
Is Increasing Diet Diversity of Animal-Source Foods Related to Better Health-Related Quality of Life among Chinese Men and Women?

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Dietary Assessment and Animal-Source Food Diet Diversity
2.3. Health-Related Quality of Life
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
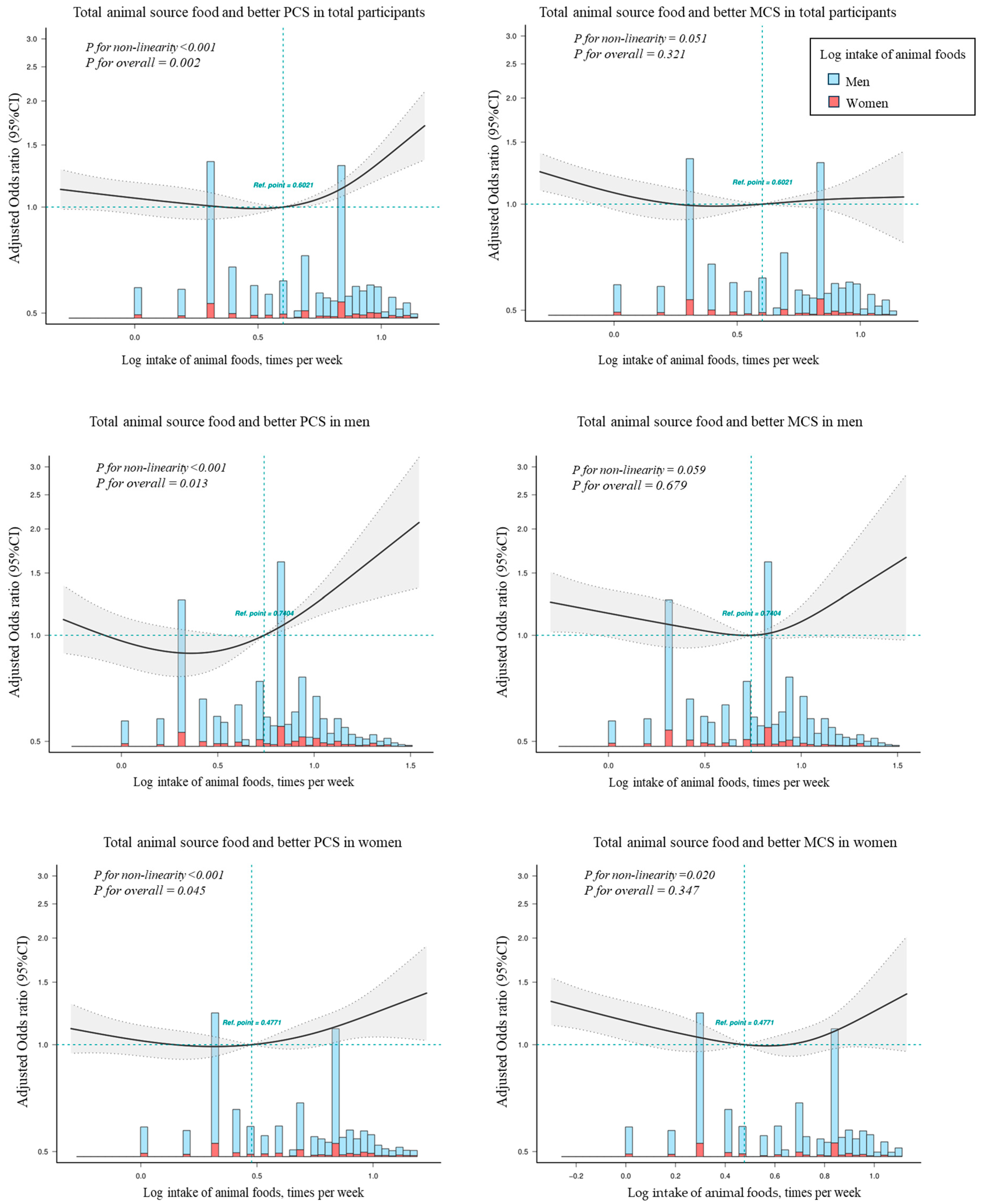
3.2. The Association of HRQoL with ASFDDS
3.3. The Association of HRQoL with Intake of Specific Animal Source Food
3.4. Subgroup Analyses and Sensitivity Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Meller, S. Can we say what diet is best for health? Annu. Rev. Public. Health 2014, 35, 83–103. [Google Scholar] [CrossRef] [PubMed]
- Galilea-Zabalza, I.; Buil-Cosiales, P.; Salas-Salvado, J.; Toledo, E.; Ortega-Azorin, C.; Diez-Espino, J.; Vazquez-Ruiz, Z.; Zomeno, M.D.; Vioque, J.; Martinez, J.A.; et al. Mediterranean diet and quality of life: Baseline cross-sectional analysis of the PREDIMED-PLUS trial. PLoS ONE 2018, 13, e0198974. [Google Scholar] [CrossRef] [PubMed]
- Govindaraju, T.; Sahle, B.W.; McCaffrey, T.A.; McNeil, J.J.; Owen, A.J. Dietary Patterns and Quality of Life in Older Adults: A Systematic Review. Nutrients 2018, 10, 971. [Google Scholar] [CrossRef]
- Baden, M.Y.; Kino, S.; Liu, X.; Li, Y.; Kim, Y.; Kubzansky, L.D.; Pan, A.; Okereke, O.I.; Willett, W.C.; Hu, F.B.; et al. Changes in plant-based diet quality and health-related quality of life in women. Br. J. Nutr. 2020, 124, 960–970. [Google Scholar] [CrossRef]
- Sanchez-Aguadero, N.; Alonso-Dominguez, R.; Garcia-Ortiz, L.; Agudo-Conde, C.; Rodriguez-Martin, C.; de Cabo-Laso, A.; Sanchez-Salgado, B.; Ramos, R.; Maderuelo-Fernandez, J.A.; Gomez-Marcos, M.A.; et al. Diet and physical activity in people with intermediate cardiovascular risk and their relationship with the health-related quality of life: Results from the MARK study. Health Qual. Life Outcomes 2016, 14, 169. [Google Scholar] [CrossRef]
- Munoz, M.A.; Fito, M.; Marrugat, J.; Covas, M.I.; Schroder, H.; REGICOR and HERMES Investigators. Adherence to the Mediterranean diet is associated with better mental and physical health. Br. J. Nutr. 2009, 101, 1821–1827. [Google Scholar] [CrossRef]
- Schiepers, O.J.; de Groot, R.H.; Jolles, J.; van Boxtel, M.P. Fish consumption, not fatty acid status, is related to quality of life in a healthy population. Prostaglandins Leukot. Essent. Fat. Acids 2010, 83, 31–35. [Google Scholar] [CrossRef]
- Myint, P.K.; Welch, A.A.; Bingham, S.A.; Surtees, P.G.; Wainwright, N.W.; Luben, R.N.; Wareham, N.J.; Smith, R.D.; Harvey, I.M.; Day, N.E.; et al. Fruit and vegetable consumption and self-reported functional health in men and women in the European Prospective Investigation into Cancer-Norfolk (EPIC-Norfolk): A population-based cross-sectional study. Public. Health Nutr. 2007, 10, 34–41. [Google Scholar] [CrossRef]
- Poulose, S.M.; Miller, M.G.; Shukitt-Hale, B. Role of walnuts in maintaining brain health with age. J. Nutr. 2014, 144, 561S–566S. [Google Scholar] [CrossRef] [PubMed]
- Pano, O.; Gamba, M.; Bullón-Vela, V.; Aguilera-Buenosvinos, I.; Roa-Díaz, Z.M.; Minder, B.; Kopp-Heim, D.; Laine, J.E.; Martínez-González, M.Á.; Martinez, A.; et al. Eating behaviors and health-related quality of life: A scoping review. Maturitas 2022, 165, 58–71. [Google Scholar] [CrossRef]
- Kouvari, M.; Panagiotakos, D.B.; Chrysohoou, C.; Yannakoulia, M.; Georgousopoulou, E.N.; Tousoulis, D.; Pitsavos, C. Meat consumption, depressive symptomatology and cardiovascular disease incidence in apparently healthy men and women: Highlights from the ATTICA cohort study (2002–2012). Nutr. Neurosci. 2020, 25, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.; Reedy, J.; Cudhea, F.; Zhang, J.; Shi, P.; Erndt-Marino, J.; Coates, J.; Micha, R.; Webb, P.; Mozaffarian, D.; et al. Global, regional, and national consumption of animal-source foods between 1990 and 2018: Findings from the Global Dietary Database. Lancet Planet Health 2022, 6, e243–e256. [Google Scholar] [CrossRef] [PubMed]
- Clegg, M.E.; Williams, E.A. Optimizing nutrition in older people. Maturitas 2018, 112, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Andrews, K.G.; Engell, R.E.; Mozaffarian, D.; Global Burden of Diseases, N.; Chronic Diseases Expert, G. Global, regional and national consumption of major food groups in 1990 and 2010: A systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open 2015, 5, e008705. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, L.; Yu, D.; Wang, Z.; Ding, G. Metabolic syndrome prevalence and its risk factors among adults in China: A nationally representative cross-sectional study. PLoS ONE 2018, 13, e0199293. [Google Scholar] [CrossRef]
- Commodity Consumption by Population Characteristics. Available online: https://www.ers.usda.gov/data-products/commodity-consumption-by-population-characteristics.aspx (accessed on 11 March 2020).
- McNeill, S.; Van Elswyk, M.E. Red meat in global nutrition. Meat Sci. 2012, 92, 166–173. [Google Scholar] [CrossRef]
- Darooghegi Mofrad, M.; Mozaffari, H.; Sheikhi, A.; Zamani, B.; Azadbakht, L. The association of red meat consumption and mental health in women: A cross-sectional study. Complement. Ther. Med. 2021, 56, 102588. [Google Scholar] [CrossRef]
- Verger, E.O.; Le Port, A.; Borderon, A.; Bourbon, G.; Moursi, M.; Savy, M.; Mariotti, F.; Martin-Prevel, Y. Dietary Diversity Indicators and Their Associations with Dietary Adequacy and Health Outcomes: A Systematic Scoping Review. Adv. Nutr. 2021, 12, 1659–1672. [Google Scholar] [CrossRef]
- Kennedy, G.; Ballard, T.; Dop, M. Guidelines for Measuring Household and Individual Dietary Diversity; FAO: Rome, Italy, 2012. [Google Scholar]
- Kennedy, G.; Fanou-Fogny, N.; Seghieri, C.; Arimond, M.; Koreissi, Y.; Dossa, R.; Kok, F.J.; Brouwer, I.D. Food groups associated with a composite measure of probability of adequate intake of 11 micronutrients in the diets of women in urban Mali. J. Nutr. 2010, 140, 2070S–2078S. [Google Scholar] [CrossRef] [PubMed]
- Narmaki, E.; Siassi, F.; Fariba, K.; Qorbani, M.; Shiraseb, F.; Ataie-Jafari, A.; Sotoudeh, G. Dietary diversity as a proxy measure of blood antioxidant status in women. Nutrition 2015, 31, 722–726. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Jahangiry, L. Dietary diversity score is associated with cardiovascular risk factors and serum adiponectin concentrations in patients with metabolic syndrome. BMC Cardiovasc. Disord. 2018, 18, 68. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Li, Y.; Zhou, Y.; Zhang, C.; Li, L.; Luo, Y.; Wang, J.; Duan, Y.; Xie, J. Association of Non-alcoholic Fatty Liver Disease With Salt Intake and Dietary Diversity in Chinese Medical Examination Adults Aged 18–59 Years: A Cross-Sectional Study. Front. Nutr. 2022, 9, 930316. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, M.; Shin, Y.; Cho, J.H.; Lee, D.; Kim, Y. Association between Dietary Diversity Score and Metabolic Syndrome in Korean Adults: A Community-Based Prospective Cohort Study. Nutrients 2022, 14, 5298. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, Y.; Shi, G.; Mi, B.; Zeng, L.; Li, Q.; Shen, Y.; Zhao, Y.; Pei, L.; Kang, Y.; et al. Cohort Profile: Regional Ethnic Cohort Study in Northwest China. Int. J. Epidemiol. 2021, 51, e18–e26. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Guo, Y.; Pei, P.; Du, H.; Yang, L.; Chen, Y.; Shen, X.; Shi, Z.; Qi, L.; Chen, J.; et al. The Relative Validity and Reproducibility of Food Frequency Questionnaires in the China Kadoorie Biobank Study. Nutrients 2022, 14, 794. [Google Scholar] [CrossRef]
- Wang, S.S.; Lay, S.; Yu, H.N.; Shen, S.R. Dietary Guidelines for Chinese Residents (2016): Comments and comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef]
- Ware, J.E., Jr. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef]
- Cindy, L.K.; Lam, E.Y.Y.T. Barbara Gandek. Is the standard SF-12 Health Survey valid and equivalent for aChinese population. Qual. Life Res. 2005, 14, 539–547. [Google Scholar]
- Lin, Y.; Yu, Y.; Zeng, J.; Zhao, X.; Wan, C. Comparing the reliability and validity of the SF-36 and SF-12 in measuring quality of life among adolescents in China: A large sample cross-sectional study. Health Qual. Life Outcomes 2020, 18, 360. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinski, M.A.; Keller, S.D. SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales; The Health Institute: Boston, MA, USA, 1998. [Google Scholar]
- Bize, R.; Johnson, J.A.; Plotnikoff, R.C. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev. Med. 2007, 45, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Almagro, J.; Garcia-Manzanares, A.; Lucendo, A.J.; Hernandez-Martinez, A. Health-related quality of life in diabetes mellitus and its social, demographic and clinical determinants: A nationwide cross-sectional survey. J. Clin. Nurs. 2018, 27, 4212–4223. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Drada, J.A.; Silva da Cruz, A.J.; Soares de Faria, M.L.; Miranda Cota, L.O.; Parreiras Martins, M.A.; Almeida Pordeus, I.; Nogueira Guimaraes de Abreu, M.H. Oral Health-Related Quality of Life in Anticoagulated Patients with Warfarin Treatment: A Cross-Sectional Study. Int. J. Environ. Res. Public. Health 2021, 18, 3714. [Google Scholar] [CrossRef]
- Bennett, D.A.; Du, H.; Clarke, R.; Guo, Y.; Yang, L.; Bian, Z.; Chen, Y.; Millwood, I.; Yu, C.; He, P.; et al. Association of Physical Activity With Risk of Major Cardiovascular Diseases in Chinese Men and Women. JAMA Cardiol. 2017, 2, 1349–1358. [Google Scholar] [CrossRef]
- Albalawi, A.A.; Hambly, C.; Speakman, J.R. Consumption of takeaway and delivery meals is associated with increased BMI and percent fat among UK Biobank participants. Am. J. Clin. Nutr. 2022, 116, 173–188. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Fei, Z.; Qiu, C.; Brasher, M.S.; Kraus, V.B.; Zhao, W.; Shi, X.; Zeng, Y. Dietary Diversity and Cognitive Function among Elderly People: A Population-Based Study. J. Nutr. Health Aging 2017, 21, 1089–1094. [Google Scholar] [CrossRef]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liskiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-Analysis for Linear and Nonlinear Dose-Response Relations: Examples, an Evaluation of Approximations, and Software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef]
- Frank, E.; Harrell, J. Ordinal logistic regression. In Regression Modeling Strategies; Springer: New York, NY, USA, 2015; pp. 311–324. [Google Scholar]
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Luchini, C.; Maggi, S. Adherence to the Mediterranean diet is associated with better quality of life: Data from the Osteoarthritis Initiative. Am. J. Clin. Nutr. 2016, 104, 1403–1409. [Google Scholar] [CrossRef]
- Kathy Hoy, J.C.; Alanna, M. Estimated Protein Intake From Animal and Plant Foods by U.S.; Adults, What We Eat in America, NHANES, 2015–2016. Curr. Dev. Nutr. 2021, 5, 133. [Google Scholar]
- Monsivais, P.; Aggarwal, A.; Drewnowski, A. Are socio-economic disparities in diet quality explained by diet cost? J. Epidemiol. Community Health 2012, 66, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Nair, M.K.; Augustine, L.F.; Konapur, A. Food-Based Interventions to Modify Diet Quality and Diversity to Address Multiple Micronutrient Deficiency. Front. Public. Health 2015, 3, 277. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Decsi, T.; Fewtrell, M.; Goulet, O.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Moreno, L.; Puntis, J.; Rigo, J.; et al. Complementary feeding: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, A.; Murakami, K.; Kobayashi, S.; Suga, H.; Sasaki, S.; Three-generation Study of Women on Diets and Health Study Group. Associations of Education with Overall Diet Quality Are Explained by Different Food Groups in Middle-aged and Old Japanese Women. J. Epidemiol. 2021, 31, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhu, S.; Zhou, Y.; Pramono, A.; Zhou, Z. Changing Income-Related Inequality in Daily Nutrients Intake: A Longitudinal Analysis from China. Int. J. Environ. Res. Public. Health 2020, 17, 7627. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, H.; Shimomura, I.; Kishida, K.; Maeda, N.; Kuriyama, H.; Nagaretani, H.; Matsuda, M.; Kondo, H.; Furuyama, N.; Kihara, S.; et al. Androgens decrease plasma adiponectin, an insulin-sensitizing adipocyte-derived protein. Diabetes 2002, 51, 2734–2741. [Google Scholar] [CrossRef]
- Gluvic, Z.; Zaric, B.; Resanovic, I.; Obradovic, M.; Mitrovic, A.; Radak, D.; Isenovic, E. Link between Metabolic Syndrome and Insulin Resistance. Curr. Vasc. Pharmacol. 2017, 15, 30–39. [Google Scholar] [CrossRef]
- Liu, R.; Zhao, Y.; Wang, X.; Fu, H.; Li, Q.; Dang, S.; Yan, H. Association of Egg Consumption Frequency and Quantity with Dyslipidemia in Chinese Rural Adults. J. Am. Nutr. Assoc. 2022, 42, 548–558. [Google Scholar] [CrossRef]
- Shen, X.; Fang, A.; He, J.; Liu, Z.; Guo, M.; Gao, R.; Li, K. Trends in dietary fat and fatty acid intakes and related food sources among Chinese adults: A longitudinal study from the China Health and Nutrition Survey (1997–2011). Public Health Nutr. 2017, 20, 2927–2936. [Google Scholar] [CrossRef]
- Li, X.; Tian, D.; Qin, P.; Guo, W.; Lu, J.; Zhu, W.; Zhang, Q.; Wang, J. Dietary, physical exercises and mental stress in a Chinese population: A cross-sectional study. BMC Public Health 2021, 21, 1138. [Google Scholar] [CrossRef] [PubMed]
- Boye, J.; Wijesinha-Bettoni, R.; Burlingame, B. Protein quality evaluation twenty years after the introduction of the protein digestibility corrected amino acid score method. Br. J. Nutr. 2012, 108 (Suppl. S2), S183–S211. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.P.; Allen, L.H. Nutritional importance of animal source foods. J. Nutr. 2003, 133, 3932S–3935S. [Google Scholar] [CrossRef] [PubMed]
- Anderson, V.P.; Cornwall, J.; Jack, S.; Gibson, R.S. Intakes from non-breastmilk foods for stunted toddlers living in poor urban villages of Phnom Penh, Cambodia, are inadequate. Matern. Child Nutr. 2008, 4, 146–159. [Google Scholar] [CrossRef]
- Hajianfar, H.; Mollaghasemi, N.; Tavakoly, R.; Campbell, M.S.; Mohtashamrad, M.; Arab, A. The Association Between Dietary Zinc Intake and Health Status, Including Mental Health and Sleep Quality, Among Iranian Female Students. Biol. Trace Elem. Res. 2021, 199, 1754–1761. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A.; Baig, M.; Tunio, S.A.; Memon, A.S.; Karmani, H. Neuropsychiatric and neurological problems among Vitamin B12 deficient young vegetarians. Neurosciences 2017, 22, 228–232. [Google Scholar] [CrossRef] [PubMed]
- McCann, J.C.; Ames, B.N. Is there convincing biological or behavioral evidence linking vitamin D deficiency to brain dysfunction? FASEB J. 2008, 22, 982–1001. [Google Scholar] [CrossRef]
- Hsu, Y.H.; Liang, C.K.; Chou, M.Y.; Liao, M.C.; Lin, Y.T.; Chen, L.K.; Lo, Y.K. Association of cognitive impairment, depressive symptoms and sarcopenia among healthy older men in the veterans retirement community in southern Taiwan: A cross-sectional study. Geriatr. Gerontol. Int. 2014, 14 (Suppl. S1), 102–108. [Google Scholar] [CrossRef]
- Dobersek, U.; Wy, G.; Adkins, J.; Altmeyer, S.; Krout, K.; Lavie, C.J.; Archer, E. Meat and mental health: A systematic review of meat abstention and depression, anxiety, and related phenomena. Crit. Rev. Food Sci. Nutr. 2021, 61, 622–635. [Google Scholar] [CrossRef]
- Lang, T.F. The Bone-Muscle Relationship in Men and Women. J. Osteoporos. 2011, 2011, 702735. [Google Scholar] [CrossRef]
- Remes, O.; Brayne, C.; van der Linde, R.; Lafortune, L. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. 2016, 6, e00497. [Google Scholar] [CrossRef]
- Koochakpoor, G.; Salari-Moghaddam, A.; Keshteli, A.H.; Afshar, H.; Esmaillzadeh, A.; Adibi, P. Dietary intake of branched-chain amino acids in relation to depression, anxiety and psychological distress. Nutr. J. 2021, 20, 11. [Google Scholar] [CrossRef]
- Embling, R.; Pink, A.E.; Gatzemeier, J.; Price, M.; Lee, M.D.; Wilkinson, L.L. Effect of food variety on intake of a meal: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2021, 113, 716–741. [Google Scholar] [CrossRef]

{kind=link}
| Men n = 14,383 | Women n = 25,614 | Total n = 39,997 | p-Value | |
|---|---|---|---|---|
| Age (year), | 50.28 13.97 | 50.53 12.56 | 50.43 13.09 | 0.050 |
| Age group, n (%) | 0.041 | |||
| 40 | 3946 (27.4) | 5588 (21.8) | 9534 (23.8) | |
| 41–50 | 2397 (16.7) | 5259 (20.5) | 7656 (19.1) | |
| 51–60 | 3679 (25.6) | 8216 (32.1) | 11,895 (29.7) | |
| 61 | 4361 (30.3) | 6551 (25.6) | 10,912 (27.3) | |
| SES, n (%) | <0.001 | |||
| Low | 4130 (28.7) | 11,402 (44.5) | 15,532 (38.8) | |
| Median | 3996 (27.8) | 7490 (29.2) | 11,486 (28.7) | |
| High | 6257 (43.5) | 6722 (26.2) | 12,979 (32.4) | |
| Married, n (%) | 12,469 (86.7) | 22,831 (89.1) | 35,300 (88.3) | <0.001 |
| Urban, n (%) | 5647 (39.3) | 6374 (24.9) | 12,021 (30.1) | <0.001 |
| Drinking, n (%) | 2785 (19.4) | 454 (1.8) | 3239 (8.1) | <0.001 |
| Smoking, n (%) | 5897 (41.0) | 121 (4.7) | 6018 (15.1) | <0.001 |
| BMI (kg/m2), | 24.24 3.45 | 23.57 3.62 | 23.82 3.57 | <0.001 |
| BMI group, n (%) | <0.001 | |||
| <18.5 | 520 (3.6) | 1334 (5.2) | 1854 (4.6) | |
| 18.5–23.9 | 6452 (44.9) | 13,544 (52.9) | 19,996 (50.0) | |
| ≧24.0 | 7411 (51.5) | 10,736 (41.9) | 18,147 (45.4) | |
| History of chronic disease, n (%) | 5413 (37.6) | 9288 (36.3) | 14,701 (36.8) | 0.029 |
| Physical activity (MET:h/d), | 25.48 13.61 | 20.01 11.72 | 21.94 12.69 | <0.001 |
| More than 21.4 MET, n (%) | 8868 (61.7) | 11,131 (43.5) | 19,999 (50.0) | |
| Frequency of staple food intake (times/week), | 11.62 4.48 | 11.56 4.52 | 11.57 4.52 | 0.227 |
| More than 11 times/week, n (%) | 6517 (45.3) | 11,333 (44.2) | 17,850 (44.6) | <0.001 |
| Unhealthy eating habits(times/week), | 4.85 6.94 | 3.54 5.80 | 4.01 6.27 | <0.001 |
| More than three times/week, n (%) | 7812 (54.3) | 11,320 (44.2) | 19,132 (47.8) | <0.001 |
| ODDS, | 1.95 0.95 | 2.02 0.92 | 1.99 0.93 | <0.001 |
| Intake of animal source foods (times/week), | 5.52 5.54 | 3.82 4.74 | 4.43 5.11 | <0.001 |
| Pork, | 3.12 2.65 | 2.32 2.55 | 2.61 2.62 | <0.001 |
| Mutton, | 0.57 1.25 | 0.31 0.97 | 0.41 1.08 | <0.001 |
| Beef, | 0.68 1.36 | 0.40 1.07 | 0.50 1.19 | <0.001 |
| Poultry, | 0.71 1.40 | 0.47 1.16 | 0.56 1.26 | <0.001 |
| Seafood, | 0.44 1.01 | 0.32 0.89 | 0.36 0.94 | <0.001 |
| Eggs, | 2.57 2.61 | 2.26 2.57 | 2.37 2.59 | <0.001 |
| Pure milk, | 1.56 2.43 | 1.39 2.43 | 1.45 2.43 | <0.001 |
| Yogurt, | 0.91 1.75 | 0.93 1.87 | 0.92 1.83 | 0.512 |
| ASFDDS, | 1.07 1.24 | 0.92 1.17 | 0.98 1.20 | <0.001 |
| 0, n (%) | 5570 (38.7) | 11,875 (46.4) | 17,445 (43.6) | |
| 1, n (%) | 5084 (35.3) | 7938 (31.0) | 13,022 (32.6) | |
| 2, n (%) | 2199 (15.3) | 3353 (13.1) | 5552 (13.9) | |
| 2, n (%) | 1530 (10.6) | 2448 (9.6) | 3978 (9.9) | |
| Life quality score | ||||
| PCS, | 49.86 7.20 | 49.29 7.44 | 49.49 7.35 | <0.001 |
| Better PCS | 1643 (11.4) | 2745 (10.7) | 4388 (11.0) | 0.016 |
| MCS, | 52.70 6.98 | 52.34 7.18 | 52.47 7.11 | <0.001 |
| Better MCS | 1588 (11.0) | 2676 (10.4) | 4264 (10.7) | 0.034 |
| ASFDDS | ASFDDS Category | |||||||
|---|---|---|---|---|---|---|---|---|
| 0 (n = 17,445) | 1 (n = 13,022) | ≥2 (n = 9530) | ||||||
| OR (95%CI) | p | Reference | OR (95%CI) | p | OR (95%CI) | p | ||
| Total | ||||||||
| PCS | Model 1 | 1.12 (1.10, 1.14) | <0.001 | Ref. | 1.00 (0.93, 1.08) | 0.959 | 1.33 (1.23, 1.43) | <0.001 |
| Model 2 | 1.04 (1.02, 1.07) | 0.001 | Ref. | 0.93 (0.86, 1.00) | 0.063 | 1.07 (0.99, 1.17) | 0.091 | |
| Model 3 | 1.09 (1.04, 1.14) | <0.001 | Ref. | 1.06 (0.97, 1.17) | 0.179 | 1.26 (1.13, 1.40) | <0.001 | |
| MCS | Model 1 | 0.91 (0.89, 0.94) | <0.001 | Ref. | 0.85 (0.79, 0.91) | <0.001 | 0.75 (0.69, 0.82) | <0.001 |
| Model 2 | 1.00 (0.97, 1.03) | 0.899 | Ref. | 0.91 (0.85, 0.98) | 0.012 | 0.97 (0.89, 1.06) | 0.496 | |
| Model 3 | 1.03 (0.98, 1.07) | 0.252 | Ref. | 0.97 (0.89, 1.06) | 0.469 | 1.12 (1.00, 1.26) | 0.056 | |
| Men | ||||||||
| PCS | Model 1 | 1.10 (1.06, 1.15) | <0.001 | Ref. | 0.89 (0.78, 1.00) | 0.059 | 1.25 (1.10, 1.41) | 0.001 |
| Model 2 | 1.04 (1.00, 1.08) | 0.062 | Ref. | 0.83 (0.73, 0.94) | 0.003 | 1.04 (0.91, 1.18) | 0.609 | |
| Model 3 | 1.08 (1.01, 1.15) | 0.026 | Ref. | 0.93 (0.80, 1.08) | 0.931 | 1.16 (1.01, 1.34) | 0.002 | |
| MCS | Model 1 | 0.93 (0.89, 0.98) | 0.002 | Ref. | 0.84 (0.74, 0.95) | 0.004 | 0.80 (0.70, 0.92) | 0.001 |
| Model 2 | 1.03 (0.99, 1.08) | 0.157 | Ref. | 0.93 (0.82, 1.14) | 0.207 | 1.07 (0.93, 1.23) | 0.350 | |
| Model 3 | 1.11 (1.04, 1.19) | 0.003 | Ref. | 1.02 (0.89, 1.18) | 0.759 | 1.24 (1.03, 1.48) | 0.020 | |
| Women | ||||||||
| PCS | Model 1 | 1.12 (1.09, 1.16) | <0.001 | Ref. | 1.07 (0.97, 1.17) | 0.173 | 1.36 (1.23, 1.50) | <0.001 |
| Model 2 | 1.05 (1.01, 1.08) | 0.010 | Ref. | 1.00 (0.91, 1.10) | 0.949 | 1.09 (0.98, 1.21) | 0.120 | |
| Model 3 | 1.10 (1.04, 1.16) | 0.001 | Ref. | 1.15 (1.01, 1.29) | 0.017 | 1.34 (1.16, 1.54) | <0.001 | |
| MCS | Model 1 | 0.89 (0.86, 0.93) | <0.001 | Ref. | 0.85 (0.77, 0.93) | <0.001 | 0.72 (0.64, 0.80) | <0.001 |
| Model 2 | 0.97 (0.94, 1.01) | 0.188 | Ref. | 0.90 (0.82, 0.99) | 0.031 | 0.91 (0.81, 1.02) | 0.097 | |
| Model 3 | 0.97 (0.93, 1.04) | 0.973 | Ref. | 0.94 (0.84, 1.05) | 0.260 | 1.04 (0.90, 1.22) | 0.580 | |
| PCS | MCS | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Red meat (pork, mutton, beef) | ||||
| Total | 1.02 (1.01, 1.03) | 0.003 | 1.00 (0.99, 1.02) | 0.509 |
| Men | 1.02 (1.00, 1.04) | 0.017 | 1.01 (0.99, 1.03) | 0.418 |
| Women | 1.02 (1.00, 1.03) | 0.005 | 1.00 (0.98, 1.02) | 0.908 |
| White meat (poultry) | ||||
| Total | 1.08 (1.04, 1.11) | <0.001 | 0.97 (0.93, 1.02) | 0.239 |
| Men | 1.07 (1.04, 1.11) | <0.001 | 1.02 (0.97, 1.06) | 0.451 |
| Women | 1.07 (1.04, 1.10) | <0.001 | 0.99 (0.95, 1.04) | 0.706 |
| Seafood | ||||
| Total | 1.13 (1.08, 1.18) | <0.001 | 1.06 (1.00, 1.12) | 0.050 |
| Men | 1.13 (1.06, 1.20) | <0.001 | 1.09 (1.01, 1.18) | 0.032 |
| Women | 1.13 (1.07, 1.20) | <0.001 | 1.03 (0.95, 1.11) | 0.479 |
| Eggs | ||||
| Total | 1.02 (1.01, 1.04) | 0.006 | 1.02 (1.01, 1.04) | 0.009 |
| Men | 1.01 (0.98, 1.04) | 0.463 | 1.02 (1.00, 1.05) | 0.115 |
| Women | 1.03 (1.01, 1.05) | 0.004 | 1.02 (1.00, 1.04) | 0.041 |
| Dairy | ||||
| Total | 1.04 (1.02, 1.06) | <0.001 | 1.00 (0.98, 1.02) | 0.979 |
| Men | 1.04 (1.01, 1.07) | 0.005 | 1.01 (0.99, 1.04) | 0.363 |
| Women | 1.04 (1.02, 1.06) | <0.001 | 0.99 (0.97, 1.02) | 0.484 |
| Overall animal source of food | ||||
| Total | 1.01 (1.01, 1.03) | <0.001 | 1.00 (0.99, 1.01) | 0.528 |
| Men | 1.02 (1.01, 1.04) | <0.001 | 1.02 (0.99, 1.05) | 0.115 |
| Women | 1.02 (1.01, 1.03) | 0.001 | 1.00 (0.99, 1.01) | 0.976 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jing, H.; Teng, Y.; Chacha, S.; Wang, Z.; Shi, G.; Mi, B.; Zhang, B.; Cai, J.; Liu, Y.; Li, Q.; et al. Is Increasing Diet Diversity of Animal-Source Foods Related to Better Health-Related Quality of Life among Chinese Men and Women? Nutrients 2023, 15, 4183. https://doi.org/10.3390/nu15194183
Jing H, Teng Y, Chacha S, Wang Z, Shi G, Mi B, Zhang B, Cai J, Liu Y, Li Q, et al. Is Increasing Diet Diversity of Animal-Source Foods Related to Better Health-Related Quality of Life among Chinese Men and Women? Nutrients. 2023; 15(19):4183. https://doi.org/10.3390/nu15194183
Chicago/Turabian StyleJing, Hui, Yuxin Teng, Samuel Chacha, Ziping Wang, Guoshuai Shi, Baibing Mi, Binyan Zhang, Jiaxin Cai, Yezhou Liu, Qiang Li, and et al. 2023. "Is Increasing Diet Diversity of Animal-Source Foods Related to Better Health-Related Quality of Life among Chinese Men and Women?" Nutrients 15, no. 19: 4183. https://doi.org/10.3390/nu15194183
APA StyleJing, H., Teng, Y., Chacha, S., Wang, Z., Shi, G., Mi, B., Zhang, B., Cai, J., Liu, Y., Li, Q., Shen, Y., Yang, J., Kang, Y., Li, S., Liu, D., Wang, D., Yan, H., & Dang, S. (2023). Is Increasing Diet Diversity of Animal-Source Foods Related to Better Health-Related Quality of Life among Chinese Men and Women? Nutrients, 15(19), 4183. https://doi.org/10.3390/nu15194183