
Effect of Vitamin D Supplementation on Fatigue in Multiple Sclerosis: A Systematic Review and Meta-Analysis

 , ,
, ,  , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction
2.4. Classification of the Disease, Baseline Level of 25(OH) D, and Outcome
2.5. Risk of Bias Assessment
2.6. Data Synthesis
3. Results
3.1. Literature Search
3.2. Study Characteristics
3.3. Interventions
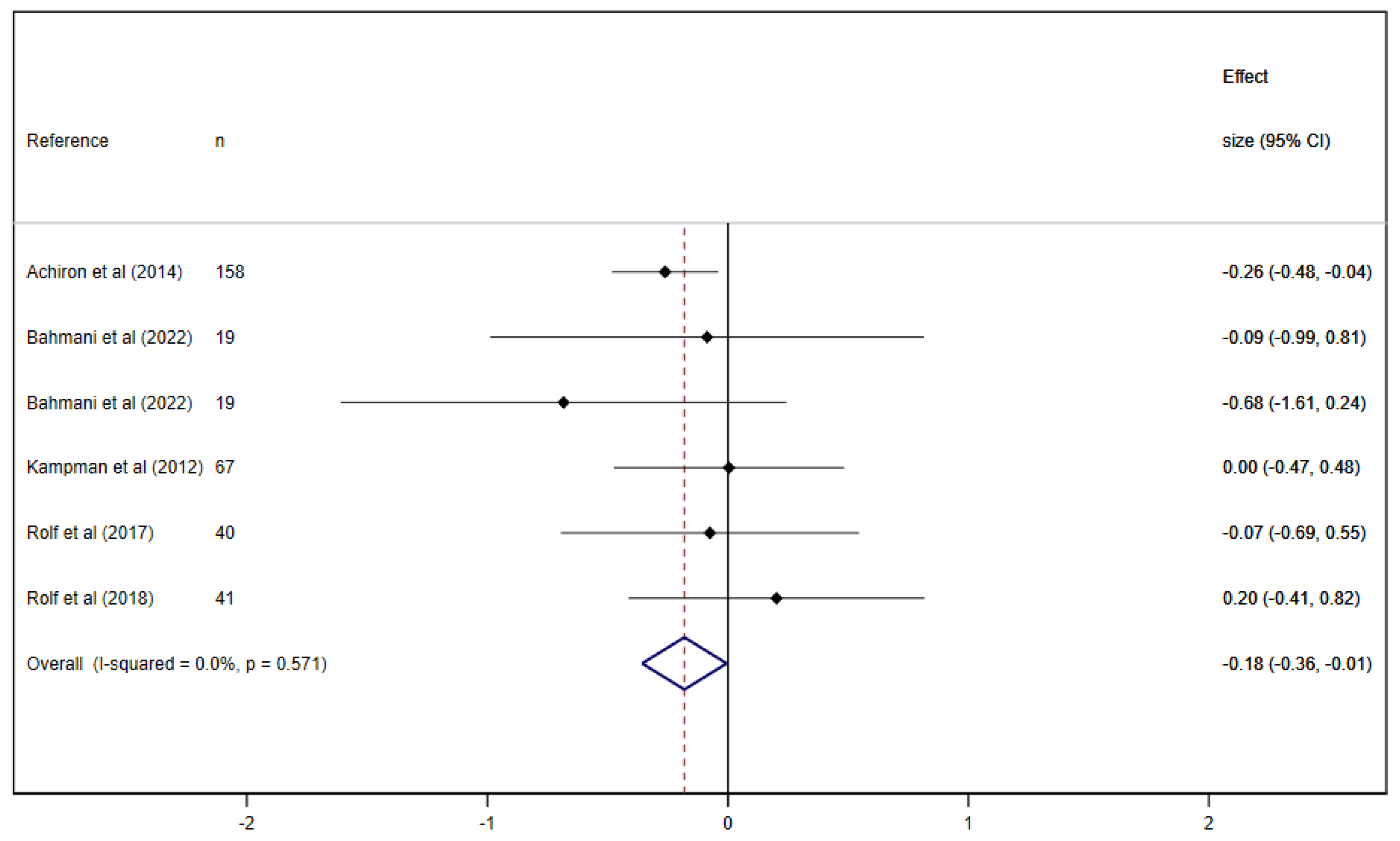
3.4. Meta-Analysis
3.5. Sensitivity Analyses, Meta-Regression Models, and Publication Bias
3.6. Risk of Bias Assessment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ayache, S.S.; Chalah, M.A. Fatigue in multiple sclerosis—Insights into evaluation and management. Neurophysiol. Clin. 2017, 47, 139–171. [Google Scholar] [CrossRef] [PubMed]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Torres-Costoso, A.; Martínez-Vizcaíno, V.; Reina-Gutiérrez, S.; Álvarez-Bueno, C.; Guzmán-Pavón, M.J.; Pozuelo-Carrascosa, D.P.; Fernández-Rodríguez, R.; Sanchez-López, M.; Cavero-Redondo, I. Effect of Exercise on Fatigue in Multiple Sclerosis: A Network Meta-analysis Comparing Different Types of Exercise. Arch. Phys. Med. Rehabil. 2022, 103, 970–987.e18. [Google Scholar] [CrossRef] [PubMed]
- Rooney, S.; McFadyen, A.; Wood, L.; Moffat, F.; Paul, L. Minimally important difference of the fatigue severity scale and modified fatigue impact scale in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 35, 158–163. [Google Scholar] [CrossRef]
- Langeskov-Christensen, M.; Bisson, E.J.; Finlayson, M.L.; Dalgas, U. Potential pathophysiological pathways that can explain the positive effects of exercise on fatigue in multiple sclerosis: A scoping review. J. Neurol. Sci. 2017, 373, 307–320. [Google Scholar] [CrossRef]
- Englund, S.; Piehl, F.; Kierkegaard, M. High-intensity resistance training in people with multiple sclerosis experiencing fatigue: A randomised controlled trial. Mult. Scler. Relat. Disord. 2022, 68, 104106. [Google Scholar] [CrossRef]
- Tarasiuk, J.; Kapica-Topczewska, K.; Czarnowska, A.; Chorąży, M.; Kochanowicz, J.; Kułakowska, A. Co-occurrence of Fatigue and Depression in People with Multiple Sclerosis: A Mini-Review. Front. Neurol. 2022, 12, 817256. [Google Scholar] [CrossRef]
- Rooney, S.; Wood, L.; Moffat, F.; Paul, L. Prevalence of fatigue and its association with clinical features in progressive and non-progressive forms of Multiple Sclerosis. Mult. Scler. Relat. Disord. 2019, 28, 276–282. [Google Scholar] [CrossRef]
- Nourbakhsh, B.; Revirajan, N.; Morris, B.; Cordano, C.; Creasman, J.; Manguinao, M.; Krysko, K.; Rutatangwa, A.; Auvray, C.; Aljarallah, S.; et al. Safety and efficacy of amantadine, modafinil, and methylphenidate for fatigue in multiple sclerosis: A randomised, placebo-controlled, crossover, double-blind trial. Lancet Neurol. 2021, 20, 38–48. [Google Scholar] [CrossRef]
- Yuan, X.; Guo, L.; Jiang, C.; Yang, X.; Huang, J. The Effect of Different Administration Time and Dosage of Vitamin D Supplementation in Patients with Multiple Sclerosis: A Meta-Analysis of Randomized Controlled Trials. Neuroimmunomodulation 2021, 28, 118–128. [Google Scholar] [CrossRef]
- Boltjes, R.; Knippenberg, S.; Gerlach, O.; Hupperts, R.; Damoiseaux, J. Vitamin D supplementation in multiple sclerosis: An expert opinion based on the review of current evidence. Expert Rev. Neurother. 2021, 21, 715–725. [Google Scholar] [CrossRef]
- Zheng, C.; He, L.; Liu, L.; Zhu, J.; Jin, T. The efficacy of vitamin D in multiple sclerosis: A meta-analysis. Mult. Scler. Relat. Disord. 2018, 23, 56–61. [Google Scholar] [CrossRef]
- Mokry, L.E.; Ross, S.; Ahmad, O.S.; Forgetta, V.; Smith, G.D.; Leong, A.; Greenwood, C.M.T.; Thanassoulis, G.; Richards, J.B. Vitamin D and Risk of Multiple Sclerosis: A Mendelian Randomization Study. PLoS Med. 2015, 12, e1001866. [Google Scholar] [CrossRef]
- Ghajarzadeh, M.; Hanaei, S.; Sahraian, M.A.; Mohammadifar, M.; Ramagopalan, S.V. Effect of Vitamin D Supplements on Relapse Rate and Expanded Disability Status Scale (EDSS) in Multiple Sclerosis (MS): A Systematic Review and Meta-Analysis. Int. J. Prev. Med. 2021, 12, 42. [Google Scholar] [CrossRef]
- McLaughlin, L.; Clarke, L.; Khalilidehkordi, E.; Butzkueven, H.; Taylor, B.; Broadley, S.A. Vitamin D for the treatment of multiple sclerosis: A meta-analysis. J. Neurol. 2018, 265, 2893–2905. [Google Scholar] [CrossRef]
- Głąbska, D.; Kołota, A.; Lachowicz, K.; Skolmowska, D.; Stachoń, M.; Guzek, D. Vitamin D Supplementation and Mental Health in Multiple Sclerosis Patients: A Systematic Review. Nutrients 2021, 13, 4207. [Google Scholar] [CrossRef]
- Jagannath, V.A.; Filippini, G.; Di Pietrantonj, C.; Asokan, G.V.; Robak, E.W.; Whamond, L.; Robinson, S.A. Vitamin D for the management of multiple sclerosis. Cochrane Database Syst. Rev. 2018, 9, CD008422. [Google Scholar] [CrossRef]
- Brum, D.G.; Comini-Frota, E.R.; Vasconcelos, C.C.F.; Dias-Tosta, E. Supplementation and therapeutic use of vitamin D in patients with multiple sclerosis: Consensus of the Scientific Department of Neuroimmunology of the Brazilian Academy of Neurology. Arq. Neuropsiquiatr. 2014, 72, 152–156, (In English, In Portuguese). [Google Scholar] [CrossRef]
- Simpson-Yap, S.; Morahan, J.; Campbell, H.; Luker, T.; Mckay, F.; Chitranjan, A.; Zarghami, A.; Bruce Taylor, B.; Marck, C.; Black, L.; et al. Adapting Your Lifestyle: A Guide for People with MS. MS Research Australia. Available online: https://www.msaustralia.org.au/wp-content/uploads/2021/10/adapting-your-lifestyle-a-guide-for-people-with-ms.pdf (accessed on 31 May 2023).
- Burgos, R.; Bretón, I.; Cereda, E.; Desport, J.C.; Dziewas, R.; Genton, L.; Gomes, F.; Jésus, P.; Leischker, A.; Muscaritoli, M.; et al. ESPEN guideline clinical nutrition in neurology. Clin. Nutr. 2018, 37, 354–396. [Google Scholar] [CrossRef]
- Golan, D.; Halhal, B.; Glass-Marmor, L.; Staun-Ram, E.; Rozenberg, O.; Lavi, I.; Dishon, S.; Barak, M.; Ish-Shalom, S.; Miller, A. Vitamin D supplementation for patients with multiple sclerosis treated with interferon-beta: A randomized controlled trial assessing the effect on flu-like symptoms and immunomodulatory properties. BMC Neurol. 2013, 13, 60. [Google Scholar] [CrossRef]
- Shaygannejad, V.; Janghorbani, M.; Ashtari, F.; Dehghan, H. Effects of adjunct low-dose vitamin d on relapsing-remitting multiple sclerosis progression: Preliminary findings of a randomized placebo-controlled trial. Mult. Scler. Int. 2012, 2012, 452541. [Google Scholar] [CrossRef] [PubMed]
- Langlois, J.; Denimal, D. Clinical and Imaging Outcomes after Vitamin D Supplementation in Patients with Multiple Sclerosis: A Systematic Review. Nutrients 2023, 15, 1945. [Google Scholar] [CrossRef] [PubMed]
- Hupperts, R.; Smolders, J.; Vieth, R.; Holmøy, T.; Marhardt, K.; Schluep, M.; Killestein, J.; Barkhof, F.; Beelke, M.; Grimaldi, L.M.; et al. Randomized trial of daily high-dose vitamin D3 in patients with RRMS receiving subcutaneous interferon β-1a. Neurology 2019, 93, e1906–e1916. [Google Scholar] [CrossRef]
- Dörr, J.; Bäcker-Koduah, P.; Wernecke, K.-D.; Becker, E.; Hoffmann, F.; Faiss, J.; Brockmeier, B.; Hoffmann, O.; Anvari, K.; Wuerfel, J.; et al. High-dose vitamin D supplementation in multiple sclerosis—Results from the randomized EVIDIMS (efficacy of vitamin D supplementation in multiple sclerosis) trial. Mult. Scler. J. Exp. Transl. Clin. 2020, 6, 2055217320903474. [Google Scholar] [CrossRef] [PubMed]
- Camu, W.; Lehert, P.; Pierrot-Deseilligny, C.; Hautecoeur, P.; Besserve, A.; Deleglise, A.-S.J.; Payet, M.; Thouvenot, E.; Souberbielle, J.C. Cholecalciferol in relapsing-remitting MS: A randomized clinical trial (CHOLINE). Neurol. Neuroimmunol. Neuroinflamm. 2019, 6, e597. [Google Scholar] [CrossRef]
- Miclea, A.; Bagnoud, M.; Chan, A.; Hoepner, R. A Brief Review of the Effects of Vitamin D on Multiple Sclerosis. Front. Immunol. 2020, 11, 781. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V.; Flemyng, E. Cochrane Handbook for Systematic Reviews of Interventions. 2021. Version 6.2. Available online: www.training.cochrane.org/handbook (accessed on 1 April 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Haber, A.; LaRocca, N.G. Minimal Record of Disability for Multiple Sclerosis; National Multiple Sclerosis Society: New York, NY, USA, 1985. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompsonm, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Page, M.J.; Sterne, J.A.C.; Higgins, J.P.T.; Egger, M. Investigating and dealing with publication bias and other reporting biases in meta-analyses of health research: A review. Res. Synth. Methods 2021, 12, 248–259. [Google Scholar] [CrossRef]
- Achiron, A.; Givon, U.; Magalashvili, D.; Dolev, M.; Zaltzman, S.L.; Kalron, A.; Stern, Y.; Mazor, Z.; Ladkani, D.; Barak, Y. Effect of Alfacalcidol on multiple sclerosis-related fatigue: A randomized, double-blind placebo-controlled study. Mult. Scler. 2015, 21, 767–775. [Google Scholar] [CrossRef]
- Bahmani, E.; Hoseini, R.; Amiri, E. The effect of home-based aerobic training and vitamin D supplementation on fatigue and quality of life in patients with multiple sclerosis during COVID-19 outbreak. Sci. Sports 2022, 37, 710–719. [Google Scholar] [CrossRef]
- Kampman, M.T.; Steffensen, L.H.; Mellgren, S.I.; Jørgensen, L. Effect of vitamin D3 supplementation on relapses, disease progression, and measures of function in persons with multiple sclerosis: Exploratory outcomes from a double-blind randomised controlled trial. Mult. Scler. 2012, 18, 1144–1151. [Google Scholar] [CrossRef]
- Rolf, L.; Damoiseaux, J.; Huitinga, I.; Kimenai, D.; van den Ouweland, J.; Hupperts, R.; Smolders, J. Stress-Axis Regulation by Vitamin D3 in Multiple Sclerosis. Front. Neurol. 2018, 9, 263. [Google Scholar] [CrossRef]
- Rolf, L.; Muris, A.-H.; Bol, Y.; Damoiseaux, J.; Smolders, J.; Hupperts, R. Vitamin D3 supplementation in multiple sclerosis: Symptoms and biomarkers of depression. J. Neurol. Sci. 2017, 378, 30–35. [Google Scholar] [CrossRef]
- Sintzel, M.B.; Rametta, M.; Reder, A.T. Vitamin D and Multiple Sclerosis: A Comprehensive Review. Neurol. Ther. 2018, 7, 59–85. [Google Scholar] [CrossRef]
- Esteve, I.R.; Lozano, C.W.-B.; Sanz-Valero, J. Efectos del estado nutricional en la enfermedad de la esclerosis múltiple: Revisión sistemática [Effects of nutritional status on the multiple sclerosis disease: Systematic review]. Nutr. Hosp. 2018, 35, 211–223. (In Spanish) [Google Scholar] [CrossRef]
- Tredinnick, A.R.; Probst, Y.C. Evaluating the Effects of Dietary Interventions on Disease Progression and Symptoms of Adults with Multiple Sclerosis: An Umbrella Review. Adv. Nutr. 2020, 11, 1603–1615. [Google Scholar] [CrossRef]
- Albrechtsen, M.; Langeskov-Christensen, M.; Jørgensen, M.; Dalgas, U.; Hansen, M. Is diet associated with physical capacity and fatigue in persons with multiple sclerosis? -Results from a pilot study. Mult. Scler. Relat. Disord. 2020, 40, 101921. [Google Scholar] [CrossRef]
- Bhargava, P.; Steele, S.U.; Waubant, E.; Revirajan, N.R.; Marcus, J.; Dembele, M.; Cassard, S.D.; Hollis, B.W.; Crainiceanu, C.; Mowry, E.M. Multiple sclerosis patients have a diminished serologic response to vitamin D supplementation compared to healthy controls. Mult. Scler. 2016, 22, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, P.; Fitzgerald, K.C.; Calabresi, P.A.; Mowry, E.M. Metabolic alterations in multiple sclerosis and the impact of vitamin D supplementation. JCI Insight 2017, 2, e95302. [Google Scholar] [CrossRef] [PubMed]
- Ianniello, A.; Sottosanti, A.; Borriello, G.; Vincenti, M. Perception of Quality of Life and Fatigue in Multiple Sclerosis Patients Treated with High-Dose Vitamin D. Clin. Transl. Neurosci. 2023, 7, 12. [Google Scholar] [CrossRef]
- Amon, U.; Yaguboglu, R.; Ennis, M.; Holick, M.F.; Amon, J. Safety Data in Patients with Autoimmune Diseases during Treatment with High Doses of Vitamin D3 According to the “Coimbra Protocol”. Nutrients 2022, 14, 1575. [Google Scholar] [CrossRef] [PubMed]
- Haines, S.T.; Park, S. Vitamin D supplementation: What’s known, what to do, and what’s needed. Pharmacotherapy 2012, 32, 354–382. [Google Scholar] [CrossRef]
- Feige, J.; Moser, T.; Bieler, L.; Schwenker, K.; Hauer, L.; Sellner, J. Vitamin D Supplementation in Multiple Sclerosis: A Critical Analysis of Potentials and Threats. Nutrients 2020, 12, 783. [Google Scholar] [CrossRef]
- Ross, A.C. The 2011 report on dietary reference intakes for calcium and vitamin D. Public Health Nutr. 2011, 14, 938–939. [Google Scholar] [CrossRef]
- Berezowska, M.; Coe, S.; Dawes, H. Effectiveness of Vitamin D Supplementation in the Management of Multiple Sclerosis: A Systematic Review. Int. J. Mol. Sci. 2019, 20, 1301. [Google Scholar] [CrossRef]
- Faqeeh, M.; Alkhotani, A.; Aldoobi, R.; Sheikh, G.; Halabi, R.; Alsharif, W. The effect of Vitamin D in multiple sclerosis: An updated review. Saudi J. Health Sci. 2021, 10, 149–154. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. Horm. Res. Paediatr. 2016, 85, 83–106. [Google Scholar] [CrossRef]
- Podbielska, M.; Ariga, T.; Pokryszko-Dragan, A. Sphingolipid Players in Multiple Sclerosis: Their Influence on the Initiation and Course of the Disease. Int. J. Mol. Sci. 2022, 23, 5330. [Google Scholar] [CrossRef] [PubMed]
- Podbielska, M.; Macala, J.; Jakubiak-Augustyn, A.; Szulc, Z.M.; Fortuna, W.; Budrewicz, S.; Jaskiewicz, E.; Bilinska, M.; Hogan, E.L.; Pokryszko-Dragan, A. Ceramide is implicated in humoral peripheral and intrathecal autoimmune response in MS patients. Mult. Scler. Relat. Disord. 2023, 71, 104565. [Google Scholar] [CrossRef] [PubMed]
- Gulec, B.; Everest, E.; Gorkey, O.D.; Koc, M.; Tutuncu, M.; Saip, S.; Siva, A.; Uygunoglu, U. Comparison of multiple sclerosis patients with or without rebound activity after fingolimod cessation: Five-year clinical outcomes. Eur. J. Neurol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, T.; Bell, R.M.; Hannun, Y.A. Sphingomyelin turnover induced by vitamin D3 in HL-60 cells. Role in cell differentiation. J. Biol. Chem. 1989, 264, 19076–19080. [Google Scholar] [CrossRef]
- Balachandar, R.; Pullakhandam, R.; Kulkarni, B.; Sachdev, H.S. Relative Efficacy of Vitamin D2 and Vitamin D3 in Improving Vitamin D Status: Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3328. [Google Scholar] [CrossRef]
- Knippenberg, S.; Damoiseaux, J.; Bol, Y.; Hupperts, R.; Taylor, B.V.; Ponsonby, A.-L.; Dwyer, T.; Simpson, S.; van der Mei, I.A.F. Higher levels of reported sun exposure, and not vitamin D status, are associated with less depressive symptoms and fatigue in multiple sclerosis. Acta Neurol. Scand. 2014, 129, 123–131. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Characteristics | Population Characteristics | Intervention Characteristics | Outcome | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author (Year) | Country | n (Female) | Age (Years) Mean ± SD | BMI (kg/m2) Mean ± SD | Disease Severity (EDSS) Mean ± SD | MS Type | Disease Duration (Years) Mean ± SD | 25(OH)D Baseline Level (ng/mL) | Duration/w | Frequency(x/Week) | Vit D Dose | Comparator | Adherence | Side Effects | Fatigue Scale |
| Achiron et al., (2014) [35] | Israel | 158 (118) | 41.1 ± 9.2 | NR | 2.9 ± 2.6 | RR: 91.7% | 6.2 ± 5.5 | NR | 6 months | 7 | 1 mcg | Placebo | IG: 90% | IG: headache and dizziness | FIS; MFIS |
| CG: 91% | CG: abdominal pain | ||||||||||||||
| Bahmani et al., (2022) [36] | Irán | 38 (38) | AT + VitD: 27.70 ± 2.68 | NR | 3–5 (range) | NR | NR | AT + VitD: 25.80 ± 1.81 | 8 | 1 | 50,000 units | AT Placebo (CG) | AT + VitD: 100% | NR | MFIS |
| AT: 26.77 ± 2.27 | AT: 26.55 ± 1.50 | AT: 90% | |||||||||||||
| VitD: 25.44 ± 2.29 | VitD: 26.44 ± 1.42 | VitD: 90% | |||||||||||||
| CG: 28.11 ± 3.62 | CG: 27.20 ± 3.45 | CG: 100% | |||||||||||||
| Kampman et al., (2012) [37] | Norway | 68 (48) | IG: 40 (21–50) ** | IG: 28 (21–41) ** | IG: 2.5 (0–4.5) *** | RR: 100% | IG: 11 (1–27) ** | IG: 55.56 (46.87; 64.26) nmol/L **** | 96 | 1 | 20,000 IU + 500 mg calcium/day | Placebo + 500 mg calcium/day | IG: 100% | No adverse events | FSS |
| CG:41 (26–50) ** | CG: 26 (18–40) ** | CG: 2.0 (0–4.5) *** | CG: 10 (2–26) ** | CG: 57.33 (48.37; 66.28) nmol/L **** | CG: 91.67% | ||||||||||
| Rolf et al., (2017) [39] | Netherlands | 40 (26) | IG: 38.5 ± 7.8 | NR | IG: 2.0 (1.5–2.5) * | RR: 100% | IG: 7.5 (4.4–11.7) months * | IG: 58 (38–82) nmol/L * | 48 | 7 | 7000 IU first 4 weeks and 14,000 IU up to week 48 | Placebo | IG: 90.91% | NR | FSS |
| CG: 37.6 ± 9.6 | CG: 2.0 (1.5–2.3) * | CG: 5.7 (3.9–11.7) months * | CG: 53 (43–63) nmol/L * | CG: 92% | |||||||||||
| Rolf et al., (2018) [38] | Netherlands | 41 (41) | IG: 38.6 (28.0–45.0) * | NR | IG: 2.0 (1.4–2.0) * | RR: 100% | IG: 3.8 (2.8–11.4) * | IG: 85 (71–111) nmol/L * | 16 | 7 | 4000 IU | Placebo | IG: 92% | IG: headache and dizziness | FSS |
| CG: 35.1 (33.0–45.0) * | CG: 2.0 (1.0–2.5) * | CG: 5.4 (1.2–7.9) * | CG: 78 (68–95) nmol/L * | CG: 72.41% | CG: abdominal pain and stomach discomfort | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Muñoz, P.; Torres-Costoso, A.I.; Fernández-Rodríguez, R.; Guzmán-Pavón, M.J.; de Arenas-Arroyo, S.N.; Basco-López, J.Á.; Reina-Gutiérrez, S. Effect of Vitamin D Supplementation on Fatigue in Multiple Sclerosis: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2861. https://doi.org/10.3390/nu15132861
López-Muñoz P, Torres-Costoso AI, Fernández-Rodríguez R, Guzmán-Pavón MJ, de Arenas-Arroyo SN, Basco-López JÁ, Reina-Gutiérrez S. Effect of Vitamin D Supplementation on Fatigue in Multiple Sclerosis: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(13):2861. https://doi.org/10.3390/nu15132861
Chicago/Turabian StyleLópez-Muñoz, Purificación, Ana Isabel Torres-Costoso, Rubén Fernández-Rodríguez, María José Guzmán-Pavón, Sergio Núñez de Arenas-Arroyo, Julián Ángel Basco-López, and Sara Reina-Gutiérrez. 2023. "Effect of Vitamin D Supplementation on Fatigue in Multiple Sclerosis: A Systematic Review and Meta-Analysis" Nutrients 15, no. 13: 2861. https://doi.org/10.3390/nu15132861
APA StyleLópez-Muñoz, P., Torres-Costoso, A. I., Fernández-Rodríguez, R., Guzmán-Pavón, M. J., de Arenas-Arroyo, S. N., Basco-López, J. Á., & Reina-Gutiérrez, S. (2023). Effect of Vitamin D Supplementation on Fatigue in Multiple Sclerosis: A Systematic Review and Meta-Analysis. Nutrients, 15(13), 2861. https://doi.org/10.3390/nu15132861