
Trends in Adherence to the Mediterranean Diet in Spanish Children and Adolescents across Two Decades

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  , , ,
, , ,  ,
,  ,
,  ,
,  , , ,
, , ,  ,
,  , ,
, ,  and
and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Participants
2.1.1. 1998–2000 Study
2.1.2. 2019–2020 Study
2.2. Dependent Variable
Mediterranean Diet Pattern Adequacy
2.3. Independent Variables
2.3.1. Residential Place Characteristics
2.3.2. Parental Education Level
2.3.3. Sleeping Hours
2.4. Statistical Analysis
3. Results
3.1. Comparison of Sociodemographic Characteristics of the Two Studies
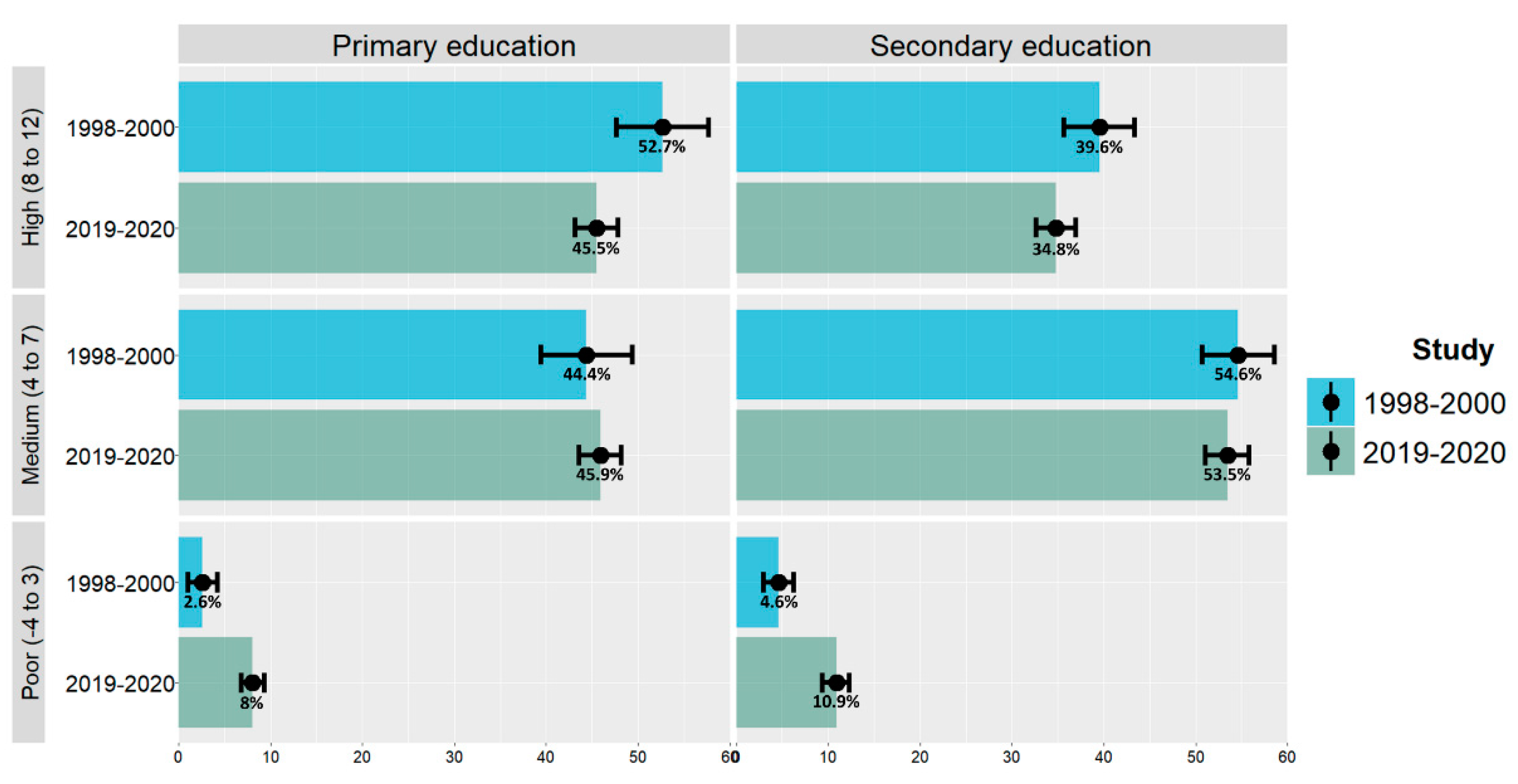
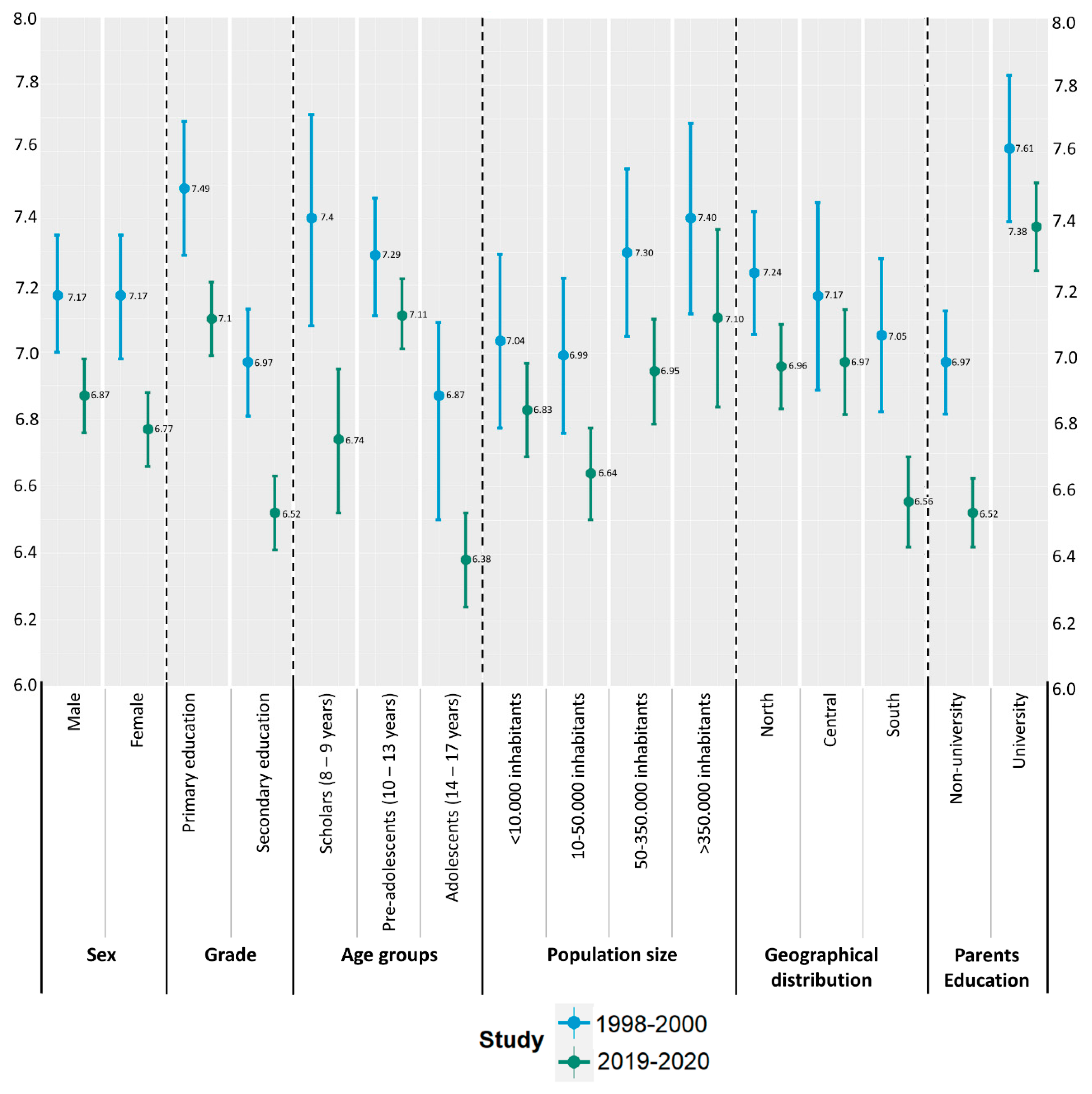
3.2. Adherence to the Mediterranean Diet
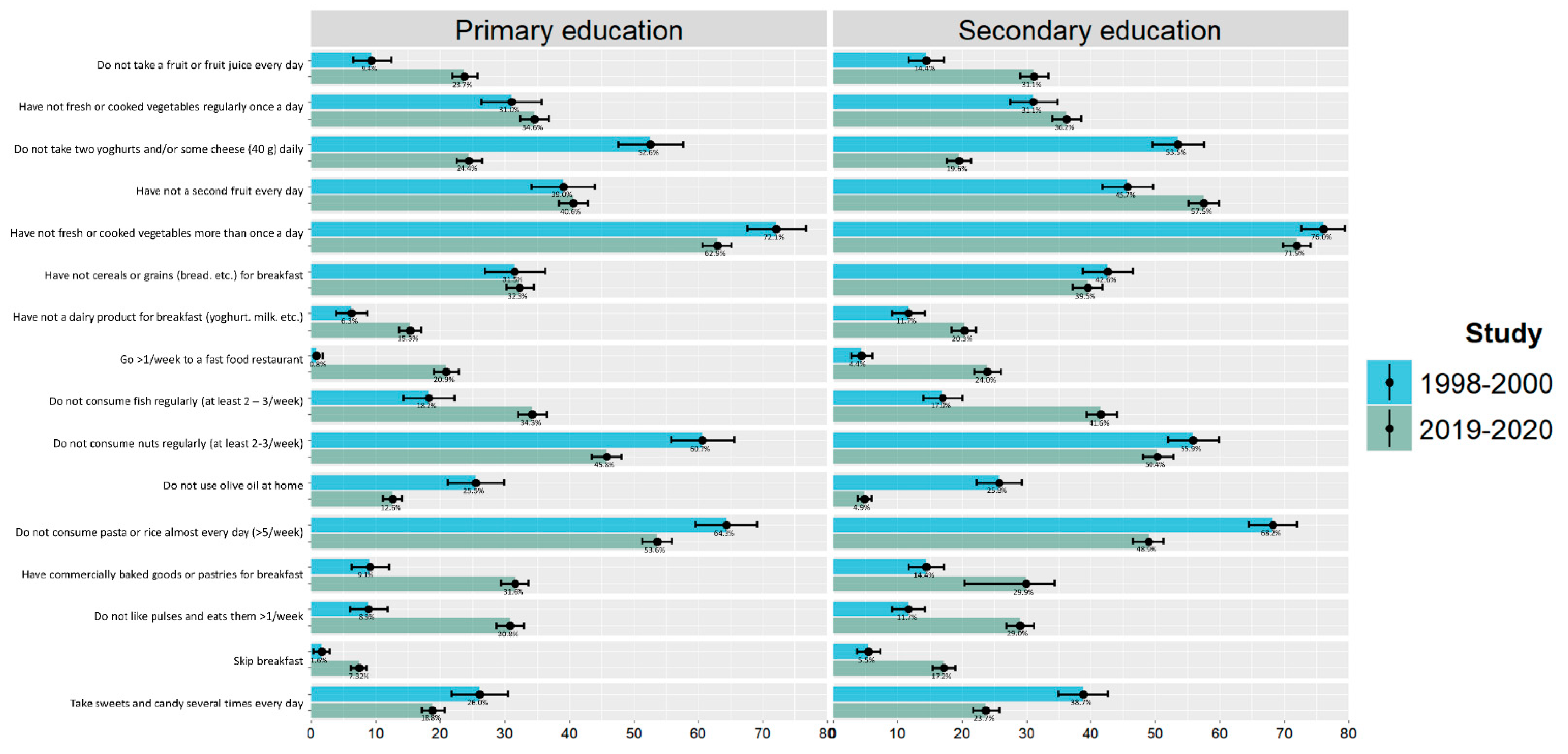
3.3. Food Habits
3.4. Sleep Hours
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dernini, S.; Berry, E.M. Mediterranean Diet: From a Healthy Diet to a Sustainable Dietary Pattern. Front. Nutr. 2015, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61 (Suppl. 6), 1402S–1406S. [Google Scholar] [CrossRef]
- Anand, S.S.; Hawkes, C.; de Souza, R.J.; Mente, A.; Dehghan, M.; Nugent, R.; Zulyniak, M.A.; Weis, T.; Bernstein, A.M.; Krauss, R.M. Food consumption and its impact on cardiovascular disease: Importance of solutions focused on the globalized food system. J. Am. Coll. Cardiol. 2015, 66, 1590–1614. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ezzatvar, Y.; López-Gil, J.F.; Ramírez-Vélez, R.; Olloquequi, J.; Izquierdo, M. Is adherence to the Mediterranean diet associated with healthy habits and physical fitness? A systematic review and meta-analysis including 565 421 youths. Br. J. Nutr. 2022, 128, 1433–1444. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Marventano, S.; Yang, J.; Micek, A.; Pajak, A.; Scalfi, L.; Galvano, F.; Kales, S.N. A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: Are individual components equal? Crit. Rev. Food Sci. Nutr. 2017, 57, 3218–3232. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.B.; Giugliano, D. A journey into a Mediterranean diet and type 2 diabetes: A systematic review with meta-analyses. BMJ Open 2015, 5, e008222. [Google Scholar] [CrossRef]
- Morze, J.; Danielewicz, A.; Przybyłowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2020, 60, 1561–1586. [Google Scholar] [CrossRef]
- Biagi, C.; Di Nunzio, M.; Bordoni, A.; Gori, D.; Lanari, M. Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review. Nutrients 2019, 11, 997. [Google Scholar] [CrossRef]
- Soltani, S.; Jayedi, A.; Shab-Bidar, S.; Becerra-Tomás, N.; Salas-Salvadó, J. Adherence to the Mediterranean Diet in Relation to All-Cause Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2019, 10, 1029–1039. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Unwin, N. Global diet and health: Old questions, fresh evidence, and new horizons. Lancet 2019, 393, 1916–1918. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Rosi, A.; Paolella, G.; Biasini, B.; Scazzina, F.; SINU Working Group on Nutritional Surveillance in Adolescents. Dietary habits of adolescents living in North America, Europe or Oceania: A review on fruit, vegetable and legume consumption, sodium intake, and adherence to the Mediterranean Diet. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 544–560. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef]
- Mariscal-Arcas, M.; Rivas, A.; Velasco, J.; Ortega, M.; Caballero, A.M.; Olea-Serrano, F. Evaluation of the Mediterranean Diet Quality Index (KIDMED) in children and adolescents in Southern Spain. Public Health Nutr. 2009, 12, 1408–1412. [Google Scholar] [CrossRef]
- Grao-Cruces, A.; Fernández-Martínez, A.; Nuviala, A. Association of Fitness with Life Satisfaction, Health Risk Behaviors, and Adherence to the Mediterranean Diet in Spanish Adolescents. J. Strength Cond. Res. 2014, 28, 2164–2172. [Google Scholar] [CrossRef]
- Arriscado, D.; Muros, J.J.; Zabala, M.; Dalmau, J.M. Factors associated with low adherence to a Mediterranean diet in healthy children in northern Spain. Appetite 2014, 80, 28–34. [Google Scholar] [CrossRef]
- Doménech-Asensi, G.; Sánchez-Martínez, Á.; Ros-Berruezo, G. Cross-sectional study to evaluate the associated factors with differences between city and districts secondary school students of the southeast of Spain (Murcia) for their adherence to the Mediterranean diet. Nutr. Hosp. 2014, 31, 1359–1365. [Google Scholar] [CrossRef]
- Arcila-Agudelo, A.M.; Ferrer-Svoboda, C.; Torres-Fernàndez, T.; Farran-Codina, A. Determinants of Adherence to Healthy Eating Patterns in a Population of Children and Adolescents: Evidence on the Mediterranean Diet in the City of Mataró (Catalonia, Spain). Nutrients 2019, 11, 854. [Google Scholar] [CrossRef]
- Bawaked, R.A.; Gomez, S.F.; Homs, C.; Esteve, R.C.; Cardenas, G.; Fíto, M.; Schröder, H. Association of eating behaviors, lifestyle, and maternal education with adherence to the Mediterranean diet in Spanish children. Appetite 2018, 130, 279–285. [Google Scholar] [CrossRef]
- Gómez, S.F.; Homs, C.; Wärnberg, J.; Medrano, M.; Gonzalez-Gross, M.; Gusi, N.; Aznar, S.; Cascales, E.M.; González-Valeiro, M.; Serra-Majem, L.; et al. Study protocol of a population-based cohort investigating Physical Activity, Sedentarism, lifestyles and Obesity in Spanish youth: The PASOS study. BMJ Open 2020, 10, e036210. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Ribas, L.; Pérez-Rodrigo, C.; García-Closas, R.; Peña-Quintana, L.; Aranceta, J. Determinants of Nutrient Intake among Children and Adolescents: Results from the enKid Study. Ann. Nutr. Metab. 2002, 46 (Suppl. 1), 31–38. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, A.R.; Carskadon, M.A.; Acebo, C.; Seifer, R.; Fallone, G.; Labyak, S.E.; Martin, J.L. Evidence for the Validity of a Sleep Habits Survey for Adolescents. Sleep 2003, 26, 213–216. [Google Scholar] [CrossRef]
- Bonaccio, M.; Bes-Rastrollo, M.; de Gaetano, G.; Iacoviello, L. Challenges to the Mediterranean diet at a time of economic crisis. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Abellán Alemán, J.; Zafrilla Rentero, M.P.; Montoro-García, S.; Mulero, J.; Pérez Garrido, A.; Leal, M.; Guerrero, L.; Ramos, E.; Ruilope, L.M. Adherence to the “Mediterranean Diet” in Spain and Its Relationship with Cardiovascular Risk (DIMERICA Study). Nutrients 2016, 8, 680. [Google Scholar] [CrossRef]
- Bibiloni, M.D.M.; Fernández-Blanco, J.; Pujol-Plana, N.; Martín-Galindo, N.; Fernández-Vallejo, M.M.; Roca-Domingo, M.; Chamorro-Medina, J.; Tur, J.A. Mejora de la calidad de la dieta y del estado nutricional en población infantil mediante un programa innovador de educación nutricional: INFADIMED. Gac. Sanit. 2017, 31, 472–477. [Google Scholar] [CrossRef]
- Papadaki, S.; Carayanni, V.; Notara, V.; Chaniotis, D. Anthropometric, Lifestyle Characteristics, Adherence to the Mediterranean Diet, and COVID-19 Have a High Impact on the Greek Adolescents’ Health-Related Quality of Life. Foods 2022, 11, 2726. [Google Scholar] [CrossRef]
- Sánchez-Rodríguez, L.; Fernández-Escobar, C.; Ordaz-Castillo, E.; Royo-Bordonada, M.Á. Adherencia a la dieta mediterránea y su asociación con factores sociodemográficos y antropométricos en adolescentes de Madrid [Adherence to mediterranean diet and its associated factors in adolescents from Madrid.]. Rev. Esp. Salud Publica (In Spanish). 2022, 96, e202210076. [Google Scholar]
- World Health Organization; Regional Office for Europe. Marketing of Foods High in Fat, Salt and Sugar to Children: Update 2012–2013. Regional Office for Europe. 2013. Available online: https://apps.who.int/iris/handle/10665/344812 (accessed on 18 November 2022).
- DBK Observatorio Sectorial. Repunte de las Ventas de las Empresas de Comida Rápida, Que Lograron Crecer un 9% en 2002. Fast Food. Nota de Prensa, Abril 2003. Available online: https://www.dbk.es/es/detalle-nota/fast-food-507 (accessed on 12 May 2021).
- Santaliestra-Pasías, A.M.; Felez, A.P.; Huybrechts, I.; Censi, L.; González-Gross, M.; Forsner, M.; Sjöström, M.; Lambrinou, C.P.; Amaro, F.; Kersting, M.; et al. Social Environment and Food and Beverage Intake in European Adolescents: The Helena Study. J. Am. Nutr. Assoc. 2022, 41, 468–480. [Google Scholar] [CrossRef]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Mokdad, A.H.; Ballestros, K.; Echko., M.; Glenn, S.; Olsen, H.E.; Mullany, E.; Lee, A.; Khan, A.R.; Ahmadi, A.; et al.; US Burden of Disease Collaborators The State of US Health, 1990–2016: Burden of Diseases, injuries, and risk factors among US States. JAMA 2018, 319, 1444–1472. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128.9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [PubMed]
- Appannah, G.; Murray, K.; Trapp, G.; Dymock, M.; Oddy, W.H.; Ambrosini, G.L. Dietary pattern trajectories across adolescence and early adulthood and their associations with childhood and parental factors. Am. J. Clin. Nutr. 2021, 113, 36–46. [Google Scholar] [CrossRef]
- Kanellopoulou, A.; Giannakopoulou, S.-P.; Notara, V.; Antonogeorgos, G.; Rojas-Gil, A.P.; Kornilaki, E.N.; Konstantinou, E.; Lagiou, A.; Panagiotakos, D.B. The association between adherence to the Mediterranean diet and childhood obesity; the role of family structure: Results from an epidemiological study in 1728 Greek students. Nutr. Health 2021, 27, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Gidding, S.S.; Dennison, B.A.; Birch, L.L.; Daniels, S.R.; Gilman, M.W.; Lichtenstein, A.H.; Rattay, K.T.; Steinberger, J.; Stettler, N.; Van Horn, L.; et al. Dietary Recommendations for Children and Adolescents: A guide for practitioners: Consensus statement from the American Heart Association. Circulation 2005, 112, 2061–2075. [Google Scholar] [CrossRef] [PubMed]
- Dalwood, P.; Marshall, S.; Burrows, T.L.; McIntosh, A.; Collins, C.E. Diet quality indices and their associations with health-related outcomes in children and adolescents: An updated systematic review. Nutr. J. 2020, 19, 118. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Adherence to Mediterranean Diet (KIDMED Index Categories) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Poor ≤ 3 | Medium 4–7 | High ≥ 8 | |||||||||||||
| 1998–2000 | 2019–2020 | p | 1998–2000 | 2019–2020 | p | 1998–2000 | 2019–2020 | p | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||||
| Sex | |||||||||||||||
| Male | 18 | 46.2 | 154 | 46 | 258 | 50.4 | 841 | 47.6 | 229 | 50.9 | 712 | 49.5 | |||
| Female | 21 | 53.8 | 181 | 54 | - | 254 | 49.6 | 927 | 52.4 | - | 221 | 49.1 | 725 | 50.5 | - |
| School grade | |||||||||||||||
| Primary education | 10 | 25.6 | 147 | 43.9 | 171 | 33.4 | 838 | 47.4 | 203 | 45.1 | 831 | 57.8 | |||
| Secondary education | 29 | 74.4 | 188 | 56.1 | <0.05 | 341 | 66.6 | 930 | 52.6 | <0.001 | 247 | 54.9 | 606 | 42.2 | <0.001 |
| Age group | |||||||||||||||
| (8–10] | 5 | 13.2 | 77 | 23.1 | 71 | 14.1 | 273 | 15.5 | 84 | 18.9 | 241 | 16.9 | |||
| (10–12] | 4 | 10.5 | 56 | 16.8 | 100 | 19.8 | 471 | 26.8 | 106 | 23.8 | 499 | 35.1 | |||
| (12–14] | 14 | 36.8 | 68 | 20.4 | 159 | 31.5 | 402 | 22.9 | 139 | 31.2 | 339 | 23.8 | |||
| (14–17] | 15 | 39.5 | 132 | 39.6 | - | 174 | 34.5 | 613 | 34.8 | <0.001 | 116 | 26.1 | 344 | 24.2 | <0.001 |
| Population size | |||||||||||||||
| <10,000 inhabitants | 10 | 25.6 | 83 | 24.8 | 132 | 25.8 | 553 | 31.3 | 105 | 23.3 | 425 | 29.6 | |||
| 10–50,000 inhabitants | 11 | 28.2 | 136 | 40.6 | 159 | 31.1 | 630 | 35.6 | 112 | 24.9 | 462 | 32.2 | |||
| 50–350,000 inhabitants | 10 | 25.6 | 92 | 27.5 | 132 | 25.8 | 435 | 24.6 | 124 | 27.6 | 409 | 28.5 | |||
| >350,000 inhabitants | 8 | 20.5 | 24 | 7.2 | <0.05 | 89 | 17.4 | 150 | 8.5 | <0.001 | 109 | 24.2 | 141 | 9.8 | <0.001 |
| Population size | |||||||||||||||
| <50,000 inhabitants | 21 | 53.8 | 219 | 65.4 | 291 | 56.8 | 1183 | 66.9 | 217 | 48.2 | 887 | 61.7 | |||
| >50,000 inhabitants | 18 | 46.2 | 116 | 34.6 | - | 221 | 43.2 | 585 | 33.1 | <0.001 | 233 | 51.8 | 550 | 38.3 | <0.001 |
| Geographical distribution | |||||||||||||||
| North | 17 | 43.6 | 112 | 33.4 | 245 | 47.9 | 677 | 38.3 | 226 | 50.2 | 582 | 40.5 | |||
| Centre | 11 | 28.2 | 80 | 23.9 | 109 | 21.3 | 432 | 24.4 | 97 | 21.6 | 394 | 27.4 | |||
| South | 11 | 28.2 | 143 | 42.7 | - | 158 | 30.9 | 659 | 37.3 | 0.001 | 127 | 28.2 | 461 | 32.1 | 0.001 |
| Geographical distribution | |||||||||||||||
| Centre | 11 | 28.2 | 80 | 23.9 | 109 | 21.3 | 432 | 24.4 | 97 | 21.6 | 394 | 27.4 | |||
| Northeast | 11 | 28.2 | 69 | 20.6 | 91 | 17.8 | 419 | 23.7 | 128 | 28.4 | 342 | 23.8 | |||
| North | 6 | 15.4 | 43 | 12.8 | 154 | 30.1 | 258 | 14.6 | 98 | 21.8 | 240 | 16.7 | |||
| South and Canary Islands | 6 | 15.4 | 90 | 26.9 | 103 | 20.1 | 364 | 20.6 | 80 | 17.8 | 263 | 18.3 | |||
| Levante | 5 | 12.8 | 53 | 15.8 | - | 55 | 10.7 | 295 | 16.7 | <0.001 | 47 | 10.4 | 198 | 13.8 | <0.001 |
| Comply with sleep recommendations | |||||||||||||||
| Yes | 33 | 84.6 | 178 | 54.1 | 450 | 88.2 | 1206 | 68.7 | 392 | 88.1 | 1130 | 79.5 | |||
| No | 6 | 15.4 | 151 | 45.9 | <0.001 | 60 | 11.8 | 550 | 31.3 | <0.001 | 53 | 11.9 | 291 | 20.5 | <0.001 |
| Parental Education | |||||||||||||||
| Non-university | 32 | 82.1 | 251 | 79.2 | 373 | 72.9 | 1131 | 68.1 | 287 | 63.8 | 773 | 56.5 | |||
| University | 7 | 17.9 | 66 | 20.8 | - | 139 | 27.1 | 531 | 31.9 | - | 163 | 36.2 | 594 | 43.5 | <0.01 |
| Adherence to Mediterranean Diet (KIDMED Index Scores) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1998–2000 | 2019–2020 | ||||||||
| n | Mean ± SD | Min | Max | n | Mean ± SD | Min | Max | p | |
| Sex | |||||||||
| Male | 505 | 7.17 ± 2.04 | 1 | 12 | 1707 | 6.87 ± 2.39 | −3 | 12 | 0.024 |
| Female | 496 | 7.17 ± 2.06 | 2 | 12 | 1833 | 6.77 ± 2.44 | −2 | 12 | 0.002 |
| Grade | |||||||||
| Primary education | 384 | 7.49 ± 1.98 | 2 | 12 | 1816 | 7.10 ± 2.41 | −2 | 12 | 0.012 |
| Secondary education | 617 | 6.97 ± 2.07 | 1 | 12 | 1724 | 6.52 ± 2.38 | −3 | 12 | 0.00005 |
| Age groups | |||||||||
| Scholars (8–9 years) | 159 | 7.40 ± 1.99 | 2 | 12 | 589 | 6.73 ± 2.63 | −1 | 12 | 0.008 |
| Pre-adolescents (10–13 years) | 520 | 7.29 ± 2.07 | 2 | 12 | 1835 | 7.11 ± 2.32 | −2 | 12 | - |
| Adolescents (14–17 years) | 322 | 6.87 ± 2.02 | 1 | 11 | 1116 | 6.38 ± 2.38 | −3 | 12 | 0.001 |
| Academic Year | |||||||||
| 3° primary degree | 68 | 7.38 ± 2.02 | 3 | 11 | 353 | 6.73 ± 2.58 | −1 | 12 | - |
| 4° primary degree | 88 | 7.35 ± 2.07 | 2 | 12 | 395 | 6.89 ± 2.54 | −1 | 12 | - |
| 5° primary degree | 124 | 7.68 ± 1.83 | 2 | 12 | 544 | 7.44 ± 2.21 | −1 | 12 | - |
| 6° primary degree | 104 | 7.45 ± 2.03 | 2 | 11 | 523 | 7.16 ± 2.34 | −2 | 12 | - |
| 1° secondary degree | 137 | 7.12 ± 2.16 | 2 | 11 | 370 | 7.03 ± 2.39 | 1 | 12 | - |
| 2° secondary degree | 170 | 6.96 ± 2.07 | 2 | 11 | 380 | 6.49 ± 2.26 | −1 | 12 | 0.025 |
| 3° secondary degree | 174 | 6.83 ± 2.05 | 2 | 11 | 450 | 6.48 ± 2.39 | −3 | 12 | - |
| 4° secondary degree | 136 | 7.01 ± 2.03 | 1 | 12 | 525 | 6.22 ± 2.40 | 1 | 12 | 0.00032 |
| Population size | |||||||||
| <10,000 inhabitants | 247 | 7.04 ± 2.07 | 2 | 12 | 1061 | 6.83 ± 2.32 | −1 | 12 | - |
| 10–50,000 inhabitants | 282 | 6.99 ± 1.98 | 2 | 11 | 1228 | 6.64 ± 2.45 | −1 | 12 | 0.045 |
| 50–350,000 inhabitants | 266 | 7.30 ± 2.07 | 1 | 12 | 936 | 6.95 ± 2.45 | −3 | 12 | - |
| >350,000 inhabitants | 206 | 7.40 ± 2.07 | 2 | 12 | 315 | 7.10 ± 2.39 | 1 | 12 | - |
| Spain region | |||||||||
| North | 488 | 7.24 ± 2.07 | 1 | 12 | 1371 | 6.96 ± 2.38 | −2 | 12 | 0.037 |
| Center | 217 | 7.17 ± 2.09 | 2 | 12 | 906 | 6.97 ± 2.41 | −1 | 12 | - |
| South | 296 | 7.05 ± 1.99 | 2 | 11 | 1263 | 6.56 ± 2.43 | −3 | 12 | 0.002 |
| Parents Education | |||||||||
| Non-university | 692 | 6.97 ± 2.06 | 1 | 12 | 2155 | 6.52 ± 2.42 | −3 | 12 | 0.000046 |
| University | 309 | 7.61 ± 1.95 | 3 | 12 | 1191 | 7.38 ± 2.31 | −1 | 12 | - |
| KIDMED Test Items | Answers Scoring | 1998–2000 n (%) | 2019–2020 n (%) | χ2 p-Value | |
|---|---|---|---|---|---|
| Takes a fruit or fruit juice every day | No | 0 | 125 (12.5) | 969 (27.4) | <0.001 |
| Yes | 1 | 876 (87.5) | 2571 (72.6) | ||
| Has a second fruit every day | No | 0 | 432 (43.2) | 1730 (48.9) | 0.001 |
| Yes | 1 | 569 (56.8) | 1810 (51.1) | ||
| Has fresh or cooked vegetables regularly once a day | No | 0 | 311 (31.1) | 1253 (35.4) | - |
| Yes | 1 | 690 (68.9) | 2287 (64.6) | ||
| Has fresh or cooked vegetables more than once a day | No | 0 | 746 (74.5) | 2382 (67.3) | <0.001 |
| Yes | 1 | 255 (25.5) | 1158 (32.7) | ||
| Consumes fish regularly (at least 2–3 times/week) | No | 0 | 175 (17.5) | 1339 (37.8) | <0.001 |
| Yes | 1 | 826 (82.5) | 2201 (62.2) | ||
| Goes > 1 time/week to a fast-food restaurant | No | 0 | 971 (97) | 2747 (77.6) | <0.001 |
| Yes | −1 | 30 (3) | 793 (22.4) | ||
| Likes pulses and eats them >1 time/week | No | 0 | 106 (10.6) | 1060 (29.9) | <0.001 |
| Yes | 1 | 895 (89.4) | 2480 (70.1) | ||
| Consumes pasta or rice almost every day (5 or more times per week) | No | 0 | 668 (66.7) | 1817 (51.3) | <0.001 |
| Yes | 1 | 333 (33.3) | 1723 (48.7) | ||
| Has cereals or grains (bread, etc.) for breakfast | No | 0 | 384 (38.4) | 1268 (35.8) | - |
| Yes | 1 | 617 (61.6) | 2272 (64.2) | ||
| Consumes nuts regularly (at least 2–3 times/week) | No | 0 | 578 (57.7) | 1701 (48.1) | <0.001 |
| Yes | 1 | 423 (42.3) | 1839 (51.9) | ||
| Uses olive oil at home | No | 0 | 257 (25.7) | 312 (8.8) | <0.001 |
| Yes | 1 | 744 (74.3) | 3228 (91.2) | ||
| Has breakfast | No | −1 | 40 (4) | 429 (12.1) | <0.001 |
| Yes | 0 | 961 (96) | 3111 (87.9) | ||
| Has a dairy product for breakfast (yoghurt, milk, etc.) | No | 0 | 96 (9.6) | 628 (17.7) | <0.001 |
| Yes | 1 | 905 (90.4) | 2912 (82.3) | ||
| Has commercially baked goods or pastries for breakfast | No | 0 | 877 (87.6) | 2414 (68.2) | <0.001 |
| Yes | −1 | 124 (12.4) | 1126 (31.8) | ||
| Takes two yoghurts and/or some cheese (40 g) daily | No | 0 | 532 (53.1) | 781 (22.1) | <0.001 |
| Yes | 1 | 469 (46.9) | 2759 (77.9) | ||
| Takes sweets and candy several times every day | No | 0 | 662 (66.1) | 2788 (78.8) | <0.001 |
| Yes | −1 | 339 (33.9) | 752 (21.2) | ||
| Primary Education | Secondary Education | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | ||||||||||||||||||
| 1998–2000 | 2019–2020 | χ2 | 1998–2000 | 2019–2020 | χ2 | 1998–2000 | 2019–2020 | χ2 | 1998–2000 | 2019–2020 | χ2 | ||||||||||
| KIDMED Test Items | n | (%) | n | (%) | p | n | (%) | n | (%) | p | n | (%) | n | (%) | p | n | (%) | n | (%) | p | |
| Takes a fruit or fruit juice every day | No | 17 | (8.7) | 221 | (24.6) | 19 | (10.1) | 210 | (22.9) | 45 | (14.6) | 257 | (31.7) | 44 | (14.3) | 281 | (30.7) | ||||
| Yes | 179 | (91.3) | 676 | (75.4) | a | 169 | (89.9) | 709 | (77.1) | a | 264 | (85.4) | 553 | (68.3) | a | 264 | (85.7) | 633 | (69.3) | a | |
| Has a second fruit every day | No | 75 | (38.3) | 381 | (42.5) | 75 | (39.9) | 357 | (38.8) | 146 | (47.2) | 472 | (58.3) | 136 | (44.2) | 520 | (56.9) | ||||
| Yes | 121 | (61.7) | 516 | (57.5) | 113 | (60.1) | 562 | (61.2) | 163 | (52.8) | 338 | (41.7) | b | 172 | (55.8) | 394 | (43.1) | a | |||
| Has fresh or cooked vegetables regularly once a day | No | 63 | (32.1) | 318 | (35.5) | 56 | (29.8) | 311 | (33.8) | 108 | (35) | 315 | (38.9) | 84 | (27.3) | 309 | (33.8) | ||||
| Yes | 133 | (67.9) | 579 | (64.5) | 132 | (70.2) | 608 | (66.2) | 201 | (65) | 495 | (61.1) | 224 | (72.7) | 605 | (66.2) | |||||
| Has fresh or cooked vegetables >1 time/day | No | 130 | (66.3) | 572 | (63.8) | 147 | (78.2) | 571 | (62.1) | 206 | (66.7) | 589 | (72.7) | 263 | (85.4) | 650 | (71.1) | ||||
| Yes | 66 | (33.7) | 325 | (36.2) | 41 | (21.8) | 348 | (37.9) | a | 103 | (33.3) | 221 | (27.3) | 45 | (14.6) | 264 | (28.9) | a | |||
| Consumes fish regularly (at least 2–3 times/week) | No | 42 | (21.4) | 310 | (34.6) | 28 | (14.9) | 312 | (33.9) | 54 | (17.5) | 308 | (38) | 51 | (16.6) | 409 | (44.7) | ||||
| Yes | 154 | (78.6) | 587 | (65.4) | a | 160 | (85.1) | 607 | (66.1) | a | 255 | (82.5) | 502 | (62) | a | 257 | (83.4) | 505 | (55.3) | a | |
| Goes >1 time/week to a fast- food restaurant | No | 196 | (100) | 714 | (79.6) | 185 | (98.4) | 722 | (78.6) | 294 | (95.1) | 607 | (74.9) | 296 | (96.1) | 704 | (77) | ||||
| Yes | 1 | (0) | 183 | (20.4) | a | 3 | (1.6) | 197 | (21.4) | a | 15 | (4.9) | 203 | (25.1) | a | 12 | (3.9) | 210 | (23) | a | |
| Likes pulses and eats them >1 time/week | No | 17 | (8.7) | 281 | (31.3) | 17 | (9) | 279 | (30.4) | 35 | (11.3) | 209 | (25.8) | 37 | (12) | 291 | (31.8) | ||||
| Yes | 179 | (91.3) | 616 | (68.7) | a | 171 | (91) | 640 | (69.6) | a | 274 | (88.7) | 601 | (74.2) | a | 271 | (88) | 623 | (68.2) | a | |
| Consumes pasta or rice almost every day (≥5 times per week) | No | 131 | (66.8) | 468 | (52.2) | 116 | (61.7) | 505 | (55) | 203 | (65.7) | 377 | (46.5) | 218 | (70.8) | 467 | (51.1) | ||||
| Yes | 65 | (33.2) | 429 | (47.8) | a | 72 | (38.3) | 414 | (45) | 106 | (34.3) | 433 | (53.5) | a | 90 | (29.2) | 447 | (48.9) | a | ||
| Has cereals or grains (bread, etc.) for breakfast | No | 50 | (25.5) | 296 | (33) | 71 | (37.8) | 291 | (31.7) | 115 | (37.2) | 306 | (37.8) | 148 | (48.1) | 375 | (41) | ||||
| Yes | 146 | (74.5) | 601 | (67) | 117 | (62.2) | 628 | (68.3) | 194 | (62.8) | 504 | (62.2) | 160 | (51.9) | 539 | (59) | |||||
| Consumes nuts regularly (at least 2–3 times/week) | No | 126 | (64.3) | 413 | (46) | 107 | (56.9) | 419 | (45.6) | 168 | (54.4) | 398 | (49.1) | 177 | (57.5) | 471 | (51.5) | ||||
| Yes | 70 | (35.7) | 484 | (54) | a | 81 | (43.1) | 500 | (54.4) | 141 | (45.6) | 412 | (50.9) | 131 | (42.5) | 443 | (48.5) | ||||
| Uses olive oil at home | No | 44 | (22.4) | 128 | (14.3) | 54 | (28.7) | 100 | (10.9) | 86 | (27.8) | 55 | (6.8) | 73 | (23.7) | 29 | (3.2) | ||||
| Yes | 152 | (77.6) | 769 | (85.7) | 134 | (71.3) | 819 | (89.1) | a | 223 | (72.2) | 755 | (93.2) | a | 235 | (76.3) | 885 | (96.8) | a | ||
| Has breakfast | No | 3 | (1.5) | 55 | (6.1) | 3 | (1.6) | 78 | (8.5) | 15 | (4.9) | 106 | (13.1) | 19 | (6.2) | 190 | (20.8) | ||||
| Yes | 193 | (98.5) | 842 | (93.9) | 185 | (98.4) | 841 | (91.5) | b | 294 | (95.1) | 704 | (86.9) | a | 289 | (93.8) | 724 | (79.2) | a | ||
| Has a dairy product for breakfast (yoghurt, milk, etc.) | No | 10 | (5.1) | 134 | (14.9) | 14 | (7.4) | 144 | (15.7) | 30 | (9.7) | 134 | (16.5) | 42 | (13.6) | 216 | (23.6) | ||||
| Yes | 186 | (94.9) | 763 | (85.1) | a | 174 | (92.6) | 775 | (84.3) | c | 279 | (90.3) | 676 | (83.5) | 266 | (86.4) | 698 | (76.4) | a | ||
| Has commercially baked goods/pastries for breakfast | No | 179 | (91.3) | 616 | (68.7) | 170 | (90.4) | 627 | (68.2) | 262 | (84.8) | 544 | (67.2) | 266 | (86.4) | 627 | (68.6) | ||||
| Yes | 17 | (8.7) | 281 | (31.3) | a | 18 | (9.6) | 292 | (31.8) | a | 47 | (15.2) | 266 | (32.8) | a | 42 | (13.6) | 287 | (31.4) | a | |
| Takes two yoghurts and/or some cheese (40 g) daily | No | 97 | (49.5) | 232 | (25.9) | 105 | (55.9) | 212 | (23.1) | 159 | (51.5) | 152 | (18.8) | 171 | (55.5) | 185 | (20.2) | ||||
| Yes | 99 | (50.5) | 665 | (74.1) | a | 83 | (44.1) | 707 | (76.9) | a | 150 | (48.5) | 658 | (81.2) | a | 137 | (44.5) | 729 | (79.8) | a | |
| Takes sweets and candy several times every day | No | 147 | (75) | 733 | (81.7) | 137 | (72.9) | 741 | (80.6) | 175 | (56.6) | 637 | (78.6) | 203 | (65.9) | 677 | (74.1) | ||||
| Yes | 49 | (25) | 164 | (18.3) | 51 | (27.1) | 178 | (19.4) | 134 | (43.4) | 173 | (21.4) | a | 105 | (34.1) | 237 | (25.9) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Ramos, E.; Tomaino, L.; Sánchez-Villegas, A.; Ribas-Barba, L.; Gómez, S.F.; Wärnberg, J.; Osés, M.; González-Gross, M.; Gusi, N.; Aznar, S.; et al. Trends in Adherence to the Mediterranean Diet in Spanish Children and Adolescents across Two Decades. Nutrients 2023, 15, 2348. https://doi.org/10.3390/nu15102348
Herrera-Ramos E, Tomaino L, Sánchez-Villegas A, Ribas-Barba L, Gómez SF, Wärnberg J, Osés M, González-Gross M, Gusi N, Aznar S, et al. Trends in Adherence to the Mediterranean Diet in Spanish Children and Adolescents across Two Decades. Nutrients. 2023; 15(10):2348. https://doi.org/10.3390/nu15102348
Chicago/Turabian StyleHerrera-Ramos, Estefanía, Laura Tomaino, Almudena Sánchez-Villegas, Lourdes Ribas-Barba, Santiago F. Gómez, Julia Wärnberg, Maddi Osés, Marcela González-Gross, Narcis Gusi, Susana Aznar, and et al. 2023. "Trends in Adherence to the Mediterranean Diet in Spanish Children and Adolescents across Two Decades" Nutrients 15, no. 10: 2348. https://doi.org/10.3390/nu15102348
APA StyleHerrera-Ramos, E., Tomaino, L., Sánchez-Villegas, A., Ribas-Barba, L., Gómez, S. F., Wärnberg, J., Osés, M., González-Gross, M., Gusi, N., Aznar, S., Marín-Cascales, E., González-Valeiro, M. Á., Terrados, N., Tur, J. A., Segú, M., Fitó, M., Homs, C., Benavente-Marín, J. C., Labayen, I., ... Serra-Majem, L. (2023). Trends in Adherence to the Mediterranean Diet in Spanish Children and Adolescents across Two Decades. Nutrients, 15(10), 2348. https://doi.org/10.3390/nu15102348