
Prevention and Treatment of Retinal Vein Occlusion: The Role of Diet—A Review



Abstract
1. Introduction
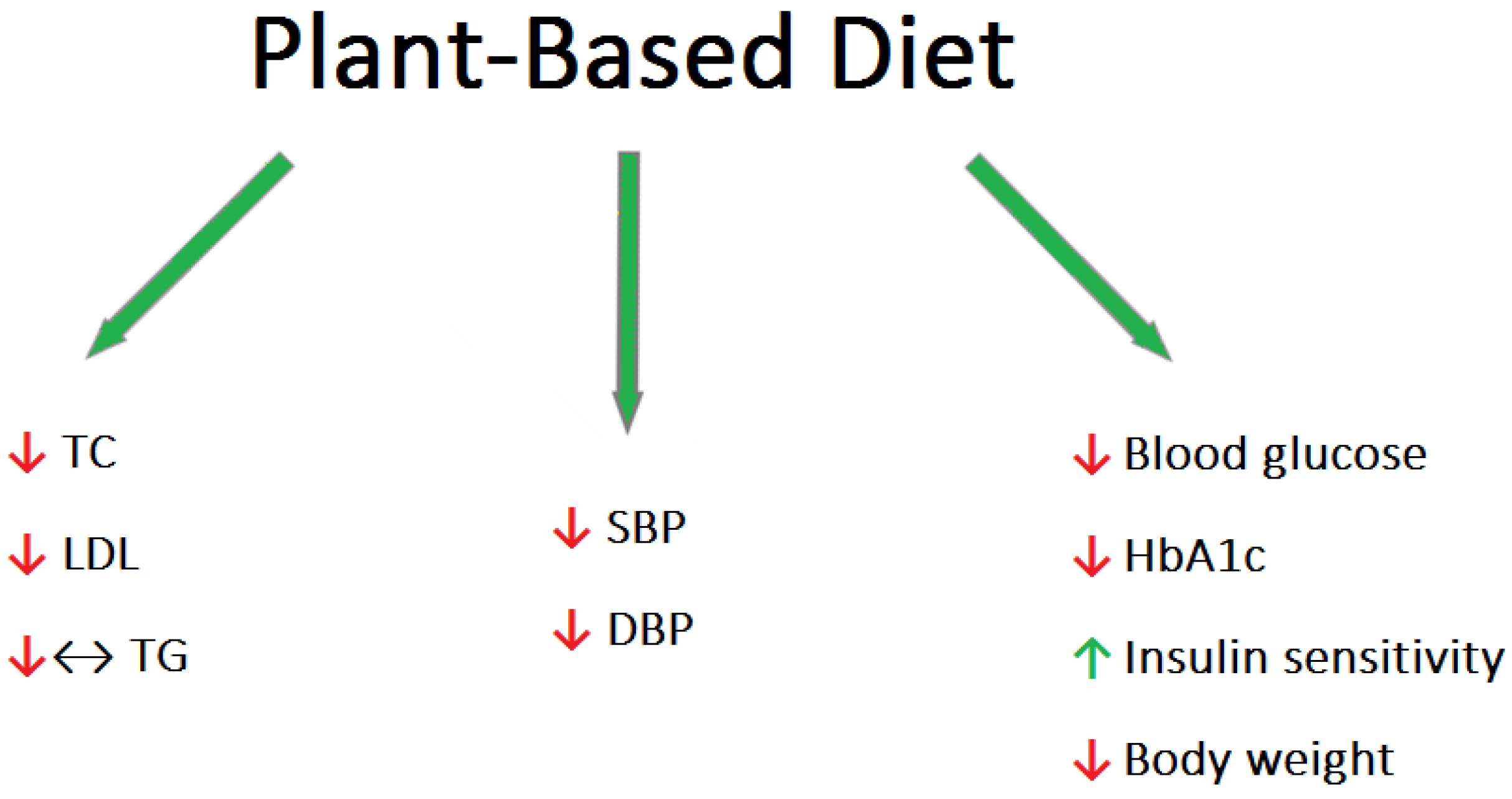
2. Plant-Based Diets Reducing the Main RVO Risk Factors: Hypertension, Hyperlipidemia, and Diabetes
3. Mediterranean Diet
4. Iron
5. Homocysteine, B Vitamins, and Folic Acid
6. Vitamin D, A, C, and Potassium
7. Coenzyme Q10
8. COVID-19 Pandemic and Dietary Habits
9. Summary
10. Method of Literature Search
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ho, M.; Liu, D.T.L.; Lam, D.S.C.; Jonas, J.B. Retinal Vein Occlusions, from Basics to the Latest Treatment. Retina 2016, 36, 432–448. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wang, J.J.; Mackey, D.A.; Wong, T.Y. Retinal Vascular Caliber: Systemic, Environmental, and Genetic Associations. Surv. Ophthalmol. 2009, 54, 74–95. [Google Scholar] [CrossRef] [PubMed]
- Green, W.R.; Chan, C.C.; Hutchins, G.M.; Terry, J.M. Central Retinal Vein Occlusion: A Prospective Histopathologic Study of 29 Eyes in 28 Cases. Trans. Am. Ophthalmol. Soc. 1981, 79, 371–422. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Cheng, Y.; Wang, S.; Wang, Y.; Liu, P.; Wu, H. Review: The Development of Risk Factors and Cytokines in Retinal Vein Occlusion. Front. Med. 2022, 9, 910600. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.Y.; Uppuluri, A.; Zarbin, M.A.; Bhagat, N. Risk Factors for Central Retinal Vein Occlusion in Young Adults. Eur. J. Ophthalmol. 2021, 31, 2546–2555. [Google Scholar] [CrossRef]
- Neo, T.; Gozawa, M.; Takamura, Y.; Inatani, M.; Oki, M. Gene Expression Profile Analysis of the Rabbit Retinal Vein Occlusion Model. PLoS ONE 2020, 15, e0236928. [Google Scholar] [CrossRef]
- McIntosh, R.L.; Rogers, S.L.; Lim, L.; Cheung, N.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.P.; Wong, T.Y. Natural History of Central Retinal Vein Occlusion: An Evidence-Based Systematic Review. Ophthalmology 2010, 117, 1113–1123.e15. [Google Scholar] [CrossRef]
- Braithwaite, T.; Nanji, A.A.; Lindsley, K.; Greenberg, P.B. Anti-Vascular Endothelial Growth Factor for Macular Oedema Secondary to Central Retinal Vein Occlusion. Cochrane Database Syst. Rev. 2014, 5, CD007325. [Google Scholar] [CrossRef]
- Hayreh, S.S. Photocoagulation for Retinal Vein Occlusion. Prog. Retin. Eye Res. 2021, 85, 100964. [Google Scholar] [CrossRef]
- Ghanchi, F.; Bourne, R.; Downes, S.M.; Gale, R.; Rennie, C.; Tapply, I.; Sivaprasad, S. An Update on Long-Acting Therapies in Chronic Sight-Threatening Eye Diseases of the Posterior Segment: AMD, DMO, RVO, Uveitis and Glaucoma. Eye 2022, 36, 1154–1167. [Google Scholar] [CrossRef]
- Senthil, M.P.; Khadka, J.; Gilhotra, J.S.; Simon, S.; Fenwick, E.K.; Lamoureux, E.; Pesudovs, K. Understanding Quality of Life Impact in People with Retinal Vein Occlusion: A Qualitative Inquiry. Clin. Exp. Optom. 2019, 102, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Demmig-Adams, B.; Adams, R.B. Eye Nutrition in Context: Mechanisms, Implementation, and Future Directions. Nutrients 2013, 5, 2483–2501. [Google Scholar] [CrossRef] [PubMed]
- Lavrovsky, Y.; Chatterjee, B.; Clark, R.A.; Roy, A.K. Role of Redox-Regulated Transcription Factors in Inflammation, Aging and Age-Related Diseases. Exp. Gerontol. 2000, 35, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Halloran, A.; Rippin, H.L.; Oikonomidou, A.C.; Dardavesis, T.I.; Williams, J.; Wickramasinghe, K.; Breda, J.; Chourdakis, M. Intake and Adequacy of the Vegan Diet. A Systematic Review of the Evidence. Clin. Nutr. 2021, 40, 3503–3521. [Google Scholar] [CrossRef]
- Kahleova, H.; Levin, S.; Barnard, N. Cardio-Metabolic Benefits of Plant-Based Diets. Nutrients 2017, 9, 848. [Google Scholar] [CrossRef]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Nishimura, K.; Barnard, N.D.; Takegami, M.; Watanabe, M.; Sekikawa, A.; Okamura, T.; Miyamoto, Y. Vegetarian Diets and Blood Pressure. JAMA Intern. Med. 2014, 174, 577–587. [Google Scholar] [CrossRef]
- Carroll, M.D.; Lacher, D.A.; Sorlie, P.D.; Cleeman, J.I.; Gordon, D.J.; Wolz, M.; Grundy, S.M.; Johnson, C.L. Trends in Serum Lipids and Lipoproteins of Adults, 1960–2002. JAMA 2005, 294, 1773–1781. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.B.; Brewer, H.B.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C.; Stone, N.J. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J. Am. Coll. Cardiol. 2004, 44, 720–732. [Google Scholar] [CrossRef]
- Howard, B.V.; Roman, M.J.; Devereux, R.B.; Fleg, J.L.; Galloway, J.M.; Henderson, J.A.; Howard, W.J.; Lee, E.T.; Mete, M.; Poolaw, B.; et al. Effect of Lower Targets for Blood Pressure and LDL Cholesterol on Atherosclerosis in Diabetes. JAMA 2008, 299, 1678–1689. [Google Scholar] [CrossRef]
- Mensink, R.P.; Katan, M.B. Effect of dietary fatty acids on serum lipids and lipoproteins. A meta-analysis of 27 trials. Arterioscler. Thromb. 1992, 12, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Gylling, H.; Plat, J.; Turley, S.; Ginsberg, H.N.; Ellegård, L.; Jessup, W.; Jones, P.J.H.; Lütjohann, D.; Mӓrz, W.; Masana, L.; et al. Plant sterols and plant stanols in the management of dyslipidaemia and prevention of cardiovascular disease. Atherosclerosis 2014, 232, 346–360. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zheng, J.; Yang, B.; Jiang, J.; Fu, Y.; Li, D. Effects of Vegetarian Diets on Blood Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2015, 4, e002408. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, Y.; Levin, S.M.; Barnard, N.D. Association between plant-based diets and plasma lipids: A systematic review and meta-analysis. Nutr. Rev. 2017, 75, 683–698. [Google Scholar] [CrossRef] [PubMed]
- De Biase, S.G.; Fernandes, S.F.C.; Gianini, R.J.; Duarte, J.L.G. Vegetarian diet and cholesterol and triglycerides levels. Arq. Bras. Cardiol. 2007, 88, 35–39. [Google Scholar] [CrossRef]
- Hannon, B.A.; Thompson, S.V.; Edwards, C.G.; Skinner, S.K.; Niemiro, G.M.; Burd, N.A.; Holscher, H.D.; Teran-Garcia, M.; Khan, N.A. Dietary Fiber Is Independently Related to Blood Triglycerides Among Adults with Overweight and Obesity. Curr. Dev. Nutr. 2018, 3, nzy094. [Google Scholar] [CrossRef]
- Dall, T.M.; Yang, W.; Gillespie, K.; Mocarski, M.; Byrne, E.; Cintina, I.; Beronja, K.; Semilla, A.P.; Iacobucci, W.; Hogan, P.F. The Economic Burden of Elevated Blood Glucose Levels in 2017: Diagnosed and Undiagnosed Diabetes, Gestational Diabetes Mellitus, and Prediabetes. Diabetes Care 2019, 42, 1661–1668. [Google Scholar] [CrossRef]
- McMacken, M.; Shah, S. A plant-based diet for the prevention and treatment of type 2 diabetes. J. Geriatr. Cardiol. 2017, 14, 342–354. [Google Scholar] [CrossRef]
- Marrone, G.; Guerriero, C.; Palazzetti, D.; Lido, P.; Marolla, A.; Di Daniele, F.; Noce, A. Vegan Diet Health Benefits in Metabolic Syndrome. Nutrients 2021, 13, 817. [Google Scholar] [CrossRef]
- Toumpanakis, A.; Turnbull, T.; Alba-Barba, I. Effectiveness of plant-based diets in promoting well-being in the management of type 2 diabetes: A systematic review. BMJ Open Diabetes Res. Care 2018, 6, e000534. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Barnard, N.D.; Levin, S.M.; Watanabe, M. Vegetarian diets and glycemic control in diabetes: A systematic review and meta-analysis. Cardiovasc. Diagn. Ther. 2014, 4, 373–382. [Google Scholar] [CrossRef] [PubMed]
- van Nielen, M.; Feskens, J.E.; Rietman, A.; Siebelink, E.; Mensink, M. Partly Replacing Meat Protein with Soy Protein Alters Insulin Resistance and Blood Lipids in Postmenopausal Women with Abdominal Obesity. J. Nutr. 2014, 144, 1423–1429. [Google Scholar] [CrossRef] [PubMed]
- Suárez, A.; Pulido, N.; Casla, A.; Casanova, B.; Arrieta, F.J.; Rovira, A. Impaired tyrosine-kinase activity of muscle insulin receptors from hypomagnesaemic rats. Diabetologia 1995, 38, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Sahyoun, N.R.; Anderson, A.L.; Tylavsky, F.A.; Lee, J.S.; Sellmeyer, D.E.; Harris, T.B. Dietary glycemic index and glycemic load and the risk of type 2 diabetes in older adults. Am. J. Clin. Nutr. 2008, 87, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Fitó, M.; Konstantinidou, V. Nutritional Genomics and the Mediterranean Diet’s Effects on Human Cardiovascular Health. Nutrients 2016, 8, 218. [Google Scholar] [CrossRef]
- Khayyal, M.T.; El-Ghazaly, M.A.; Abdallah, D.M.; Nassar, N.N.; Okpanyi, S.N.; Kreuter, M.-H. Blood Pressure Lowering Effect of an Olive Leaf Extract (Olea Europae) in L-NAME Induced Hypertension in Rats. Arzneimittelforschung 2002, 52, 797–802. [Google Scholar] [CrossRef]
- Fki, I.; Bouaziz, M.; Sahnoun, Z.; Sayadi, S. Hypocholesterolemic Effects of Phenolic-Rich Extracts of Chemlali Olive Cultivar in Rats Fed a Cholesterol-Rich Diet. Bioorg. Med. Chem. 2005, 13, 5362–5370. [Google Scholar] [CrossRef]
- Brzosko, S.; De Curtis, A.; Murzilli, S.; de Gaetano, G.; Donati, M.B.; Iacoviello, L. Effect of Extra Virgin Olive Oil on Experimental Thrombosis and Primary Hemostasis in Rats. Nutr. Metab. Cardiovasc. Dis. 2002, 12, 337–342. [Google Scholar]
- Dub, A.M.; Dugani, A.M. Antithrombotic Effect of Repeated Doses of the Ethanolic Extract of Local Olive (Olea europaea L.) Leaves in Rabbits. Libyan J. Med. 2013, 8, 20947. [Google Scholar] [CrossRef]
- Visioli, F.; Bellosta, S.; Galli, C. Oleuropein, the Bitter Principle of Olives, Enhances Nitric Oxide Production by Mouse Macrophages. Life Sci. 1998, 62, 541–546. [Google Scholar] [CrossRef]
- De Lucas, S.; Bartolome, J.; Carreno, V. Nitric Oxide Downregulates Factor VII Gene by Inhibiting the Binding of SP1 and HNF-4. J. Hepatol. 2003, 38, 75–76. [Google Scholar] [CrossRef]
- Manna, C.; Napoli, D.; Cacciapuoti, G.; Porcelli, M.; Zappia, V. Olive Oil Phenolic Compounds Inhibit Homocysteine-Induced Endothelial Cell Adhesion regardless of Their Different Antioxidant Activity. J. Agric. Food Chem. 2009, 57, 3478–3482. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Heiss, E.H.; Waltenberger, B.; Blažević, T.; Schachner, D.; Jiang, B.; Krystof, V.; Liu, W.; Schwaiger, S.; Peña-Rodríguez, L.M.; et al. Constituents of Mediterranean Spices Counteracting Vascular Smooth Muscle Cell Proliferation: Identification and Characterization of Rosmarinic Acid Methyl Ester as a Novel Inhibitor. Mol. Nutr. Food Res. 2018, 62, e1700860. [Google Scholar] [CrossRef]
- Casas, R.; Castro-Barquero, S.; Estruch, R.; Sacanella, E. Nutrition and Cardiovascular Health. Int. J. Mol. Sci. 2018, 19, 3988. [Google Scholar] [CrossRef] [PubMed]
- Violi, F.; Pastori, D.; Pignatelli, P.; Carnevale, R. Nutrition, Thrombosis, and Cardiovascular Disease. Circ. Res. 2020, 126, 1415–1442. [Google Scholar] [CrossRef] [PubMed]
- Steffen, L.M.; Folsom, A.R.; Cushman, M.; Jacobs, D.R.; Rosamond, W.D. Greater Fish, Fruit, and Vegetable Intakes Are Related to Lower Incidence of Venous Thromboembolism: The Longitudinal Investigation of Thromboembolism Etiology. Circulation 2007, 115, 188–195. [Google Scholar] [CrossRef]
- Yuan, S.; Bruzelius, M.; Damrauer, S.M.; Håkansson, N.; Wolk, A.; Åkesson, A.; Larsson, S.C. Anti-Inflammatory Diet and Venous Thromboembolism: Two Prospective Cohort Studies. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2831–2838. [Google Scholar] [CrossRef]
- Hurrell, R.F. Bioavailability of iron. Eur. J. Clin. Nutr. 1997, 51, S4–S8. [Google Scholar]
- Trumbo, P.; Yates, A.A.; Schlicker, S.; Poos, M. Dietary Reference Intakes: Vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. J. Am. Diet. Assoc. 2001, 101, 294–301. [Google Scholar] [CrossRef]
- Moiseyev, G.; Takahashi, Y.; Chen, Y.; Gentleman, S.; Redmond, T.M.; Crouch, R.K.; Ma, J.-X. RPE65 Is an Iron(II)-dependent Isomerohydrolase in the Retinoid Visual Cycle. J. Biol. Chem. 2006, 281, 2835–2840. [Google Scholar] [CrossRef]
- Chen, H.; Lukas, T.J.; Du, N.; Suyeoka, G.; Neufeld, A.H. Dysfunction of the Retinal Pigment Epithelium with Age: Increased Iron Decreases Phagocytosis and Lysosomal Activity. Investig. Ophthalmol. Vis. Sci. 2009, 50, 1895–1902. [Google Scholar] [CrossRef] [PubMed]
- Gnana-Prakasam, J.P.; Martin, P.M.; Smith, S.B.; Ganapathy, V. Expression and function of iron-regulatory proteins in retina. IUBMB Life 2010, 62, 363–370. [Google Scholar] [CrossRef]
- Goralska, M.; Ferrell, J.; Harned, J.; Lall, M.; Nagar, S.; Fleisher, L.; McGahan, M. Iron metabolism in the eye: A review. Exp. Eye Res. 2009, 88, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Miret, S.; Simpson, R.J.; McKie, A.T. Physiology and molecular biology of dietary iron absorption. Annu. Rev. Nutr. 2003, 23, 283–301. [Google Scholar] [CrossRef] [PubMed]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on Iron and Its Importance for Human Health. J. Res. Med. Sci. 2014, 19, 164–174. [Google Scholar]
- Kalff, H.; Cario, H.; Holzhauer, S. Iron deficiency anemia and thrombosis risk in children—Revisiting an old hypothesis. Front. Pediatr. 2022, 10, 926925. [Google Scholar] [CrossRef]
- Bill, A. Some aspects of the ocular circulation. Friedenwald lecture. Investig. Ophthalmol. Vis. Sci. 1985, 26, 410–424. [Google Scholar]
- Chabanel, A.; Glacet-Bernard, A.; Lelong, F.; Taccoen, A.; Coscas, G.; Samama, M.M. Increased red blood cell aggregation in retinal vein occlusion. Br. J. Haematol. 1990, 75, 127–131. [Google Scholar] [CrossRef]
- Li, X.; Li, N.; Zhao, G.; Wang, X. Effect of iron supplementation on platelet count in adult patients with iron deficiency anemia. Platelets 2022, 33, 1214–1219. [Google Scholar] [CrossRef]
- Brandão, M.M.; Castro, M.D.L.R.; Fontes, A.; Cesar, C.L.; Costa, F.F.; Saad, S.T. Impaired red cell deformability in iron deficient subjects. Clin. Hemorheol. Microcirc. 2009, 43, 217–221. [Google Scholar] [CrossRef]
- Kaur, C.; Foulds, W.S.; Ling, E.-A. Hypoxia-ischemia and retinal ganglion cell damage. Clin. Ophthalmol. 2008, 2, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Yang, V.; Turner, L.D.; Imrie, F. Central retinal vein occlusion secondary to severe iron-deficiency anaemia resulting from a plant-based diet and menorrhagia: A case presentation. BMC Ophthalmol. 2020, 20, 112. [Google Scholar] [CrossRef]
- Nagai, T.; Komatsu, N.; Sakata, Y.; Miura, Y.; Ozawa, K. Iron Deficiency Anemia with Marked Thrombocytosis Complicated by Central Retinal Vein Occlusion. Intern. Med. 2005, 44, 1090–1092. [Google Scholar] [CrossRef]
- Taubert, M.; Dowd, T.C.; Wood, A. Malnutrition and bilateral central retinal vein occlusion in a young woman: A case report. J. Med Case Rep. 2008, 2, 77. [Google Scholar] [CrossRef]
- Kirkham, T.H.; Wrigley, P.F.; Holt, J.M. Central retinal vein occlusion complicating iron deficiency anaemia. Br. J. Ophthalmol. 1971, 55, 777–780. [Google Scholar] [CrossRef]
- Haider, L.M.; Schwingshackl, L.; Hoffmann, G.; Ekmekcioglu, C. The effect of vegetarian diets on iron status in adults: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2018, 58, 1359–1374. [Google Scholar] [CrossRef] [PubMed]
- Hunt, J.R. Bioavailability of iron, zinc, and other trace minerals from vegetarian diets. Am. J. Clin. Nutr. 2003, 78, 633S–639S. [Google Scholar] [CrossRef] [PubMed]
- Lönnerdal, B. Soybean ferritin: Implications for iron status of vegetarians. Am. J. Clin. Nutr. 2009, 89, 1680S–1685S. [Google Scholar] [CrossRef] [PubMed]
- Messina, V.K.; Burke, K.I. Position of The American Dietetic Association: Vegetarian Diets. J. Am. Diet. Assoc. 1997, 97, 1317–1321. [Google Scholar] [CrossRef]
- Hallberg, L.; Hulthén, L. Prediction of dietary iron absorption: An algorithm for calculating absorption and bioavailability of dietary iron. Am. J. Clin. Nutr. 2000, 71, 1147–1160. [Google Scholar] [CrossRef]
- Hallberg, L. Bioavailability of dietary iron in man. Annu. Rev. Nutr. 1981, 1, 123–147. [Google Scholar] [CrossRef] [PubMed]
- García-Casal, M.N.; Layrisse, M.; Solano, L.; Barón, M.A.; Arguello, F.; Llovera, D.; Ramírez, J.; Leets, I.; Tropper, E. Vitamin A and β-Carotene Can Improve Nonheme Iron Absorption from Rice, Wheat and Corn by Humans. J. Nutr. 1998, 128, 646–650. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.D.; Monsen, E.R. Vitamin C, the common cold, and iron absorption. Am. J. Clin. Nutr. 1977, 30, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Kumari, M.; Gupta, S.; Lakshmi, A.; Prakash, J. Iron bioavailability in green leafy vegetables cooked in different utensils. Food Chem. 2004, 86, 217–222. [Google Scholar] [CrossRef]
- O’leary, F.; Samman, S. Vitamin B12 in Health and Disease. Nutrients 2010, 2, 299–316. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, M. Hyperhomocysteinemia, Atherosclerosis and Thrombosis. Thromb. Haemost. 1999, 81, 165–176. [Google Scholar] [CrossRef]
- Postea, O.; Krotz, F.; Henger, A.; Keller, C.; Weiss, N. Stereospecific and Redox-Sensitive Increase in Monocyte Adhesion to Endothelial Cells by Homocysteine. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 508–513. [Google Scholar] [CrossRef]
- Weiss, N. Mechanisms of Increased Vascular Oxidant Stress in Hyperhomocysteinemia and Its Impact on Endothelial Function. Curr. Drug Metab. 2005, 6, 27–36. [Google Scholar] [CrossRef]
- Varga, E.A.; Sturm, A.C.; Misita, C.P.; Moll, S. Cardiology patient pages. Homocysteine and MTHFR mutations: Relation to thrombosis and coronary artery disease. Circulation 2005, 111, e289–e293. [Google Scholar] [CrossRef]
- Moghimi, S.; Najmi, Z.; Faghihi, H.; Karkhaneh, R.; Farahvash, M.S.; Maghsoudipour, M. Hyperhomocysteinemia and central retinal vein occlusion in Iranian population. Int. Ophthalmol. 2008, 28, 23–28. [Google Scholar] [CrossRef]
- Gao, W.; Wang, Y.; Zhang, P.; Wang, H. Hyperhomocysteinemia and low plasma folate as risk factors for central retinal vein occlusion: A case–control study in a Chinese population. Graefes Arch. Clin. Exp. Ophthalmol. 2006, 244, 1246–1249. [Google Scholar] [CrossRef] [PubMed]
- Narayanasamy, A.; Subramaniam, B.; Karunakaran, C.; Ranganathan, P.; Sivaramakrishnan, R.; Sharma, T.; Badrinath, V.S.; Roy, J. Hyperhomocysteinemia and Low Methionine Stress Are Risk Factors for Central Retinal Venous Occlusion in an Indian Population. Investig. Opthalmol. Vis. Sci. 2007, 48, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Wenzler, E.M.; Rademakers, A.J.; Boers, G.H.; Cruysberg, J.R.; Webers, C.A.; Deutman, A.F. Hyperhomocysteinemia in Retinal Artery and Retinal Vein Occlusion. Am. J. Ophthalmol. 1993, 115, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Biousse, V.; Newman, N.J.; Sternberg, P. Retinal Vein Occlusion and Transient Monocular Visual Loss Associated With Hyperhomocystinemia. Am. J. Ophthalmol. 1997, 124, 257–260. [Google Scholar] [CrossRef]
- de Bruijne, E.L.; Vos, G.H.K.-D.; Ouwendijk, R.J. Ocular Venous Occlusion and Hyperhomocysteinemia. Ann. Intern. Med. 1999, 130, 78. [Google Scholar] [CrossRef] [PubMed]
- Cahill, M.; Karabatzaki, M.; Meleady, R.; Refsum, H.; Ueland, P.; Shields, D.; Mooney, D.; Graham, I. Raised plasma homocysteine as a risk factor for retinal vascular occlusive disease. Br. J. Ophthalmol. 2000, 84, 154–157. [Google Scholar] [CrossRef]
- Martin, S.C.; Rauz, S.; Marr, J.E.; Martin, N.; Jones, A.F.; Dodson, P.M. Plasma total homocysteine and retinal vascular disease. Eye 2000, 14, 590–593. [Google Scholar] [CrossRef]
- Marcucci, R.; Bertini, L.; Giusti, B.; Brunelli, T.; Fedi, S.; Cellai, A.P.; Poli, D.; Pepe, G.; Abbate, R.; Prisco, D. Thrombophilic Risk Factors in Patients with Central Retinal Vein Occlusion. Thromb. Haemost. 2001, 86, 772–776. [Google Scholar] [CrossRef]
- Weger, M.; Stanger, O.; Deutschmann, H.; Temmel, W.; Renner, W.; Schmut, O.; Quehenberger, F.; Semmelrock, J.; Haas, A. Hyperhomocyst(e)inemia, but not methylenetetrahydrofolate reductase C677T mutation, as a risk factor in branch retinal vein occlusion. Ophthalmology 2002, 109, 1105–1109. [Google Scholar] [CrossRef]
- Arthur, D.; John, D.; Fleming, J.J.; Rebekah, G.; Gowri, M.; John, S.S. Role of Hyperhomocysteinemia and Vitamin B12 Deficiency in Central and Hemi-Central Retinal Vein Occlusion: A Case-Control Study. Oman J. Ophthalmol. 2022, 15, 6–12. [Google Scholar] [CrossRef]
- Parodi, M.B.; Di Crecchio, L. Hyperhomocysteinemia in central retinal vein occlusion in young adults. Semin. Ophthalmol. 2003, 18, 154–159. [Google Scholar] [CrossRef]
- McGimpsey, S.J.; Woodside, J.V.; Cardwell, C.; Cahill, M.; Chakravarthy, U. Homocysteine, Methylenetetrahydrofolate Reductase C677T Polymorphism, and Risk of Retinal Vein Occlusion: A Meta-analysis. Ophthalmology 2009, 116, 1778–1787.e1. [Google Scholar] [CrossRef] [PubMed]
- Larsson, J.; Hultberg, B.; Hillarp, A. Hyperhomocysteinemia and the MTHFR C677T mutation in central retinal vein occlusion. Acta Ophthalmol. Scand. 2000, 78, 340–343. [Google Scholar] [CrossRef]
- Boyd, S.; Owens, D.; Gin, T.; Bunce, K.; Sherafat, H.; Perry, D.; Hykin, P.G. Plasma homocysteine, methylene tetrahydrofolate reductase C677T and factor II G20210A polymorphisms, factor VIII, and VWF in central retinal vein occlusion. Br. J. Ophthalmol. 2001, 85, 1313–1315. [Google Scholar] [CrossRef]
- Cahill, M.T.; Stinnett, S.S.; Fekrat, S. Meta-analysis of plasma homocysteine, serum folate, serum vitamin B12, and thermolabile MTHFR genotype as risk factors for retinal vascular occlusive disease. Am. J. Ophthalmol. 2003, 136, 1136–1150. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Marcucci, R.; Bolli, P.; Giambene, B.; Sodi, A.; Fedi, S.; Menchini, U.; Gensini, G.F.; Abbate, R.; Prisco, D. Low vitamin B6 and folic acid levels are associated with retinal vein occlusion independently of homocysteine levels. Atherosclerosis 2008, 198, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, K.D.; Mukherjee, S.; Ghosh, S.; Mukherjee, S.; Dutta, J.; Datta, H.; Das, H.N. Hyperhomocysteinemia, a Biochemical Tool for Differentiating Ischemic and Nonischemic Central Retinal Vein Occlusion during the Early Acute Phase. Korean J. Ophthalmol. 2015, 29, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Calevo, M.G.; Giannattasio, A.; Camicione, P.; Armani, U.; Lorini, R.; Piana, G. Plasma Homocysteine in Patients with Retinal Vein Occlusion. Eur. J. Ophthalmol. 2014, 24, 735–743. [Google Scholar] [CrossRef]
- Schoene, N.W.; Chanmugam, P.; Reynolds, R.D. Effect of oral vitamin B6 supplementation on in vitro platelet aggregation. Am. J. Clin. Nutr. 1986, 43, 825–830. [Google Scholar] [CrossRef]
- Chang, S.-J.; Chuang, H.-J.; Chen, H.-H. Vitamin B6 Down-Regulates the Expression of Human GPIIb Gene. J. Nutr. Sci. Vitaminol. 1999, 45, 471–479. [Google Scholar] [CrossRef]
- Selhub, J.; Jacques, P.F.; Wilson, P.W.F.; Rush, D.; Rosenberg, I.H. Vitamin Status and Intake as Primary Determinants of Homocysteinemia in an Elderly Population. JAMA 1993, 270, 2693–2698. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, K.D.; Dutta, J.; Datta, H.; Das, H.N. Hyperhomocysteinemia, as an Independent Risk Factor for Retinal Venous Occlusion in an Indian Population. Indian J. Clin. Biochem. 2013, 28, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Nurk, E.; Tell, G.S.; Vollset, S.E.; Nygård, O.; Refsum, H.; Nilsen, R.M.; Ueland, P.M. Changes in lifestyle and plasma total homocysteine: The Hordaland Homocysteine Study. Am. J. Clin. Nutr. 2004, 79, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Spence, J.D.; Giovannucci, E.L.; Kim, Y.-I.; Josse, R.G.; Vieth, R.; Sahye-Pudaruth, S.; Paquette, M.; Patel, D.; Mejia, S.B.; et al. Supplemental Vitamins and Minerals for Cardiovascular Disease Prevention and Treatment: JACC Focus Seminar. J. Am. Coll. Cardiol. 2021, 77, 423–436. [Google Scholar] [CrossRef]
- Pieroth, R.; Paver, S.; Day, S.; Lammersfeld, C. Folate and Its Impact on Cancer Risk. Curr. Nutr. Rep. 2018, 7, 70–84. [Google Scholar] [CrossRef]
- Rock, C.L. Multivitamin-multimineral supplements: Who uses them? Am. J. Clin. Nutr. 2007, 85, 277S–279S. [Google Scholar] [CrossRef]
- Boyles, A.L.; Yetley, E.A.; Thayer, K.A.; Coates, P.M. Safe Use of High Intakes of Folic Acid: Research Challenges and Paths Forward. Nutr. Rev. 2016, 74, 469–474. [Google Scholar] [CrossRef]
- Chait, A.; Malinow, M.R.; Nevin, D.N.; Morris, C.D.; Eastgard, R.L.; Kris-Etherton, P.; Pi-Sunyer, F.X.; Oparil, S.; Resnick, L.M.; Stern, J.S.; et al. Increased dietary micronutrients decrease serum homocysteine concentrations in patients at high risk of cardiovascular disease. Am. J. Clin. Nutr. 1999, 70, 881–887. [Google Scholar] [CrossRef]
- Appel, L.J.; Miller, E.R.; Jee, S.H.; Stolzenberg-Solomon, R.; Rd; Lin, P.-H.; Erlinger, T.; Nadeau, M.R.; Selhub, J. Effect of Dietary Patterns on Serum Homocysteine: Results of a randomized, controlled feeding study. Circulation 2000, 102, 852–857. [Google Scholar] [CrossRef]
- Food and Drug Administration. Food standards: Amendment of standards of identity for enriched grain products to require addition of folic acid. Federal Register. 1996, 61, 8781–8797. [Google Scholar]
- Health Canada. Regulations amending the Food and Drug Regulations (1066). Can Gaz Part 1 1997, 13, 3702–3737. [Google Scholar]
- Jacques, P.F.; Selhub, J.; Bostom, A.G.; Wilson, P.W.; Rosenberg, I.H. The Effect of Folic Acid Fortification on Plasma Folate and Total Homocysteine Concentrations. N. Engl. J. Med. 1999, 340, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- Cravo, M.L.; Glória, L.M.; Selhub, J.; Nadeau, M.R.; Camilo, M.E.; Resende, M.P.; Cardoso, J.N.; Leitão, C.N.; Mira, F.C. Hyperhomocysteinemia in chronic alcoholism: Correlation with folate, vitamin B(-1)2, and vitamin B-6 status. Am. J. Clin. Nutr. 1996, 63, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Nygård, O.O.; Refsum, H.; Ueland, P.M.; Vollset, S.E. Major lifestyle determinants of plasma total homocysteine distribution: The Hordaland Homocysteine Study. Am. J. Clin. Nutr. 1998, 67, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Grubben, M.J.; Boers, G.H.; Blom, H.J.; Broekhuizen, R.; de Jong, R.; van Rijt, L.; de Ruijter, E.; Swinkels, D.W.; Nagengast, F.M.; Katan, M.B. Unfiltered coffee increases plasma homocysteine concentrations in healthy volunteers: A randomized trial. Am. J. Clin. Nutr. 2000, 71, 480–484. [Google Scholar] [CrossRef]
- Spiro, A.; Buttriss, J.L. Vitamin D: An overview of vitamin D status and intake in Europe. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef]
- Bikle, D.D. Vitamin D Metabolism, Mechanism of Action, and Clinical Applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef]
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689S–1696S. [Google Scholar] [CrossRef]
- Alsalem, J.A.; Patel, D.; Susarla, R.; Coca-Prados, M.; Bland, R.; Walker, E.A.; Rauz, S.; Wallace, G.R. Characterization of Vitamin D Production by Human Ocular Barrier Cells. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2140–2147. [Google Scholar] [CrossRef]
- Rullo, J.; Pennimpede, T.; Far, P.M.; Strube, Y.N.; Irrcher, I.; Urton, T.; Bona, M.; Gonder, T.; Campbell, R.J.; Hove, M.T.; et al. Intraocular calcidiol: Uncovering a role for vitamin D in the eye. J. Steroid Biochem. Mol. Biol. 2020, 197, 105536. [Google Scholar] [CrossRef]
- Reins, R.Y.; McDermott, A.M. Vitamin D: Implications for ocular disease and therapeutic potential. Exp. Eye Res. 2015, 134, 101–110. [Google Scholar] [CrossRef]
- Caban, M.; Lewandowska, U. Vitamin D, the Vitamin D Receptor, Calcitriol Analogues and Their Link with Ocular Diseases. Nutrients 2022, 14, 2353. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Schaffer, A.; Sartori, C.; Barbieri, L.; Cassetti, E.; Marino, P.; Galasso, G.; De Luca, G.; Novara Atherosclerosis Study Group (NAS). Vitamin D deficiency is independently associated with the extent of coronary artery disease. Eur. J. Clin. Investig. 2014, 44, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Brøndum-Jacobsen, P.; Benn, M.; Tybjærg-Hansen, A.; Nordestgaard, B.G. 25-Hydroxyvitamin D concentrations and risk of venous thromboembolism in the general population with 18 791 participants. J. Thromb. Haemost. 2013, 11, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Garland, C.F.; Kim, J.J.; Mohr, S.B.; Gorham, E.D.; Grant, W.B.; Giovannucci, E.L.; Baggerly, L.; Hofflich, H.; Ramsdell, J.W.; Zeng, K.; et al. Meta-analysis of All-Cause Mortality According to Serum 25-Hydroxyvitamin D. Am. J. Public Health 2014, 104, e43–e50. [Google Scholar] [CrossRef]
- Arntz, H.-R.; Willich, S.; Schreiber, C.; Brüggemann, T.; Stern, R.; Schultheiß, H.-P. Diurnal, weekly and seasonal variation of sudden death. Population-based analysis of 24061 consecutive cases. Eur. Heart J. 2000, 21, 315–320. [Google Scholar] [CrossRef]
- Khan, F.A.; Engstrom, G.; Jerntorp, I.; Pessah-Rasmussen, H.; Janzon, L. Seasonal Patterns of Incidence and Case Fatality of Stroke in Malmö, Sweden: The STROMA Study. Neuroepidemiology 2005, 24, 26–31. [Google Scholar] [CrossRef]
- Epstein, D.; Kvanta, A.; Lindqvist, P.G. Seasonality and Incidence of Central Retinal Vein Occlusion in Sweden: A 6-Year Study. Ophthalmic Epidemiol. 2015, 22, 94–97. [Google Scholar] [CrossRef]
- Ho, J.-D.; Tsai, C.-Y.; Liou, S.-W.; Tsai, R.J.-F.; Lin, H.-C. Seasonal Variations in the Occurrence of Retinal Vein Occlusion: A Five-Year Nationwide Population-Based Study from Taiwan. Am. J. Ophthalmol. 2008, 145, 722–728.e3. [Google Scholar] [CrossRef]
- Shoben, A.B.; Kestenbaum, B.; Levin, G.; Hoofnagle, A.N.; Psaty, B.M.; Siscovick, D.S.; de Boer, I.H. Seasonal Variation in 25-Hydroxyvitamin D Concentrations in the Cardiovascular Health Study. Am. J. Epidemiol. 2011, 174, 1363–1372. [Google Scholar] [CrossRef]
- Talcott, K.E.; Eliott, D. Central Retinal Vein Occlusion Associated with Severe Vitamin D Deficiency. Ophthalmic Surg. Lasers Imaging Retina 2016, 47, 372–375. [Google Scholar] [CrossRef]
- Epstein, D.; Kvanta, A.; Lindqvist, P.G. Vitamin D Deficiency in Patients with Central Retinal Vein Occlusion: A Case Control Study. Curr. Eye Res. 2017, 42, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Oli, A.; Joshi, D. Serum vitamin D levels in Indian patients with retinal venous occlusions. Saudi J. Ophthalmol. 2017, 31, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Karimi, S.; Parvizi, F.; Arabi, A.; Shahraki, T.; Safi, S. Oral Vitamin D Supplementation and Clinical Outcomes of Intravitreal Bevacizumab Injection for Macular Edema Secondary to Retinal Vein Occlusions. J. Ophthalmic Vis. Res. 2022, 17, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Molinari, C.; Uberti, F.; Grossini, E.; Vacca, G.; Carda, S.; Invernizzi, M.; Cisari, C. 1α,25-Dihydroxycholecalciferol Induces Nitric Oxide Production in Cultured Endothelial Cells. Cell. Physiol. Biochem. 2011, 27, 661–668. [Google Scholar] [CrossRef] [PubMed]
- El-Sharkawy, A.; Malki, A. Vitamin D Signaling in Inflammation and Cancer: Molecular Mechanisms and Therapeutic Implications. Molecules 2020, 25, 3219. [Google Scholar] [CrossRef]
- Hewison, M. Vitamin D and the Immune System: New Perspectives on an Old Theme. Rheum. Dis. Clin. North Am. 2012, 38, 125–139. [Google Scholar] [CrossRef]
- Agrawal, D.; Yin, K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar] [CrossRef]
- Li, Y.C.; Qiao, G.; Uskokovic, M.; Xiang, W.; Zheng, W.; Kong, J. Vitamin D: A negative endocrine regulator of the renin–angiotensin system and blood pressure. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 387–392. [Google Scholar] [CrossRef]
- Expert Consultation on Vitamin and Mineral Requirement in Human Nutrition: Second Edition FAO Rome. Available online: https://apps.who.int/iris/bitstream/handle/10665/42716/9241546123.pdf;jsessionid=3A893750E1EEE89B2C501C7FAAB728F7?sequence=1 (accessed on 15 June 2023).
- Ikonne, E.U.; Ikpeazu, V.O.; Ugbogu, E.A. The potential health benefits of dietary natural plant products in age related eye diseases. Heliyon 2020, 6, e04408. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Wang, J.J.; Rochtchina, E.; Wong, T.Y.; Mitchell, P. Is quality of diet associated with the microvasculature? An analysis of diet quality and retinal vascular calibre in older adults. Br. J. Nutr. 2013, 110, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Edo, A.; Ibrahim, D.G.; Hirooka, K.; Toda, R.; Kamaruddin, M.I.; Kawano, R.; Nagao, A.; Ohno, H.; Yoneda, M.; Kiuchi, Y. Dietary Vitamins A, C, and Potassium Intake Is Associated with Narrower Retinal Venular Caliber. Front. Med. 2022, 9, 818139. [Google Scholar] [CrossRef] [PubMed]
- Seidelmann, S.B.; Claggett, B.; Bravo, P.E.; Gupta, A.; Farhad, H.; Klein, B.E.; Klein, R.; Di Carli, M.; Solomon, S.D. Retinal Vessel Calibers in Predicting Long-Term Cardiovascular Outcomes: The Atherosclerosis Risk in Communities Study. Circulation 2016, 134, 1328–1338. [Google Scholar] [CrossRef] [PubMed]
- Serre, K.; Sasongko, M.B. Modifiable Lifestyle and Environmental Risk Factors Affecting the Retinal Microcirculation. Microcirculation 2012, 19, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Iso, H.; Date, C.; Kikuchi, S.; Watanabe, Y.; Wada, Y.; Inaba, Y.; Tamakoshi, A.; the JACC Study Group. Dietary Intakes of Antioxidant Vitamins and Mortality from Cardiovascular Disease: The Japan Collaborative Cohort Study (JACC) study. Stroke 2011, 42, 1665–1672. [Google Scholar] [CrossRef]
- D’Elia, L.; Barba, G.; Cappuccio, F.P.; Strazzullo, P. Potassium Intake, Stroke, and Cardiovascular Disease: A Meta-Analysis of Prospective Studies. J. Am. Coll. Cardiol. 2011, 57, 1210–1219. [Google Scholar] [CrossRef]
- Ikram, M.K.; de Jong, F.J.; Vingerling, J.R.; Witteman, J.C.M.; Hofman, A.; Breteler, M.M.B.; de Jong, P.T.V.M. Are Retinal Arteriolar or Venular Diameters Associated with Markers for Cardiovascular Disorders? The Rotterdam Study. Investig. Ophthalmol. Vis. Sci. 2004, 45, 2129–2134. [Google Scholar] [CrossRef]
- Yanagi, M.; Misumi, M.; Kawasaki, R.; Takahashi, I.; Itakura, K.; Fujiwara, S.; Akahoshi, M.; Neriishi, K.; Wong, T.Y.; Kiuchi, Y. Is the Association Between Smoking and the Retinal Venular Diameter Reversible Following Smoking Cessation? Investig. Ophthalmol. Vis. Sci. 2014, 55, 405–411. [Google Scholar] [CrossRef]
- Tamai, K.; Matsubaraa, A.; Tomidaa, K.; Matsudaa, Y.; Moritaa, H.; Armstrongb, D.; Oguraa, Y. Lipid Hydroperoxide Stimulates Leukocyte–Endothelium Interaction in the Retinal Microcirculation. Exp. Eye Res. 2002, 75, 69–75. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E.K.; Knudtson, M.D.; Wong, T.Y.; Tsai, M.Y. Are Inflammatory Factors Related to Retinal Vessel Caliber? The Beaver Dam Eye Study. Arch. Ophthalmol. 2006, 124, 87–94. [Google Scholar] [CrossRef]
- Shi, H.Y.; Yan, S.M.; Guo, Y.M.; Zhang, B.Q.; Guo, X.Y.; Shi, B.L. Vitamin A pretreatment protects NO-induced bovine mammary epithelial cells from oxidative stress by modulating Nrf2 and NF-κB signaling pathways. J. Anim. Sci. 2018, 96, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Conner, E.M.; Grisham, M.B. Inflammation, Free Radicals, and Antioxidants. Nutrition 1996, 12, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M. Potassium and Health. Adv. Nutr. 2013, 4, 368S–377S. [Google Scholar] [CrossRef] [PubMed]
- Somayajulu, M.; McCarthy, S.; Hung, M.; Sikorska, M.; Borowy-Borowski, H.; Pandey, S. Role of mitochondria in neuronal cell death induced by oxidative stress; neuroprotection by Coenzyme Q10. Neurobiol. Dis. 2005, 18, 618–627. [Google Scholar] [CrossRef]
- Manzar, H.; Abdulhussein, D.; Yap, T.E.; Cordeiro, M.F. Cellular Consequences of Coenzyme Q10 Deficiency in Neurodegeneration of the Retina and Brain. Int. J. Mol. Sci. 2020, 21, 9299. [Google Scholar] [CrossRef]
- Fernández-Vega, B.; Nicieza, J.; Barrios, A.; Álvarez, L.; García, M.; Fernández-Vega, C.; Vega, J.A.; González-Iglesias, H. The Use of Vitamins and Coenzyme Q10 for the Treatment of Vascular Occlusion Diseases Affecting the Retina. Nutrients 2020, 12, 723. [Google Scholar] [CrossRef]
- Głąbska, D.; Skolmowska, D.; Guzek, D. Population-Based Study of the Changes in the Food Choice Determinants of Secondary School Students: Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Nutrients 2020, 12, 2640. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 outbreak: Changes in diet and physical activity increase the risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef]
- Allabadi, H.; Dabis, J.; Aghabekian, V.; Khader, A.; Khammash, U. Impact of COVID-19 lockdown on dietary and lifestyle behaviours among adolescents in Palestine. Dynam. Human Health 2020, 7, 2170. [Google Scholar]
- Bracale, R.; Vaccaro, C.M. Changes in food choice following restrictive measures due to COVID-19. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1423–1426. [Google Scholar] [CrossRef]
- Moretti, A.; Liguori, S.; Paoletta, M.; Migliaccio, S.; Toro, G.; Gimigliano, F.; Iolascon, G. Bone fragility during the COVID-19 pandemic: The role of macro- and micronutrients. Ther. Adv. Musculoskelet. Dis. 2023, 15, 1759720X231158200. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620938149. [Google Scholar] [CrossRef] [PubMed]
- Schnichels, S.; Rohrbach, J.M.; Bayyoud, T.; Thaler, S.; Ziemssen, F.; Hurst, J. Can SARS-CoV-2 infect the eye? An overview of the receptor status in ocular tissue. Ophthalmologe 2021, 118, 81–84. [Google Scholar] [CrossRef]
- Senanayake, P.D.; Drazba, J.; Shadrach, K.; Milsted, A.; Rungger-Brandle, E.; Nishiyama, K.; Miura, S.-I.; Karnik, S.; Sears, J.E.; Hollyfield, J.G. Angiotensin II and Its Receptor Subtypes in the Human Retina. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3301–3311. [Google Scholar] [CrossRef]
- Fonollosa, A.M.; Hernández-Rodríguez, J.M.; Cuadros, C.; Giralt, L.; Sacristán, C.; Artaraz, J.; Pelegrín, L.M.; Olate-Pérez, Á.; Romero, R.; Pastor-Idoate, S.P.; et al. Characterizing COVID-19–Related Retinal Vascular Occlusions. Retina 2022, 42, 465–475. [Google Scholar] [CrossRef]
- World Health Organization. Nutrition Advice for Adults during the COVID-19 Outbreak. Available online: https://www.emro.who.int/nutrition/covid-19/nutrition-advice-for-adults-during-the-covid-19-outbreak.html (accessed on 15 June 2023).


{kind=link}
| PBD |  | CRP, TNF-α, TNFR-60, IL-1, IL-4, IL-6, fibrinogen, sE-selectin |
 | γδ-T cell populations | |
| MD |  | CRP, TNF-α, TNFR-60, IL-1, IL-6, IL-7, IL-8, IL-10, IL-13, IL-18, VEGF, MMP-9, MCP-1, sVCAM-1, sICAM-1, PAI-1, leptin |
 | Adiponectine |
| Enhancers | Inhibitors |
|---|---|
| Meat, poultry, fish | Phytic acid |
| Ascorbic Acid | Polyphenols |
| Retinol and carotenes | Calcium and proteins in milk products |
| Alcohol | Egg |
| Soy protein |
| Vitamin D Content in Food Products | |
|---|---|
| Name of the Product | Vitamin D (µg/100 g) |
| Mackerel chilled/frozen, raw, flesh only | 8.0 |
| Salmon, raw | 5.0 |
| Sardines chilled/frozen, raw, flesh only | 4.0 |
| Yellowfin tuna chilled/frozen, raw, flesh only | 3.2 |
| Cod chilled/frozen, raw, flesh only | Trace |
| Prawns, king, raw | Trace |
| Eggs, chicken, whole raw | 3.2 |
| Pork leg joint, raw | 0.9 |
| Lamb chop, raw | 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lendzioszek, M.; Mrugacz, M.; Bryl, A.; Poppe, E.; Zorena, K. Prevention and Treatment of Retinal Vein Occlusion: The Role of Diet—A Review. Nutrients 2023, 15, 3237. https://doi.org/10.3390/nu15143237
Lendzioszek M, Mrugacz M, Bryl A, Poppe E, Zorena K. Prevention and Treatment of Retinal Vein Occlusion: The Role of Diet—A Review. Nutrients. 2023; 15(14):3237. https://doi.org/10.3390/nu15143237
Chicago/Turabian StyleLendzioszek, Maja, Małgorzata Mrugacz, Anna Bryl, Ewa Poppe, and Katarzyna Zorena. 2023. "Prevention and Treatment of Retinal Vein Occlusion: The Role of Diet—A Review" Nutrients 15, no. 14: 3237. https://doi.org/10.3390/nu15143237
APA StyleLendzioszek, M., Mrugacz, M., Bryl, A., Poppe, E., & Zorena, K. (2023). Prevention and Treatment of Retinal Vein Occlusion: The Role of Diet—A Review. Nutrients, 15(14), 3237. https://doi.org/10.3390/nu15143237