
Dietary Diversity Changes and Cognitive Frailty in Chinese Older Adults: A Prospective Community-Based Cohort Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Definitions of DDS Change Patterns
2.3. Assessment of CF
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
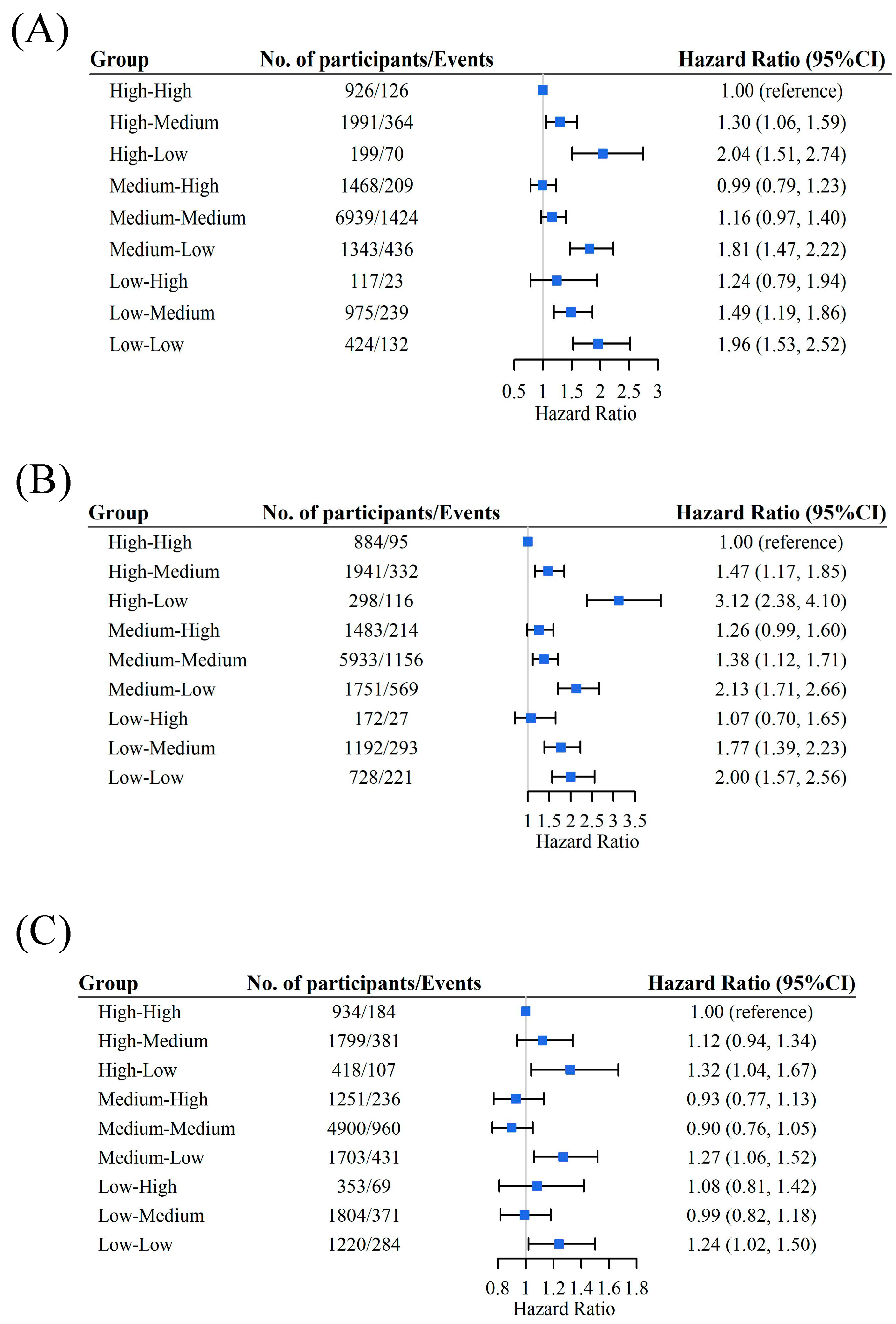
3.2. Relative DDS Change Patterns and CF
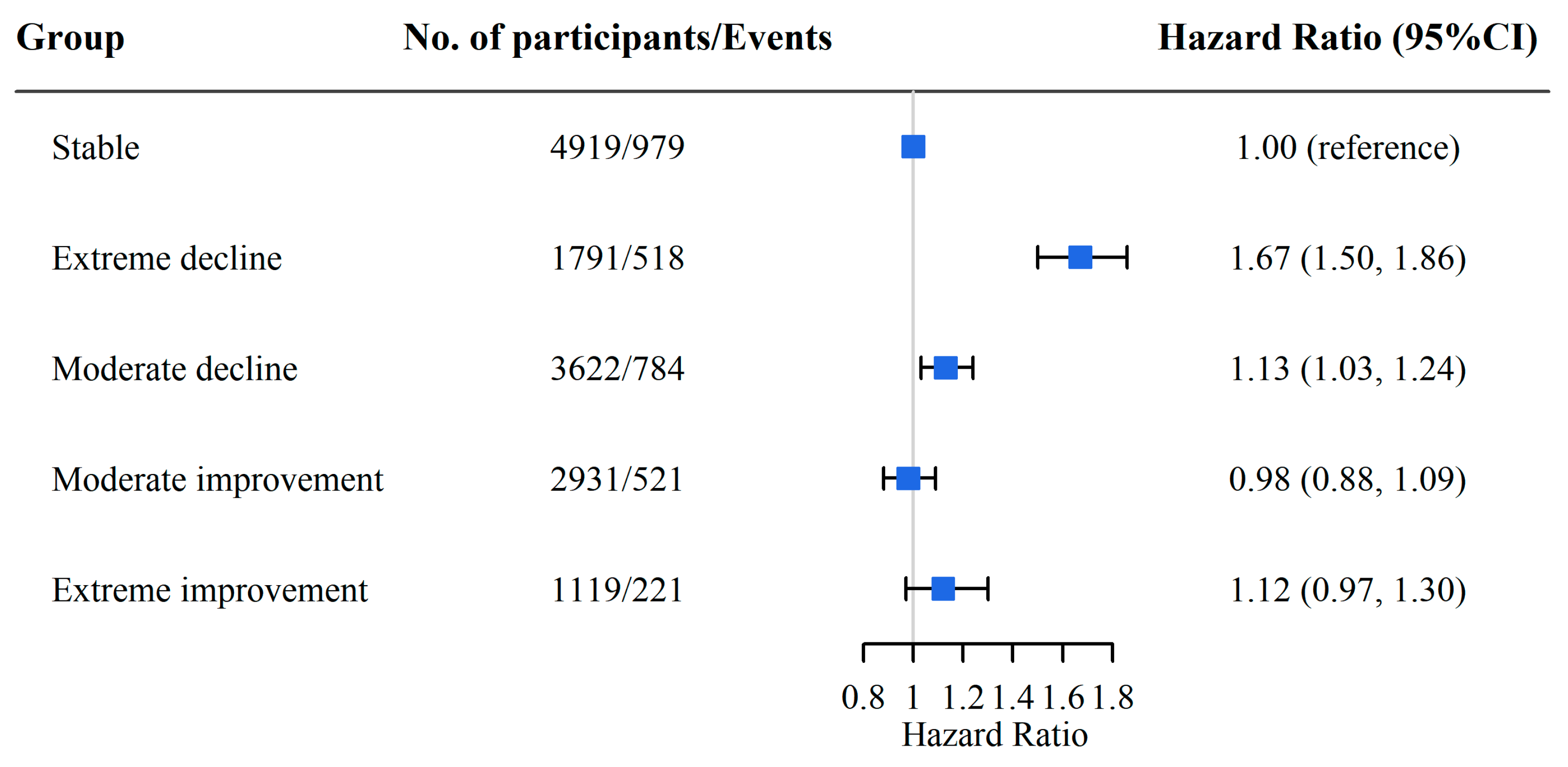
3.3. Absolute DDS Change Patterns and CF
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; Abellan van Kan, G.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Nyunt, M.S.Z.; Gao, Q.; Feng, L.; Lee, T.S.; Tsoi, T.; Chong, M.S.; Lim, W.S.; Collinson, S.; Yap, P.; et al. Physical Frailty, Cognitive Impairment, and the Risk of Neurocognitive Disorder in the Singapore Longitudinal Ageing Studies. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Zin Nyunt, M.S.; Gao, Q.; Feng, L.; Yap, K.B.; Ng, T.P. Cognitive Frailty and Adverse Health Outcomes: Findings From the Singapore Longitudinal Ageing Studies (SLAS). J. Am. Med. Dir. Assoc. 2017, 18, 252–258. [Google Scholar] [CrossRef]
- Esteban-Cornejo, I.; Cabanas-Sánchez, V.; Higueras-Fresnillo, S.; Ortega, F.B.; Kramer, A.F.; Rodriguez-Artalejo, F.; Martinez-Gomez, D. Cognitive Frailty and Mortality in a National Cohort of Older Adults: The Role of Physical Activity. Mayo Clin. Proc. 2019, 94, 1180–1189. [Google Scholar] [CrossRef]
- Liu, L.K.; Chen, C.H.; Lee, W.J.; Wu, Y.H.; Hwang, A.C.; Lin, M.H.; Shimada, H.; Peng, L.N.; Loh, C.H.; Arai, H.; et al. Cognitive Frailty and Its Association with All-Cause Mortality Among Community-Dwelling Older Adults in Taiwan: Results from I-Lan Longitudinal Aging Study. Rejuvenation Res. 2018, 21, 510–517. [Google Scholar] [CrossRef]
- Solfrizzi, V.; Scafato, E.; Lozupone, M.; Seripa, D.; Giannini, M.; Sardone, R.; Bonfiglio, C.; Abbrescia, D.I.; Galluzzo, L.; Gandin, C.; et al. Additive Role of a Potentially Reversible Cognitive Frailty Model and Inflammatory State on the Risk of Disability: The Italian Longitudinal Study on Aging. Am. J. Geriatr. Psychiatry 2017, 25, 1236–1248. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.A.; Savva, G.M.; Kenny, R.A. Frailty and cognitive impairment--a review of the evidence and causal mechanisms. Ageing Res. Rev. 2013, 12, 840–851. [Google Scholar] [CrossRef]
- Matusik, P.; Tomaszewski, K.; Chmielowska, K.; Nowak, J.; Nowak, W.; Parnicka, A.; Dubiel, M.; Gąsowski, J.; Grodzicki, T. Severe frailty and cognitive impairment are related to higher mortality in 12-month follow-up of nursing home residents. Arch. Gerontol. Geriatr. 2012, 55, 22–24. [Google Scholar] [CrossRef]
- Ruan, Q.; Yu, Z.; Chen, M.; Bao, Z.; Li, J.; He, W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res Rev. 2015, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Di Giosia, P.; Stamerra, C.A.; Giorgini, P.; Jamialahamdi, T.; Butler, A.E.; Sahebkar, A. The role of nutrition in inflammaging. Ageing Res. Rev. 2022, 77, 101596. [Google Scholar] [CrossRef]
- Shlisky, J.; Bloom, D.E.; Beaudreault, A.R.; Tucker, K.L.; Keller, H.H.; Freund-Levi, Y.; Fielding, R.A.; Cheng, F.W.; Jensen, G.L.; Wu, D.; et al. Nutritional Considerations for Healthy Aging and Reduction in Age-Related Chronic Disease. Adv. Nutr. 2017, 8, 17–26. [Google Scholar] [CrossRef]
- Kurotani, K.; Honjo, K.; Nakaya, T.; Ikeda, A.; Mizoue, T.; Sawada, N.; Tsugane, S.; Japan Public Health Center-based Prospective Study Group. Diet Quality Affects the Association between Census-Based Neighborhood Deprivation and All-Cause Mortality in Japanese Men and Women: The Japan Public Health Center-Based Prospective Study. Nutrients 2019, 11, 2194. [Google Scholar] [CrossRef]
- Otsuka, R.; Tange, C.; Nishita, Y.; Kato, Y.; Tomida, M.; Imai, T.; Ando, F.; Shimokata, H. Dietary Diversity and All-Cause and Cause-Specific Mortality in Japanese Community-Dwelling Older Adults. Nutrients 2020, 12, 1052. [Google Scholar] [CrossRef]
- Maila, G.; Audain, K.; Marinda, P.A. Association between dietary diversity, health and nutritional status of older persons in rural Zambia. S. Afr. J. Clin. Nutr. 2021, 34, 34–39. [Google Scholar] [CrossRef]
- Rezazadegan, M.; Mirjalili, F.; Jalilpiran, Y.; Aziz, M.; Jayedi, A.; Setayesh, L.; Yekaninejad, M.S.; Casazza, K.; Mirzaei, K. The Association Between Dietary Diversity Score and Odds of Diabetic Nephropathy: A Case-Control Study. Front. Nutr. 2022, 9, 767415. [Google Scholar] [CrossRef]
- Torres-Collado, L.; García-de la Hera, M.; Cano-Ibañez, N.; Bueno-Cavanillas, A.; Vioque, J. Association between Dietary Diversity and All-Cause Mortality: A Multivariable Model in a Mediterranean Population with 18 Years of Follow-Up. Nutrients 2022, 14, 1583. [Google Scholar] [CrossRef]
- Huang, W.C.; Huang, Y.C.; Lee, M.S.; Chang, H.Y.; Doong, J.Y. Frailty Severity and Cognitive Impairment Associated with Dietary Diversity in Older Adults in Taiwan. Nutrients 2021, 13, 418. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, W.T.; Wang, J.H.; Shen, D.; Zhang, P.D.; Li, Z.H.; Chen, P.L.; Zhang, X.R.; Huang, Q.M.; Zhong, W.F.; et al. Association between Dietary Diversity Changes and Cognitive Impairment among Older People: Findings from a Nationwide Cohort Study. Nutrients 2022, 14, 1251. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, X.R.; Li, Z.H.; Zhang, Y.J.; Lv, Y.B.; Wang, Z.H.; Shen, D.; Chen, P.L.; Zhong, W.F.; Huang, Q.M.; et al. Association of dietary diversity changes and mortality among older people: A prospective cohort study. Clin. Nutr. 2021, 40, 2620–2629. [Google Scholar] [CrossRef]
- Yi, Z.D., Jr.; Vlosky, D.A.; Gu, D. Healthy Longevity in China: Demographic, Socioeconomic, and Psychological Dimensions; Springer: Berlin/Heidelberg, Germany, 2008; Volume 20. [Google Scholar]
- Zhao, W.; Hasegawa, K.; Chen, J. The use of food-frequency questionnaires for various purposes in China. Public Health Nutr. 2002, 5, 829–833. [Google Scholar] [CrossRef]
- Kant, A.K.; Schatzkin, A.; Harris, T.B.; Ziegler, R.G.; Block, G. Dietary diversity and subsequent mortality in the First National Health and Nutrition Examination Survey Epidemiologic Follow-up Study. Am. J. Clin. Nutr. 1993, 57, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Kraus, V.B.; Gao, X.; Yin, Z.; Zhou, J.; Mao, C.; Duan, J.; Zeng, Y.; Brasher, M.S.; Shi, W.; et al. Higher dietary diversity scores and protein-rich food consumption were associated with lower risk of all-cause mortality in the oldest old. Clin. Nutr. 2020, 39, 2246–2254. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Gu, D.; Hayward, M.D. Early life influences on cognitive impairment among oldest old Chinese. J. Gerontol. B Psychol. Sci. Soc. Sci. 2008, 63, S25–S33. [Google Scholar] [CrossRef]
- Zhang, M.; Katzman, R.; Salmon, D.; Jin, H.; Cai, G.; Wang, Z.; Qu, G.; Grant, I.; Yu, E.; Levy, P.; et al. The prevalence of dementia and Alzheimer’s disease in Shanghai, China: Impact of age, gender, and education. Ann. Neurol. 1990, 27, 428–437. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Wang, H.Y.; Lv, X.; Du, J.; Kong, G.; Zhang, L. Age- and Gender-Specific Prevalence of Frailty and Its Outcomes in the Longevous Population: The Chinese Longitudinal Healthy Longevity Study. Front. Med. (Lausanne) 2021, 8, 719806. [Google Scholar] [CrossRef]
- Romaniuk, H.; Patton, G.C.; Carlin, J.B. Multiple imputation in a longitudinal cohort study: A case study of sensitivity to imputation methods. Am. J. Epidemiol. 2014, 180, 920–932. [Google Scholar] [CrossRef]
- Zheng, J.; Zhou, R.; Li, F.; Chen, L.; Wu, K.; Huang, J.; Liu, H.; Huang, Z.; Xu, L.; Yuan, Z.; et al. Association between dietary diversity and cognitive impairment among the oldest-old: Findings from a nationwide cohort study. Clin. Nutr. 2021, 40, 1452–1462. [Google Scholar] [CrossRef]
- Kobayashi, M.; Sasazuki, S.; Shimazu, T.; Sawada, N.; Yamaji, T.; Iwasaki, M.; Mizoue, T.; Tsugane, S. Association of dietary diversity with total mortality and major causes of mortality in the Japanese population: JPHC study. Eur. J. Clin. Nutr. 2020, 74, 54–66. [Google Scholar] [CrossRef]
- Jayanama, K.; Theou, O.; Godin, J.; Cahill, L.; Shivappa, N.; Hébert, J.R.; Wirth, M.D.; Park, Y.M.; Fung, T.T.; Rockwood, K. Relationship between diet quality scores and the risk of frailty and mortality in adults across a wide age spectrum. BMC Med. 2021, 19, 64. [Google Scholar] [CrossRef]
- Alaghehband, F.R.; Erkkilä, A.T.; Rikkonen, T.; Sirola, J.; Kröger, H.; Isanejad, M. Association of Baltic Sea and Mediterranean diets with frailty phenotype in older women, Kuopio OSTPRE-FPS study. Eur. J. Nutr. 2021, 60, 821–831. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Barnes, L.L.; Bennett, D.A.; Aggarwal, N.T. MIND diet slows cognitive decline with aging. Alzheimers Dement. 2015, 11, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Healthy Diet. Updated. 29 April 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 15 September 2022).
- Phillips, J.A. Dietary Guidelines for Americans, 2020–2025. Workplace Health Saf. 2021, 69, 395. [Google Scholar] [CrossRef] [PubMed]
- Society, C.N. Dietary Guidelines for Chinese Residents (2022). Updated 2022-04-29. Available online: http://dg.cnsoc.org/article/04/K7tlcs-UQh67DBC5XY1Jqw.html (accessed on 15 September 2022).
- Azadbakht, L.; Akbari, F.; Esmaillzadeh, A. Diet quality among Iranian adolescents needs improvement. Public Health Nutr. 2015, 18, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Khorsha, F.; Mirzababaei, A.; Togha, M.; Mirzaei, K. Association of dietary diversity score (DDS) and migraine headache severity among women. Neurol. Sci. 2021, 42, 3403–3410. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Avgerinou, C.; Iliffe, S.; Jivraj, S.; Sekiguchi, K.; Walters, K. Fruit and vegetables Consumption and Frailty: A Systematic Review. J. Nutr. Health Aging 2018, 22, 1010–1017. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Niti, M.; Kua, E.H.; Yap, K.B. Tea consumption and cognitive impairment and decline in older Chinese adults. Am. J. Clin. Nutr. 2008, 88, 224–231. [Google Scholar] [CrossRef]
- Rahman, K. Garlic and aging: New insights into an old remedy. Ageing Res. Rev. 2003, 2, 39–56. [Google Scholar] [CrossRef]
- Kouvari, M.; Tyrovolas, S.; Panagiotakos, D.B. Red meat consumption and healthy ageing: A review. Maturitas 2016, 84, 17–24. [Google Scholar] [CrossRef]
- Mulero, J.; Zafrilla, P.; Martinez-Cacha, A. Oxidative stress, frailty and cognitive decline. J. Nutr. Health Aging 2011, 15, 756–760. [Google Scholar] [CrossRef]
- Daly, R.M.; Gianoudis, J.; Prosser, M.; Kidgell, D.; Ellis, K.A.; O’Connell, S.; Nowson, C.A. The effects of a protein enriched diet with lean red meat combined with a multi-modal exercise program on muscle and cognitive health and function in older adults: Study protocol for a randomised controlled trial. Trials 2015, 16, 339. [Google Scholar] [CrossRef] [PubMed]
- de Haas, S.C.; de Jonge, E.A.; Voortman, T.; Graaff, J.S.D.; Franco, O.H.; Ikram, M.A.; Rivadeneira, F.; Kiefte-de Jong, J.C.; Schoufour, J.D. Dietary patterns and changes in frailty status: The Rotterdam study. Eur. J. Nutr. 2018, 57, 2365–2375. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics a | Total | DDS Change Patterns from Baseline to First Follow-Up | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| High to High | High to Medium | High to Low | Medium to High | Medium to Medium | Medium to Low | Low to High | Low to Medium | Low to Low | ||
| No. of participants | 14,382 | 926 | 1991 | 199 | 1468 | 6939 | 1343 | 117 | 975 | 424 |
| Age, mean (SD) | 82.3 (10.8) | 79.1 (10.6) | 81.2 (10.6) | 85.2 (11.2) | 80.3 (10.3) | 82.5 (10.9) | 84.7 (10.9) | 84.4 (11.7) | 84.0 (10.5) | 85.5 (9.9) |
| Sex | ||||||||||
| Female | 7729 (53.7) | 356 (38.4) | 913 (45.9) | 115 (57.8) | 662 (45.1) | 3829 (55.2) | 864 (64.3) | 77 (65.8) | 620 (63.6) | 293 (69.1) |
| Male | 6653 (46.3) | 570 (61.6) | 1078 (54.1) | 84 (42.2) | 806 (54.9) | 3110 (44.8) | 479 (35.7) | 40 (34.2) | 355 (36.4) | 131 (30.9) |
| Living area | ||||||||||
| Rural | 8431 (58.6) | 343 (37.0) | 959 (48.2) | 123 (61.8) | 708 (48.2) | 4269 (61.5) | 944 (70.3) | 69 (59.0) | 704 (72.2) | 312 (73.6) |
| Urban | 5951 (41.4) | 583 (63.0) | 1032 (51.8) | 76 (38.2) | 760 (51.8) | 2670 (38.5) | 399 (29.7) | 48 (41.0) | 271 (27.8) | 112 (26.4) |
| Marital status | ||||||||||
| Married | 6086 (42.3) | 541 (58.4) | 977 (49.1) | 64 (32.2) | 721 (49.1) | 2836 (40.9) | 456 (34.0) | 37 (31.6) | 328 (33.6) | 126 (29.7) |
| Not married | 8296 (57.7) | 385 (41.6) | 1014 (50.9) | 135 (67.8) | 747 (50.9) | 4103 (59.1) | 887 (66.0) | 80 (68.4) | 647 (66.4) | 298 (70.3) |
| Occupation | ||||||||||
| Farmer | 9111 (63.4) | 327 (35.3) | 1054 (52.9) | 126 (63.3) | 756 (51.5) | 4713 (67.9) | 989 (73.6) | 78 (66.7) | 743 (76.2) | 325 (76.7) |
| Other | 5271 (36.6) | 599 (64.7) | 937 (47.1) | 73 (36.7) | 712 (48.5) | 2226 (32.1) | 354 (26.4) | 39 (33.3) | 232 (23.8) | 99 (23.3) |
| Years of education, y | ||||||||||
| 0 | 8271 (57.5) | 321 (34.7) | 952 (47.8) | 118 (59.3) | 672 (45.8) | 4145 (59.7) | 942 (70.1) | 87 (74.4) | 710 (72.8) | 324 (76.4) |
| ≥1 | 6111 (42.5) | 605 (65.3) | 1039 (52.2) | 81 (40.7) | 796 (54.2) | 2794 (40.3) | 401 (29.9) | 30 (25.6) | 265 (27.2) | 100 (23.6) |
| Income source | ||||||||||
| Pension | 2930 (20.4) | 457 (49.4) | 597 (30.0) | 30 (15.1) | 453 (30.9) | 1140 (16.4) | 124 (9.2) | 17 (14.5) | 89 (9.1) | 23 (5.4) |
| Others | 11,452 (79.6) | 469 (50.6) | 1394 (70.0) | 169 (84.9) | 1015 (69.1) | 5799 (83.6) | 1219 (90.8) | 100 (85.5) | 886 (90.9) | 401 (94.6) |
| Sufficient income | ||||||||||
| Yes | 11,395 (79.2) | 856 (92.4) | 1775 (89.2) | 170 (85.4) | 1238 (84.3) | 5485 (79.0) | 978 (72.8) | 84 (71.8) | 575 (59.0) | 234 (55.2) |
| No | 2987 (20.8) | 70 (7.6) | 216 (10.8) | 29 (14.6) | 230 (15.7) | 1454 (21.0) | 365 (27.2) | 33 (28.2) | 400 (41.0) | 190 (44.8) |
| Living arrangement | ||||||||||
| Living alone/at nursing home | 2533 (17.6) | 99 (10.7) | 257 (12.9) | 37 (18.6) | 200 (13.6) | 1224 (17.6) | 280 (20.8) | 24 (20.5) | 270 (27.7) | 142 (33.5) |
| Living with family member | 11,849 (82.4) | 827 (89.3) | 1734 (87.1) | 162 (81.4) | 1268 (86.4) | 5715 (82.4) | 1063 (79.2) | 93 (79.5) | 705 (72.3) | 282 (66.5) |
| BMI, kg/m2 | 20.23 (4.3) | 21.7 (4.2) | 20.9 (4.5) | 19.9 (3.6) | 20.8 (5.3) | 20.1 (4.3) | 19.5 (3.6) | 19.7 (3.8) | 19.3 (3.5) | 18.8 (3.7) |
| Regular exercise | 5215 (36.3) | 536 (57.9) | 931 (46.8) | 90 (45.2) | 633 (43.1) | 2291 (33.0) | 375 (27.9) | 24 (20.5) | 242 (24.8) | 93 (21.9) |
| Smoking status | ||||||||||
| Current smoker | 3114 (21.7) | 247 (26.7) | 500 (25.1) | 51 (25.6) | 367 (25.0) | 1459 (21.0) | 239 (17.8) | 24 (20.5) | 178 (18.3) | 49 (11.6) |
| Former smoker | 2073 (14.4) | 184 (19.9) | 337 (16.9) | 25 (12.6) | 253 (17.2) | 945 (13.6) | 154 (11.5) | 17 (14.5) | 107 (11.0) | 51 (12.0) |
| Nonsmoker | 9195 (63.9) | 495 (53.5) | 1154 (58.0) | 123 (61.8) | 848 (57.8) | 4535 (65.4) | 950 (70.7) | 76 (65.0) | 690 (70.8) | 324 (76.4) |
| Drinking status | ||||||||||
| Current drinker | 3229 (22.5) | 308 (33.3) | 538 (27.0) | 54 (27.1) | 374 (25.5) | 1496 (21.6) | 238 (17.7) | 20 (17.1) | 155 (15.9) | 46 (10.8) |
| Former drinker | 1551 (10.8) | 105 (11.3) | 231 (11.6) | 24 (12.1) | 185 (12.6) | 710 (10.2) | 125 (9.3) | 18 (15.4) | 114 (11.7) | 39 (9.2) |
| Nondrinker | 9602 (66.8) | 513 (55.4) | 1222 (61.4) | 121 (60.8) | 909 (61.9) | 4733 (68.2) | 980 (73.0) | 79 (67.5) | 706 (72.4) | 339 (80.0) |
| Hypertension | 6503 (45.2) | 464 (50.1) | 930 (46.7) | 97 (48.7) | 703 (47.9) | 2994 (43.1) | 584 (43.5) | 66 (56.4) | 457 (46.9) | 208 (49.1) |
| Diabetes | 322 (2.2) | 25 (2.7) | 60 (3.0) | 2 (1.0) | 35 (2.4) | 159 (2.3) | 21 (1.6) | 2 (1.7) | 15 (1.5) | 3 (0.7) |
| Stroke | 668 (4.6) | 53 (5.7) | 112 (5.6) | 8 (4.0) | 80 (5.4) | 290 (4.2) | 57 (4.2) | 7 (6.0) | 41 (4.2) | 20 (4.7) |
| Heart disease | 1273 (8.9) | 121 (13.1) | 191 (9.6) | 16 (8.0) | 163 (11.1) | 545 (7.9) | 106 (7.9) | 10 (8.5) | 77 (7.9) | 44 (10.4) |
| Foods | DDS Change Patterns from Baseline to First Follow-Up | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Often to Often | Often to Occasionally | Often to Rarely | Occasionally to Often | Occasionally to Occasionally | Occasionally to Rarely | Rarely to Often | Rarely to Occasionally | Rarely to Rarely | |
| Fresh vegetables | |||||||||
| No. of CF/person-years | 2153/65,525 | 330/5468 | 182/1693 | 197/5247 | 48/1107 | 36/422 | 51/1033 | 17/241 | 9/124 |
| Incidence rate of CF | 32.9 | 60.4 | 107.5 | 37.5 | 43.4 | 85.3 | 49.4 | 70.5 | 72.6 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 1.62 (1.44, 1.82) | 2.42 (2.08, 2.82) | 1.04 (0.90, 1.20) | 1.04 (0.78, 1.39) | 2.53 (1.82, 3.51) | 1.08 (0.82, 1.43) | 1.90 (1.18, 3.07) | 1.53 (0.79, 2.94) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 1.61 (1.43, 1.81) | 2.37 (2.03, 2.76) | 1.04 (0.90, 1.21) | 1.02 (0.76, 1.36) | 2.47 (1.77, 3.43) | 1.09 (0.83, 1.44) | 1.76 (1.09, 2.85) | 1.57 (0.82, 3.03) |
| Fresh fruit | |||||||||
| No. of CF/person-years | 488/16,179 | 312/8991 | 263/4986 | 297/9610 | 451/13,593 | 411/8632 | 185/4311 | 266/7064 | 350/7495 |
| Incidence rate of CF | 30.2 | 34.7 | 52.7 | 30.9 | 33.2 | 47.6 | 42.9 | 37.7 | 46.7 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 1.08 (0.93, 1.24) | 1.51 (1.30, 1.76) | 1.02 (0.89, 1.18) | 1.05 (0.92, 1.19) | 1.39 (1.22, 1.59) | 1.32 (1.12, 1.57) | 1.20 (1.03, 1.40) | 1.38 (1.20, 1.58) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 1.11 (0.96, 1.28) | 1.59 (1.36, 1.85) | 1.08 (0.93, 1.25) | 1.14 (1.00, 1.30) | 1.52 (1.32, 1.74) | 1.38 (1.16, 1.64) | 1.30 (1.12, 1.52) | 1.49 (1.29, 1.72) |
| Tea | |||||||||
| No. of CF/person-years | 293/13,491 | 164/4813 | 354/8405 | 110/4439 | 105/3175 | 299/6852 | 191/5836 | 240/6003 | 1267/27,846 |
| Incidence rate of CF | 21.7 | 34.1 | 42.1 | 24.8 | 33.1 | 43.6 | 32.7 | 40.0 | 45.5 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 1.42 (1.18, 1.72) | 1.47 (1.26, 1.72) | 1.12 (0.90, 1.40) | 1.29 (1.03, 1.62) | 1.39 (1.18, 1.64) | 1.26 (1.05, 1.51) | 1.36 (1.15, 1.62) | 1.40 (1.23, 1.60) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 1.46 (1.20, 1.76) | 1.51 (1.29, 1.76) | 1.08 (0.86, 1.34) | 1.26 (1.00, 1.57) | 1.41 (1.20, 1.66) | 1.22 (1.01, 1.47) | 1.37 (1.16, 1.63) | 1.43 (1.25, 1.63) |
| Garlic | |||||||||
| No. of CF/person-years | 120/5695 | 257/8261 | 179/3787 | 240/8283 | 608/19,050 | 544/11,829 | 111/3388 | 404/10,050 | 560/10,517 |
| Incidence rate of CF | 21.1 | 31.1 | 47.3 | 29.0 | 31.9 | 46.0 | 32.8 | 40.2 | 53.2 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 1.28 (1.03, 1.59) | 1.71 (1.35, 2.15) | 1.23 (0.99, 1.53) | 1.15 (0.94, 1.39) | 1.54 (1.27, 1.88) | 1.32 (1.02, 1.71) | 1.34 (1.09, 1.64) | 1.63 (1.33, 1.98) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 1.33 (1.07, 1.65) | 1.79 (1.42, 2.26) | 1.24 (0.99, 1.54) | 1.20 (0.98, 1.46) | 1.60 (1.31, 1.95) | 1.31 (1.01, 1.69) | 1.38 (1.13, 1.70) | 1.66 (1.36, 2.02) |
| Beans | |||||||||
| No. of CF/person-years | 314/9510 | 553/13,234 | 139/2863 | 307/8826 | 1019/29,672 | 251/6107 | 85/1848 | 239/6256 | 116/2544 |
| Incidence rate of CF | 33.0 | 41.8 | 48.6 | 34.8 | 34.3 | 41.1 | 46 | 38.2 | 45.6 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 0.95 (0.83, 1.09) | 1.21 (0.99, 1.48) | 1.00 (0.85, 1.17) | 0.79 (0.69, 0.89) | 0.91 (0.77, 1.08) | 1.23 (0.97, 1.56) | 0.92 (0.78, 1.09) | 1.07 (0.87, 1.33) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 0.99 (0.86, 1.14) | 1.30 (1.06, 1.59) | 1.01 (0.86, 1.18) | 0.84 (0.74, 0.96) | 0.99 (0.84, 1.18) | 1.24 (0.97, 1.57) | 0.98 (0.83, 1.17) | 1.15 (0.93, 1.43) |
| Preserved vegetables | |||||||||
| No. of CF/person-years | 196/6850 | 240/8209 | 281/6280 | 150/5892 | 392/12,651 | 480/11,442 | 133/3713 | 379/10,198 | 772/15,625 |
| Incidence rate of CF | 28.6 | 29.2 | 44.7 | 25.5 | 31.0 | 42.0 | 35.8 | 37.2 | 49.4 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 0.91 (0.75, 1.10) | 1.25 (1.04, 1.50) | 0.79 (0.63, 0.97) | 0.85 (0.71, 1.01) | 0.95 (0.80, 1.12) | 0.89 (0.71, 1.11) | 0.92 (0.77, 1.09) | 1.06 (0.90, 1.24) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 0.94 (0.77, 1.13) | 1.26 (1.05, 1.52) | 0.79 (0.64, 0.98) | 0.86 (0.72, 1.02) | 0.97 (0.82, 1.15) | 0.89 (0.71, 1.11) | 0.93 (0.79, 1.11) | 1.06 (0.90, 1.24) |
| Meat | |||||||||
| No. of CF/person-years | 557/14,800 | 454/11,182 | 111/2037 | 387/10,721 | 769/25,032 | 263/5612 | 71/1891 | 228/6138 | 183/3446 |
| Incidence rate of CF | 37.6 | 40.6 | 54.5 | 36.1 | 30.7 | 46.9 | 37.5 | 37.1 | 53.1 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 1.14 (1.01, 1.30) | 1.57 (1.28, 1.92) | 1.00 (0.88, 1.14) | 0.91 (0.81, 1.01) | 1.56 (1.35, 1.81) | 1.18 (0.92, 1.51) | 1.07 (0.92, 1.25) | 1.64 (1.38, 1.93) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 1.14 (1.01, 1.29) | 1.60 (1.30, 1.97) | 1.02 (0.89, 1.16) | 0.93 (0.83, 1.04) | 1.57 (1.35, 1.83) | 1.11 (0.87, 1.43) | 1.09 (0.93, 1.27) | 1.62 (1.36, 1.92) |
| Fish | |||||||||
| No. of CF/person-years | 135/3865 | 319/8060 | 97/1900 | 173/5120 | 969/32,005 | 470/9746 | 54/1443 | 407/10,164 | 399/8556 |
| Incidence rate of CF | 34.9 | 39.6 | 51.1 | 33.8 | 30.3 | 48.2 | 37.4 | 40.0 | 46.6 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 1.07 (0.88, 1.31) | 1.23 (0.95, 1.59) | 0.90 (0.71, 1.12) | 0.84 (0.70, 1.01) | 1.17 (0.96, 1.42) | 0.99 (0.72, 1.36) | 0.95 (0.78, 1.16) | 1.16 (0.95, 1.40) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 1.10 (0.90, 1.35) | 1.32 (1.02, 1.72) | 0.91 (0.73, 1.14) | 0.89 (0.74, 1.07) | 1.25 (1.03, 1.52) | 1.03 (0.75, 1.42) | 1.03 (0.85, 1.26) | 1.25 (1.02, 1.52) |
| Eggs | |||||||||
| No. of CF/person-years | 659/15,901 | 527/13,172 | 116/2414 | 389/10,561 | 724/23,000 | 216/5418 | 95/2376 | 199/5296 | 98/2721 |
| Incidence rate of CF | 41.4 | 40.0 | 48.1 | 36.8 | 31.5 | 39.9 | 40.0 | 37.6 | 36.0 |
| HR (95%CI) (model 1) a | 1.00 (ref) | 0.93 (0.83, 1.04) | 1.37 (1.12, 1.67) | 0.91 (0.80, 1.03) | 0.76 (0.68, 0.84) | 0.96 (0.82, 1.12) | 1.04 (0.84, 1.28) | 0.93 (0.79, 1.09) | 1.01 (0.82, 1.25) |
| HR (95%CI) (model 2) b | 1.00 (ref) | 0.96 (0.85, 1.07) | 1.42 (1.16, 1.73) | 0.92 (0.81, 1.05) | 0.79 (0.71, 0.88) | 1.02 (0.87, 1.20) | 1.02 (0.82, 1.26) | 0.95 (0.81, 1.12) | 1.04 (0.84, 1.29) |
| Subgroups | DDS Change Patterns from Baseline to First Follow-Up | p for Interaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| High to High | High to Medium | High to Low | Medium to High | Medium to Medium | Medium to Low | Low to High | Low to Medium | Low to Low | ||
| Age, years | 0.221 | |||||||||
| <80 | 1.00 (ref) | 0.99 (0.57, 1.74) | 2.35 (0.92, 5.96) | 1.28 (0.74, 2.20) | 1.34 (0.82, 2.17) | 2.04 (1.17, 3.59) | 0.65 (0.09, 4.91) | 1.75 (0.95, 3.22) | 1.84 (0.85, 3.98) | |
| ≥80 | 1.00 (ref) | 1.31 (1.05, 1.63) | 2.00 (1.46, 2.73) | 0.91 (0.71, 1.16) | 1.12 (0.91, 1.37) | 1.75 (1.41, 2.18) | 1.24 (0.78, 1.97) | 1.41 (1.11, 1.79) | 1.90 (1.45, 2.49) | |
| Sex | 0.020 | |||||||||
| Female | 1.00 (ref) | 0.99 (0.77, 1.28) | 1.37 (0.96, 1.98) | 0.74 (0.56, 0.99) | 0.85 (0.68, 1.08) | 1.30 (1.02, 1.67) | 0.97 (0.59, 1.60) | 1.02 (0.78, 1.34) | 1.44 (1.07, 1.95) | |
| Male | 1.00 (ref) | 1.82 (1.30, 2.57) | 3.76 (2.27, 6.23) | 1.50 (1.04, 2.17) | 1.83 (1.33, 2.51) | 2.99 (2.09, 4.27) | 1.43 (0.51, 3.99) | 2.89 (1.95, 4.30) | 3.14 (1.95, 5.05) | |
| Living area | 0.789 | |||||||||
| Rural | 1.00 (ref) | 1.22 (0.89, 1.69) | 1.93 (1.27, 2.92) | 1.02 (0.72, 1.44) | 1.09 (0.82, 1.46) | 1.67 (1.23, 2.27) | 1.34 (0.75, 2.39) | 1.37 (0.99, 1.90) | 1.98 (1.39, 2.81) | |
| Urban | 1.00 (ref) | 1.34 (1.02, 1.74) | 2.09 (1.35, 3.23) | 0.95 (0.71, 1.28) | 1.21 (0.95, 1.55) | 1.97 (1.47, 2.63) | 1.00 (0.48, 2.08) | 1.63 (1.17, 2.29) | 1.71 (1.13, 2.58) | |
| Smoking | 0.026 | |||||||||
| Never smoker | 1.00 (ref) | 1.16 (0.91, 1.48) | 2.10 (1.48, 2.96) | 0.88 (0.67, 1.15) | 1.00 (0.80, 1.24) | 1.46 (1.14, 1.86) | 1.04 (0.62, 1.76) | 1.22 (0.94, 1.59) | 1.61 (1.20, 2.15) | |
| Current or former smoker | 1.00 (ref) | 1.57 (1.08, 2.28) | 1.75 (0.99, 3.12) | 1.22 (0.81, 1.83) | 1.61 (1.14, 2.27) | 3.03 (2.07, 4.45) | 1.81 (0.76, 4.33) | 2.33 (1.52, 3.57) | 3.28 (1.97, 5.45) | |
| Drinking | 0.145 | |||||||||
| Never drinker | 1.00 (ref) | 1.31 (1.01, 1.70) | 1.94 (1.31, 2.87) | 0.98 (0.74, 1.30) | 1.16 (0.92, 1.48) | 1.75 (1.35, 2.26) | 1.55 (0.92, 2.60) | 1.45 (1.10, 1.92) | 1.77 (1.31, 2.40) | |
| Current or former drinker | 1.00 (ref) | 1.26 (0.90, 1.76) | 2.16 (1.37, 3.41) | 1.03 (0.72, 1.47) | 1.17 (0.86, 1.58) | 1.99 (1.41, 2.81) | 0.72 (0.28, 1.81) | 1.58 (1.07, 2.32) | 3.05 (1.89, 4.90) | |
| Regular exercises | 0.179 | |||||||||
| Yes | 1.00 (ref) | 1.16 (0.86, 1.56) | 1.45 (0.91, 2.31) | 0.95 (0.69, 1.32) | 1.16 (0.89, 1.51) | 1.59 (1.16, 2.18) | 0.82 (0.20, 3.34) | 1.15 (0.78, 1.70) | 1.58 (0.96, 2.60) | |
| No | 1.00 (ref) | 1.39 (1.05, 1.85) | 2.61 (1.77, 3.87) | 1.01 (0.74, 1.38) | 1.18 (0.91, 1.54) | 1.90 (1.44, 2.52) | 1.33 (0.81, 2.19) | 1.64 (1.22, 2.20) | 2.11 (1.53, 2.91) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhong, W.-F.; Song, W.-Q.; Wang, X.-M.; Li, Z.-H.; Shen, D.; Liu, D.; Zhang, P.-D.; Shen, Q.-Q.; Liang, F.; Nan, Y.; et al. Dietary Diversity Changes and Cognitive Frailty in Chinese Older Adults: A Prospective Community-Based Cohort Study. Nutrients 2023, 15, 3784. https://doi.org/10.3390/nu15173784
Zhong W-F, Song W-Q, Wang X-M, Li Z-H, Shen D, Liu D, Zhang P-D, Shen Q-Q, Liang F, Nan Y, et al. Dietary Diversity Changes and Cognitive Frailty in Chinese Older Adults: A Prospective Community-Based Cohort Study. Nutrients. 2023; 15(17):3784. https://doi.org/10.3390/nu15173784
Chicago/Turabian StyleZhong, Wen-Fang, Wei-Qi Song, Xiao-Meng Wang, Zhi-Hao Li, Dong Shen, Dan Liu, Pei-Dong Zhang, Qiao-Qiao Shen, Fen Liang, Ying Nan, and et al. 2023. "Dietary Diversity Changes and Cognitive Frailty in Chinese Older Adults: A Prospective Community-Based Cohort Study" Nutrients 15, no. 17: 3784. https://doi.org/10.3390/nu15173784
APA StyleZhong, W.-F., Song, W.-Q., Wang, X.-M., Li, Z.-H., Shen, D., Liu, D., Zhang, P.-D., Shen, Q.-Q., Liang, F., Nan, Y., Xiang, J.-X., Chen, Z.-T., Li, C., Li, S.-T., Lv, X.-G., Lin, X.-R., Lv, Y.-B., Gao, X., Kraus, V. B., ... Mao, C. (2023). Dietary Diversity Changes and Cognitive Frailty in Chinese Older Adults: A Prospective Community-Based Cohort Study. Nutrients, 15(17), 3784. https://doi.org/10.3390/nu15173784