

Serum Sulfur-Containing Amino Acids and Risk of Maternal Gestational Diabetes and Adverse Growth Patterns in Offspring

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Measurement of Serum Sulfur-Containing Amino Acids
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
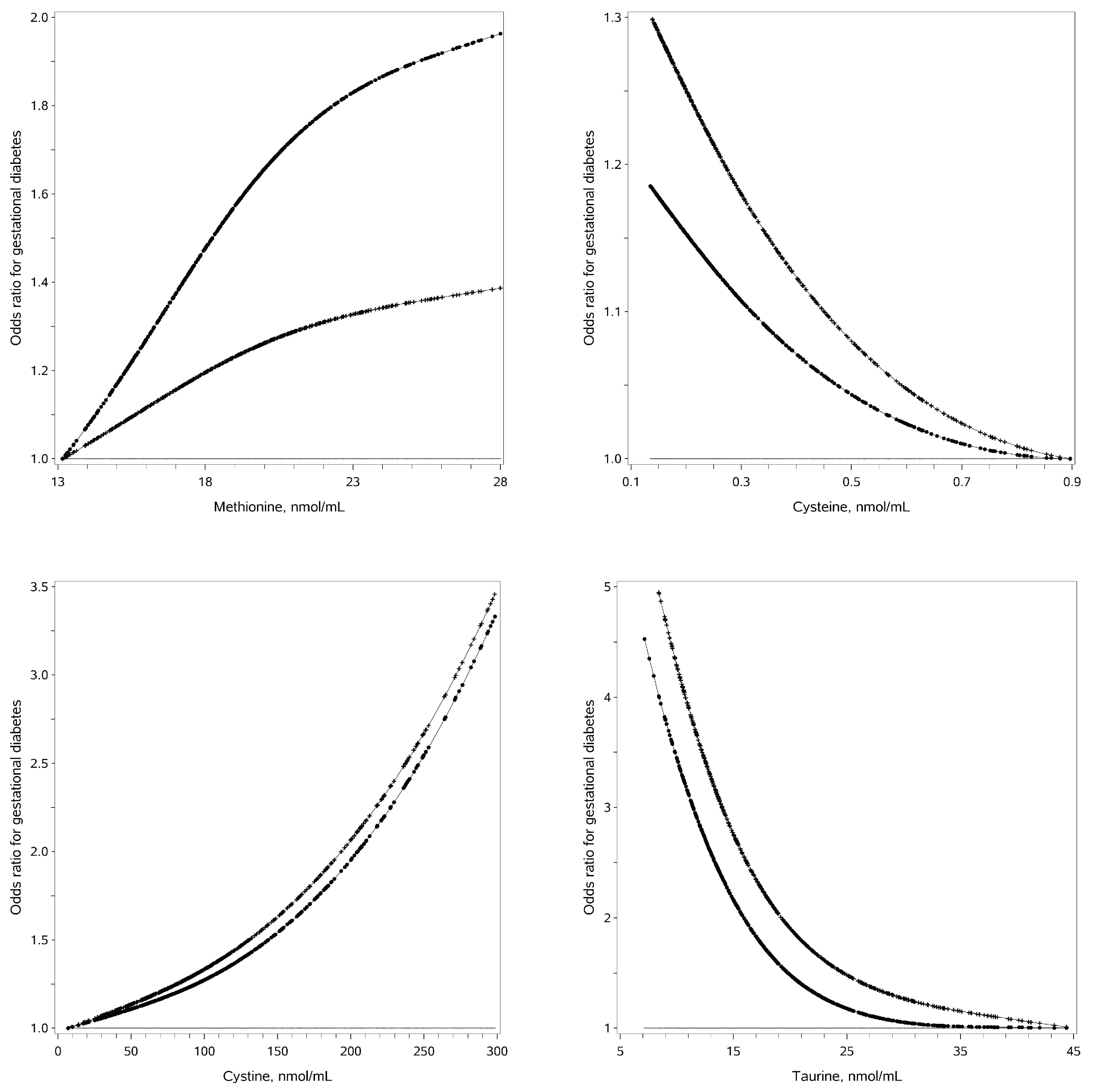
3.2. Associations of Serum SAAs with GDM
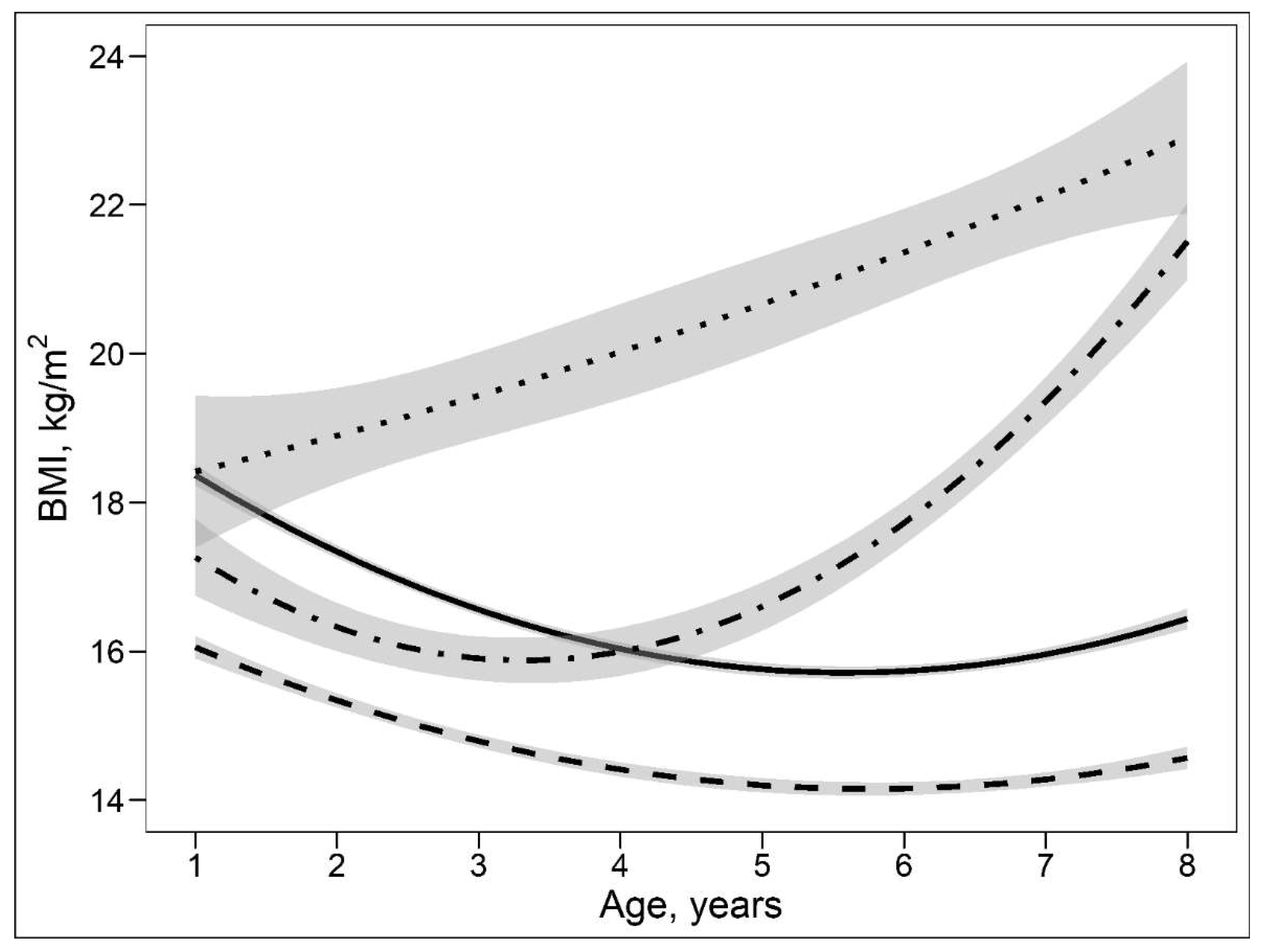
3.3. Characteristics of Offspring and Mothers by Different Growth Patterns from 1 to 8 Years of Age
3.4. Associations of Maternal Serum SAAs with POGP and LOGP in Offspring
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Li, N.; Chivese, T.; Werfalli, M.; Sun, H.; Yuen, L.; Hoegfeldt, C.A.; Elise Powe, C.; Immanuel, J.; Karuranga, S.; et al. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res. Clin. Pract. 2022, 183, 109050. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational diabetes and the risk of cardiovascular disease in women: A systematic review and meta-analysis. Diabetologia 2019, 62, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Song, C.; Li, C.; Liu, P.; Sun, Z.; Yang, X. Increased risk of cardiovascular disease in women with prior gestational diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2018, 140, 324–338. [Google Scholar] [CrossRef] [PubMed]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef]
- Song, C.; Lyu, Y.; Li, C.; Liu, P.; Li, J.; Ma, R.C.; Yang, X. Long-term risk of diabetes in women at varying durations after gestational diabetes: A systematic review and meta-analysis with more than 2 million women. Obes. Rev. 2018, 19, 421–429. [Google Scholar] [CrossRef]
- Gao, M.; Cao, S.; Li, N.; Liu, J.; Lyu, Y.; Li, J.; Yang, X. Risks of overweight in the offspring of women with gestational diabetes at different developmental stages: A meta-analysis with more than half a million offspring. Obes. Rev. 2022, 23, e13395. [Google Scholar] [CrossRef]
- Nijs, H.; Benhalima, K. Gestational Diabetes Mellitus and the Long-Term Risk for Glucose Intolerance and Overweight in the Offspring: A Narrative Review. J. Clin. Med. 2020, 9, 599. [Google Scholar] [CrossRef]
- Song, C.; Li, J.; Leng, J.; Ma, R.C.; Yang, X. Lifestyle intervention can reduce the risk of gestational diabetes: A meta-analysis of randomized controlled trials. Obes. Rev. 2016, 17, 960–969. [Google Scholar] [CrossRef]
- Brosnan, J.T.; Brosnan, M.E. The sulfur-containing amino acids: An overview. J. Nutr. 2006, 136, 1636s–1640s. [Google Scholar] [CrossRef]
- Hill, C.R.; Shafaei, A.; Balmer, L.; Lewis, J.R.; Hodgson, J.M.; Millar, A.H.; Blekkenhorst, L.C. Sulfur compounds: From plants to humans and their role in chronic disease prevention. Crit. Rev. Food. Sci. Nutr. 2022, 1–23. [Google Scholar] [CrossRef]
- Barbosa, P.; Melnyk, S.; Bennuri, S.C.; Delhey, L.; Reis, A.; Moura, G.R.; Børsheim, E.; Rose, S.; Carvalho, E. Redox Imbalance and Methylation Disturbances in Early Childhood Obesity. Oxid. Med. Cell. Longev. 2021, 2021, 2207125. [Google Scholar] [CrossRef] [PubMed]
- Go, Y.M.; Jones, D.P. Cysteine/cystine redox signaling in cardiovascular disease. Free Radic. Biol. Med. 2011, 50, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Yun, K.U.; Ryu, C.S.; Oh, J.M.; Kwak, H.C.; Lee, J.Y.; Park, S.K.; Kim, B.H.; Oh, S.J.; Kim, S.K. Alterations in hepatic metabolism of sulfur amino acids in non-obese type-2 diabetic Goto-Kakizaki rats. Chem. Biol. Interact. 2013, 204, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Yun, K.U.; Ryu, C.S.; Lee, J.Y.; Noh, J.R.; Lee, C.H.; Lee, H.S.; Kang, J.S.; Park, S.K.; Kim, B.H.; Kim, S.K. Hepatic metabolism of sulfur amino acids in db/db mice. Food. Chem. Toxicol. 2013, 53, 180–186. [Google Scholar] [CrossRef]
- Fiehn, O.; Garvey, W.T.; Newman, J.W.; Lok, K.H.; Hoppel, C.L.; Adams, S.H. Plasma metabolomic profiles reflective of glucose homeostasis in non-diabetic and type 2 diabetic obese African-American women. PLoS ONE 2010, 5, e15234. [Google Scholar] [CrossRef]
- Barker, D.J. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef]
- Nehring, I.; Chmitorz, A.; Reulen, H.; von Kries, R.; Ensenauer, R. Gestational diabetes predicts the risk of childhood overweight and abdominal circumference independent of maternal obesity. Diabet. Med. 2013, 30, 1449–1456. [Google Scholar] [CrossRef]
- Pham, M.T.; Brubaker, K.; Pruett, K.; Caughey, A.B. Risk of childhood obesity in the toddler offspring of mothers with gestational diabetes. Obstet. Gynecol. 2013, 121, 976–982. [Google Scholar] [CrossRef]
- Liu, J.X.; Liu, J.H.; Frongillo, E.A.; Boghossian, N.S.; Cai, B.; Hazlett, L.J. Body mass index trajectories during infancy and pediatric obesity at 6 years. Ann. Epidemiol. 2017, 27, 708–715.e701. [Google Scholar] [CrossRef]
- Tu, A.W.; Mâsse, L.C.; Lear, S.A.; Gotay, C.C.; Richardson, C.G. Body mass index trajectories from ages 1 to 20: Results from two nationally representative canadian longitudinal cohorts. Obesity 2015, 23, 1703–1711. [Google Scholar] [CrossRef]
- Leng, J.; Shao, P.; Zhang, C.; Tian, H.; Zhang, F.; Zhang, S.; Dong, L.; Li, L.; Yu, Z.; Chan, J.C.; et al. Prevalence of gestational diabetes mellitus and its risk factors in Chinese pregnant women: A prospective population-based study in Tianjin, China. PLoS ONE 2015, 10, e0121029. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huo, X.; Cao, Y.F.; Li, S.N.; Du, Z.; Shao, P.; Leng, J.; Zhang, C.; Sun, X.Y.; Ma, R.C.W.; et al. Bile acid metabolites in early pregnancy and risk of gestational diabetes in Chinese women: A nested case-control study. EBioMedicine 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.; Hod, M.; Kitzmiler, J.L.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Li, J.; Wang, H.; Liu, J.; Li, W.; Yang, K.; Huo, X.; Leng, J.; Yu, Z.; Hu, G.; et al. Branched-Chain Amino Acids and Their Interactions with Lipid Metabolites for Increased Risk of Gestational Diabetes. J. Clin. Endocrinol. Metab. 2022, 107, e3058–e3065. [Google Scholar] [CrossRef] [PubMed]
- Huo, X.; Li, J.; Cao, Y.F.; Li, S.N.; Shao, P.; Leng, J.; Li, W.; Liu, J.; Yang, K.; Ma, R.C.W.; et al. Trimethylamine N-Oxide Metabolites in Early Pregnancy and Risk of Gestational Diabetes: A Nested Case-Control Study. J. Clin. Endocrinol. Metab. 2019, 104, 5529–5539. [Google Scholar] [CrossRef]
- Liu, J.; Li, J.; Li, S.; Leng, J.; Li, W.; Yang, W.; Huo, X.; Chen, L.; Ma, R.C.W.; Hu, G.; et al. Circulating Lysophosphatidylcholines in Early Pregnancy and Risk of Gestational Diabetes in Chinese Women. J. Clin. Endocrinol. Metab. 2020, 105, dgaa058. [Google Scholar] [CrossRef]
- Nagin, D.S. Group-based trajectory modeling: An overview. Ann. Nutr. Metab. 2014, 65, 205–210. [Google Scholar] [CrossRef]
- Kwak, H.C.; Kim, Y.M.; Oh, S.J.; Kim, S.K. Sulfur amino acid metabolism in Zucker diabetic fatty rats. Biochem. Pharmacol. 2015, 96, 256–266. [Google Scholar] [CrossRef]
- Alqudah, A.; Wedyan, M.; Qnais, E.; Jawarneh, H.; McClements, L. Plasma Amino Acids Metabolomics’ Important in Glucose Management in Type 2 Diabetes. Front. Pharmacol. 2021, 12, 695418. [Google Scholar] [CrossRef]
- Liu, P.J.; Liu, Y.; Ma, L.; Liu, L.; Hu, T.; An, Z.; Yao, A.M.; Xia, L.Y. The relationship between plasma taurine levels in early pregnancy and later gestational diabetes mellitus risk in Chinese pregnant women. Sci. Rep. 2021, 11, 7993. [Google Scholar] [CrossRef]
- Mukwevho, E.; Ferreira, Z.; Ayeleso, A. Potential role of sulfur-containing antioxidant systems in highly oxidative environments. Molecules 2014, 19, 19376–19389. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Li, Y.Z.; Li, R.; Lan, L.; Li, C.L.; Huang, M.; Shi, D.; Feng, R.N.; Sun, C.H. Dietary Sulfur-Containing Amino Acids Are Associated with Higher Prevalence of Overweight/Obesity in Northern Chinese Adults, an Internet-Based Cross-Sectional Study. Ann. Nutr. Metab. 2018, 73, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Korai, M.; Kitazato, K.T.; Tada, Y.; Miyamoto, T.; Shimada, K.; Matsushita, N.; Kanematsu, Y.; Satomi, J.; Hashimoto, T.; Nagahiro, S. Hyperhomocysteinemia induced by excessive methionine intake promotes rupture of cerebral aneurysms in ovariectomized rats. J. Neuroinflammation 2016, 13, 165. [Google Scholar] [CrossRef]
- Rosa, F.T.; Freitas, E.C.; Deminice, R.; Jordão, A.A.; Marchini, J.S. Oxidative stress and inflammation in obesity after taurine supplementation: A double-blind, placebo-controlled study. Eur. J. Nutr. 2014, 53, 823–830. [Google Scholar] [CrossRef]
- Wang, X.; Martinez, M.P.; Chow, T.; Xiang, A.H. BMI growth trajectory from ages 2 to 6 years and its association with maternal obesity, diabetes during pregnancy, gestational weight gain, and breastfeeding. Pediatr. Obes 2020, 15, e12579. [Google Scholar] [CrossRef]
- Kwon, S.; Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Levy, S.M. Association between body mass index percentile trajectories in infancy and adiposity in childhood and early adulthood. Obesity 2017, 25, 166–171. [Google Scholar] [CrossRef]
- Ziyab, A.H.; Karmaus, W.; Kurukulaaratchy, R.J.; Zhang, H.; Arshad, S.H. Developmental trajectories of Body Mass Index from infancy to 18 years of age: Prenatal determinants and health consequences. J. Epidemiol. Community Health 2014, 68, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Ma, R.C.; Tutino, G.E.; Lillycrop, K.A.; Hanson, M.A.; Tam, W.H. Maternal diabetes, gestational diabetes and the role of epigenetics in their long term effects on offspring. Prog. Biophys. Mol. Biol. 2015, 118, 55–68. [Google Scholar] [CrossRef]
- Dudley, K.J.; Sloboda, D.M.; Connor, K.L.; Beltrand, J.; Vickers, M.H. Offspring of mothers fed a high fat diet display hepatic cell cycle inhibition and associated changes in gene expression and DNA methylation. PLoS ONE 2011, 6, e21662. [Google Scholar] [CrossRef]
- Lillycrop, K.A.; Phillips, E.S.; Jackson, A.A.; Hanson, M.A.; Burdge, G.C. Dietary protein restriction of pregnant rats induces and folic acid supplementation prevents epigenetic modification of hepatic gene expression in the offspring. J. Nutr. 2005, 135, 1382–1386. [Google Scholar] [CrossRef]
- Strakovsky, R.S.; Zhang, X.; Zhou, D.; Pan, Y.X. Gestational high fat diet programs hepatic phosphoenolpyruvate carboxykinase gene expression and histone modification in neonatal offspring rats. J. Physiol. 2011, 589, 2707–2717. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, J.; Zhang, C.; Liu, G.; Leng, J.; Wang, L.; Li, W.; Yu, Z.; Hu, G.; Chan, J.C.N.; et al. Effects of Lifestyle Intervention of Maternal Gestational Diabetes Mellitus on Offspring Growth Pattern Before Two Years of Age. Diabetes Care 2021, 44, e42–e44. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Yang, Y.; Cui, D.; Li, C.; Ma, R.C.W.; Li, J.; Yang, X. Effects of lifestyle intervention on long-term risk of diabetes in women with prior gestational diabetes: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2021, 22, e13122. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Non-GDM (n = 243) | GDM (n = 243) | p |
|---|---|---|---|
| At registration | |||
| Gestational weeks | 10.1 ± 2.0 | 10.1 ± 2.1 | 0.798 * |
| Age, year | 29.2 ± 3.3 | 29.2 ± 2.7 | - |
| Height, cm | 163.2 ± 4.6 | 163.1 ± 5.0 | 0.950 * |
| Weight, kg | 58.2 ± 9.6 | 63.7 ± 10.5 | <0.001 * |
| BMI, kg/m2 | 21.8 ± 3.4 | 23.9 ± 3.6 | <0.001 * |
| BMI in category | <0.001 ** | ||
| ≥24.0–<28.0 | 45 (18.5) | 77 (31.7) | |
| ≥28.0 | 12 (4.9) | 31 (12.8) | |
| Systolic blood pressure, mmHg | 104.0 ± 10.5 | 108.3 ± 10.5 | <0.001 * |
| Diastolic blood pressure, mmHg | 67.9 ± 7.7 | 70.6 ± 8.0 | <0.001 * |
| Han nationality | 234 (96.3) | 238 (98.0) | 0.285 ** |
| Education > 12 year | 132 (54.3) | 135 (55.6) | 0.780 ** |
| Parity ≥ 1 | 12 (4.9) | 14 (5.8) | 0.683 ** |
| Family history of diabetes | 14 (5.8) | 30 (12.4) | 0.014 ** |
| Smoking before pregnancy | 9 (3.7) | 10 (4.1) | 0.815 ** |
| Drinking before pregnancy | 57 (23.5) | 72 (29.6) | 0.120 ** |
| Serum sulfur-containing amino acids, nmol/mL | |||
| Methionine | 18.8 (16.4–21.0) | 19.3 (16.9–21.8) | 0.060 * |
| Cysteine | 0.35 (0.20–0.82) | 0.30 (0.21–0.66) | 0.359 * |
| Cystine | 91.1 (66.9–129.9) | 111.4 (68.8–187.2) | 0.001 * |
| Taurine | 21.3 (15.8–27.5) | 17.7 (12.8–22.4) | <0.001 * |
| At the time of GCT | |||
| Smoking before and during pregnancy | 9 (3.7) | 11 (4.5) | 0.637 ** |
| Drinking before and during pregnancy | 57 (23.5) | 73 (30.0) | 0.099 ** |
| Weight gain to GCT, kg | 8.7 ± 3.2 | 8.4 ± 3.6 | 0.128 * |
| OR (95%CI) | p | |
|---|---|---|
| Model 1 | ||
| Methionine, nmol/mL | ||
| <20.5 | 1.00 | |
| ≥20.5 | 1.71 (1.15–2.55) | 0.0086 |
| Cysteine, nmol/mL | ||
| >0.38 | 1.00 | |
| ≤0.38 | 1.31 (0.91–1.88) | 0.1453 |
| Cystine, nmol/mL | ||
| <150 | 1.00 | |
| ≥150 | 2.50 (1.61–3.88) | <0.0001 |
| Taurine, nmol/mL | ||
| >21.9 | 1.00 | |
| ≤21.9 | 1.98 (1.35–2.89) | 0.0005 |
| Model 2 | ||
| Methionine, nmol/mL | ||
| <20.5 | 1.00 | |
| ≥20.5 | 1.60 (1.04–2.48) | 0.0341 |
| Cysteine, nmol/mL | ||
| >0.38 | 1.00 | |
| ≤0.38 | 1.52 (1.01–2.27) | 0.0428 |
| Cystine, nmol/mL | ||
| <150 | 1.00 | |
| ≥150 | 2.58 (1.58–4.21) | 0.0001 |
| Taurine, nmol/mL | ||
| >21.9 | 1.00 | |
| ≤21.9 | 2.14 (1.41–3.26) | 0.0004 |
| Model 3 | ||
| Methionine, nmol/mL | ||
| <20.5 | 1.00 | |
| ≥20.5 | 1.92 (1.18–3.13) | 0.0084 |
| Cystine, nmol/mL | ||
| <150 | 1.00 | |
| ≥150 | 2.69 (1.59–4.53) | 0.0002 |
| Taurine, nmol/mL | ||
| >21.9 | 1.00 | |
| ≤21.9 | 2.61 (1.64–4.16) | <0.0001 |
| Characteristics | Normal or Persistent Lean Growth Pattern (n = 353) | Persistent Obesity Growth Pattern (n = 23) | Late Obesity Growth Pattern (n = 25) | p-Value |
|---|---|---|---|---|
| At registration | ||||
| Gestational weeks | 10.2 ± 2.0 | 9.9 ± 2.0 | 9.4 ± 1.9 | 0.1725 * |
| Age, year | 29.3 ± 3.0 | 28.7 ± 2.3 | 29.8 ± 3.4 | 0.4406 * |
| Height, cm | 163.3 ± 4.7 | 162.0 ± 4.9 | 162.2 ± 5.9 | 0.2928 * |
| Weight, kg | 60.5 ± 10.4 | 67.3 ± 11.8 | 63.8 ± 8.3 | 0.0040 * |
| BMI, kg/m2 | 22.7 ± 3.6 | 25.6 ± 4.3 | 24.2 ± 2.4 | 0.0001 * |
| BMI in category | <0.0001 ** | |||
| ≥24.0–<28.0 | 87 (24.7) | 6 (26.1) | 15 (60.0) | |
| ≥28.0 | 27 (7.7) | 8 (34.8) | 0 (0.0) | |
| Systolic blood pressure, mmHg | 106.1 ± 10.8 | 105.7 ± 10.8 | 106.6 ± 12.4 | 0.9550 * |
| Diastolic blood pressure, mmHg | 69.0 ± 8.1 | 70.2 ± 7.6 | 69.8 ± 8.4 | 0.7355 * |
| Han nationality | 343 (97.2) | 22 (95.7) | 24 (96.0) | 0.7264 ** |
| Education >12 year | 202 (57.2) | 10 (43.5) | 16 (64.0) | 0.3299 ** |
| Parity ≥1 | 13 (3.7) | 0 (0.0) | 4 (16.0) | 0.0306 ** |
| Family history of diabetes | 27 (7.7) | 2 (8.7) | 4 (16.0) | 0.2417 ** |
| Smoking before pregnancy | 9 (3.7) | 2 (8.7) | 2 (8.0) | 0.1315 ** |
| Drinking before pregnancy | 91 (25.8) | 7 (30.4) | 6 (24.0) | 0.8626 ** |
| Serum sulfur-containing amino acids, nmol/mL | ||||
| Methionine | 19.1 (16.7–21.1) | 21.4 (17.6–22.6) | 18.5 (16.0–22.0) | 0.2373 * |
| Cysteine | 0.31 (0.20–0.77) | 0.24 (0.21–0.52) | 0.32 (0.22–0.45) | 0.7154 * |
| Cystine | 99.0 (69.8–153.9) | 151.5 (75.5–221.4) | 85.9 (62.0–206.8) | 0.2016 * |
| Taurine | 19.4 (13.6–25.5) | 17.5 (11.8–20.1) | 17.0 (14.1–20.4) | 0.0491 * |
| During pregnancy | ||||
| Smoking during pregnancy | 1 (0.3) | 1 (4.4) | 0 (0.0) | 0.1153 ** |
| Smoking before and during pregnancy | 11 (3.1) | 3 (13.0) | 2 (8.0) | 0.0319 ** |
| Drinking during pregnancy | 2 (0.6) | 0 (0.0) | 0 (0.0) | 1.0000 ** |
| Drinking before and during pregnancy | 91 (25.8) | 7 (30.4) | 6 (24.0) | 0.8626 ** |
| Gestational diabetes mellitus | 168 (47.6) | 14 (60.9) | 18 (72.0) | 0.0343 ** |
| Gestational weeks at delivery | 39.0 ± 1.7 | 39.3 ± 1.4 | 38.6 ± 1.2 | 0.3441 * |
| Persistent Obesity Growth Pattern | Late Obesity Growth Pattern | |||
|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | |
| Model 1 | ||||
| Methionine, nmol/mL | ||||
| <20.5 | 1.00 | 1.00 | ||
| ≥20.5 | 2.20 (0.94–5.14) | 0.0682 | 1.14 (0.49–2.64) | 0.7699 |
| Cysteine, nmol/mL | ||||
| >0.38 | 1.00 | 1.00 | ||
| ≤0.38 | 1.47 (0.61–3.55) | 0.3947 | 1.17 (0.51–2.69) | 0.7036 |
| Cystine, nmol/mL | ||||
| <150 | 1.00 | 1.00 | ||
| ≥150 | 3.05 (1.30–7.15) | 0.0103 | 1.32 (0.55–3.15) | 0.5380 |
| Taurine, nmol/mL | ||||
| >21.9 | 1.00 | 1.00 | ||
| ≤21.9 | 4.23 (1.23–14.50) | 0.0218 | 2.54 (0.93–6.92) | 0.0689 |
| Model 2 | ||||
| Methionine, nmol/mL | ||||
| <20.5 | 1.00 | 1.00 | ||
| ≥20.5 | 1.54 (0.63–3.77) | 0.3428 | 1.04 (0.42–2.53) | 0.9391 |
| Cysteine, nmol/mL | ||||
| >0.38 | 1.00 | 1.00 | ||
| ≤0.38 | 1.48 (0.59–3.69) | 0.4019 | 1.08 (0.45–2.57) | 0.8621 |
| Cystine, nmol/mL | ||||
| <150 | 1.00 | 1.00 | ||
| ≥150 | 2.66 (1.10–6.45) | 0.0304 | 0.96 (0.38–2.43) | 0.9277 |
| Taurine, nmol/mL | ||||
| >21.9 | 1.00 | 1.00 | ||
| ≤21.9 | 3.85 (1.10–13.44) | 0.0344 | 2.41 (0.87–6.70) | 0.0927 |
| Model 3 | ||||
| Cystine, nmol/mL | ||||
| <150 | 1.00 | 1.00 | ||
| ≥150 | 2.68 (1.10–6.54) | 0.0308 | 0.98 (0.39–2.49) | 0.9661 |
| Taurine, nmol/mL | ||||
| >21.9 | 1.00 | 1.00 | ||
| ≤21.9 | 3.89 (1.10–13.71) | 0.0345 | 2.40 (0.86–6.70) | 0.0932 |
| Model 4 | ||||
| Cystine, nmol/mL | ||||
| <150 | 1.00 | 1.00 | ||
| ≥150 | 2.79 (1.09–7.17) | 0.0328 | 0.87 (0.34–2.23) | 0.7756 |
| Taurine, nmol/mL | ||||
| >21.9 | 1.00 | 1.00 | ||
| ≤21.9 | 3.92 (1.11–13.89) | 0.0340 | 2.26 (0.81–6.32) | 0.1192 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, N.; Li, J.; Wang, H.; Qiao, Y.; Li, W.; Gao, M.; Liu, E.; Yu, Z.; Hu, G.; Fang, Z.; et al. Serum Sulfur-Containing Amino Acids and Risk of Maternal Gestational Diabetes and Adverse Growth Patterns in Offspring. Nutrients 2023, 15, 4089. https://doi.org/10.3390/nu15184089
Li N, Li J, Wang H, Qiao Y, Li W, Gao M, Liu E, Yu Z, Hu G, Fang Z, et al. Serum Sulfur-Containing Amino Acids and Risk of Maternal Gestational Diabetes and Adverse Growth Patterns in Offspring. Nutrients. 2023; 15(18):4089. https://doi.org/10.3390/nu15184089
Chicago/Turabian StyleLi, Ninghua, Jing Li, Hui Wang, Yijuan Qiao, Weiqin Li, Ming Gao, Enqing Liu, Zhijie Yu, Gang Hu, Zhongze Fang, and et al. 2023. "Serum Sulfur-Containing Amino Acids and Risk of Maternal Gestational Diabetes and Adverse Growth Patterns in Offspring" Nutrients 15, no. 18: 4089. https://doi.org/10.3390/nu15184089
APA StyleLi, N., Li, J., Wang, H., Qiao, Y., Li, W., Gao, M., Liu, E., Yu, Z., Hu, G., Fang, Z., Leng, J., & Yang, X. (2023). Serum Sulfur-Containing Amino Acids and Risk of Maternal Gestational Diabetes and Adverse Growth Patterns in Offspring. Nutrients, 15(18), 4089. https://doi.org/10.3390/nu15184089