
Dietary Strategies in Adult Patients with Eosinophilic Esophagitis: A State-of-the-Art Review
 ,
,  and
and
Abstract
:1. Introduction
2. Methods
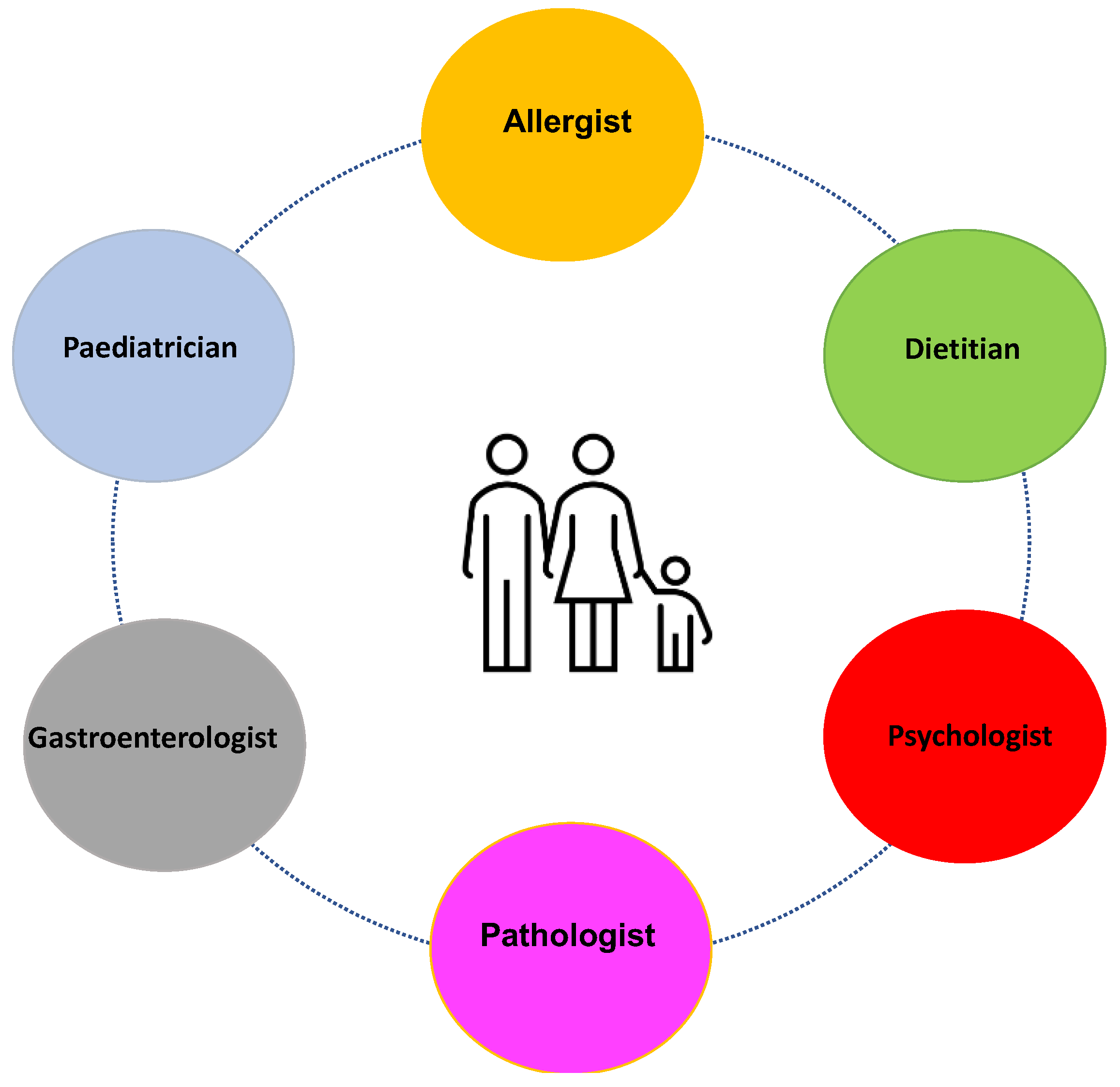
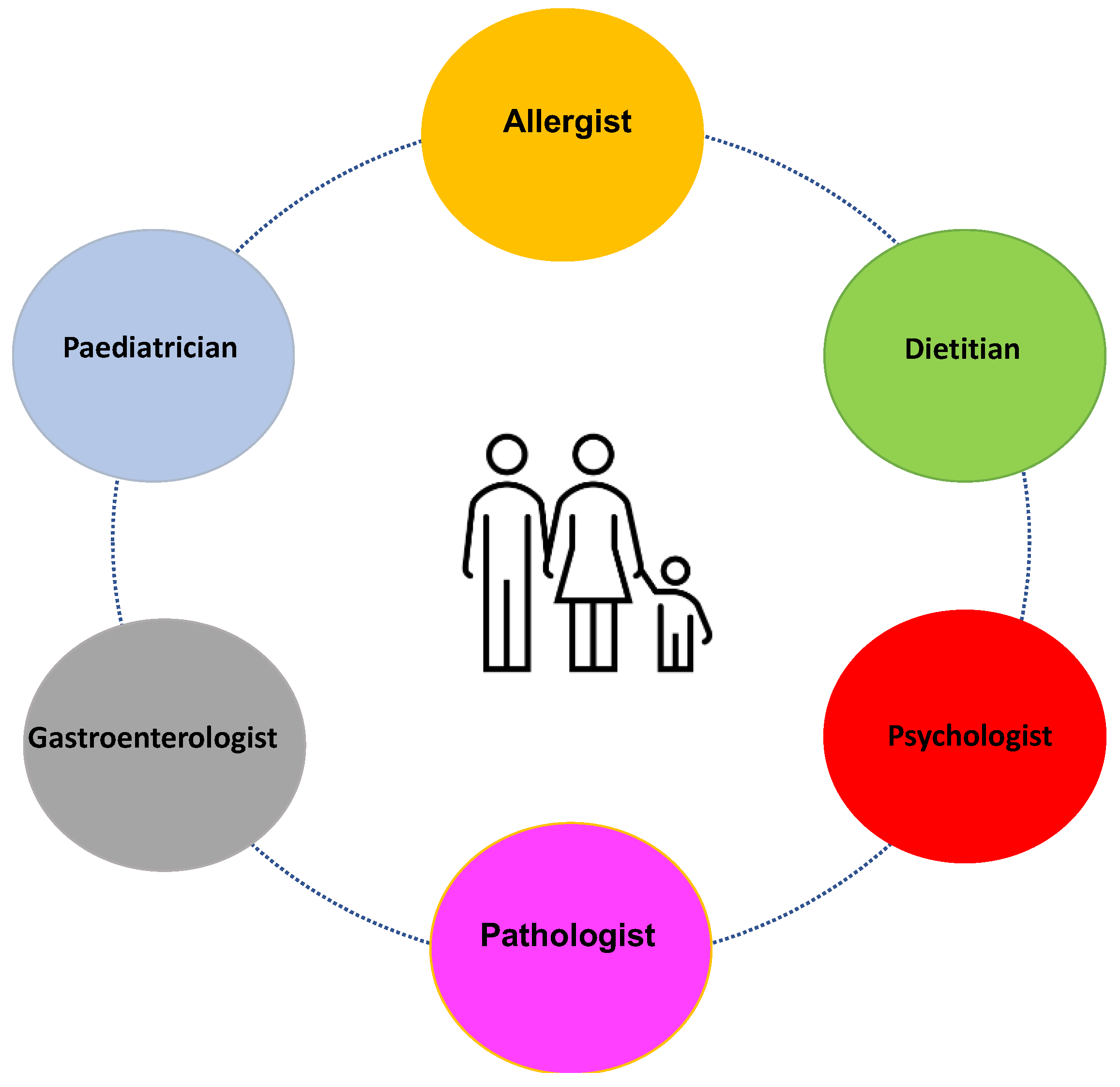
2.1. The Positioning of Dietary Therapy in the Management of EoE
2.2. Preliminary Considerations for Elimination Diets in the Clinical Setting
2.3. Dietary Treatment Possibilities
2.4. Elemental Diet
2.5. Elimination Diet Based on Food Allergy Testing
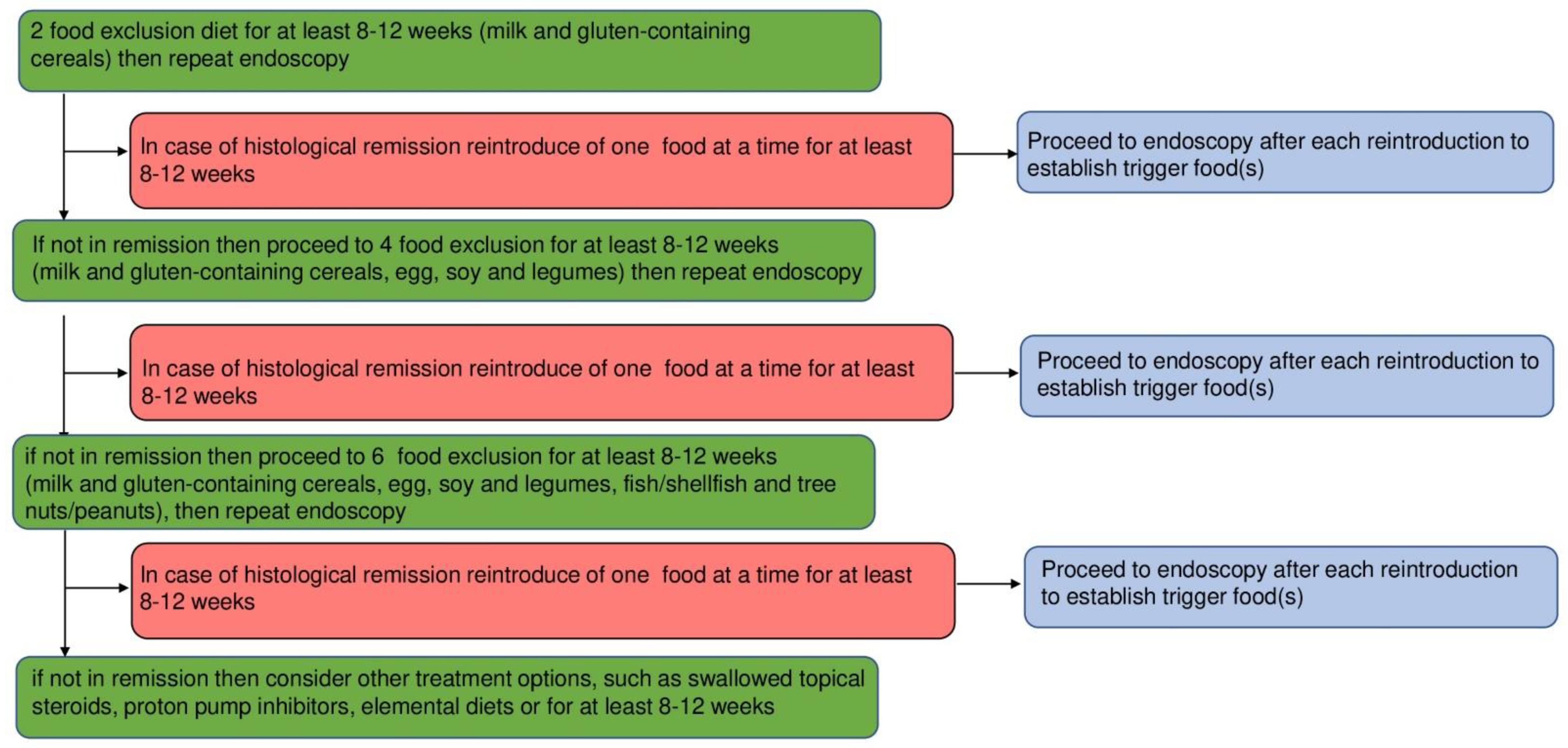
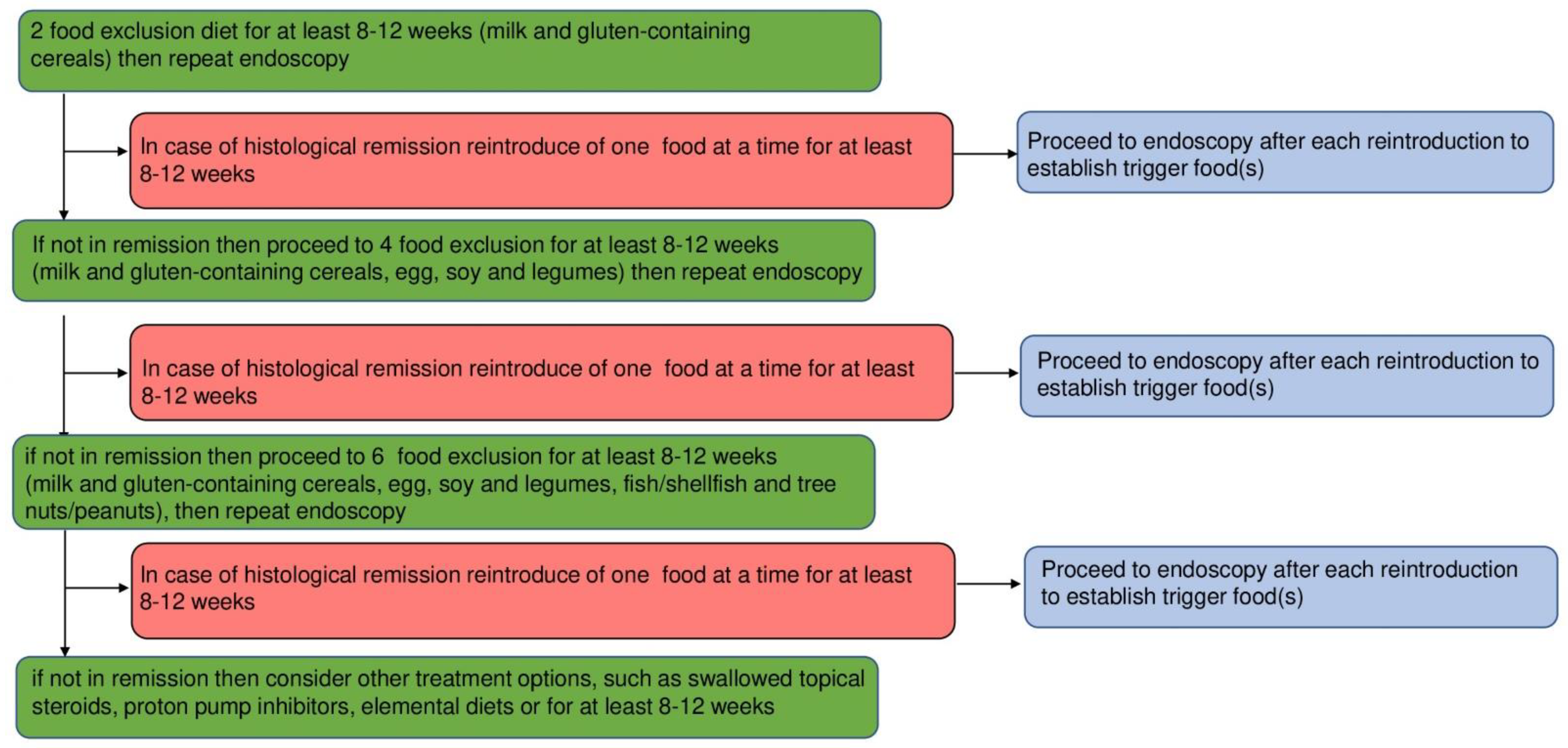
2.6. Empiric Elimination Diets
3. Geographical Factors
4. Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Dellon, E.S.; Hirano, I. Epidemiology and Natural History of Eosinophilic Esophagitis. Gastroenterology 2018, 154, 319–332.e3. [Google Scholar] [CrossRef]
- Allin, K.H.; Poulsen, G.; Melgaard, D.; Frandsen, L.T.; Jess, T.; Krarup, A.L. Eosinophilic oesophagitis in Denmark: Population-based incidence and prevalence in a nationwide study from 2008 to 2018. United Eur. Gastroenterol. J. 2022, 10, 640–650. [Google Scholar] [CrossRef]
- Bredenoord, A.J.; Patel, K.; Schoepfer, A.M.; Dellon, E.S.; Chehade, M.; Aceves, S.S.; Spergel, J.M.; Shumel, B.; Deniz, Y.; Rowe, P.J.; et al. Disease Burden and Unmet Need in Eosinophilic Esophagitis. Am. J. Gastroenterol. 2022, 117, 1231–1241. [Google Scholar] [CrossRef]
- Lu, M.; Goodwin, B.; Vera-Llonch, M.; Williams, J. Disease Burden and Treatment Patterns Associated with Eosinophilic Esophagitis in the United States: A Retrospective Claims Study. J. Clin. Gastroenterol. 2022, 56, 133–140. [Google Scholar] [CrossRef]
- Kidambi, T.; Toto, E.; Ho, N.; Taft, T.; Hirano, I. Temporal trends in the relative prevalence of dysphagia etiologies from 1999–2009. World J. Gastroenterol. 2012, 18, 4335–4341. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.J.; Lazenby, A.J.; Rowe, P.C.; Yardley, J.H.; Perman, J.A.; Sampson, H.A. Eosinophilic esophagitis attributed to gastroesophageal reflux: Improvement with an amino acid-based formula. Gastroenterology 1995, 109, 1503–1512. [Google Scholar] [CrossRef] [PubMed]
- Lucendo, A.J.; Molina-Infante, J.; Arias, Á.; von Arnim, U.; Bredenoord, A.J.; Bussmann, C.; Amil Dias, J.; Bove, M.; González-Cervera, J.; Larsson, H.; et al. Guidelines on eosinophilic esophagitis: Evidence-based statements and recommendations for diagnosis and management in children and adults. United Eur. Gastroenterol. J. 2017, 5, 335–358. [Google Scholar] [CrossRef]
- Rank, M.A.; Sharaf, R.N.; Furuta, G.T.; Aceves, S.S.; Greenhawt, M.; Spergel, J.M.; Falck-Ytter, Y.T.; Dellon, E.S.; AGA Institute. Technical Review on the Management of Eosinophilic Esophagitis: A Report from the AGA Institute and the Joint Task Force on Allergy-Immunology Practice Parameters. Gastroenterology 2020, 158, 1789–1810.e15. [Google Scholar] [CrossRef]
- Dhar, A.; Haboubi, H.N.; Attwood, S.E.; Auth, M.K.H.; Dunn, J.M.; Sweis, R.; Morris, D.; Epstein, J.; Novelli, M.R.; Hunter, H.; et al. British Society of Gastroenterology (BSG) and British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN) joint consensus guidelines on the diagnosis and management of eosinophilic oesophagitis in children and adults. Gut 2022, 71, 1459–1487. [Google Scholar] [CrossRef]
- Votto, M.; De Filippo, M.; Lenti, M.V.; Rossi, C.M.; Di Sabatino, A.; Marseglia, G.L.; Licari, A. Diet Therapy in Eosinophilic Esophagitis. Focus on a Personalized Approach. Front. Pediatr. 2022, 9, 820192. [Google Scholar] [CrossRef] [PubMed]
- Molina-Infante, J.; Lucendo, A.J. Dietary therapy for eosinophilic esophagitis. J. Allergy Clin. Immunol. 2018, 142, 41–47. [Google Scholar] [CrossRef]
- Visaggi, P.; Mariani, L.; Pardi, V.; Rosi, E.M.; Pugno, C.; Bellini, M.; Zingone, F.; Ghisa, M.; Marabotto, E.; Giannini, E.G.; et al. Dietary Management of Eosinophilic Esophagitis: Tailoring the Approach. Nutrients 2021, 13, 1630. [Google Scholar] [CrossRef] [PubMed]
- Pitsios, C.; Vassilopoulou, E.; Pantavou, K.; Terreehorst, I.; Nowak-Wegzryn, A.; Cianferoni, A.; Tsigkrelis, G.P.; Papachristodoulou, M.; Bonovas, S.; Nikolopoulos, G.K. Allergy-Test-Based Elimination Diets for the Treatment of Eosinophilic Esophagitis: A Systematic Review of Their Efficacy. J. Clin. Med. 2022, 11, 5631. [Google Scholar] [CrossRef] [PubMed]
- Hirano, I.; Chan, E.S.; Rank, M.A.; Sharaf, R.N.; Stollman, N.H.; Stukus, D.R.; Wang, K.; Greenhawt, M.; Falck-Ytter, Y.T.; AGA Institute Clinical Guidelines Committee; et al. AGA institute and the joint task force on allergy-immunology practice parameters clinical guidelines for the management of eosinophilic esophagitis. Ann. Allergy Asthma Immunol. 2020, 124, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Kagalwalla, A.F.; Sentongo, T.A.; Ritz, S.; Hess, T.; Nelson, S.P.; Emerick, K.M.; Melin-Aldana, H.; Li, B.U. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. 2006, 4, 1097–1102. [Google Scholar] [CrossRef]
- Gonsalves, N.; Yang, G.Y.; Doerfler, B.; Ritz, S.; Ditto, A.M.; Hirano, I. Elimination diet effectively treats eosinophilic esophagitis in adults; food reintroduction identifies causative factors. Gastroenterology 2012, 142, 1451–1459.e1. [Google Scholar] [CrossRef]
- Lucendo, A.J.; Arias, Á.; González-Cervera, J.; Yagüe-Compadre, J.L.; Guagnozzi, D.; Angueira, T.; Jiménez-Contreras, S.; González-Castillo, S.; Rodríguez-Domíngez, B.; De Rezende, L.C.; et al. Empiric 6-food elimination diet induced and maintained prolonged remission in patients with adult eosinophilic esophagitis: A prospective study on the food cause of the disease. J. Allergy Clin. Immunol. 2013, 13, 797–804. [Google Scholar] [CrossRef]
- Philpott, H.; Nandurkar, S.; Royce, S.G.; Thien, F.; Gibson, P.R. Allergy tests do not predict food triggers in adult patients with eosinophilic oesophagitis. A comprehensive prospective study using five modalities. Aliment. Pharmacol. Ther. 2016, 44, 223–233. [Google Scholar] [CrossRef]
- Doerfler, B.; Bryce, P.; Hirano, I.; Gonsalves, N. Practical approach to implementing dietary therapy in adults with eosinophilic esophagitis: The Chicago experience. Dis. Esophagus 2015, 28, 42–58. [Google Scholar] [CrossRef]
- Molina-Infante, J.; Arias, Á.; Alcedo, J.; Garcia-Romero, R.; Casabona-Frances, S.; Prieto-Garcia, A.; Modolell, I.; Gonzalez-Cordero, P.L.; Perez-Martinez, I.; Martin-Lorente, J.L.; et al. Step-up empiric elimination diet for pediatric and adult eosinophilic esophagitis: The 2-4-6 study. J. Allergy Clin. Immunol. 2018, 141, 1365–1372. [Google Scholar] [CrossRef]
- Molina-Infante, J.; Arias, A.; Barrio, J.; Rodríguez-Sánchez, J.; Sanchez-Cazalilla, M.; Lucendo, A.J. Four-food group elimination diet for adult eosinophilic esophagitis: A prospective multicenter study. J. Allergy Clin. Immunol. 2014, 134, 1093–1099.e1. [Google Scholar] [CrossRef]
- Hoofien, A.; Dias, J.A.; Malamisura, M.; Rea, F.; Chong, S.; Oudshoorn, J.; Nijenhuis-Hendriks, D.; Otte, S.; Papadopoulou, A.; Romano, C.; et al. Pediatric Eosinophilic Esophagitis: Results of the European Retrospective Pediatric Eosinophilic Esophagitis Registry (RetroPEER). J. Pediatr. Gastroenterol. Nutr. 2019, 68, 552–558. [Google Scholar] [CrossRef]
- van Rhijn, B.D.; van Ree, R.; Versteeg, S.A.; Vlieg-Boerstra, B.J.; Sprikkelman, A.B.; Terreehorst, I.; Smout, A.J.P.M.; Bredenoord, A.J. Birch pollen sensitization with cross-reactivity to food allergens predominates in adults with eosinophilic esophagitis. Allergy 2013, 68, 1475–1481. [Google Scholar] [CrossRef]
- Rossi, C.M.; Lenti, M.V.; Achilli, G.; Merli, S.; Mauro, A.; Anderloni, A.; Di Sabatino, A. High prevalence of sensitization to non-specific lipid transfer protein in adult patients with primary eosinophilic gastrointestinal disorders in Italy: A single center series. Clin. Mol. Allergy 2022, 20, 8. [Google Scholar] [CrossRef]
- Suto, D.; Murata, K.; Otake, T.; Ichiishi, E.; Sato, K.; Okada, S.; Okano, M.; Kohgo, Y. Eosinophilic esophagitis induced by sublingual immunotherapy with cedar pollen: A case report. Asia Pac. Allergy 2021, 1, e44. [Google Scholar] [CrossRef]
- Chehade, M.; Aceves, S.S. Treatment of Eosinophilic Esophagitis: Diet or Medication? J. Allergy Clin. Immunol. Pract. 2021, 9, 3249–3256. [Google Scholar] [CrossRef]
- Rossi, C.M.; Lenti, M.V.; Di Sabatino, A. The need for a reliable non-invasive diagnostic biomarker for eosinophilic oesophagitis. Lancet Gastroenterol. Hepatol. 2022, 7, 202–203. [Google Scholar] [CrossRef]
- Wechsler, J.B.; Ackerman, S.J.; Chehade, M.; Amsden, K.; Riffle, M.E.; Wang, M.Y.; Du, J.; Kleinjan, M.L.; Alumkal, P.; Gray, E.; et al. Noninvasive biomarkers identify eosinophilic esophagitis: A prospective longitudinal study in children. Allergy 2021, 76, 3755. [Google Scholar] [CrossRef]
- Rossi, C.M.; Lenti, M.V.; Merli, S.; Licari, A.; Votto, M.; Marseglia, G.L.; Di Sabatino, A. Primary eosinophilic gastrointestinal disorders and allergy: Clinical and therapeutic implications. Clin. Transl. Allergy 2022, 12, e12146. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Considerations |
|---|---|
| Factors pertaining to food/food categories to be eliminated |
|
| Factors pertaining to food/food categories to be reintroduced |
|
| Factors pertaining to the patient |
|
| Factors pertaining to the diagnostic procedure |
|
| Factors pertaining to the diet |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, C.M.; Lenti, M.V.; Merli, S.; Cena, H.; Di Sabatino, A. Dietary Strategies in Adult Patients with Eosinophilic Esophagitis: A State-of-the-Art Review. Nutrients 2023, 15, 2409. https://doi.org/10.3390/nu15102409
Rossi CM, Lenti MV, Merli S, Cena H, Di Sabatino A. Dietary Strategies in Adult Patients with Eosinophilic Esophagitis: A State-of-the-Art Review. Nutrients. 2023; 15(10):2409. https://doi.org/10.3390/nu15102409
Chicago/Turabian StyleRossi, Carlo Maria, Marco Vincenzo Lenti, Stefania Merli, Hellas Cena, and Antonio Di Sabatino. 2023. "Dietary Strategies in Adult Patients with Eosinophilic Esophagitis: A State-of-the-Art Review" Nutrients 15, no. 10: 2409. https://doi.org/10.3390/nu15102409
APA StyleRossi, C. M., Lenti, M. V., Merli, S., Cena, H., & Di Sabatino, A. (2023). Dietary Strategies in Adult Patients with Eosinophilic Esophagitis: A State-of-the-Art Review. Nutrients, 15(10), 2409. https://doi.org/10.3390/nu15102409