
Association of Serum Vitamin D Level with Temporomandibular Disorder Incidence: A Retrospective, Multi-Center Cohort Study Using Six Hospital Databases


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
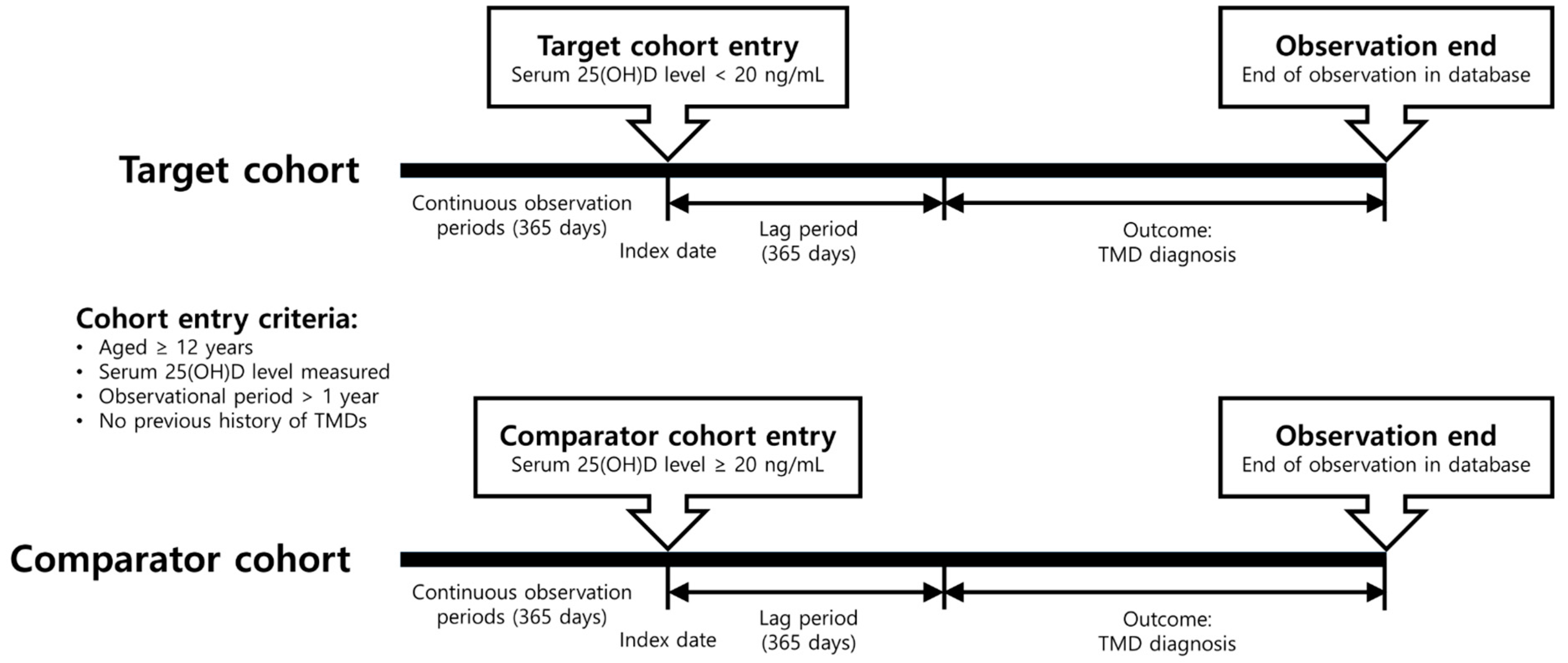
2.2. Study Design and Cohort Definition
2.3. Covariates
2.4. Statistical Analysis
2.5. Sensitivity Analysis
3. Results
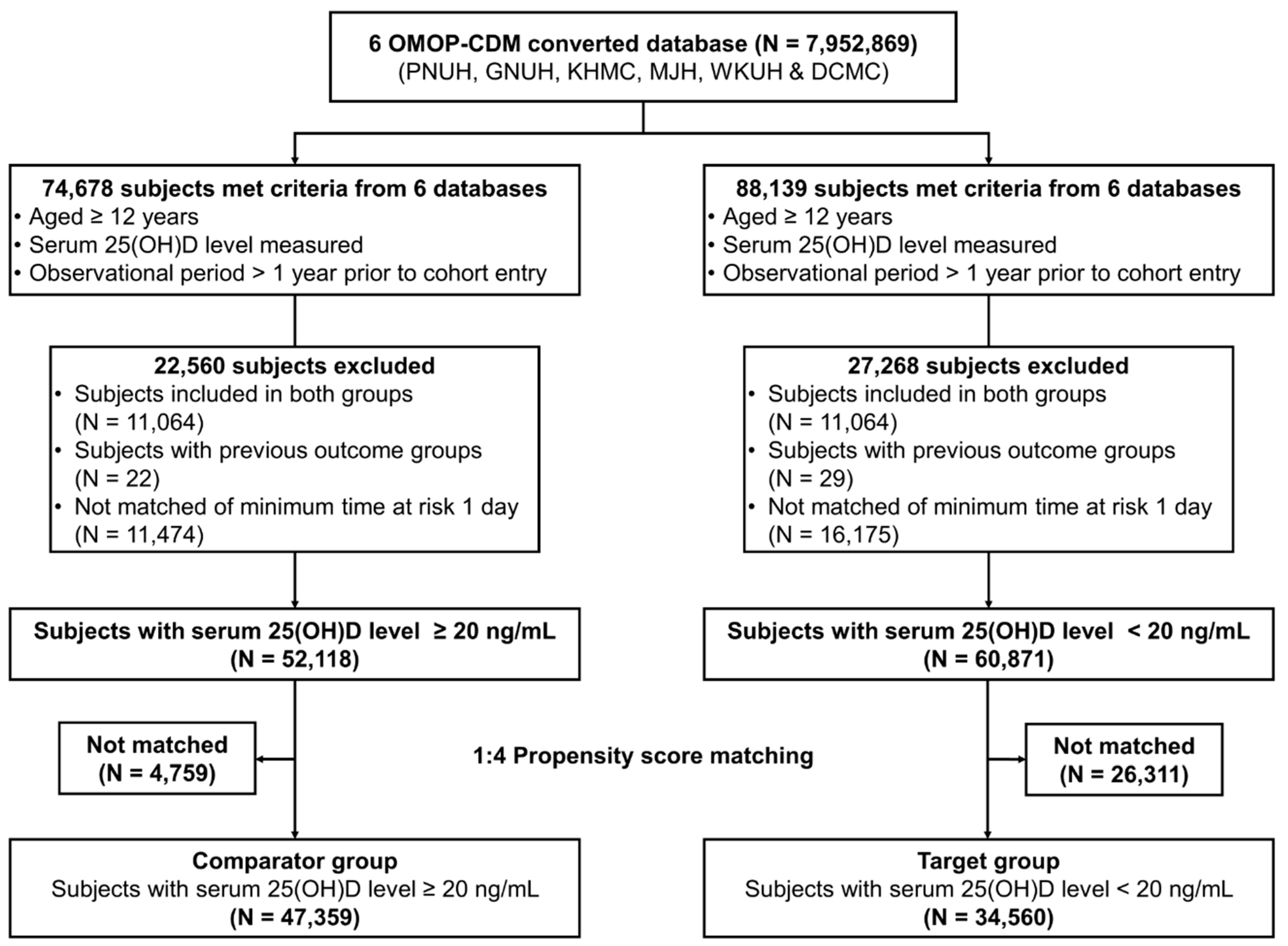
3.1. Participant Characteristics
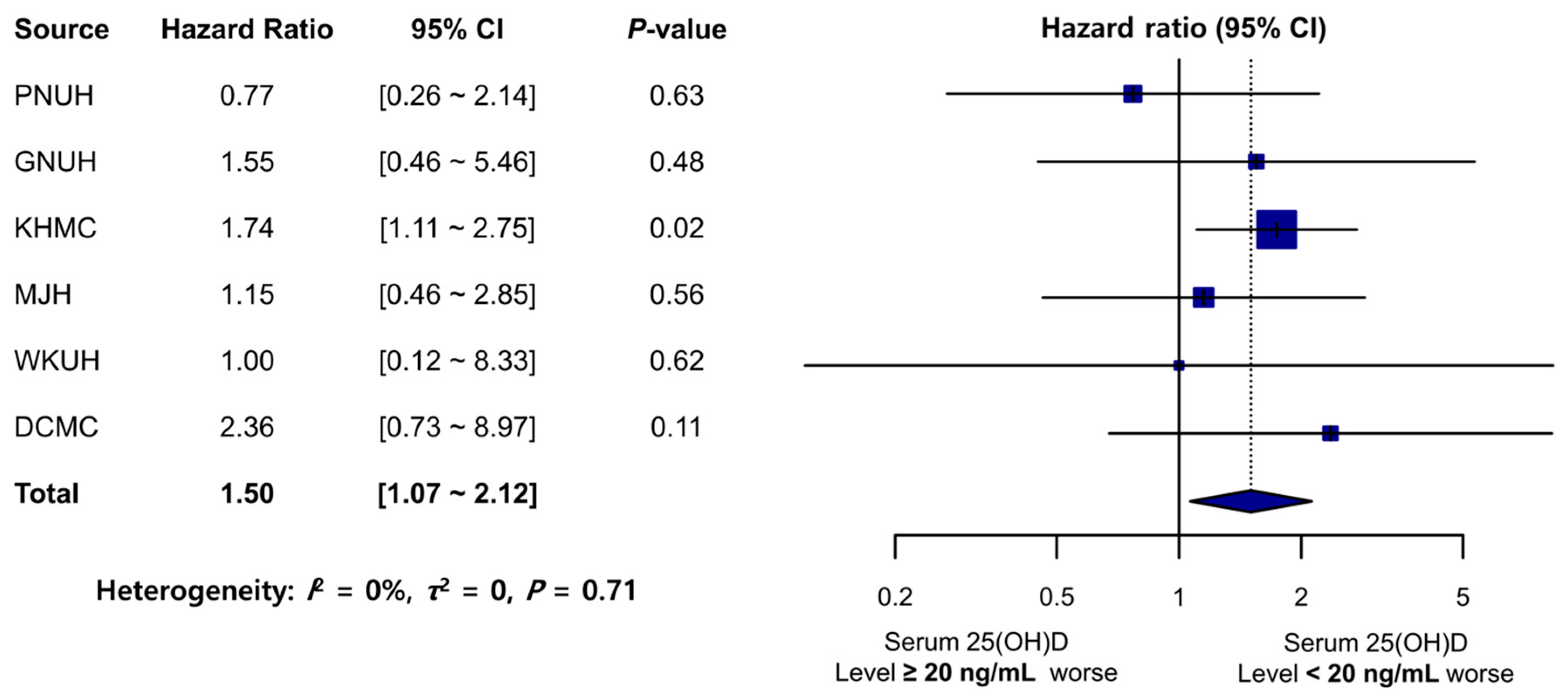
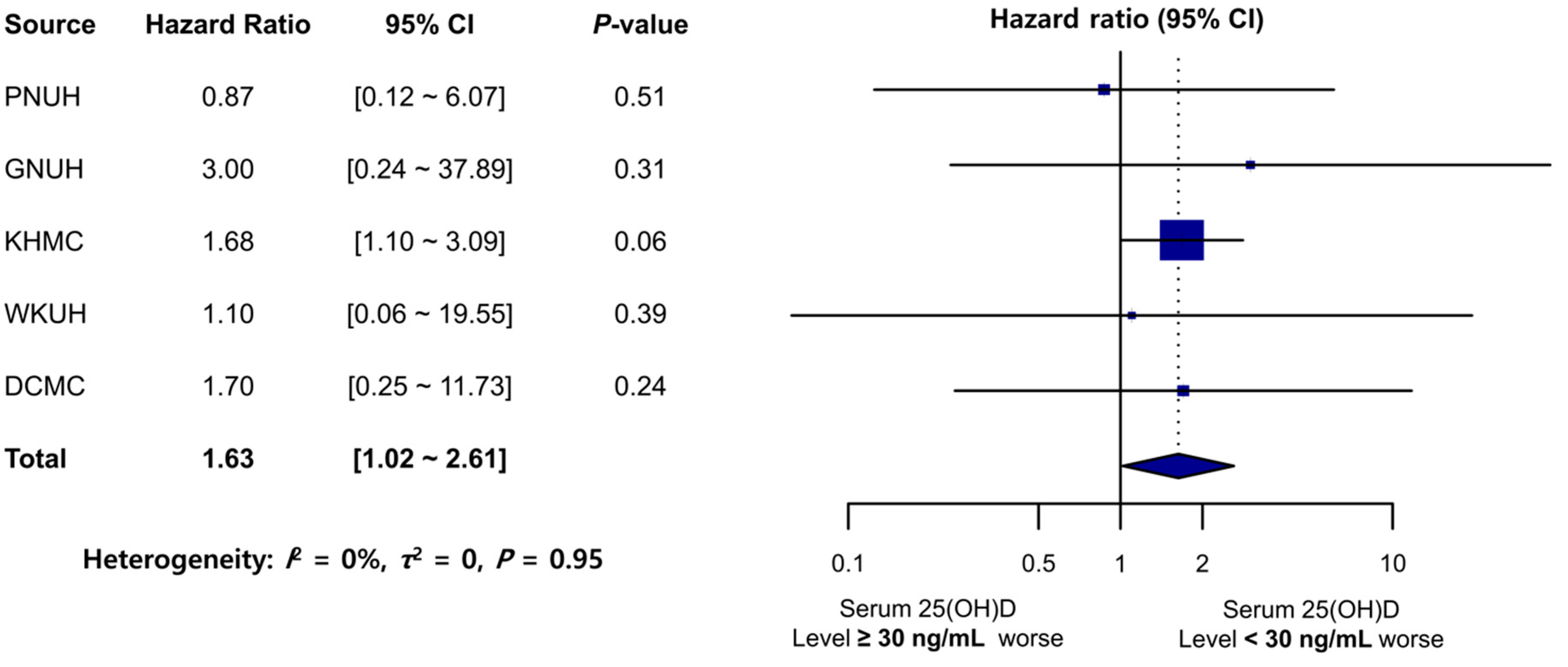
3.2. Primary Outcomes
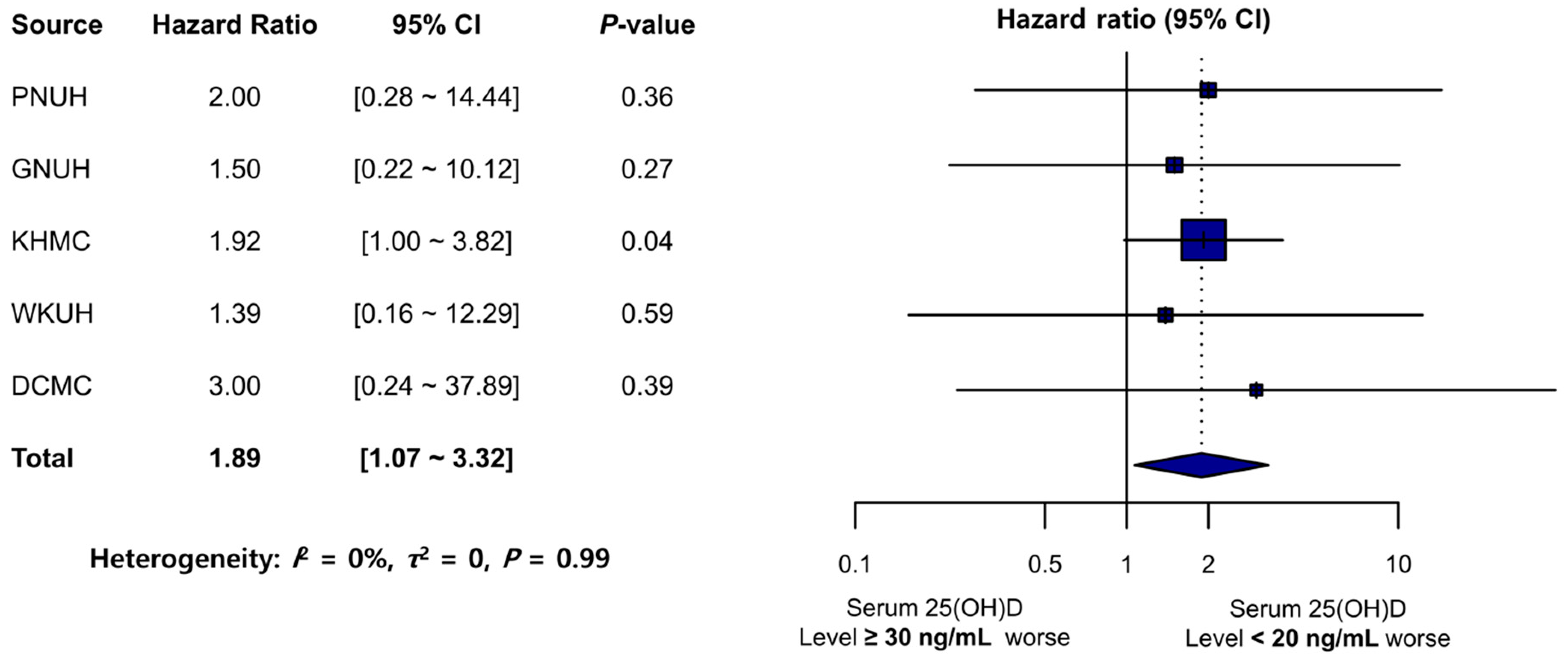
3.3. Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; Demay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The nonskeletal effects of vitamin D: An Endocrine Society scientific statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef]
- Pludowski, P.; Holick, M.F.; Pilz, S.; Wagner, C.L.; Hollis, B.W.; Grant, W.B.; Shoenfeld, Y.; Lerchbaum, E.; Llewellyn, D.J.; Kienreich, K.; et al. Vitamin D effects on musculoskeletal health, immunity, autoimmunity, cardiovascular disease, cancer, fertility, pregnancy, dementia and mortality-a review of recent evidence. Autoimmun. Rev. 2013, 12, 976–989. [Google Scholar] [CrossRef]
- Garland, C.F.; Mohr, S.B.; Gorham, E.D.; Grant, W.B.; Garland, F.C. Role of ultraviolet B irradiance and vitamin D in prevention of ovarian cancer. Am. J. Prev. Med. 2006, 31, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Janssen, H.C.; Samson, M.M.; Verhaar, H.J. Vitamin D deficiency, muscle function, and falls in elderly people. Am. J. Clin. Nutr. 2002, 75, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Ceglia, L.; Harris, S.S. Vitamin D and its role in skeletal muscle. Calcif. Tissue Int. 2013, 92, 151–162. [Google Scholar] [CrossRef]
- Ceglia, L. Vitamin D and skeletal muscle tissue and function. Mol. Aspects Med. 2008, 29, 407–414. [Google Scholar] [CrossRef]
- Plotnikoff, G.A.; Quigley, J.M. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin. Proc. 2003, 78, 1463–1470. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Non-musculoskeletal benefits of vitamin D. J. Steroid Biochem. Mol. Biol. 2018, 175, 60–81. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, R.; Klasser, G.D. Chapter 8. Diagnosis and management of TMDs. In Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management, 5th ed.; Quintessence: Hanover Park, IL, USA, 2013. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Groupdagger. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardini, L.; Winocur, E.; Piccotti, F.; Ahlberg, J.; Lobbezoo, F. Research diagnostic criteria for temporomandibular disorders: A systematic review of axis I epidemiologic findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 453–462. [Google Scholar] [CrossRef]
- Slade, G.D.; Fillingim, R.B.; Sanders, A.E.; Bair, E.; Greenspan, J.D.; Ohrbach, R.; Dubner, R.; Diatchenko, L.; Smith, S.B.; Knott, C.; et al. Summary of findings from the OPPERA prospective cohort study of incidence of first-onset temporomandibular disorder: Implications and future directions. J. Pain 2013, 14, T116–T124. [Google Scholar] [CrossRef]
- Kindler, S.; Samietz, S.; Houshmand, M.; Grabe, H.J.; Bernhardt, O.; Biffar, R.; Kocher, T.; Meyer, G.; Volzke, H.; Metelmann, H.R.; et al. Depressive and anxiety symptoms as risk factors for temporomandibular joint pain: A prospective cohort study in the general population. J. Pain 2012, 13, 1188–1197. [Google Scholar] [CrossRef]
- Michelotti, A.; Iodice, G. The role of orthodontics in temporomandibular disorders. J. Oral Rehabil. 2010, 37, 411–429. [Google Scholar] [CrossRef] [PubMed]
- Kalladka, M.; Young, A.; Thomas, D.; Heir, G.M.; Quek, S.Y.P.; Khan, J. The relation of temporomandibular disorders and dental occlusion: A narrative review. Quintessence Int. 2022, 53, 450–459. [Google Scholar] [CrossRef]
- Nemati, M.; Tabrizi, R.; Rasooli, F.; Ghafari, S. Is the Prevalence of Vitamin D deficiency in Patients with Temporomandibular Disorder Higher than Healthy Control Group? J. Maxillofac. Oral Surg. 2022, 21, 1205–1208. [Google Scholar] [CrossRef]
- Ferrillo, M.; Migliario, M.; Marotta, N.; Fortunato, F.; Bindi, M.; Pezzotti, F.; Ammendolia, A.; Giudice, A.; Foglio Bonda, P.L.; de Sire, A. Temporomandibular disorders and neck pain in primary headache patients: A retrospective machine learning study. Acta Odontol. Scand. 2023, 81, 151–157. [Google Scholar] [CrossRef]
- Ayouni, I.; Chebbi, R.; Hela, Z.; Dhidah, M. Comorbidity between fibromyalgia and temporomandibular disorders: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciu, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. Cranio 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Boening, K.; Wiland, P.; Shiau, Y.Y.; Paradowska-Stolarz, A. Reported concepts for the treatment modalities and pain management of temporomandibular disorders. J. Headache Pain 2015, 16, 106. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Cai, J.; Yu, Y.; Hu, S.; Wang, Y.; Wu, M. Therapeutic Agents for the Treatment of Temporomandibular Joint Disorders: Progress and Perspective. Front. Pharmacol. 2020, 11, 596099. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Lippi, L.; Giudice, A.; Calafiore, D.; Paolucci, T.; Reno, F.; Migliario, M.; Fortunato, L.; Invernizzi, M.; de Sire, A. Temporomandibular Disorders and Vitamin D Deficiency: What Is the Linkage between These Conditions? A Systematic Review. J. Clin. Med. 2022, 11, 6231. [Google Scholar] [CrossRef]
- Yildiz, S.; Tumer, M.K.; Yigit, S.; Nursal, A.F.; Rustemoglu, A.; Balel, Y. Relation of vitamin D and BsmI variant with temporomandibular diseases in the Turkish population. Br. J. Oral Maxillofac. Surg. 2021, 59, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.W.; Kang, J.H. Bone mineral density, bone microstructure, and bone turnover markers in females with temporomandibular joint osteoarthritis. Clin. Oral Investig. 2021, 25, 6435–6448. [Google Scholar] [CrossRef]
- Madani, A.; Shamsian, S.A.; Layegh, P.; Abrisham, S.M.; Ravaghi, A.; Tayarani Najjaran, N. Are certain factors involved in calcium metabolism associated with temporomandibular disorders? Cranio 2021, 39, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Demir, C.Y.; Ersoz, M.E. Biochemical changes associated with temporomandibular disorders. J. Int. Med. Res. 2019, 47, 765–771. [Google Scholar] [CrossRef]
- Yilmaz, A.D.; Yazicioglu, D.; Tuzuner Oncul, A.M.; Yilmaz, E.; Eres, G. Vitamin D receptor gene polymorphisms (Apa1 and Taq1) in temporomandibular joint internal derangement/osteoarthritis in a group of Turkish patients. Mol. Biol. Rep. 2018, 45, 1839–1848. [Google Scholar] [CrossRef]
- Staniszewski, K.; Lygre, H.; Berge, T.; Rosen, A. Serum Analysis in Patients with Temporomandibular Disorders: A Controlled Cross-Sectional Study in Norway. Pain Res. Manag. 2019, 2019, 1360725. [Google Scholar] [CrossRef]
- Hripcsak, G.; Duke, J.D.; Shah, N.H.; Reich, C.G.; Huser, V.; Schuemie, M.J.; Suchard, M.A.; Park, R.W.; Wong, I.C.; Rijnbeek, P.R.; et al. Observational Health Data Sciences and Informatics (OHDSI): Opportunities for Observational Researchers. Stud. Health Technol. Inform. 2015, 216, 574–578. [Google Scholar]
- FitzHenry, F.; Resnic, F.S.; Robbins, S.L.; Denton, J.; Nookala, L.; Meeker, D.; Ohno-Machado, L.; Matheny, M.E. Creating a Common Data Model for Comparative Effectiveness with the Observational Medical Outcomes Partnership. Appl. Clin. Inform. 2015, 6, 536–547. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine, S. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Kostenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Luo, Y.; Niu, Y.; Chen, L.; Yuan, X.; Goltzman, D.; Chen, N.; Miao, D. 1,25(OH)2D deficiency induces temporomandibular joint osteoarthritis via secretion of senescence-associated inflammatory cytokines. Bone 2013, 55, 400–409. [Google Scholar] [CrossRef]
- Slade, G.D.; Ohrbach, R.; Greenspan, J.D.; Fillingim, R.B.; Bair, E.; Sanders, A.E.; Dubner, R.; Diatchenko, L.; Meloto, C.B.; Smith, S.; et al. Painful Temporomandibular Disorder: Decade of Discovery from OPPERA Studies. J. Dent. Res. 2016, 95, 1084–1092. [Google Scholar] [CrossRef]
- Melis, M.; Di Giosia, M. The role of genetic factors in the etiology of temporomandibular disorders: A review. Cranio 2016, 34, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Uitterlinden, A.G.; Fang, Y.; Van Meurs, J.B.; Pols, H.A.; Van Leeuwen, J.P. Genetics and biology of vitamin D receptor polymorphisms. Gene 2004, 338, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Hoseinkhani, Z.; Rastegari-Pouyani, M.; Tajemiri, F.; Yari, K.; Mansouri, K. Association of Vitamin D Receptor Polymorphisms (FokI (Rs2228570), ApaI (Rs7975232), BsmI (Rs1544410), and TaqI (Rs731236)) with Gastric Cancer in a Kurdish Population from West of Iran. Rep. Biochem. Mol. Biol. 2021, 9, 435–441. [Google Scholar] [CrossRef]
- Colombini, A.; Cauci, S.; Lombardi, G.; Lanteri, P.; Croiset, S.; Brayda-Bruno, M.; Banfi, G. Relationship between vitamin D receptor gene (VDR) polymorphisms, vitamin D status, osteoarthritis and intervertebral disc degeneration. J. Steroid Biochem. Mol. Biol. 2013, 138, 24–40. [Google Scholar] [CrossRef]
- Pasco, J.A.; Henry, M.J.; Kotowicz, M.A.; Sanders, K.M.; Seeman, E.; Pasco, J.R.; Schneider, H.G.; Nicholson, G.C. Seasonal periodicity of serum vitamin D and parathyroid hormone, bone resorption, and fractures: The Geelong Osteoporosis Study. J. Bone Miner. Res. 2004, 19, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Kerr, D.C.; Zava, D.T.; Piper, W.T.; Saturn, S.R.; Frei, B.; Gombart, A.F. Associations between vitamin D levels and depressive symptoms in healthy young adult women. Psychiatry Res. 2015, 227, 46–51. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital | Study Period | Number of Subjects (N = 81,919) | Patient-Year (Mean Follow-Up Time *) | Number of Outcome Events (TMD Diagnosis) | Incidence Rate per 1000 Patient-Years | HR | 95% CI | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Serum 25(OH)D Level ≥ 20 ng/mL (N = 47,359) | Serum 25(OH)D Level < 20 ng/mL (N = 34,560) | Serum 25(OH)D Level ≥ 20 ng/mL | Serum 25(OH)D Level < 20 ng/mL | Serum 25(OH)D Level ≥ 20 ng/mL | Serum 25(OH)D Level < 20 ng/mL | Serum 25(OH)D Level ≥ 20 ng/mL | Serum 25(OH)D Level < 20 ng/mL | |||||
| PNUH | 2011–2018 | 9354 | 7054 | 23,182 (2.478) | 16,723 (2.371) | 26 | 11 | 1.12 | 0.66 | 0.77 | 0.26–2.14 | 0.63 |
| GNUH | 2009–2022 | 3152 | 2019 | 10,620 (3.369) | 6584 (3.261) | 11 | 7 | 1.04 | 1.06 | 1.55 | 0.46–5.46 | 0.48 |
| KHMC | 2008–2018 | 21,029 | 14,997 | 51,754 (2.461) | 37,380 (2.492) | 80 | 74 | 1.55 | 1.98 | 1.74 | 1.11–2.75 | 0.02 |
| MJH | 2003–2020 | 5344 | 3950 | 14,273 (2.671) | 9533 (2.413) | 17 | 11 | 1.19 | 1.15 | 1.15 | 0.46–2.85 | 0.56 |
| WKUH | 1998–2018 | 3615 | 2555 | 7755 (2.145) | 5864 (2.295) | 5 | 5 | 0.64 | 0.85 | 1.00 | 0.12–8.33 | 0.62 |
| DCMC | 2005–2018 | 4865 | 3985 | 11,841 (2.434) | 9209 (2.311) | 8 | 11 | 0.73 | 1.19 | 2.36 | 0.73–8.97 | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Im, Y.-G.; Han, M.-Y.; Baek, H.-S. Association of Serum Vitamin D Level with Temporomandibular Disorder Incidence: A Retrospective, Multi-Center Cohort Study Using Six Hospital Databases. Nutrients 2023, 15, 2860. https://doi.org/10.3390/nu15132860
Im Y-G, Han M-Y, Baek H-S. Association of Serum Vitamin D Level with Temporomandibular Disorder Incidence: A Retrospective, Multi-Center Cohort Study Using Six Hospital Databases. Nutrients. 2023; 15(13):2860. https://doi.org/10.3390/nu15132860
Chicago/Turabian StyleIm, Yeong-Gwan, Man-Yong Han, and Hey-Sung Baek. 2023. "Association of Serum Vitamin D Level with Temporomandibular Disorder Incidence: A Retrospective, Multi-Center Cohort Study Using Six Hospital Databases" Nutrients 15, no. 13: 2860. https://doi.org/10.3390/nu15132860
APA StyleIm, Y.-G., Han, M.-Y., & Baek, H.-S. (2023). Association of Serum Vitamin D Level with Temporomandibular Disorder Incidence: A Retrospective, Multi-Center Cohort Study Using Six Hospital Databases. Nutrients, 15(13), 2860. https://doi.org/10.3390/nu15132860