
Systematic Review of Management of Moderate Wasting in Children over 6 Months of Age

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
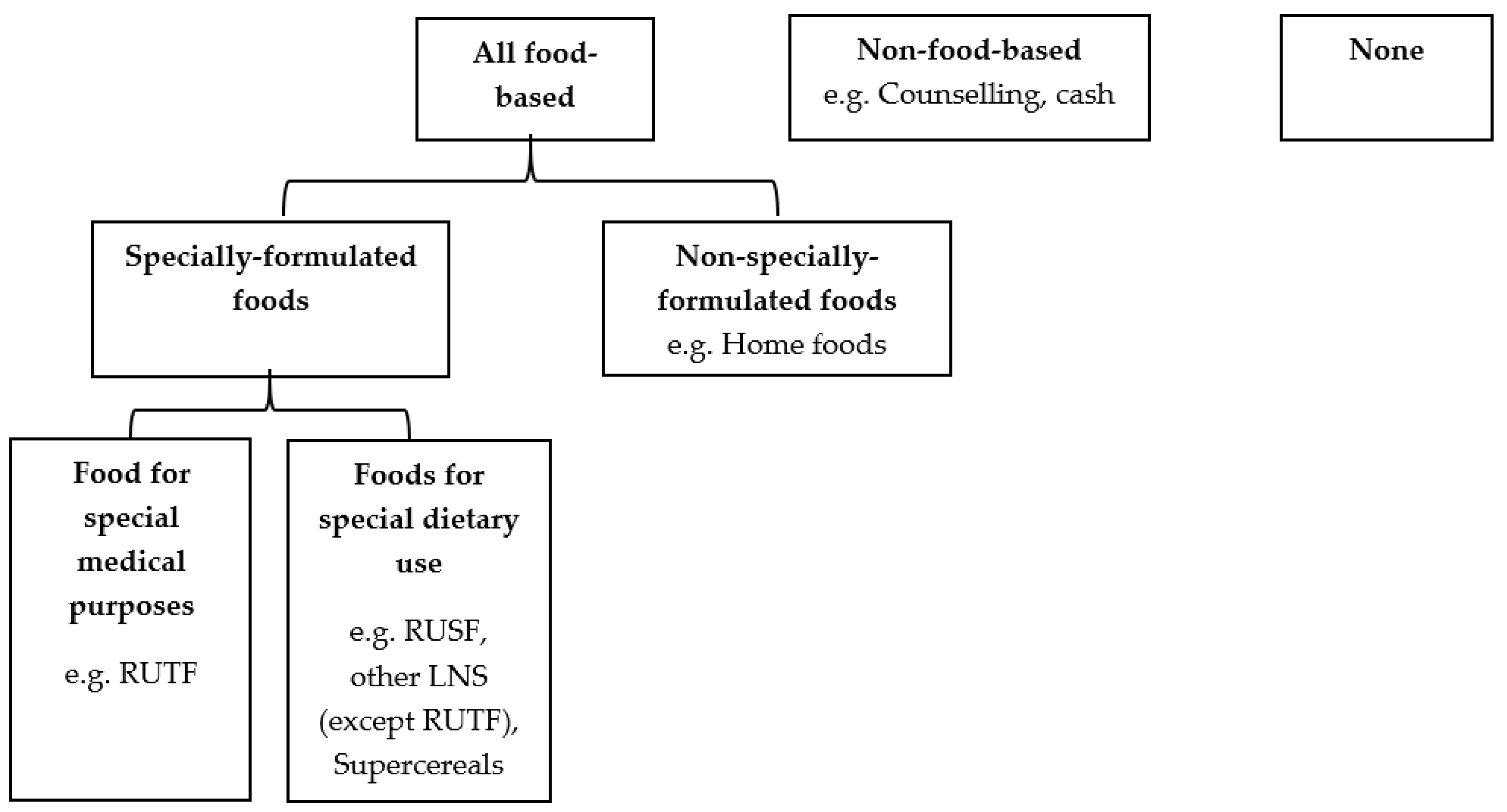
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy and Study Selection
2.3. Data Extraction
2.4. Risk of Bias (ROB) Assessment
2.5. Data Analysis
2.6. Subgroup and Sensitivity Analysis
2.7. Evidence Profiles
3. Results
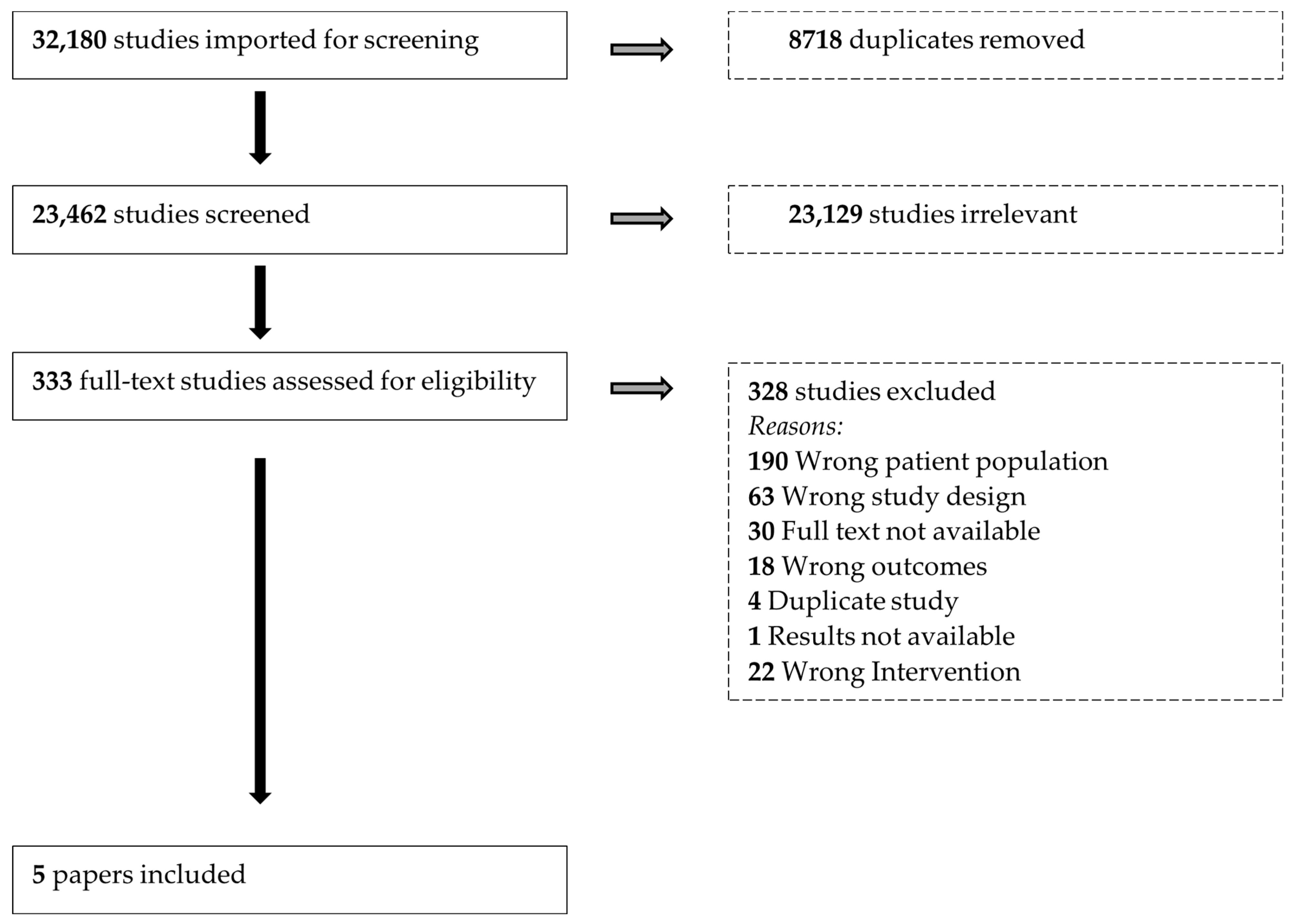
3.1. Search Results
3.2. Characteristics of Included Studies
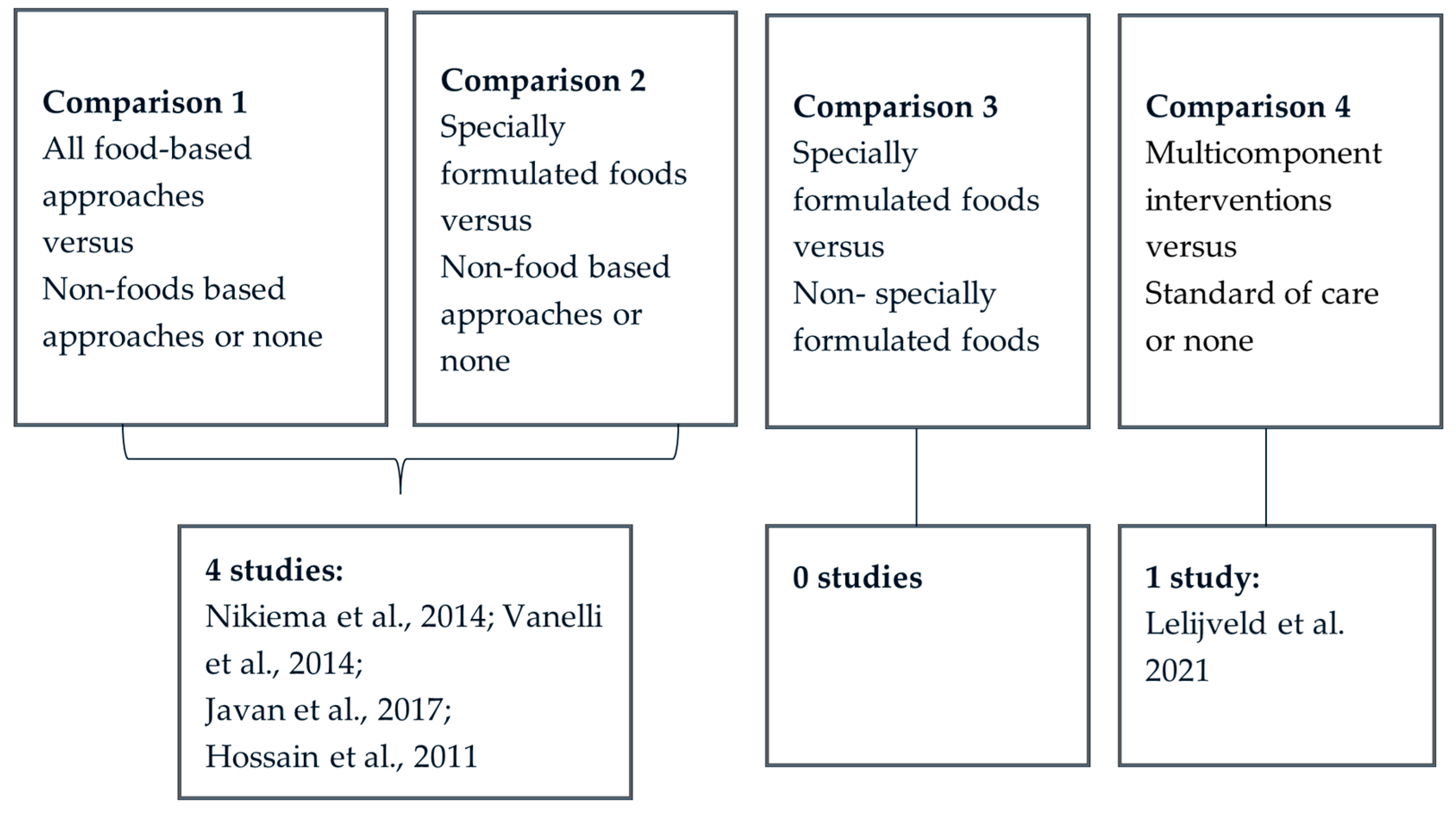
3.2.1. Comparison 2: Specially-Formulated Foods vs. Non-Food-Based or None
3.2.2. Comparison 4: Multicomponent Intervention versus Non-Food-Based or None
3.3. Quality of Included Studies
3.4. Effects of Intervention
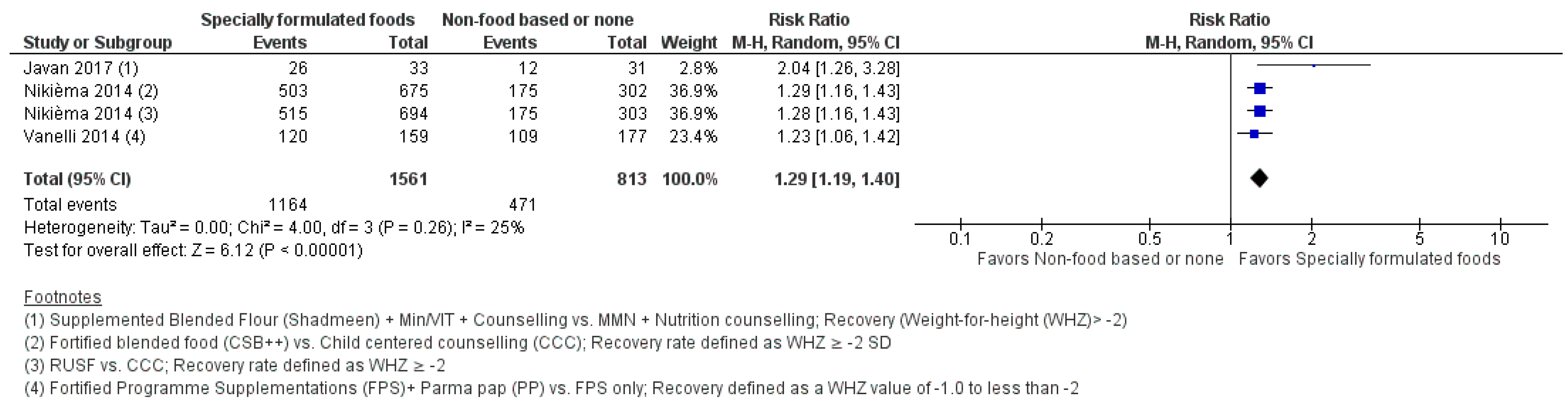
3.4.1. Comparisons 1 and 2: Specially Formulated Foods versus Non-Food-Based or None
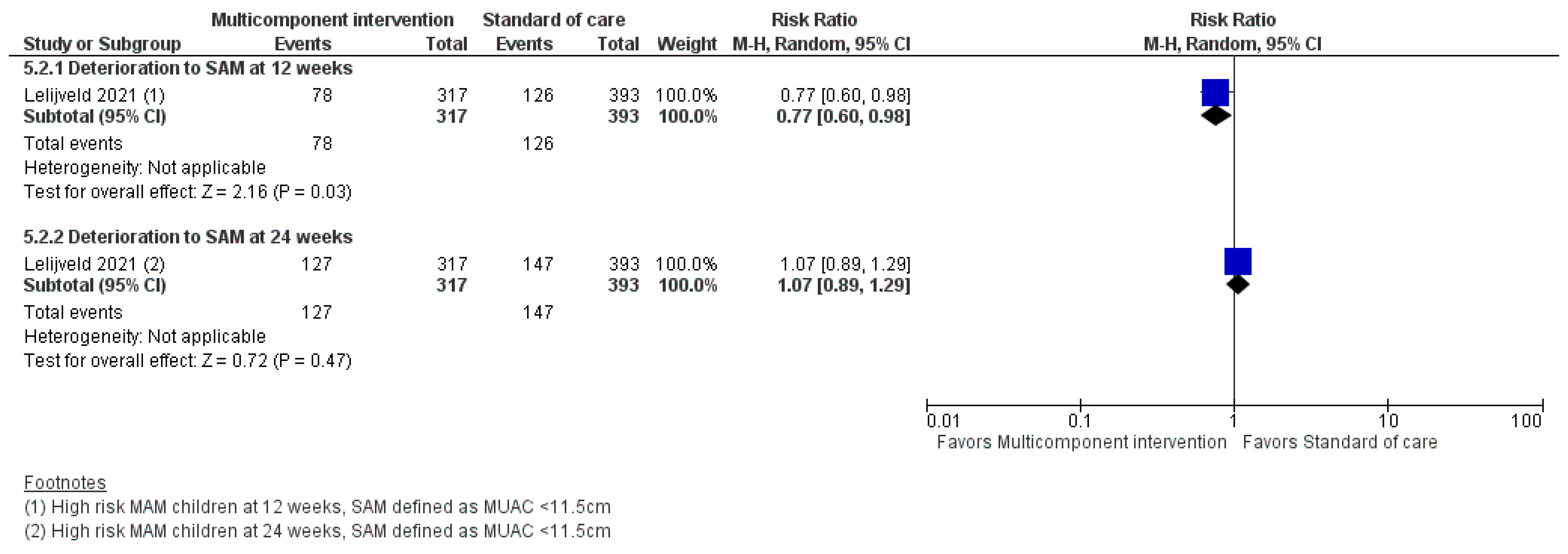
3.4.2. Comparison 4: Multicomponent Intervention versus Non-Food-Based or None
4. Discussion
4.1. Summary of Results
4.2. Overall Completeness and Applicability
4.3. Agreements and Disagreements with Other Studies or Reviews
4.4. Implications for Practice
4.5. Implications for Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olofin, I.; McDonald, C.; Ezzati, M.; Flaxman, S.; Black, R.; Fawzi, W.; Caulfield, L.; Danaei, G. Associations of Suboptimal Growth with All-Cause and Cause-Specific Mortality in Children under Five Years: A Pooled Analysis of Ten Prospective Studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund (UNICEF); World Health Organization; International Bank for Reconstruction and Development/The World Bank. Levels and Trends in Child Malnutrition: Key Findings of the 2021 Edition of the Joint Child Malnutrition Estimates; World Health Organization: Geneva, Switzerlands, 2021; Available online: https://apps.who.int/iris/handle/10665/341135 (accessed on 1 April 2022).
- Food an Agricultural Organisation (FAO); Tufts University. Twin Peaks: The Seasonality of Acute Malnutrition, Conflict and Environmental Factors—Chad, South Sudan and the Sudan; FAO: Rome, Italy, 2019. [Google Scholar]
- Grellety, E.; Golden, M.H. Weight-for-Height and Mid-Upper-Arm Circumference Should Be Used Independently to Diagnose Acute Malnutrition: Policy Implications. BMC Nutr. 2016, 2, 10. [Google Scholar] [CrossRef]
- Myatt, M. How Do We Estimate a Caseload of SAM/MAM in a Given Time Period. 2012. Available online: https://www.ennonline.net/attachments/3133/MAM-and-SAM-caseload-calculations.pdf (accessed on 21 March 2022).
- World Health Organization (WHO); United Nations Children’s Fund (UNICEF). Discussion Paper: The Extension of the 2025 Maternal, Infant and Young Child Nutrition Targets to 2030. 2021. Available online: https://data.unicef.org/resources/who-unicef-discussion-paper-nutrition-targets/ (accessed on 21 March 2022).
- Global Nutrition Cluster (GNC). Moderate Acute Malnutrition: A Decision Tool for Emergencies. 2017. Available online: https://reliefweb.int/report/world/moderate-acute-malnutrition-decision-tool-emergencies (accessed on 30 April 2022).
- World Health Organization. Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition; World Health Organization: Geneva, Switzerland, 2013. Available online: https://www.ncbi.nlm.nih.gov/books/NBK258736/ (accessed on 30 April 2022).
- Golden, M.H.; Grellety, E. Integrated Management of Acute Malnutrition (IMAM) Generic Protocol; English Version 6.6.2. 2011. Available online: https://www.researchgate.net/publication/292131715_Golden_MH_Grellety_Y_Integrated_Management_of_Acute_Malnutrition_IMAM_Generic_Protocol_ENGLISH_version_662 (accessed on 5 August 2023).
- United Nations Children’s Fund (UNICEF); International Rescue Committee (IRC). Toolkit for CHW Community-Based Treatment of Uncomplicated Wasting for Children 6–59 Months in the Context of COVID-19; Version 1.0; UNICEF: New York, NY, USA, 2020; Available online: www.ennonline.net/toolkitforchwinthecontextofcovid19 (accessed on 1 May 2022).
- United Nations Children’s Fund (UNICEF); World Health Organization. Prevention, Early Detection and Treatment of Wasting in Children 0–59 Months through National Health Systems in the Context of COVID-19; UNICEF: New York, NY, USA, 2020. [Google Scholar]
- World Food Programme. WFP’s Additional Recommendations for the Management of Maternal and Child Malnutrition Prevention and Treatment in the Context of COVID 19; World Food Programme: Rome, Italy, 2020. [Google Scholar]
- Cichon, B.; Das, J.K.; Salam, R.A.; Padhani, Z.A.; Stobaugh, H.C.; Mughal, M.; Pajak, P.; Rutishauser-Perera, A.; Bhutta, Z.A.; Black, R.E. Effectiveness of Dietary Management for Moderate Wasting among Children >6 Months of Age—A Systematic Review and Meta-Analysis Exploring Different Types, Quantities, and Durations. Nutrients 2023, 15, 1076. [Google Scholar] [CrossRef]
- Codex STAN 180-1991; Standard for Labelling of and Claims for Foods for Special Medical Purposes. Codex Alimentarius Commission: Atlanta, GA, USA; Brussels, Belgium, 1991.
- Codex STAN 146-1985; General Standard for the Labelling of and Claims for Prepackaged Foods for Special Dietary Uses. Codex Alimentarius Commission: Atlanta, GA, USA; Brussels, Belgium, 2009.
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 5 August 2023).
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. Br. Med. J. 2019, 366, l4898. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Review Manager (RevMan) [Computer Program], Version 5.4.; The Cochrane Collaboration: London, UK, 2020.
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. Br. Med. J. 2008, 336, 924. [Google Scholar] [CrossRef] [PubMed]
- Javan, R.; Kooshki, A.; Afzalaghaee, M.; Aldaghi, M.; Yousefi, M. Effectiveness of Supplementary Blended Flour Based on Chickpea and Cereals for the Treatment of Infants with Moderate Acute Malnutrition in Iran: A Randomized Clinical Trial. Electron. Physician 2017, 9, 6078–6086. [Google Scholar] [CrossRef]
- Lelijveld, N.; Godbout, C.; Krietemeyer, D.; Los, A.; Wegner, D.; Hendrixson, D.T.; Bandsma, R.; Koroma, A.; Manary, M. Treating High-Risk Moderate Acute Malnutrition Using Therapeutic Food Compared with Nutrition Counseling (Hi-MAM Study): A Cluster-Randomized Controlled Trial. Am. J. Clin. Nutr. 2021, 114, 955–964. [Google Scholar] [CrossRef]
- Nikièma, L.; Huybregts, L.; Kolsteren, P.; Lanou, H.; Tiendrebeogo, S.; Bouckaert, K.; Kouanda, S.; Sondo, B.; Roberfroid, D. Treating Moderate Acute Malnutrition in First-Line Health Services: An Effectiveness Cluster-Randomized Trial in Burkina Faso. Am. J. Clin. Nutr. 2014, 100, 241–249. [Google Scholar] [CrossRef]
- Vanelli, M.; Virdis, R.; Contini, S.; Corradi, M.; Cremonini, G.; Marchesi, M.; Mele, A.; Monti, F.; Pagano, B.; Proietti, I.; et al. A Hand-Made Supplementary Food for Malnourished Children. Acta Biomed. 2014, 85, 236–242. [Google Scholar]
- Hossain, M.I.; Nahar, B.; Hamadani, J.D.; Ahmed, T.; Brown, K.H. Effects of Community-Based Follow-up Care in Managing Severely Underweight Children. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 310–319. [Google Scholar] [CrossRef]
- James, P.; Sadler, K.; Wondafrash, M.; Argaw, A.; Luo, H.; Geleta, B.; Kedir, K.; Getnet, Y.; Belchew, T.; Bahwere, P. Children with Moderate Acute Malnutrition with No Access to Supplementary Feeding Programmes Experience High Rates of Deterioration and No Improvement: Results from a Prospective Cohort Study in Rural Ethiopia. PLoS ONE 2016, 11, e0153530. [Google Scholar] [CrossRef]
- Adamu, W.; Jara, D.; Alemayehu, M.; Burrowes, S. Risk Factors Associated with Poor Health Outcomes for Children under the Age of 5 with Moderate Acute Malnutrition in Rural Fagita Lekoma District, Awi Zone, Amhara, Ethiopia, 2016. BMC Nutr. 2017, 3, 88. [Google Scholar] [CrossRef]
- Chang, C.Y.; Trehan, I.; Wang, R.J.; Thakwalakwa, C.; Maleta, K.; Deitchler, M.; Manary, M.J. Children Successfully Treated for Moderate Acute Malnutrition Remain at Risk for Malnutrition and Death in the Subsequent Year after Recovery. J. Nutr. 2013, 143, 215–220. [Google Scholar] [CrossRef]
- Stobaugh, H.C.; Ryan, K.N.; Kennedy, J.A.; Grise, J.B.; Crocker, A.H.; Thakwalakwa, C.; Litkowski, P.E.; Maleta, K.M.; Manary, M.J.; Trehan, I. Including Whey Protein and Whey Permeate in Ready-to-Use Supplementary Food Improves Recovery Rates in Children with Moderate Acute Malnutrition: A Randomized, Double-Blind Clinical Trial. Am. J. Clin. Nutr. 2016, 103, 926–933. [Google Scholar] [CrossRef]
- McDonald, C.; Olofin, I.; Flaxman, S.; Fawzi, W.; Spiegelman, D.; Caulfield, L.; Black, R.; Ezzati, M.; Danaei, G. The Effect of Multiple Anthropometric Deficits on Child Mortality: Meta-Analysis of Individual Data in 10 Propective Studies from Developing Countries. Am. J. Clin. Nutr. 2013, 97, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Myatt, M.; Khara, T.; Dolan, C.; Garenne, M.; Briend, A. Improving Screening for Malnourished Children at High Risk of Death: A Study of Children Aged 6-59 Months in Rural Senegal—ERRATUM. Public Health Nutr. 2019, 22, 872–873. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guideline on the Prevention and Management of Wasting and Nutritional Oedema (Acute Malnutrition) in Infants under 5 Years (Version 1.1); WHO: Geneva, Switzerland, 2023; Available online: https://www.childwasting.org/normative-guidance (accessed on 5 August 2023).
- Lelijveld, N.; Beedle, A.; Farhikhtah, A.; Elrayah, E.E.; Bourdaire, J.; Aburto, N. Systematic Review of the Treatment of Moderate Acute Malnutrition Using Food Products. Matern. Child. Nutr. 2020, 16, e12898. [Google Scholar] [CrossRef]
- Gluning, I.; Kerac, M.; Bailey, J.; Bander, A.; Opondo, C. The Management of Moderate Acute Malnutrition in Children Aged 6-59 Months in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Lelijveld, N.; Musyoki, E.; Adongo, S.W.; Mayberry, A.; Wells, J.C.; Opondo, C.; Kerac, M.; Bailey, J. Relapse and Post-Discharge Body Composition of Children Treated for Acute Malnutrition Using a Simplified, Combined Protocol: A Nested Cohort from the ComPAS RCT. PLoS ONE 2021, 16, e0245477. [Google Scholar] [CrossRef] [PubMed]
- Fabiansen, C.; Yaméogo, C.W.; Iuel-Brockdorf, A.-S.; Cichon, B.; Rytter, M.J.H.; Kurpad, A.; Wells, J.C.; Ritz, C.; Ashorn, P.; Filteau, S.; et al. Effectiveness of Food Supplements in Increasing Fat-Free Tissue Accretion in Children with Moderate Acute Malnutrition: A Randomised 2 × 2 × 3 Factorial Trial in Burkina Faso. PLoS Med. 2017, 14, e1002387. [Google Scholar] [CrossRef]
- McDonald, C.M.; Ackatia-Armah, R.S.; Doumbia, S.; Kupka, R.; Duggan, C.P.; Brown, K.H. Percent Fat Mass Increases with Recovery, But Does Not Vary According to Dietary Therapy in Young Malian Children Treated for Moderate Acute Malnutrition. J. Nutr. 2019, 149, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Chui, J.; Donnelly, A.; Cichon, B.; Mayberry, A.; Keane, E. The Cost-Efficiency and Cost-Effectiveness of Management of Wasting in Children: A Review of the Evidence, Approaches and Lessons; AAH (Action Against Hunger): New York, NY, USA; Save the Children UK: London, UK, 2020; Available online: https://resourcecentre.savethechildren.net/document/cost-efficiency-and-cost-effectiveness-management-wasting-children-review-evidence/ (accessed on 1 May 2022).
- Ackatia-Armah, R.; McDonald, C.; Doumbia, S.; Erhardt, J.; Hamer, D.; Brown, K. Malian Children with Moderate Acute Malnutrition Who Are Treated with Lipid-Based Dietary Supplements Have Greater Weight Gains and Recovery Rates than Those Treated with Locally Produced Cereal-Legume Products: A Community-Based, Cluster-Randomized Trial. Am. J. Clin. Nutr. 2015, 101, 632–645. [Google Scholar] [CrossRef]
- Isanaka, S.; Barnhart, D.A.; McDonald, C.; Ackatia-Armah, R.; Kupka, R.; Seydou, D.; Brown, K.; Menzies, N.A. Cost-Effectiveness of Community-Based Screening and Treatment of Moderate Acute Malnutrition in Mali. BMJ Glob. Health 2019, 4, e001227. [Google Scholar] [CrossRef]
- LaGrone, L.; Trehan, I.; Meuli, G.; Wang, R.; Thakwalakwa, C.; Maleta, K.; Manary, M. A Novel Fortified Blended Flour, Corn-Soy Blend “plus-plus,” Is Not Inferior to Lipid-Based Ready-to-Use Supplementary Foods for the Treatment of Moderate Acute Malnutrition in Malawian Children. Am. J. Clin. Nutr. 2012, 95, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Griswold, S.P.; Langlois, B.K.; Shen, Y.; Cliffer, I.R.; Suri, D.J.; Walton, S.; Chui, K.; Rosenberg, I.H.; Koroma, A.S.; Wegner, D.; et al. Effectiveness and Cost-Effectiveness of 4 Supplementary Foods for Treating Moderate Acute Malnutrition: Results from a Cluster-Randomized Intervention Trial in Sierra Leone. Am. J. Clin. Nutr. 2021, 114, 973–985. [Google Scholar] [CrossRef]
- Sphere Association. The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response, 4th ed.; Sphere Association: Geneva, Switzerland, 2018; Available online: www.spherestandards.org/handbook (accessed on 5 August 2023).
- Cichon, B.; Fabiansen, C.; Yaméogo, C.W.; Rytter, M.J.H.; Ritz, C.; Briend, A.; Christensen, V.B.; Michaelsen, K.F.; Oummani, R.; Filteau, S.; et al. Children with Moderate Acute Malnutrition Have Inflammation Not Explained by Maternal Reports of Illness and Clinical Symptoms: A Cross-Sectional Study in Burkina Faso. BMC Nutr. 2016, 2, 57. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Details |
|---|---|
| Study Participants | Children aged over six months with MAM, defined as WHZ ≥ −3 and <−2 and/or a MUAC of ≥11.5 cm and <12.5 cm or a WHZ between >70% and <80% of the median and without any oedema, treated either as inpatients or outpatients. |
| Intervention | Food-based approaches for the treatment of MAM with or without SFFs, including multicomponent interventions. |
| Comparison | Intervention with non-specially formulated foods, non-food based interventions, standard of care or none. |
| Outcomes | Anthropometric recovery, anthropometric outcomes (such as WHZ, weight for age z-score (WAZ), MUAC, weight and height gain), non-response, sustained recovery, recovery time, deterioration to SAM, and mortality. |
| Type of Study | Included: Experimental studies (Randomized controlled trials (RCTs) both individual and cluster randomised and quasi experimental/non-RCTs).Excluded: Observational studies, animal studies, grey literature, reviews, conference abstracts, and studies with external comparison groups. |
| Author, Year | Study Design and Setting | Participants, Admission and Recovery Criteria | Description of Intervention and Control Groups | Outcomes |
|---|---|---|---|---|
| Hossain et al., 2011 [24] | RCT | 507 participants of which 301 had a WHZ < −2 and ≥−3. In this review we included data only from the subsample of 301 children who met the wasting criteria. Dhaka Hospital and four community clinics in police Districts of Demra, Gulshan, Sabujbagh, and Mirpur. |
| Weight-for-age (WAZ), weight-for-length (WHZ), height-for-age (HAZ), weight |
| Nikièma et al., 2014 [22] | cRCT Rural health centres in Hounde, Burkina Faso | 1974 children aged 6–24 months with a WHZ < −2 and ≥−3 Recovery was defined as a WHZ ≥ −2 at the end of a 12\week period |
| Number of children recovered, died, or dropped out, attendance, time to recovery, weight, length, and daily mid upper arm circumference (MUAC) gains |
| Javan et al., 2017 [20] | Randomised investigator blinded (single blind) controlled trial 17 Health centers in Urban areas of Sabzevar, Iran | 70 children aged 9–24 months with MAM defined as WHZ < −2 and ≥−3. Recovery was defined as WHZ > −2 at the end of intervention period |
| Rate of weight gain, length gain and Z-score WHZ gain, recovery proportion and adverse events. |
| Lelijveld 2021 [21] | cRCT 22 community nutrition clinics in Pujehun District, Sierra Leone | 1322 children aged 6–59 months with MAM, defined as MUAC ≥ 11.5 and <12.5 cm without oedema or clinical complications, Only 710 of these were in the High-risk group which met inclusion criteriaRecovery was defined as MUAC > 12.5 cm two consecutive visits |
| MUAC, WAZ, HAZ, WHZ, weight gain Kg, Subscapular skinfold thickness for age, triceps skinfold thickness for age, skinfold thickness ratio, recovered, died, deteriorate to SAM, Remained with MAM, recent illness |
| Vanelli et al., 2014 [23] | RCT Outpatient clinics in Makeni, Northern region, Sierra Leone | 332 children aged 6–60 months with a WHZ < −2 and ≥−3. Recovery was defined as achieving a WHZ-score > −2. |
| Weight, length, WHZ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padhani, Z.A.; Cichon, B.; Das, J.K.; Salam, R.A.; Stobaugh, H.C.; Mughal, M.; Rutishauser-Perera, A.; Black, R.E.; Bhutta, Z.A. Systematic Review of Management of Moderate Wasting in Children over 6 Months of Age. Nutrients 2023, 15, 3781. https://doi.org/10.3390/nu15173781
Padhani ZA, Cichon B, Das JK, Salam RA, Stobaugh HC, Mughal M, Rutishauser-Perera A, Black RE, Bhutta ZA. Systematic Review of Management of Moderate Wasting in Children over 6 Months of Age. Nutrients. 2023; 15(17):3781. https://doi.org/10.3390/nu15173781
Chicago/Turabian StylePadhani, Zahra A., Bernardette Cichon, Jai K. Das, Rehana A. Salam, Heather C. Stobaugh, Muzna Mughal, Alexandra Rutishauser-Perera, Robert E. Black, and Zulfiqar A. Bhutta. 2023. "Systematic Review of Management of Moderate Wasting in Children over 6 Months of Age" Nutrients 15, no. 17: 3781. https://doi.org/10.3390/nu15173781
APA StylePadhani, Z. A., Cichon, B., Das, J. K., Salam, R. A., Stobaugh, H. C., Mughal, M., Rutishauser-Perera, A., Black, R. E., & Bhutta, Z. A. (2023). Systematic Review of Management of Moderate Wasting in Children over 6 Months of Age. Nutrients, 15(17), 3781. https://doi.org/10.3390/nu15173781