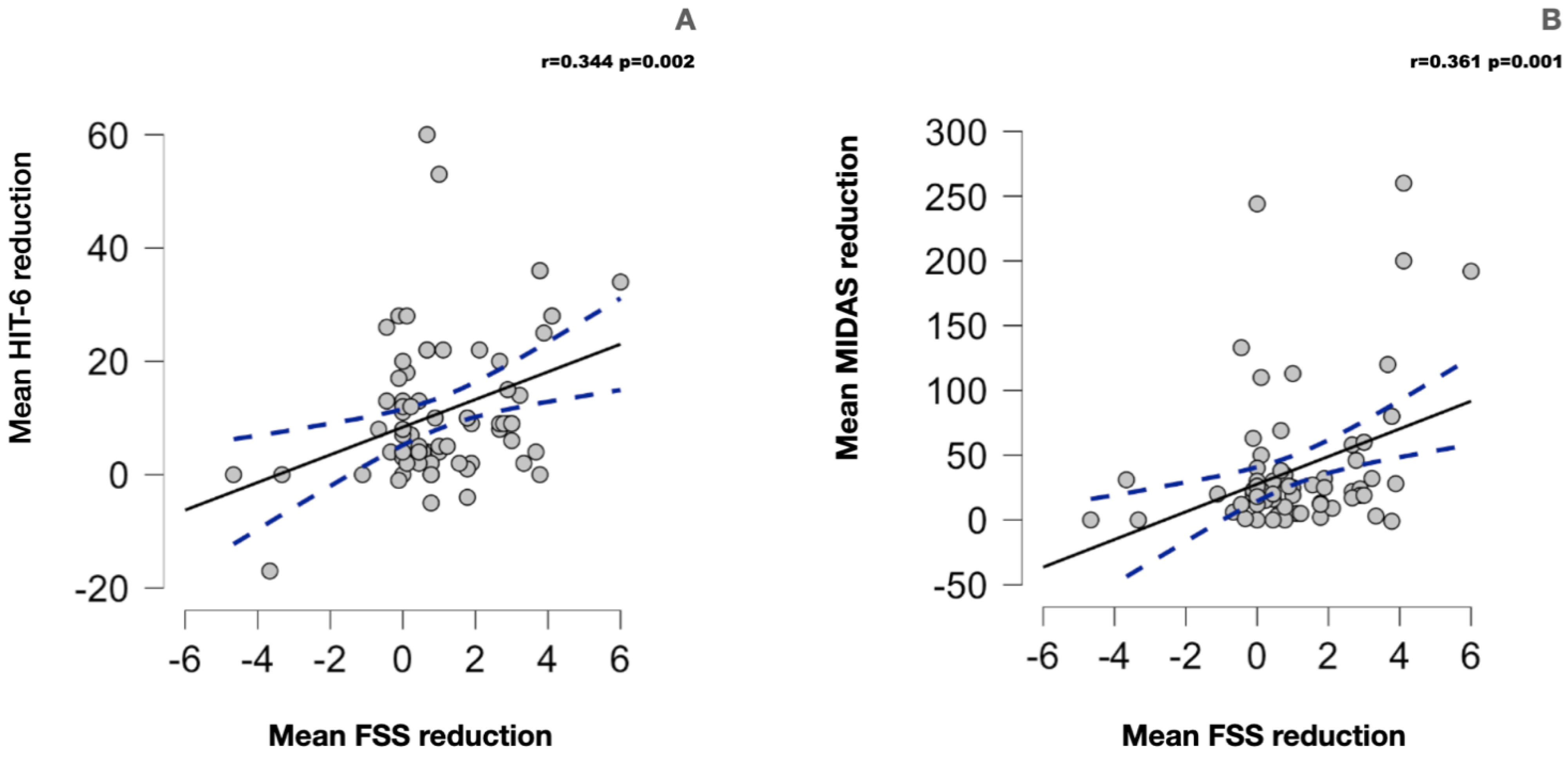
| Mean FSS Reduction | |
|---|---|
| Mean MIDAS reduction | r = 0.361 p = 0.001 |
| Mean HIT-6 reduction | r = 0.344 p = 0.002 |
| Mean frequency (days/month) reduction | r = 0.127 p = 0.296 |
| Mean intensity (NRS) reduction | r = −0.196 p = 0.090 |
| Mean FM reduction | r = 0.016 p = 0.888 |
| Mean BMI reduction | r = −0.053 p = 0.652 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tereshko, Y.; Dal Bello, S.; Di Lorenzo, C.; Pittino, A.; Filippi, F.; Belgrado, E.; Lettieri, C.; Merlino, G.; Gigli, G.L.; Valente, M. The Effect of Three Different Ketogenic Diet Protocols on Migraine and Fatigue in Chronic and High-Frequency Episodic Migraine: A Pilot Study. Nutrients 2023, 15, 4334. https://doi.org/10.3390/nu15204334
Tereshko Y, Dal Bello S, Di Lorenzo C, Pittino A, Filippi F, Belgrado E, Lettieri C, Merlino G, Gigli GL, Valente M. The Effect of Three Different Ketogenic Diet Protocols on Migraine and Fatigue in Chronic and High-Frequency Episodic Migraine: A Pilot Study. Nutrients. 2023; 15(20):4334. https://doi.org/10.3390/nu15204334
Chicago/Turabian StyleTereshko, Yan, Simone Dal Bello, Cherubino Di Lorenzo, Alice Pittino, Francesca Filippi, Enrico Belgrado, Christian Lettieri, Giovanni Merlino, Gian Luigi Gigli, and Mariarosaria Valente. 2023. "The Effect of Three Different Ketogenic Diet Protocols on Migraine and Fatigue in Chronic and High-Frequency Episodic Migraine: A Pilot Study" Nutrients 15, no. 20: 4334. https://doi.org/10.3390/nu15204334
APA StyleTereshko, Y., Dal Bello, S., Di Lorenzo, C., Pittino, A., Filippi, F., Belgrado, E., Lettieri, C., Merlino, G., Gigli, G. L., & Valente, M. (2023). The Effect of Three Different Ketogenic Diet Protocols on Migraine and Fatigue in Chronic and High-Frequency Episodic Migraine: A Pilot Study. Nutrients, 15(20), 4334. https://doi.org/10.3390/nu15204334