
Dietary Behaviour and Sociocultural Determinants of Dietary Diversity among Rural Women of Reproductive Age: A Case of Amhara Region, Ethiopia


Abstract
1. Introduction
2. Materials and Methods
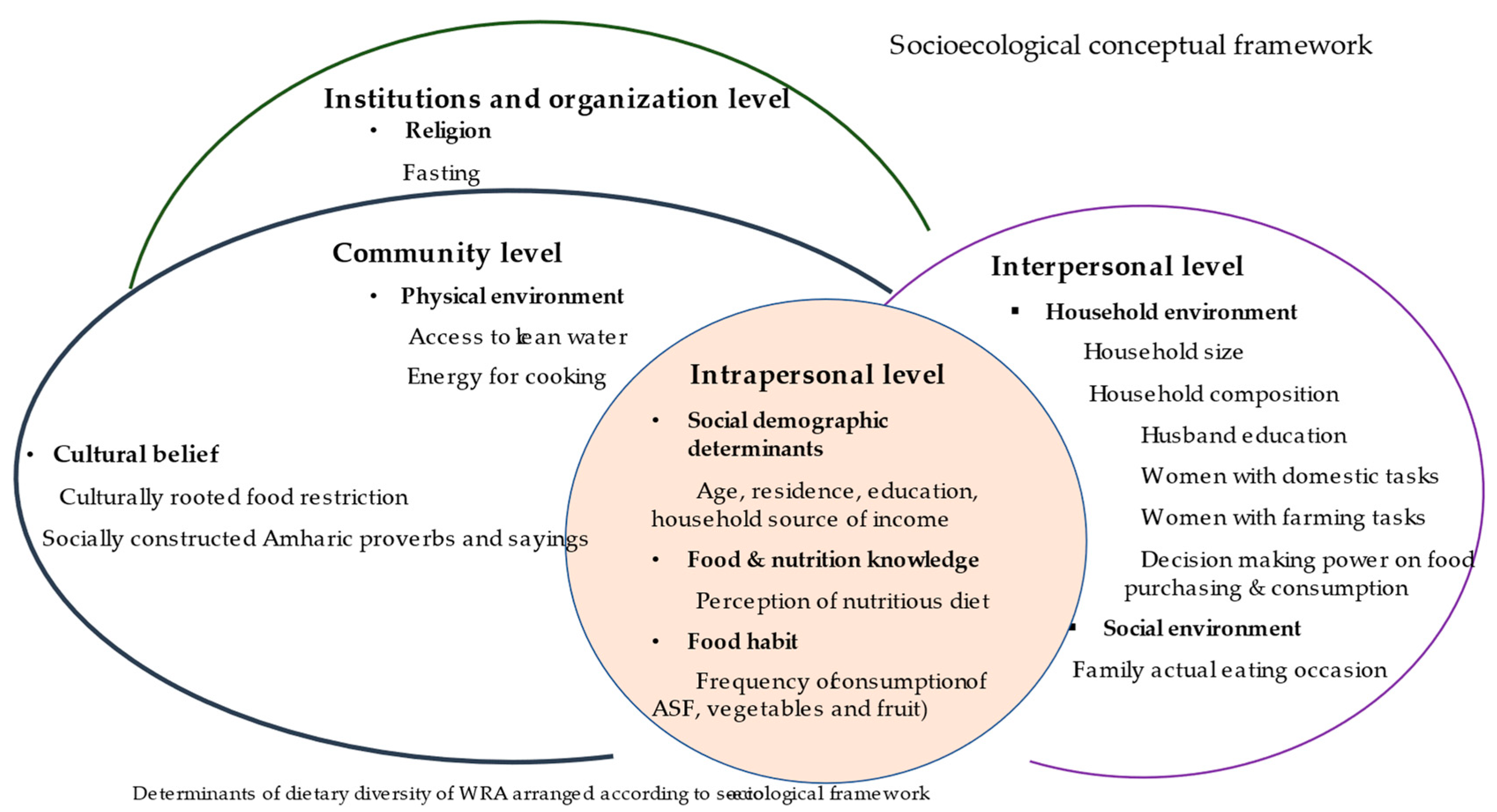
2.1. Study Design and Conceptual Framework
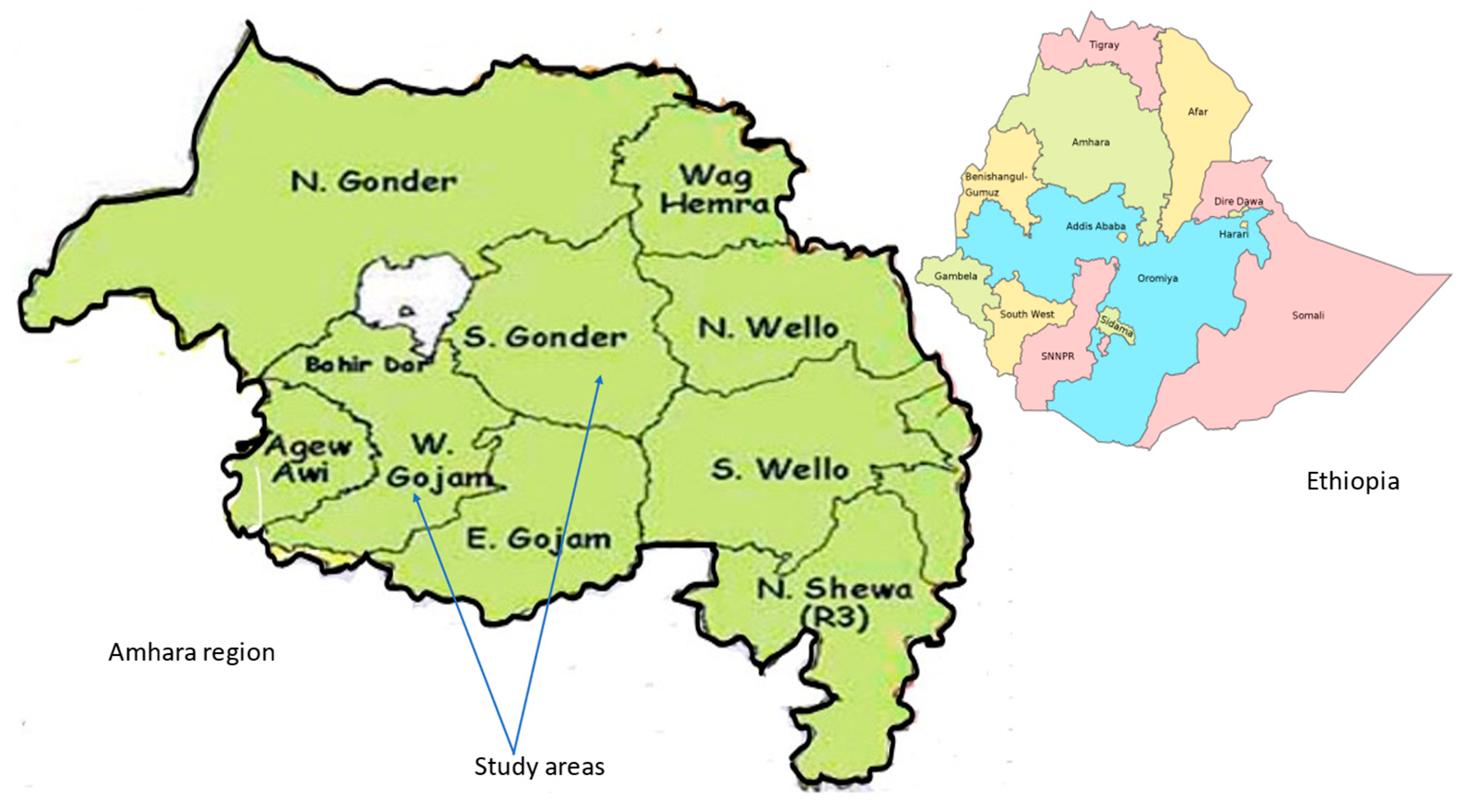
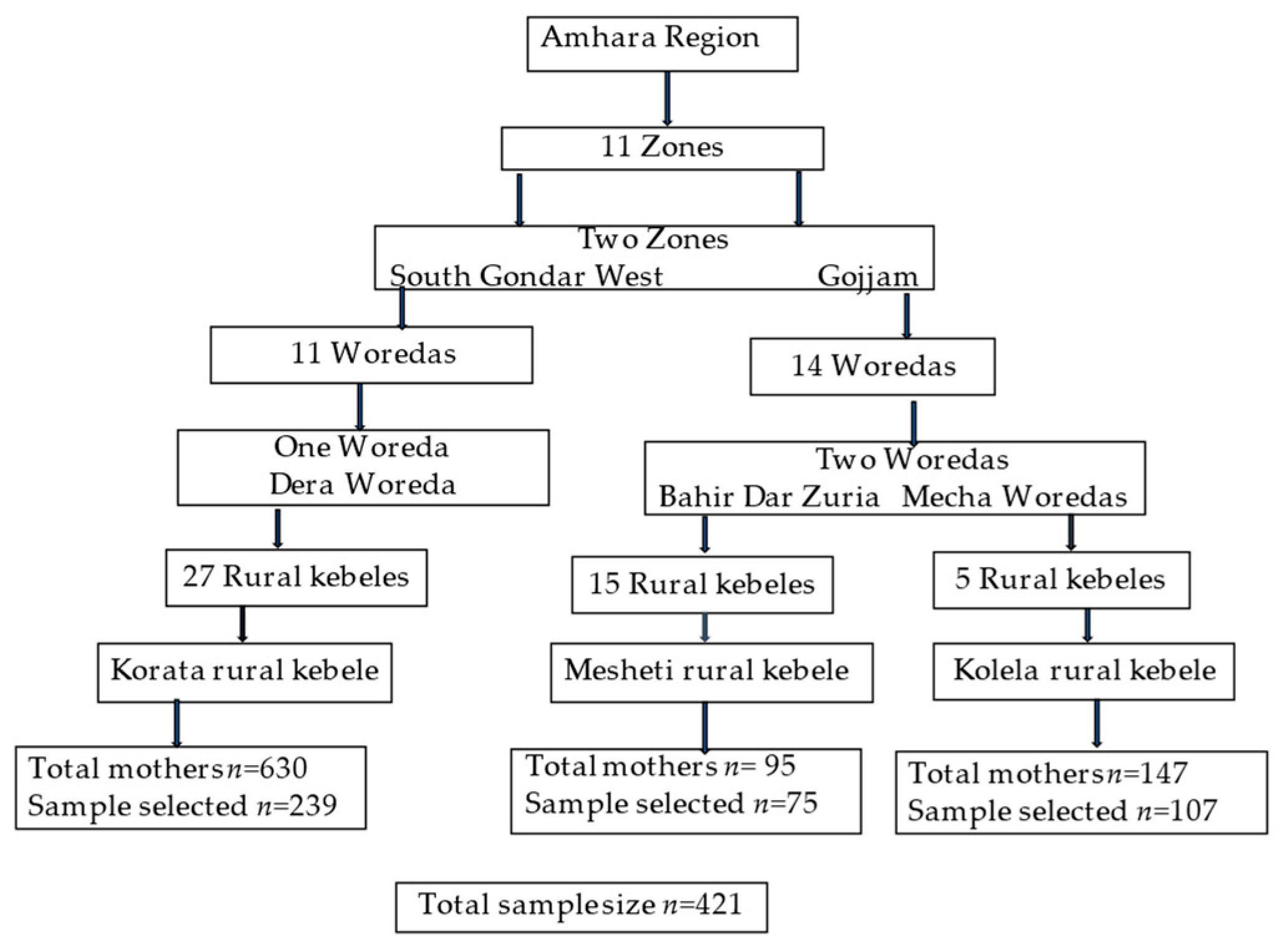
2.2. Study Setting and Selection of Study Area and Sample Size
2.3. Data Collection Procedure
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Sociodemographic Characteristics
3.2. Dietary Behaviour of WRA
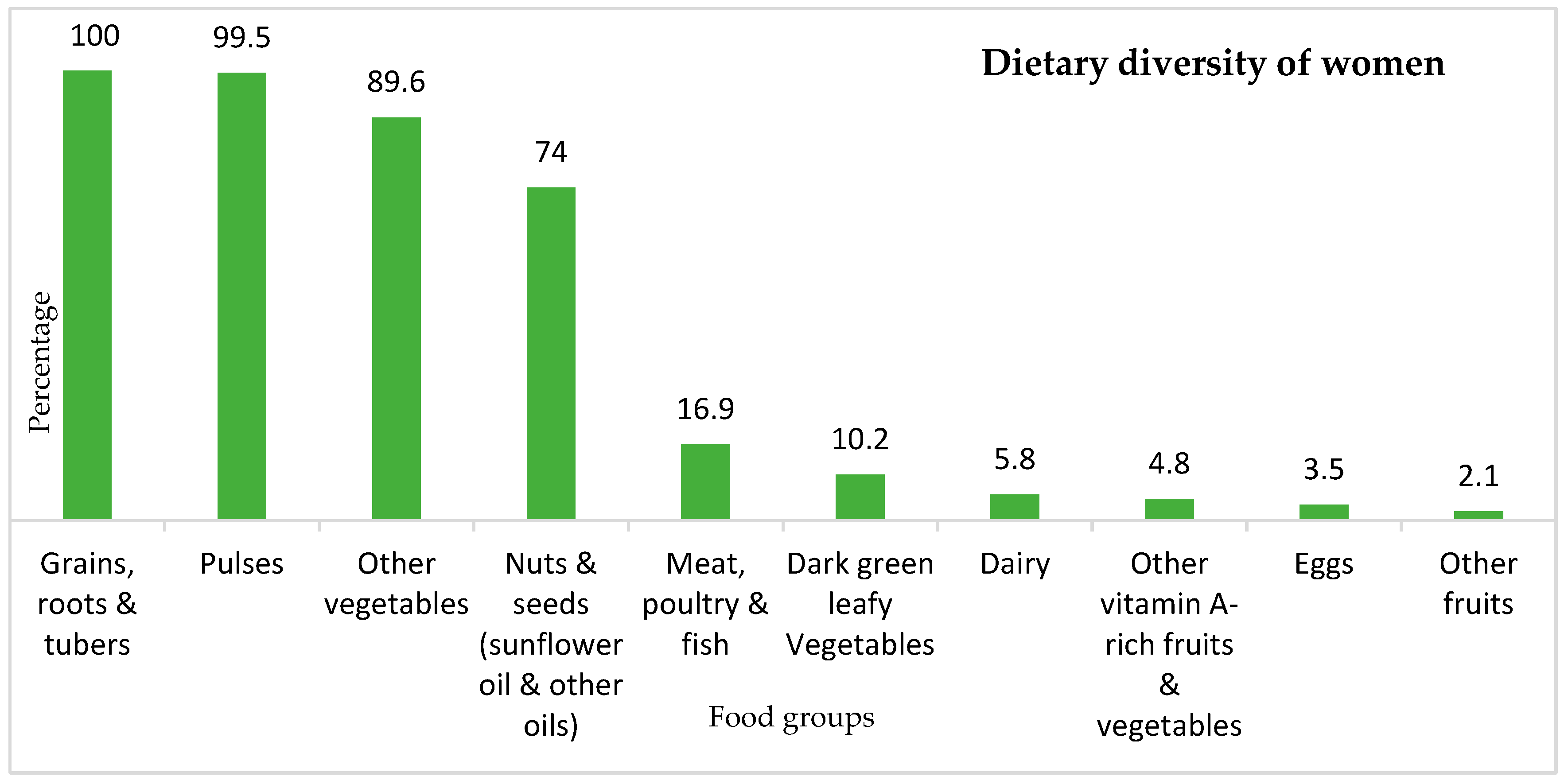
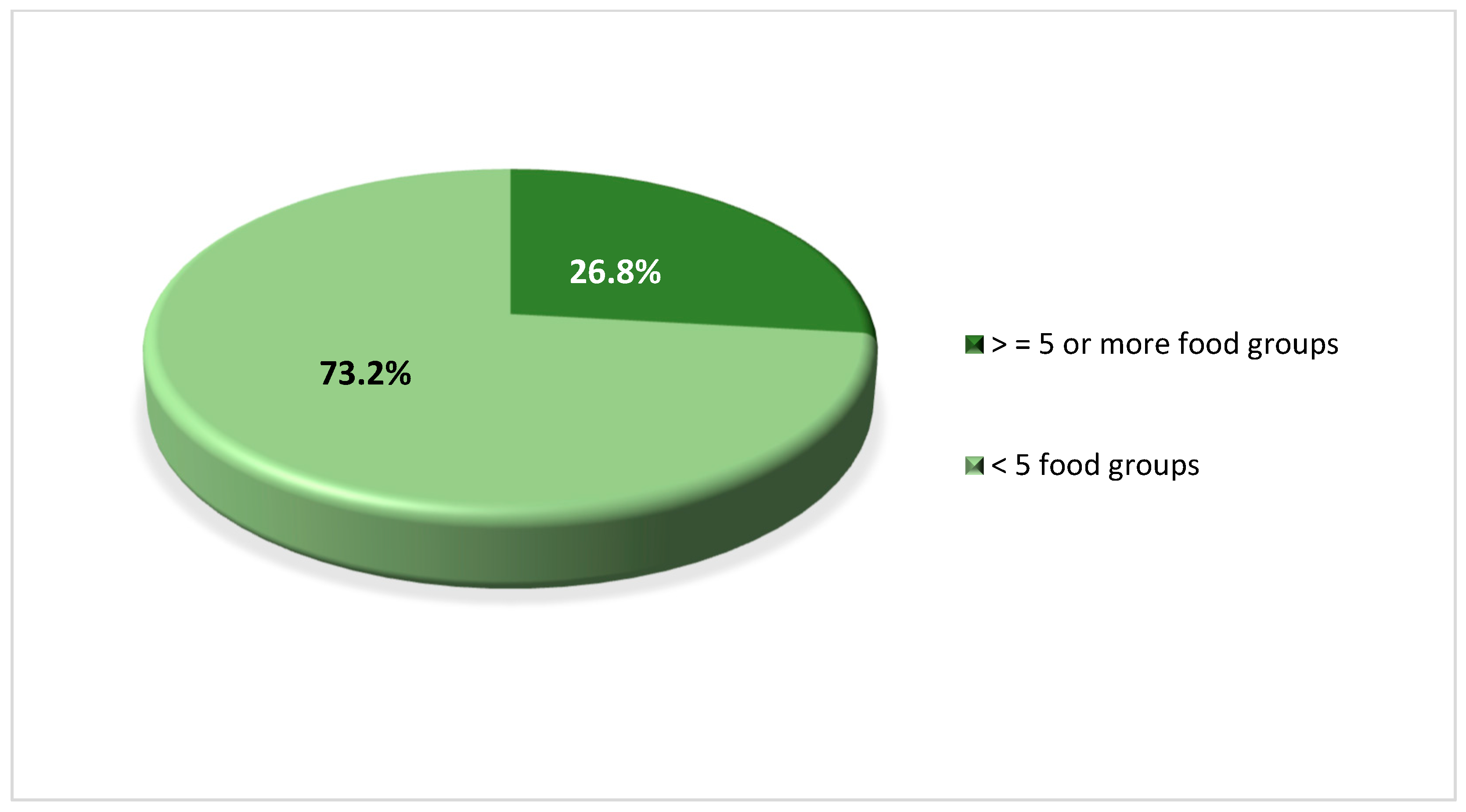
3.2.1. Dietary Diversity Practice
3.2.2. Eating Habits of WRAs within the Family’s Actual Eating Occasion
3.2.3. Eating Practices Related to Religion and Culture
3.2.4. Perception of Nutritious Diets
3.3. Determinants of Dietary Diversity of WRA
3.3.1. Intrapersonal/Individual-Level Determinants
3.3.2. Interpersonal/Household Level Determinants
3.3.3. Community Level Determinants
- •
- ቅልጥም እና ፈረሰኛ ለአባወራ (k’lt’m ena feresegna leabawora): a girl/woman should not eat the main parts of the lamb or chicken, but these parts should rather be given to the husband/man;
- •
- ሴት ልጅ መንገድ ላይ አትበላም (set liji menged lay atbelam): a woman should not eat on the street (in public);
- •
- ከሴት ሆዳም የአንድ አመት በረዶ ይሻላል (keset hodam yand amet beredo yshalall): a seasonal disaster is better than a woman who is a voracious eater;
- •
- የሴት ምራቋ ወፍራም ነው (yeset mɨrak’wa wefram new): a woman’s saliva is thick, so a woman cannot be hungry/she does not need to eat much, whereas a man is encouraged to eat a lot;
- •
- እንኳን የሸመተ የአረሰም አይችልሽ (Enkuan yeshemete yearesem aychilish): no one can cover your food expenses as you are voracious eater (the woman). This proverb is mostly related to the manner of eating (i.e., WRAs should eat slowly, not eat in front of elders and guests, and should not eat much food)
3.3.4. Institutions and Organisation Level
4. Discussion
4.1. Minimum Dietary Diversity Score (MDD-W)
4.2. Food Habits
4.3. Food Restrictions
4.4. Determinants of Dietary Diversity at Intrapersonal/Interpersonal/Community/Institutional Level
- Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stok, F.M.; Renner, B.; Allan, J.; Boeing, H.; Ensenauer, R.; Issanchou, S.; Kiesswetter, E.; Lien, N.; Mazzocchi, M.; Monsivais, P.; et al. Dietary Behavior: An Interdisciplinary Conceptual Analysis and Taxonomy. Front. Psychol. 2018, 9, 1689. [Google Scholar] [CrossRef] [PubMed]
- UN Food and Agriculture Organization (FAO). Minimum Dietary Diversity for Women; UN Food and Agriculture Organisation (FAO): Rome, Italy, 2021; Available online: https://www.fao.org/3/cb3434en/cb3434en.pdf (accessed on 10 March 2022).
- World Health Organization, Regional Office for Europe. Good Maternal Nutrition: The Best Start in Life; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2016; Available online: https://apps.who.int/iris/handle/10665/329459 (accessed on 26 June 2022).
- Global Nutrition Report. 2021 Global Nutrition Report: The State of Global Nutrition; Development Initiatives: Bristol, UK, 2021; Available online: https://globalnutritionreport.org/reports/2021-global-nutrition-report/ (accessed on 25 January 2023).
- Ethiopian Public Health Institute. Ethiopian National Micronutrient Survey Report; Ethiopian Public Health Institute: Addis Ababa, Ethiopia, 2016. [Google Scholar]
- Jiwani, S.S.; Gatica-Domínguez, G.; Crochemore-Silva, I.; Maïga, A.; Walton, S.; Hazel, E.; Baille, B.; Bose, S.; Bosu, W.K.; Busia, K.; et al. Trends and inequalities in the nutritional status of adolescent girls and adult women in sub-Saharan Africa since 2000: A cross-sectional series study. BMJ Glob. Health 2020, 5, e002948. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Liu, J.; Qi, X.; Wang, R.; Wang, X.; Wang, K.; Xu, Q.; Chen, P.; Meng, N.; Wu, Q.; et al. Global, Regional, and National Estimates of Nutritional Deficiency Burden among Reproductive Women from 2010 to 2019. Nutrients 2022, 14, 832. [Google Scholar] [CrossRef] [PubMed]
- Harika, R.; Faber, M.; Samuel, F.; Kimiywe, J.; Mulugeta, A.; Eilander, A. Micronutrient Status and Dietary Intake of Iron, Vitamin A, Iodine, Folate and Zinc in Women of Reproductive Age and Pregnant Women in Ethiopia, Kenya, Nigeria and South Africa: A Systematic Review of Data from 2005 to 2015. Nutrients 2017, 9, 1096. [Google Scholar] [CrossRef] [PubMed]
- Amegbor, P.M.; Yankey, O.; Davies, M.; Sabel, C.E. Individual and contextual predictors of overweight or obesity among women in Uganda: A spatio-temporal perspective. GeoJournal 2022, 87, 3793–3813. [Google Scholar] [CrossRef]
- Abraham, S.; Miruts, G.; Shumye, A. Magnitude of chronic energy deficiency and its associated factors among women of reproductive age in the Kunama population, Tigray, Ethiopia, in 2014. BMC Nutr. 2015, 1, 12. [Google Scholar] [CrossRef]
- Ferede, A.; Lemessa, F.; Tafa, M.; Sisay, S. The prevalence of malnutrition and its associated risk factors among women of reproductive age in Ziway Dugda district, Arsi Zone, Oromia Regional State, Ethiopia. Public Health 2017, 152, 1–8. [Google Scholar] [CrossRef]
- Kassie Tesema, A.; Liyew, A.M.; Alem, A.Z.; Yeshaw, Y.; Tesema, G.A.; Teshale, A.B. Spatial distribution and determinants of undernutrition among reproductive age women of Ethiopia: A multilevel analysis. PLoS ONE 2021, 16, e0257664. [Google Scholar] [CrossRef]
- Woldu, B.; Enawgaw, B.; Asrie, F.; Shiferaw, E.; Getaneh, Z.; Melku, M. Prevalence and Associated Factors of Anemia among Reproductive-Aged Women in Sayint Adjibar Town, Northeast Ethiopia: Community-Based Cross-Sectional Study. Anemia 2020, 2020, 8683946. [Google Scholar] [CrossRef]
- Omer, I.; Derese, T.; Sintayehu, Y. Overweight and Its Associated Factors among Women of Reproductive Age in Dire Dawa, Eastern Ethiopia, 2021: Community-Based Cross-Sectional Study. J. Obes. 2022, 2022, 7268573. [Google Scholar] [CrossRef]
- Collaborators, G.D. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Kedir, H.; Berhane, Y.; Worku, A. Magnitude and determinants of malnutrition among pregnant women in eastern Ethiopia: Evidence from rural, community-based setting. Matern. Child Nutr. 2016, 12, 51–63. [Google Scholar] [CrossRef]
- Forbes, L.E.; Graham, J.E.; Berglund, C.; Bell, R.R. Dietary Change during Pregnancy and Women’s Reasons for Change. Nutrients 2018, 10, 1032. [Google Scholar] [CrossRef]
- Yiga, P.; Seghers, J.; Ogwok, P.; Matthys, C. Determinants of dietary and physical activity behaviours among women of reproductive age in urban sub-Saharan Africa: A systematic review. Br. J. Nutr. 2020, 124, 761–772. [Google Scholar] [CrossRef]
- Gitagia, M.W.; Ramkat, R.C.; Mituki, D.M.; Termote, C.; Covic, N.; Cheserek, M.J. Determinants of dietary diversity among women of reproductive age in two different agro-ecological zones of Rongai Sub-County, Nakuru, Kenya. Food Nutr. Res. 2019, 63. [Google Scholar] [CrossRef]
- Merga, G.; Mideksa, S.; Dida, N.; Kennedy, G. Dietary diversity and associated factors among women of reproductive age in Jeldu District, West Shoa Zone, Oromia Ethiopia. PLoS ONE 2022, 17, e0279223. [Google Scholar] [CrossRef]
- Wachamo, D.; Tegene, Y. Dietary Diversity Score of Women of Reproductive Age and Infant and Young Children and Associated Factors among Rural Dwellers in Shalla Bura District, Oromia, Ethiopia Demelash. Int. J. Nutr. Disord. Ther. 2020, 3, 9–15. [Google Scholar]
- Girma, W.; Genebo, T. Determinants of the Nutritional Status of Mothers and Children in Ethiopia; ORC Macro: Calverton, MA, USA, 2002; Available online: https://dhsprogram.com/pubs/pdf/fa39/02-nutrition.pdf (accessed on 10 February 2023).
- Nega, G.; Endris, M.; Teferi, D.; Nana, A.; Michael, R.W. Dietary Diversity and Associated Factors among Rural Households in South Gondar Zone, Northwest Ethiopia; Feed the Future: Bahir Dar, Ethiopia, 2015; Available online: https://agri-learning-ethiopia.org/wp-content/uploads/2016/07/Girma-Nega-et-al-Dietary-Diversity.pdf (accessed on 10 January 2023).
- Desalegn, B.B.; Lambert, C.; Riedel, S.; Negese, T.; Biesalski, H.K. Feeding Practices and Undernutrition in 6–23-Month-Old Children of Orthodox Christian Mothers in Rural Tigray, Ethiopia: Longitudinal Study. Nutrients 2019, 11, 138. [Google Scholar] [CrossRef]
- Bazzano, A.N.; Potts, K.S.; Mulugeta, A. How do pregnant and lactating women, and young children, experience religious food restriction at the community level? A qualitative study of fasting traditions and feeding behaviors in four regions of Ethiopia. PLoS ONE 2018, 13, e0208408. [Google Scholar] [CrossRef]
- Hadush, Z.; Birhanu, Z.; Chaka, M.; Gebreyesus, H. Foods tabooed for pregnant women in Abala district of Afar region, Ethiopia: An inductive qualitative study. BMC Nutr. 2017, 3, 40. [Google Scholar] [CrossRef]
- Zerfu, T.A.; Umeta, M.; Baye, K. Dietary habits, food taboos, and perceptions towards weight gain during pregnancy in Arsi, rural central Ethiopia: A qualitative cross-sectional study. J. Health Popul. Nutr. 2016, 35, 22. [Google Scholar] [CrossRef] [PubMed]
- Tsegaye, D.; Tamiru, D.; Belachew, T. Food-related taboos and misconceptions during pregnancy among rural communities of Illu Aba Bor zone, Southwest Ethiopia. A community based qualitative cross-sectional study. BMC Pregnancy Childbirth 2021, 21, 309. [Google Scholar] [CrossRef] [PubMed]
- Demilew, Y.M.; Alene, G.D.; Belachew, T. Dietary practices and associated factors among pregnant women in West Gojjam Zone, Northwest Ethiopia. BMC Pregnancy Childbirth 2020, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Federal Democratic Republic of Ethiopia. Seqota Declaration Implementation Plan (2016–2030): Summary Program Approach Document; Federal Democratic Republic of Ethiopia: Addis Ababa, Ethiopia, 2016. [Google Scholar]
- Figueroa, R.; Saltzman, J.; Jarick Metcalfe, J.; Wiley, A. “Culture Is So Interspersed”: Child-Minders’ and Health Workers’ Perceptions of Childhood Obesity in South Africa. J. Obes. 2017, 2017, 9629748. [Google Scholar] [CrossRef]
- Hussein, J.W. The social and ethno-cultural construction of masculinity and femininity in African proverbs. Afr. Study Monogr. 2005, 26, 59–87. [Google Scholar] [CrossRef]
- Oniang’o, R.K.; Mutuku, J.M.; Malaba, S.J. Contemporary African food habits and their nutritional and health implications. Asia Pac. J. Clin. Nutr. 2003, 12, 331–336. [Google Scholar]
- Briones Alonso, E. The Impact of Culture, Religion and Traditional Knowledge on Food and Nutrition Security in Developing Countries; LICOS—Centre for Institutions and Economic Performance: Hague, The Netherlands, 2015; Available online: https://ageconsearch.umn.edu/record/285169?ln=en (accessed on 28 May 2023).
- Ethiopian Public Health Institute (EPHI) and ICF. Ethiopia Mini Demographic and Health Survey 2019: Final Report; EPHI and ICF: Rockville, MA, USA, 2021. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiment by Nature and Design; Harvard University Press: Cambridge, MA, USA; London, UK, 1979; pp. 109–131. [Google Scholar]
- Central Statistical Agency. Population Projection of Ethiopia for All Regions at Wereda Level from 2014–2017; Central Statistical Agency: Addis Ababa, Ethiopia, 2013. [Google Scholar]
- Amhara National Regional State, Ethiopian Government Portal. 2022. Available online: https://landportal.org/node/39377 (accessed on 20 February 2023).
- Wubneh, M. Ethnic Identity Politics and the Restructuring of Administrative Units in Ethiopia. Int. J. Ethiop. Stud. 2017, 11, 105–138. [Google Scholar]
- Kifleyesus, A. Food Familiarity and Novelty in a Condition of Socio-economic Transformation in North-Central Ethiopia. J. East. Afr. Stud. 2007, 1, 449–465. [Google Scholar] [CrossRef]
- Adubra, L.; Savy, M.; Fortin, S.; Kameli, Y.; Kodjo, N.E.; Fainke, K.; Mahamadou, T.; Le Port, A.; Martin-Prevel, Y. The Minimum Dietary Diversity for Women of Reproductive Age (MDD-W) Indicator Is Related to Household Food Insecurity and Farm Production Diversity: Evidence from Rural Mali. Curr. Dev. Nutr. 2019, 3, nzz022. [Google Scholar] [CrossRef]
- Custodio, E.; Kayikatire, F.; Fortin, S.; Thomas, A.C.; Kameli, Y.; Nkunzimana, T.; Ndiaye, B.; Martin-Prevel, Y. Minimum dietary diversity among women of reproductive age in urban Burkina Faso. Matern. Child Nutr. 2020, 16, e12897. [Google Scholar] [CrossRef]
- Gezimu Gebre, G. Intra-Household Decision-Making and their Effects on Women Dietary Diversity: Evidence from Ethiopia. Ecol. Food Nutr. 2022, 61, 705–727. [Google Scholar] [CrossRef]
- Onyeji, G.N.; Sanusi, R.A. Nutrient adequacy of diets of women of childbearing age in south-east Nigeria. Prog. Nutr. 2022, 24, e2022085. [Google Scholar]
- Tamale, D.; Kagoro-Rugunda, G. Dietary diversity among women of reproductive age (15–49 years): Implication for folate deficiency in Mbarara district, Uganda. Int. J. Community Med. Public Health 2019, 6, 2745. [Google Scholar] [CrossRef]
- Getacher, L.; Egata, G.; Alemayehu, T.; Bante, A.; Molla, A. Minimum Dietary Diversity and Associated Factors among Lactating Mothers in Ataye District, North Shoa Zone, Central Ethiopia: A Community-Based Cross-Sectional Study. J. Nutr. Metab. 2020, 2020, 1823697. [Google Scholar] [CrossRef]
- Seleshe, S.; Jo, C.; Lee, M. Meat Consumption Culture in Ethiopia. Korean J. Food Sci. Anim. Resour. 2014, 34, 7–13. [Google Scholar] [CrossRef]
- Sewenet, A.; Schwarcz, P. The Impacts of Food Taboos and Preferences on Food Security in Developing Countries: Evidence from Ethiopia. EU Agrar. Law 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Tefrera, B.; Tilahun, Y. Dietary Diversity among people 40 years and above in Jima Twon, Southwest Ethiopia. Ethiop. J. Health Sci. 2007, 17, 115–120. [Google Scholar]
- Daivadanam, M.; Wahlström, R.; Thankappan, K.R.; Ravindran, S. Balancing expectations amidst limitations: The dynamics of food decision-making in rural Kerala Global health. BMC Public Health 2015, 15, 644. [Google Scholar] [CrossRef]
- Morrison, J.; Dulal, S.; Harris-Fry, H.; Basnet, M.; Sharma, N.; Shrestha, B.; Manandhar, D.; Costello, A.; Osrin, D.; Saville, N. Formative qualitative research to develop community-based interventions addressing low birth weight in the plains of Nepal. Public Health Nutr. 2018, 21, 377–384. [Google Scholar] [CrossRef]
- Morrison, J.; Giri, R.; Arjyal, A.; Kharel, C.; Harris-Fry, H.; James, P.; Baral, S.; Saville, N.; Hillman, S. Addressing anaemia in pregnancy in rural plains Nepal: A qualitative, formative study. Matern. Child Nutr. 2021, 17 (Suppl. S1), e13170. [Google Scholar] [CrossRef]
- Turner, M.D.; Teague, M.; Ayantunde, A. Eating groups within households: Differentiation in food consumption by age, gender, and genealogical position in rural Burkina Faso. Food Policy 2021, 101, 102093. [Google Scholar] [CrossRef]
- Norris, S.A.; Frongillo, E.A.; Black, M.M.; Dong, Y.; Fall, C.; Lampl, M.; Liese, A.D.; Naguib, M.; Prentice, A.; Rochat, T.; et al. Nutrition in adolescent growth and development. Lancet 2022, 399, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S.; Yajnik, C.S.; Demaio, A. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet 2020, 395, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Alemayehu, Y.K.; Theall, K.; Lemma, W.; Hajito, K.W.; Tushune, K. The Role of Empowerment in the Association between a Woman’s Educational Status and Infant Mortality in Ethiopia: Secondary Analysis of Demographic and Health Surveys. Ethiop. J. Health Sci. 2015, 25, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Zepro, N.B. Food taboos and misconceptions among pregnant women of Shashemene District, Ethiopia, 2012. Sci. J. Public Health 2015, 3, 410–416. [Google Scholar] [CrossRef]
- Tenaw, Z.; Arega, M.; Tachbele, E. Nutritional knowledge, attitude and practices among pregnant women who attend antenatal care at public hospitals of Addis Ababa, Ethiopia. Int. J. Nurs. Midwifery 2018, 10, 81–89. [Google Scholar] [CrossRef]
- Yoseph, H.H. Prevalence of food aversions, cravings and pica during pregnancy and their association with nutritional status of pregnant women in Dale Woreda, Sidama zone, SNNPRS, Ethiopia. Int. J. Nutr. Metab. 2015, 7, 1–14. [Google Scholar] [CrossRef]
- Gyan, C.; Abbey, E.; Baffoe, M. Proverbs and Patriarchy: Analysis of Linguistic Prejudice and Representation of Women in Traditional Akan Communities of Ghana. Soc. Sci. 2020, 9, 22. [Google Scholar] [CrossRef]
- Leyew, Z. Asymmetrical Representation of Gender in Amharic. Ethiop. J. Soc. Sci. Humanit. 2011, 7, 71–112. [Google Scholar]
- Lukmanji, Z. Women’s workload and its impact on their health and nutritional status. Prog. Food Nutr. Sci. 1992, 16, 163–179. [Google Scholar]
- Kehoe, S.H.; Dhurde, V.; Bhaise, S.; Kale, R.; Kumaran, K.; Gelli, A.; Rengalakshmi, R.; Lawrence, W.; Bloom, I.; Sahariah, S.A. Barriers and facilitators to fruit and vegetable consumption among rural Indian women of reproductive age. Food Nutr. Bull. 2019, 40, 87–98. [Google Scholar] [CrossRef]
- Amugsi, D.A.; Lartey, A.; Kimani-Murage, E.; Mberu, B.U. Women’s participation in household decision-making and higher dietary diversity: Findings from nationally representative data from Ghana. J. Health Popul. Nutr. 2016, 35, 16. [Google Scholar] [CrossRef]
- Desta, M.; Akibu, M.; Tadese, M.; Tesfaye, M. Dietary Diversity and Associated Factors among Pregnant Women Attending Antenatal Clinic in Shashemane, Oromia, Central Ethiopia: A Cross-Sectional Study. J. Nutr. Metab. 2019, 2019, 3916864. [Google Scholar] [CrossRef]
- Assefa, G.M.; Sherif, S.; Sluijs, J.; Kuijpers, M.; Chaka, T.; Solomon, A.; Hailu, Y.; Muluneh, M.D. Gender Equality and Social Inclusion in Relation to Water, Sanitation and Hygiene in the Oromia Region of Ethiopia. Int. J. Environ. Res. Public Health 2021, 18, 4281. [Google Scholar] [CrossRef]
- UNICEF. For Every Child, Clean Water, Ethiopia. 2023. Available online: https://www.unicef.org/ethiopia/stories/women-water-bond (accessed on 10 June 2023).
- Weldehaweria, N.B.; Misgina, K.H.; Weldu, M.G.; Gebregiorgis, Y.S.; Gebrezgi, B.H.; Zewdie, S.W.; Ngusse, H.A.; Gebrewa, H.G.; Alemu, W. Dietary diversity and related factors among lactating women visiting public health facilities in Aksum town, Tigray, Northern Ethiopia. BMC Nutr. 2016, 2, 38. [Google Scholar] [CrossRef]
- Assefa, E. Lingusitic Violence against Women as Manifested in Sexist Amharic Proverbs. Ethnorêma 2015, 11, 67–94. [Google Scholar]
- Bililigne, A. Female Disempowerment: Some Expressions in Amharic, in Department of Linguistics; Addis Ababa University: Addis Ababa, Ethiopia, 2012; p. 89. Available online: http://etd.aau.edu.et/handle/123456789/6345 (accessed on 3 April 2013).
- Claeys, P. Violence against women. In Gender, Nutrition, and the Human Right to Adequate Food: Toward an Inclusive Framework; Bellows, A.C., Valente, F.L.S., Lemke, S., Nunez Burbano de Lara, M.D., Eds.; Routledge: New York, NY, USA, 2016; pp. 108–161. [Google Scholar]
- United Nations. Treaty Series: Treaties and international agreements registered or filed and recorded with the Secretariat of the United Nations. In HUMAN RIGHTS: Convention on the Elimination of All Forms of Discrimination against Women; United Nations: New York, NY, USA, 1990; p. 13. [Google Scholar]
- Seiermann, A.U.; Al-Mufti, H.; Waid, J.L.; Wendt, A.S.; Sobhan, S.; Gabrysch, S. Women’s fasting habits and dietary diversity during Ramadan in rural Bangladesh. Matern. Child Nutr. 2021, 17, e13135. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency (n) | Percent (%) |
|---|---|---|
| Age (in years) | ||
| <=21 | 58 | 13.5 |
| 22–25 | 68 | 15.8 |
| 26–28 | 65 | 15.1 |
| 29–32 | 133 | 30.9 |
| 33–38 | 60 | 13.9 |
| 39+ | 46 | 10.7 |
| Religion | ||
| Orthodox | 385 | 91.4 |
| Muslim | 36 | 8.6 |
| No religion | - | - |
| Residence | ||
| Korata rural kebele (South Gonder zone) | 239 | 55.5 |
| Kolela rural kebele (West Gojjam zone) | 107 | 24.8 |
| Meshenti rural kebele (West Gojjam zone) | 75 | 17.4 |
| Education: Women | ||
| Not able to read and write | 171 | 40.6 |
| Able to read and write | 128 | 30.4 |
| Primary education (G1-8) | 122 | 29.0 |
| Secondary education (G9-12) | - | - |
| Education: Husbands | ||
| Not able to read and write | 134 | 31.8 |
| Able to read and write | 135 | 32.1 |
| Primary education (G1-8) | 106 | 25.2 |
| Secondary education (G9-12) | 39 | 9.3 |
| Higher education | 7 | 1.7 |
| Source of HH income | ||
| Agriculture | 250 | 59.4 |
| Nonagriculture | 150 | 35.6 |
| Agriculture and others | 21 | 5.0 |
| Household size (number of children) | ||
| 1–3 | 232 | 55.1 |
| 4–6 | 172 | 40.9 |
| >=7 | 84 | 4.0 |
| Dietary Behaviours | Total n = 421 | Percent (%) |
|---|---|---|
| Eating habits | ||
| Family’s actual eating occasion | ||
| Food intake together with the family | 157 | 37.3 |
| Food intake after serving the family | 252 | 59.9 |
| Food intake before serving the family | 12 | 2.9 |
| Religious eating practice (fasting) | ||
| All fasting days | 323 | 76.7 |
| Major fasting days, Wednesday and Friday | 71 | 16.9 |
| I do not fast | 27 | 6.4 |
| Cultural eating practices (taboo foods and food restrictions) | ||
| Taboo foods | ||
| Pork meat | 420 | 99.8 |
| Goat meat | 43 | 10.2 |
| Goat milk | 183 | 43.5 |
| Food restrictions | ||
| Lamb meat (some parts like ‘kiltim’ ‘firimba’) | 112 | 26.6 |
| Chicken meat such as Feresegna, breasts, thighs and legs | 174 | 41.3 |
| Prioritize husbands for food intake | 175 | 41.6 |
| Perception of a nutritious diet | ||
| Consumption of a variety of foods | 168 | 39.9 |
| Consumption of animal-source food | 95 | 22.6 |
| Consumption of vegetables | 39 | 9.3 |
| Consumption of food until full | 14 | 3.3 |
| I do not know | 105 | 24.9 |
| Variables | MDD-W Inadequate N (%) | MDD-W Adequate N (%) | Chi-Square | p-Value |
|---|---|---|---|---|
| Intrapersonal level determinants | ||||
| Sociodemographic determinants | ||||
| Age of the respondents (in years) | ||||
| <=21 | 41 (71.9) | 16 (28.1) | ||
| 22–25 | 48 (71.6) | 19 (28.4) | ||
| 26–28 | 49 (76.6) | 15 (23.4) | ||
| 29–32 | 101 (78.3) | 28 (21.7) | ||
| 33–38 | 32 (56.1) | 25 (43.9) | 9.99 | * 0.01 |
| 39+ | 9 (80.4) | 37 (19.6) | ||
| Education of the women | 34.579 | * 0.001 | ||
| Not able to read and write | 148 (86.5) | 23 (13.5) | 26.32 | |
| Able to read and write | 92 (71.9) | 36 (28.1) | ||
| Primary (G1-8) and higher | 68 (55.7) | 54 (44.3) | 26.52 | * 0.01 |
| Household source of income | 1.859 | 0.395 | ||
| Agriculture | 180 (72.0) | 70 (28.0) | ||
| Nonagriculture | 110 (73.3) | 40 (26.7) | ||
| Agriculture and others | 23 (74.2) | 8 (25.8) | ||
| Residence | ||||
| Kolela rural kebele | 87 (81.3) | 20 (18.7) | 5.38 | * 0.02 |
| Korata rural kebele | 168 (70.3) | 71 (29.7) | ||
| Meshenti rural kebele | 53 (70.7) | 22 (29.3) | ||
| Food and nutrition knowledge | ||||
| Perception of nutritious diet | ||||
| Eat until full | 10 (71.4) | 4 (28.6) | ||
| Eat animal source foods | 76 (80.0) | 19 (20.0) | ||
| Eat variety of foods | 104 (61.9) | 64 (38.1) | 18.06 | * 0.01 |
| Eat vegetables | 33 (84.6) | 6 (15.4) | ||
| I don’t know | 85 (81.0) | 20 (19.0) | 4.33 | * 0.04 |
| Food habit | ||||
| Frequency of consumption of ASF | ||||
| Once a week | 19 (61.3) | 12 (38.7) | ||
| Twice a week | 7 (38.9) | 11 (61.1) | ||
| Twice a month | 35 (62.5) | 21 (37.5) | ||
| Once a month | 87 (69.6) | 38 (30.4) | 13.76 | * 0.01 |
| During holidays | 147 (82.6) | 31 (17.4) | 13.76 | * 0.01 |
| Never eat | 13 (100) | 0 (00) | ||
| Frequency of consumption of vegetables | ||||
| Every Day | 9 (39.1) | 14 (60.9) | 14.36 | * 0.001 |
| Once a week | 108 (69.2) | 48 (30.8) | ||
| Twice a week | 39 (72.2) | 15 (27.8) | ||
| Once a month | 137 (79.7) | 35 (20.3) | 6.25 | * 0.01 |
| Never eat | 15 (93.8) | 1 (6.3) | ||
| Frequency of consumption of fruit | ||||
| Once a week | 56 (58.3) | 40 (41.7) | 13.91 | * 0.001 |
| Twice a week | 20 (74.1) | 7 (25.9) | ||
| Once in a month | 178 (78.4) | 49 (21.6) | 6.92 | * 0.01 |
| Never eat | 54 (76.1) | 17 (23.9) | ||
| Interpersonal/Household-level determinants | ||||
| Household environment | ||||
| Household size | 0.079 | 0.779 | ||
| 1–3 children | 171 (73.7) | 61 (26.3) | ||
| 4–8 children | 137 (72.5) | 52 (27.5) | ||
| Household composition | ||||
| Husband education | ||||
| Not able to read and write | 103 (76.9) | 31 (23.1) | ||
| Able to read and write | 105 (77.8) | 30 (22.2) | ||
| Primary (G1-8) and higher | 100 (65.8) | 52 (34.2) | 6.60 | * 0.01 |
| WRA engaging in domestic tasks | ||||
| Domestic tasks without family support | 134 (78.4) | 37 (21.6) | 3.971 | * 0.046 |
| Domestic tasks with family support | 174 (69.6) | 76 (30.4) | ||
| WRAs engaging in farming tasks | ||||
| 1–3 tasks | 3 (33.3) | 6 (66.7) | 7.45 | * 0.01 |
| 4–5 tasks | 58 (84.1) | 11 (15.9) | 4.97 | * 0.03 |
| 6 or more tasks | 247 (72.0) | 96 (28.0) | ||
| WRAs decision to purchase food | ||||
| Wife | 69 (63.3) | 40 (36.7) | 7.29 | * 0.01 |
| Husband | 86 (83.5) | 17 (16.5) | 7.40 | * 0.01 |
| Both | 153 (73.2) | 56 (26.8) | ||
| WRAs decision to consume food | ||||
| Wife | 209 (75.2) | 69 (24.8) | ||
| Husband | 16 (94.1) | 1 (5.9) | 3.96 | 0.05 |
| Both | 83 (65.9) | 43 (34.1) | 4.84 | * 0.03 |
| Social environment | ||||
| Family actual eating occasion | ||||
| Food intake together with the family | 170 (68.2) | 50 (31.8) | ||
| Food intake after serving the family | 194 (77.0) | 58 (23.0) | 4.67 | * 0.03 |
| Food intake before serving the family | 7 (58.3) | 5 (41.7) | ||
| Community-level determinants | ||||
| Physical environment | ||||
| Access to clean water | ||||
| River, tap water, and groundwater | 32 (74.4) | 11 (25.6) | ||
| River and tap water | 6 (85.7) | 1 (14.3) | ||
| River and groundwater | 42 (89.4) | 5 (10.6) | 7.08 | * 0.01 |
| Tap water and groundwater | 106 (70.7) | 44 (29.3) | ||
| Tap water | 37 (58.7) | 26 (41.3) | 7.84 | * 0.01 |
| Groundwater | 85 (76.6) | 26 (23.4) | ||
| Energy for cooking | 1.856 | 0.395 | ||
| Firewood | 165 (72.2) | 65 (29.8) | ||
| Firewood and manure | 111 (76.6%) | 34 (23.4) | ||
| Manure | 28 (66.7) | 14 (33.3) | ||
| Cultural belief | ||||
| Socially constructed Amharic proverbs | ||||
| Prioritize husbands for food consumption ቅልጥም እና ፈረሰኛ ለአባወራ WRAs who accept WRAs who do not accept | 248 (82.9) 60 (49.2) | 51 (17.1) 62 (50.8) | 50.27 | * 0.01 |
| A woman should not eat on the street (in public), ሴት ልጅ መንገድ ላይ አትበላም WRAs who accept WRAs who do not accept | 210 (79.2) 98 (62.8) | 55 (20.8) 58 (37.2) | 13.47 | * 0.01 |
| Women should not eat much food (voracious eater) ከሴት ሆዳም የአንድ አመት በረዶ ይሻላል WRAs who accept WRAs who do not accept | 173 (82.0) 135 (64.3) | 38 (18.0) 65 (35.7) | 16.81 | * 0.01 |
| Manner of eating (eating slowly, not eating in front of elders and guests) እንኳን የሸመተ የአረሰም አይችልሽ WRAs who accept WRAs who do not accept | 150 (80.6) 158 (67.2) | 36 (19.4) 77 (32.8) | 9.49 | * 0.01 |
| Culturally rooted food restriction Women restricted to certain parts of chicken and lamb meat Yes No | 248 (82.9) 60 (49.2) | 51 (17.1) 62 (50.8) | 50.29 | * 0.001 |
| Institutions and organisation-level determinants | ||||
| Religion | 0.277 | 0.599 | ||
| Orthodox Christian | 283 (73.5) | 102 (26.5) | ||
| Muslim | 25 (69.4) | 11 (30.6) | ||
| Religious fasting practice | ||||
| All fasting days | 247 (76.5) | 76 (23.5) | 7.73 | * 0.01 |
| Major fasting days and Wednesday and Friday | 54 (76.1) | 17 (23.9) | ||
| Do not fast | 7 (25.9) | 20 (74.1) | 32.83 | * <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alamirew, S.K.; Lemke, S.; Stadlmayr, B.; Freyer, B. Dietary Behaviour and Sociocultural Determinants of Dietary Diversity among Rural Women of Reproductive Age: A Case of Amhara Region, Ethiopia. Nutrients 2023, 15, 3369. https://doi.org/10.3390/nu15153369
Alamirew SK, Lemke S, Stadlmayr B, Freyer B. Dietary Behaviour and Sociocultural Determinants of Dietary Diversity among Rural Women of Reproductive Age: A Case of Amhara Region, Ethiopia. Nutrients. 2023; 15(15):3369. https://doi.org/10.3390/nu15153369
Chicago/Turabian StyleAlamirew, Simegn Kassa, Stefanie Lemke, Barbara Stadlmayr, and Bernhard Freyer. 2023. "Dietary Behaviour and Sociocultural Determinants of Dietary Diversity among Rural Women of Reproductive Age: A Case of Amhara Region, Ethiopia" Nutrients 15, no. 15: 3369. https://doi.org/10.3390/nu15153369
APA StyleAlamirew, S. K., Lemke, S., Stadlmayr, B., & Freyer, B. (2023). Dietary Behaviour and Sociocultural Determinants of Dietary Diversity among Rural Women of Reproductive Age: A Case of Amhara Region, Ethiopia. Nutrients, 15(15), 3369. https://doi.org/10.3390/nu15153369