
Design and Development of ‘Diet DQ Tracker’: A Smartphone Application for Augmenting Dietary Assessment



Abstract
1. Introduction
2. Materials and Methods
2.1. Diet Diversity Indicators
2.1.1. Minimum Dietary Diversity for Women (MDD-W)
2.1.2. Infant and Young Child Feeding Practices—Minimum Dietary Diversity (IYCF-MDD)
2.1.3. Household Dietary Diversity Score (HDDS)
2.2. Diet Quality Indicator
2.2.1. SAIN, LIM
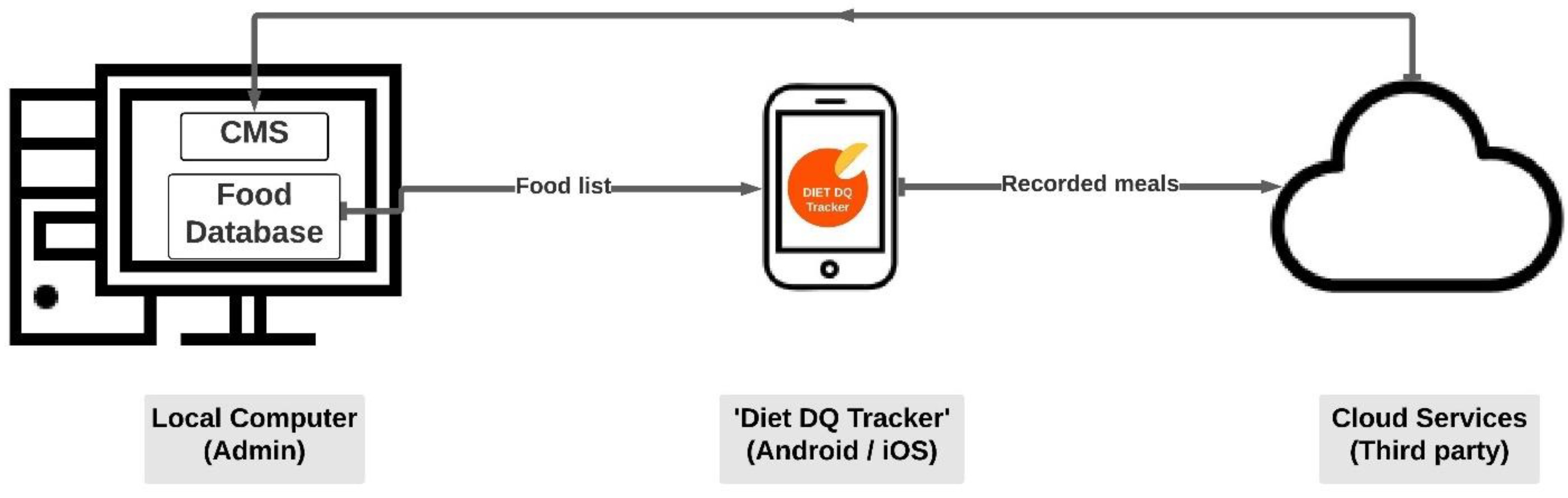
2.3. Design and Architecture of the ‘Diet DQ Tracker’
2.4. Food Database
2.5. Content Management System
2.6. Pilot Study
2.6.1. Study Sample and Recruitment
2.6.2. Dietary Assessment
2.6.3. Participant Feedback on Dietary Assessment
3. Results
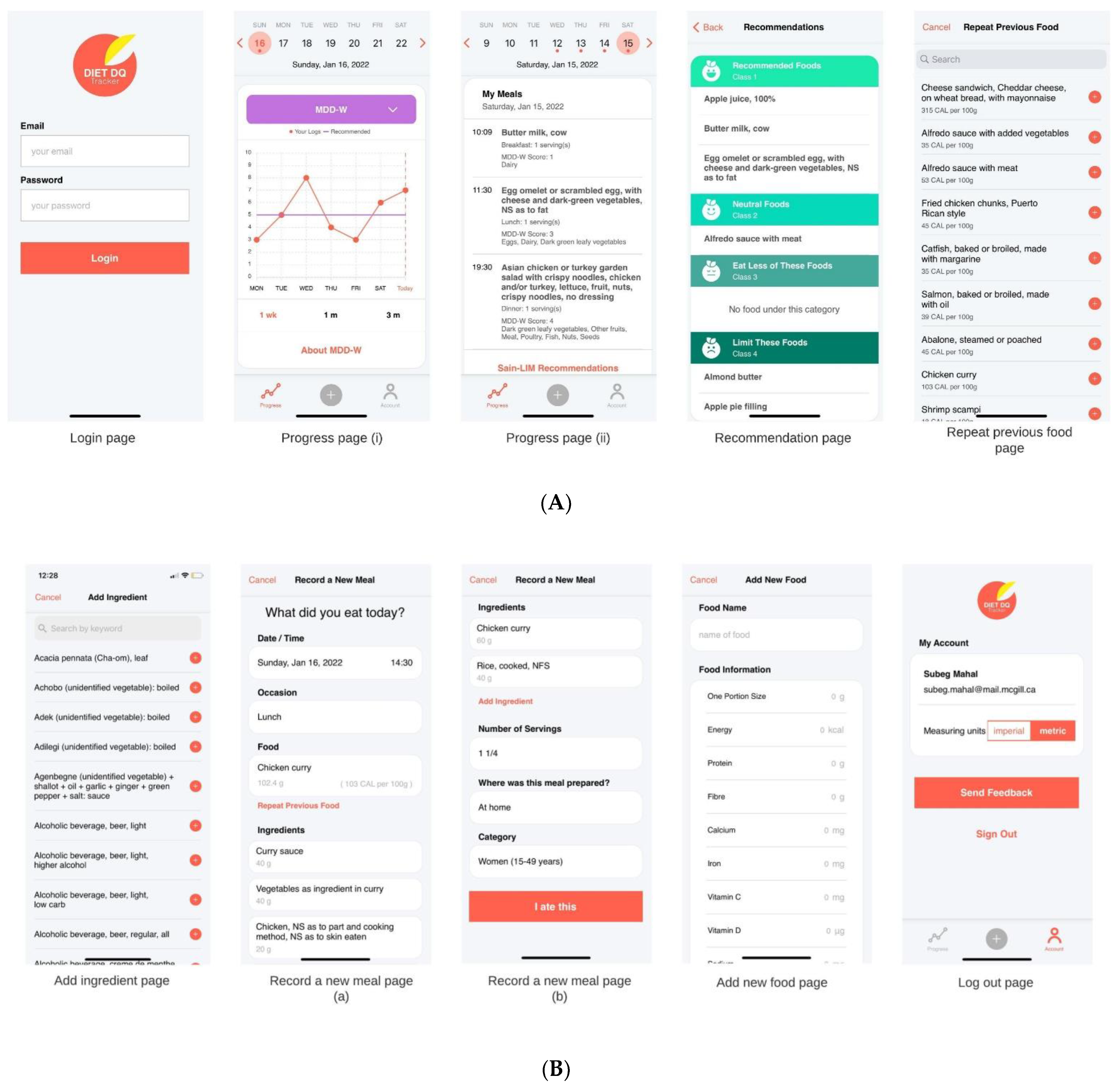
3.1. Features of ‘Diet DQ Tracker’
3.1.1. Account Creation and Login
3.1.2. ‘Progress’ Page
3.1.3. ‘SAIN, LIM Recommendations’
3.1.4. ‘My Account’ Page
3.1.5. ‘Record a New Meal’ Page
3.1.6. ‘Add New Food’ Page
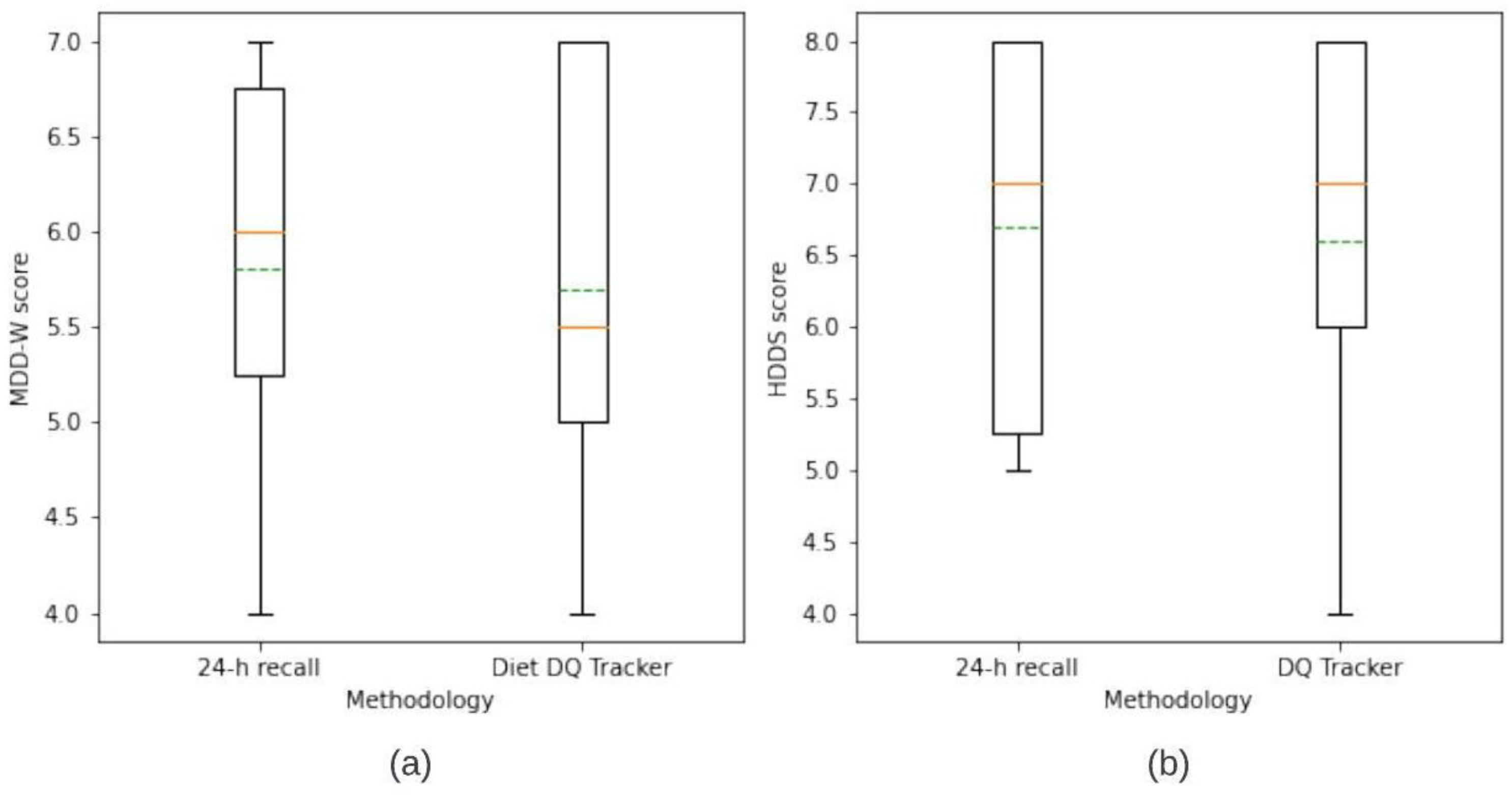
3.2. Comparison of DDS’s from ‘Diet DQ Tracker’ and 24 h Recall
3.3. Participant Feedback on ‘Diet DQ Tracker’ and 24 h Recall
4. Discussion
4.1. Principal Considerations
4.2. Strengths and Limitations
4.3. Related Work
4.4. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| User Feedback on Dietary Assessments | ||||
|---|---|---|---|---|
| Number of Respondents | 20 (10 Female; 10 Male) | |||
| 1. | General statements To begin with the survey, I’d like to read a few statements regarding the dietary survey in which you agreed to participate. I will read the statements for you; please choose one of the options below. Please select, whether you strongly agree, agree, are neutral, disagree, or strongly disagree with the following statements. | Agree/Strongly agree | Neutral | Disagree/Strongly disagree |
| 1.1 | The Diet DQ app is easy to understand. | 19 | 1 | |
| 1.2 | The Diet DQ app is easy to use. | 19 | 1 | |
| 1.3 | The foods I usually consume were easy to find on the app. | 5 | 13 | 2 |
| 1.4 | Foods and beverages were recorded on the app right after consumption. | 11 | 9 | |
| 1.5 | Recording food items right after consumption affected my daily routine. | 1 | 7 | 12 |
| 1.6 | During the interview administered recall session, remembering the food items consumed the previous day was difficult. | 5 | 6 | 9 |
| 1.7 | Meals logged the day before were checked prior to or during the interviewer-administered recall session. | 13 | 4 | 3 |
| 1.8 | Recording food items in the ‘Search-as-you-type’ textbox was convenient. | 10 | 6 | 4 |
| 1.9 | Estimating the number of servings of a standard portion size was easy. | 6 | 5 | 9 |
| 1.10 | Custom recipes were frequently recorded on the Diet DQ app. | 8 | 7 | 5 |
| 1.11 | Recording custom recipes on the app was difficult. | 4 | 12 | 4 |
| 1.12 | The ‘repeat previous food’ feature was often used. | 2 | 7 | 11 |
| 1.13 | Graphic visualizations of the diet diversity scores were frequently accessed. | 19 | 1 | |
| 1.14 | The graphic visualizations prompted the consumption of diverse food groups for the purpose of achieving a higher score. | 15 | 5 | |
| 1.15 | SAIN, LIM recommendations for foods consumed were frequently checked. | 15 | 4 | 1 |
| 1.16 | SAIN, LIM recommendations prompted the consumption of healthy foods. | 16 | 4 | |
| 1.17 | Overall, the Diet DQ app proved to be highly satisfactory. | 18 | 2 | |
| 1. | The Preferred Methodology | ||
| 1.1 | Which is your preferred methodology for dietary assessment? | App | Interview-Administered Recall |
| 20 | |||
| Provide Yes or No answers below. Was your preferred dietary assessment methodology: | Yes/No | ||
| 1.2 | More convenient? | Yes (20) | |
| 1.3 | Easy to use? | Yes (20) | |
| 1.4 | Less time consuming? | Yes (20) | |
| 1.5 | Easy to remember? | - | |
| 1.6 | Portable? | Yes (20) | |
| 1.7 | Enjoyable to use? | Yes (20) | |
| 2. | Duration questions | Time (min) | |
| 2.1 | Approximately how long did it take to record an entire day’s food intake on the Diet DQ app? | 8.4 | |
| 2.2 | Approximately how long did it take to recall and inform the interviewer about the previous day’s food consumption? | 10.25 | |
References
- IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World: Transforming Food Systems for Affordable Healthy Diets; FAO: Rome, Italy, 2020. [Google Scholar]
- Thompson, F.E.; Subar, A.F.; Loria, C.M.; Reedy, J.L.; Baranowski, T. Need for technological innovation in dietary assessment. J. Am. Diet. Assoc. 2010, 110, 48. [Google Scholar] [CrossRef]
- Webb, P.; Kennedy, E. Impacts of agriculture on nutrition: Nature of the evidence and research gaps. Food Nutr. Bull. 2014, 35, 126–132. [Google Scholar] [CrossRef]
- Verger, E.O.; Ballard, T.J.; Dop, M.C.; Martin-Prevel, Y. Systematic review of use and interpretation of dietary diversity indicators in nutrition-sensitive agriculture literature. Glob. Food Secur. 2019, 20, 156–169. [Google Scholar] [CrossRef]
- Herforth, A.; Ballard, T.J. Nutrition indicators in agriculture projects: Current measurement, priorities, and gaps. Glob. Food Secur. 2016, 10, 1–10. [Google Scholar] [CrossRef]
- Ruel, M.T.; Harris, J.; Cunningham, K. Diet quality in developing countries. In Diet Quality; Springer: Berlin/Heidelberg, Germany, 2013; pp. 239–261. [Google Scholar]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V. Addressing current criticism regarding the value of self-report dietary data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012; Volume 40. [Google Scholar]
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The National Cancer Institute’s dietary assessment primer: A resource for diet research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef]
- Boeing, H. Nutritional epidemiology: New perspectives for understanding the diet-disease relationship? Eur. J. Clin. Nutr. 2013, 67, 424–429. [Google Scholar] [CrossRef]
- Ferreira, M.; Percy, L.; Holanda, M.; Araujo, A.; Torres, B.; Ito, M.K. R24móvel—24 Hour dietary recall mobile application. In Proceedings of the 2015 10th Iberian Conference on Information Systems and Technologies (CISTI), Aveiro, Portuga, 17–20 June 2015; pp. 1–5. [Google Scholar]
- Guinn, C.H.; Baxter, S.D.; Hardin, J.W.; Royer, J.A.; Smith, A.F. Intrusions in children’s dietary recalls: The roles of BMI, sex, race, interview protocol, and social desirability. Obesity 2008, 16, 2169–2174. [Google Scholar] [CrossRef]
- Baxter, S.D.; Thompson, W.O.; Davis, H.C.; Johnson, M.H. Impact of gender, ethnicity, meal component, and time interval between eating and reporting on accuracy of fourth-graders’ self-reports of school lunch. J. Am. Diet. Assoc. 1997, 97, 1293–1298. [Google Scholar] [CrossRef]
- Dulal, B.; Mundy, G.; Sawal, R.; Rana, P.P.; Cunningham, K. Homestead food production and maternal and child dietary diversity in Nepal: Variations in association by season and agroecological zone. Food Nutr. Bull. 2017, 38, 338–353. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Pearson, M.; Renker, S.; Myerburg, S.; Farino, C. A novel system for collecting longitudinal self-reported dietary consumption information: The internet data logger (iDL). J. Expo. Sci. Environ. Epidemiol. 2006, 16, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Krumpal, I. Determinants of social desirability bias in sensitive surveys: A literature review. Qual. Quant. 2013, 47, 2025–2047. [Google Scholar] [CrossRef]
- Lamanna, C.; Hachhethu, K.; Chesterman, S.; Singhal, G.; Mwongela, B.; Ng’endo, M.; Passeri, S.; Farhikhtah, A.; Kadiyala, S.; Bauer, J.-M. Strengths and limitations of computer assisted telephone interviews (CATI) for nutrition data collection in rural Kenya. PLoS ONE 2019, 14, e0210050. [Google Scholar] [CrossRef]
- Cerri, J.; Testa, F.; Rizzi, F.; Frey, M. Factorial surveys reveal social desirability bias over self-reported organic fruit consumption. Br. Food J. 2019, 121, 897–909. [Google Scholar] [CrossRef]
- Getacher, L.; Egata, G.; Alemayehu, T.; Bante, A.; Molla, A. Minimum dietary diversity and associated factors among lactating mothers in Ataye district, North Shoa zone, Central Ethiopia: A community-based cross-sectional study. J. Nutr. Metab. 2020, 2020, 1823697. [Google Scholar] [CrossRef]
- Eldridge, A.L. FITS and KNHS overview: Methodological challenges in dietary intake data collection among infants, toddlers, and children in selected countries. In Nurturing a Healthy Generation of Children: Research Gaps and Opportunities; Karger Publishers: Basel, Switzerland, 2019; Volume 91, pp. 69–78. [Google Scholar]
- Cade, J.E. Measuring diet in the 21st century: Use of new technologies. Proc. Nutr. Soc. 2017, 76, 276–282. [Google Scholar] [CrossRef]
- Ambrosini, G.L.; Hurworth, M.; Giglia, R.; Trapp, G.; Strauss, P. Feasibility of a commercial smartphone application for dietary assessment in epidemiological research and comparison with 24-h dietary recalls. Nutr. J. 2018, 17, 5. [Google Scholar] [CrossRef]
- Ashman, A.M.; Collins, C.E.; Brown, L.J.; Rae, K.M.; Rollo, M.E. Validation of a smartphone image-based dietary assessment method for pregnant women. Nutrients 2017, 9, 73. [Google Scholar] [CrossRef]
- Boushey, C.J.; Spoden, M.; Delp, E.J.; Zhu, F.; Bosch, M.; Ahmad, Z.; Shvetsov, Y.B.; DeLany, J.P.; Kerr, D.A. Reported energy intake accuracy compared to doubly labeled water and usability of the mobile food record among community dwelling adults. Nutrients 2017, 9, 312. [Google Scholar] [CrossRef]
- Bucher Della Torre, S.; Carrard, I.; Farina, E.; Danuser, B.; Kruseman, M. Development and evaluation of e-CA, an electronic mobile-based food record. Nutrients 2017, 9, 76. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Burley, V.; Nykjaer, C.; Cade, J. ‘My Meal Mate’(MMM): Validation of the diet measures captured on a smartphone application to facilitate weight loss. Br. J. Nutr. 2013, 109, 539–546. [Google Scholar] [CrossRef]
- Chae, J.; Woo, I.; Kim, S.; Maciejewski, R.; Zhu, F.; Delp, E.J.; Boushey, C.J.; Ebert, D.S. Volume estimation using food specific shape templates in mobile image-based dietary assessment. In Proceedings of the Computational Imaging IX, San Francisco, CA, USA, 24–25 January 2011; p. 78730K. [Google Scholar]
- Higgins, J.; LaSalle, A.; Zhaoxing, P.; Kasten, M.; Bing, K.; Ridzon, S.; Witten, T. Validation of photographic food records in children: Are pictures really worth a thousand words? Eur. J. Clin. Nutr. 2009, 63, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Tan, J. DietCam: Automatic dietary assessment with mobile camera phones. Pervasive Mob. Comput. 2012, 8, 147–163. [Google Scholar] [CrossRef]
- Pendergast, F.J.; Ridgers, N.D.; Worsley, A.; McNaughton, S.A. Evaluation of a smartphone food diary application using objectively measured energy expenditure. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 30. [Google Scholar] [CrossRef] [PubMed]
- Illner, A.; Freisling, H.; Boeing, H.; Huybrechts, I.; Crispim, S.; Slimani, N. Review and evaluation of innovative technologies for measuring diet in nutritional epidemiology. Int. J. Epidemiol. 2012, 41, 1187–1203. [Google Scholar] [CrossRef]
- Wellard-Cole, L.; Chen, J.; Davies, A.; Wong, A.; Huynh, S.; Rangan, A.; Allman-Farinelli, M. Relative validity of the Eat and Track (EaT) smartphone app for collection of dietary intake data in 18-to-30-year olds. Nutrients 2019, 11, 621. [Google Scholar] [CrossRef]
- Rangan, A.M.; O’Connor, S.; Giannelli, V.; Yap, M.L.; Tang, L.M.; Roy, R.; Louie, J.C.Y.; Hebden, L.; Kay, J.; Allman-Farinelli, M. Electronic Dietary Intake Assessment (e-DIA): Comparison of a mobile phone digital entry app for dietary data collection with 24-hour dietary recalls. JMIR Mhealth Uhealth 2015, 3, e4613. [Google Scholar] [CrossRef]
- Haas, J.D.; Luna, S.V.; Lung’aho, M.G.; Wenger, M.J.; Murray-Kolb, L.E.; Beebe, S.; Gahutu, J.-B.; Egli, I.M. Consuming iron biofortified beans increases iron status in Rwandan women after 128 days in a randomized controlled feeding trial. J. Nutr. 2016, 146, 1586–1592. [Google Scholar] [CrossRef]
- Ritchie, H.; Roser, M. Micronutrient Deficiency. Our World Data. 2017. Available online: https://ourworldindata.org/micronutrient-deficiency (accessed on 26 May 2023).
- Ruel, M.T.; Alderman, H. Nutrition-sensitive interventions and programmes: How can they help to accelerate progress in improving maternal and child nutrition? Lancet 2013, 382, 536–551. [Google Scholar] [CrossRef]
- Kennedy, G.; Ballard, T.; Dop, M.C. Guidelines for Measuring Household and Individual Dietary Diversity; Food and Agriculture Organization of the United Nations: Rome, Italy, 2011. [Google Scholar]
- Torheim, L.E.; Ferguson, E.L.; Penrose, K.; Arimond, M. Women in resource-poor settings are at risk of inadequate intakes of multiple micronutrients. J. Nutr. 2010, 140, 2051S–2058S. [Google Scholar] [CrossRef]
- FAO. Minimum Dietary Diversity for Women: A Guide to Measurement; FAO: Rome, Italy, 2016. [Google Scholar]
- Cusick, S.E.; Georgieff, M.K. The role of nutrition in brain development: The golden opportunity of the “first 1000 days”. J. Pediatr. 2016, 175, 16–21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1: Definitions: Conclusions of a Consensus Meeting Held 6–8 November 2007 in Washington DC, USA; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Hatløy, A.; Hallund, J.; Diarra, M.M.; Oshaug, A. Food variety, socioeconomic status and nutritional status in urban and rural areas in Koutiala (Mali). Public Health Nutr. 2000, 3, 57–65. [Google Scholar] [CrossRef]
- Swindale, A.; Bilinsky, P. Household Dietary Diversity Score (HDDS) for Measurement of Household Food Access: Indicator Guide; Food and Nutrition Technical Assistance Project, Academy for Educational Development: Washington, DC, USA, 2006. [Google Scholar]
- Wirt, A.; Collins, C.E. Diet quality–what is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Burrows, T.; Collins, C.E. Systematic review of diet quality indices and their associations with health-related outcomes in children and adolescents. J. Hum. Nutr. Diet. 2014, 27, 577–598. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Henderson, S.A.; SHORE, A.; Fischler, C.; Preziosi, P.; Hercberg, S. Diet quality and dietary diversity in France: Implications for the French paradox. J. Am. Diet. Assoc. 1996, 96, 663–669. [Google Scholar] [CrossRef]
- Patterson, R.E.; Haines, P.S.; Popkin, B.M. Diet quality index: Capturing a multidimensional behavior. J. Am. Diet. Assoc. 1994, 94, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Key, T. Diet and the risk of cancer. BMJ 2007, 335, 897. [Google Scholar] [CrossRef]
- Jacobs Jr, D.R.; Steffen, L.M. Nutrients, foods, and dietary patterns as exposures in research: A framework for food synergy. Am. J. Clin. Nutr. 2003, 78, 508S–513S. [Google Scholar] [CrossRef]
- Darmon, N.; Darmon, M.; Maillot, M.; Drewnowski, A. A nutrient density standard for vegetables and fruits: Nutrients per calorie and nutrients per unit cost. J. Am. Diet. Assoc. 2005, 105, 1881–1887. [Google Scholar] [CrossRef]
- Maillot, M.; Darmon, N.; Darmon, M.; Lafay, L.; Drewnowski, A. Nutrient-dense food groups have high energy costs: An econometric approach to nutrient profiling. J. Nutr. 2007, 137, 1815–1820. [Google Scholar] [CrossRef]
- Masset, G.; Scarborough, P.; Rayner, M.; Mishra, G.; Brunner, E.J. Can nutrient profiling help to identify foods which diet variety should be encouraged? Results from the Whitehall II cohort. Br. J. Nutr. 2015, 113, 1800–1809. [Google Scholar]
- Darmon, N.; Vieux, F.; Maillot, M.; Volatier, J.-L.; Martin, A. Nutrient profiles discriminate between foods according to their contribution to nutritionally adequate diets: A validation study using linear programming and the SAIN, LIM system. Am. J. Clin. Nutr. 2009, 89, 1227–1236. [Google Scholar] [CrossRef]
- Amato, G.; Gennaro, C.; Rabitti, F.; Savino, P. Milos: A multimedia content management system for digital library applications. In Research and Advanced Technology for Digital Libraries: 8th European Conference, ECDL 2004, Bath, UK, September 12–17, 2004. Proceedings 8; Springer: Berlin/Heidelberg, Germany, 2004; pp. 14–25. [Google Scholar]
- Touvier, M.; Méjean, C.; Kesse-Guyot, E.; Pollet, C.; Malon, A.; Castetbon, K.; Hercberg, S. Comparison between web-based and paper versions of a self-administered anthropometric questionnaire. Eur. J. Epidemiol. 2010, 25, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.L.; Slattery, M.L.; Murtaugh, M.A.; Edwards, R.L.; Bryner, J.; Pearson, M.; Rogers, A.; Edwards, A.M.; Tom-Orme, L. Development and use of touch-screen audio computer-assisted self-interviewing in a study of American Indians. Am. J. Epidemiol. 2007, 165, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Klovning, A.; Sandvik, H.; Hunskaar, S. Web-based survey attracted age-biased sample with more severe illness than paper-based survey. J. Clin. Epidemiol. 2009, 62, 1068–1074. [Google Scholar] [CrossRef]
- Sharp, D.B.; Allman-Farinelli, M. Feasibility and validity of mobile phones to assess dietary intake. Nutrition 2014, 30, 1257–1266. [Google Scholar] [CrossRef]
- Ahn, J.S.; Kim, D.W.; Kim, J.; Park, H.; Lee, J.E. Development of a smartphone application for dietary self-monitoring. Front. Nutr. 2019, 6, 149. [Google Scholar] [CrossRef] [PubMed]








| Components of ‘Diet DQ Tracker’ | Description of Functionalities | |
|---|---|---|
| 1. | ‘Progress’ page | To view the progress of the user by selecting a date To view the graphical representation of diet diversity scores by selecting ‘MDD-W’, ‘IYCF-MDD’, or ‘HDDS’ To view the visual representation over 1 week, 1 month, or 3 months by selecting ‘1 wk’, ‘1 m’, or ‘3 m’ To view the background information of indicators by clicking on ‘About MDD-W’, ‘About IYCF-MDD’, or ‘About HDDS’ To view the meals consumed on the selected date by scrolling down to ‘My meals’ To view the SAIN, LIM recommendations of foods consumed over the past week by selecting ‘SAIN-LIM Recommendations’ |
| 2. | ‘Record a new meal’ page | To specify the date and time of meal consumption by clicking on pre-set date/time To specify the occasion of meal consumption (breakfast, lunch, dinner, and snack) by clicking on ‘Select occasion’ To specify the food name by using the search-as-you-type box after clicking on ‘Food item’ To specify the food name from food items frequently consumed by the user by clicking on ‘Repeat previous food’ To add a new food to the database by clicking on ‘Add new food’ at the bottom of ‘Add Food’ page To add ingredients to the selected food item by clicking on ‘Add ingredient’ To specify the number of servings of the food item by clicking on ‘Select number of servings’ To specify the place of meal preparation (at home, at a restaurant, other) by clicking on ‘Select meal prepared at’ To specify the category of user (children, women, or household) who consumed the meal by clicking on ‘Select your category’ To upload the data by clicking on ‘I ate this’ |
| 3. | ‘My account’ page | To change the units of food portion size on the ‘Record a new meal’ page from imperial to metric by clicking on ‘Measuring units’ To send the feedback on any issue/problem/or suggestion to the research team by clicking on ‘Send feedback’ To sign out of the application by clicking on ‘Sign out’ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahal, S.S.; Kucha, C.; Kwofie, E.M.; Ngadi, M. Design and Development of ‘Diet DQ Tracker’: A Smartphone Application for Augmenting Dietary Assessment. Nutrients 2023, 15, 2901. https://doi.org/10.3390/nu15132901
Mahal SS, Kucha C, Kwofie EM, Ngadi M. Design and Development of ‘Diet DQ Tracker’: A Smartphone Application for Augmenting Dietary Assessment. Nutrients. 2023; 15(13):2901. https://doi.org/10.3390/nu15132901
Chicago/Turabian StyleMahal, Subeg Singh, Christopher Kucha, Ebenezer M. Kwofie, and Michael Ngadi. 2023. "Design and Development of ‘Diet DQ Tracker’: A Smartphone Application for Augmenting Dietary Assessment" Nutrients 15, no. 13: 2901. https://doi.org/10.3390/nu15132901
APA StyleMahal, S. S., Kucha, C., Kwofie, E. M., & Ngadi, M. (2023). Design and Development of ‘Diet DQ Tracker’: A Smartphone Application for Augmenting Dietary Assessment. Nutrients, 15(13), 2901. https://doi.org/10.3390/nu15132901