
Vitamin D in the Prevention and Treatment of Oral Cancer: A Scoping Review

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Protocol and Eligibility Criteria
2.2. Information Sources and Search
2.3. Selection of Sources of Evidence and Data Charting Process
2.4. Data Items and Synthesis of the Results
3. Results
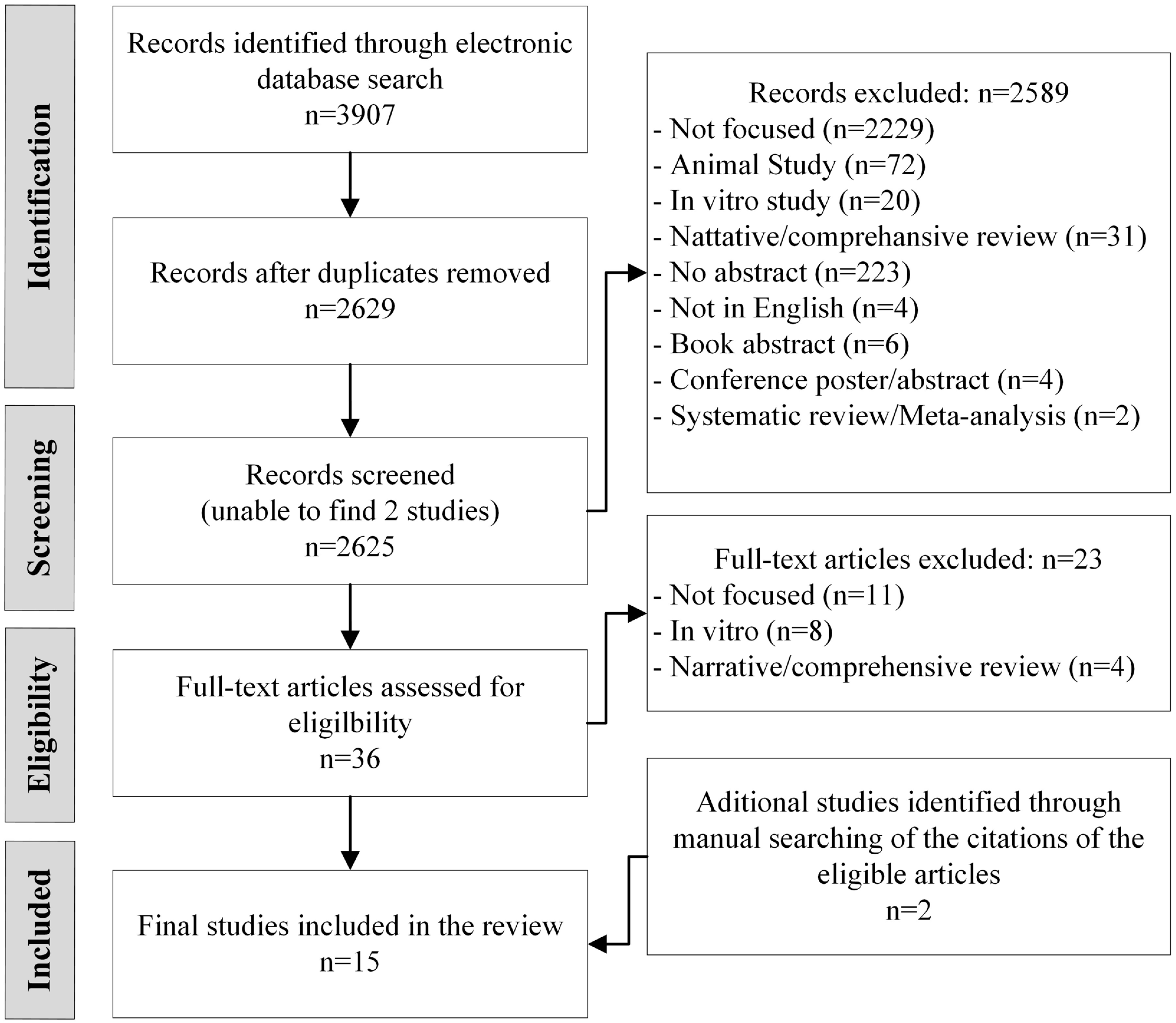
Selection, Characteristics of Sources of Evidence, and Summary Results
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ellington, T.D.; Henley, S.J.; Senkomago, V.; O’Neil, M.E.; Wilson, R.J.; Singh, S.; Thomas, C.C.; Wu, M.; Richardson, L.C. Trends in Incidence of Cancers of the Oral Cavity and Pharynx—United States 2007–2016. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 433–438. [Google Scholar] [CrossRef]
- World Cancer Research Fund International. 2022. Available online: https://www.wcrf.org/cancer-trends/mouth-and-oral-cancer-statistics/ (accessed on 28 February 2023).
- American Cancer Society (ACS). Key Statistics for Oral Cavity and Oropharyngeal Cancers. Available online: https://www.cancer.org/cancer/oral-cavity-and-oropharyngeal-cancer/about/key-statistics.html (accessed on 28 February 2023).
- Rahib, L.; Wehner, M.R.; Matrisian, L.M.; Nead, K.T. Estimated Projection of US Cancer Incidence and Death to 2040. JAMA Netw. Open. 2021, 4, e214708. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.J.; Wilson, M.J.; Crean, S.J. Exploring the link between microorganisms and oral cancer: A systematic review of the literature. Head Neck 2009, 31, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Jaber, M.A.; Porter, S.R.; Gilthorpe, M.S.; Bedi, R.; Scully, C. Risk factors for oral epithelial dysplasia--the role of smoking and alcohol. Oral. Oncol. 1999, 35, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.C.; Huang, Y.L.; Lee, C.H.; Chen, M.J.; Lin, L.M.; Tsai, C.C. Betel quid chewing, cigarette smoking and alcohol consumption related to oral cancer in Taiwan. J. Oral. Pathol. Med. 1995, 24, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Ogden, G.R.; Wight, A.J. Aetiology of oral cancer: Alcohol. Br. J. Oral. Maxillofac. Surg. 1998, 36, 247–251. [Google Scholar] [CrossRef]
- Syrjänen, S. Human papillomavirus (HPV) in head and neck cancer. J. Clin. Virol. 2005, 32 (Suppl. 1), S59–S66. [Google Scholar] [CrossRef]
- Omura, K. Current status of oral cancer treatment strategies: Surgical treatments for oral squamous cell carcinoma. Int. J. Clin. Oncol. 2014, 19, 423–430. [Google Scholar] [CrossRef]
- Xi, S.; Grandis, J.R. Gene therapy for the treatment of oral squamous cell carcinoma. J. Dent. Res. 2003, 82, 11–16. [Google Scholar] [CrossRef]
- da Silva, S.D.; Ferlito, A.; Takes, R.P.; Brakenhoff, R.H.; Valentin, M.D.; Woolgar, J.A.; Bradford, C.R.; Rodrigo, J.P.; Rinaldo, A.; Hier, M.P.; et al. Advances and applications of oral cancer basic research. Oral. Oncol. 2011, 47, 783–791. [Google Scholar] [CrossRef]
- Fathi, N.; Ahmadian, E.; Shahi, S.; Roshangar, L.; Khan, H.; Kouhsoltani, M.; Dizaj, S.M.; Sharifi, S. Role of vitamin D and vitamin D receptor (VDR) in oral cancer. Biomed. Pharmacother. 2019, 109, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.V.; Feldman, D. Mechanisms of the anti-cancer and anti-inflammatory actions of vitamin D. Annu. Rev. Pharmacol. Toxicol. 2011, 51, 311–336. [Google Scholar] [CrossRef] [PubMed]
- Ness, R.A.; Miller, D.D.; Wei, L. The role of vitamin D in cancer prevention. Chin. J. Nat. Med. 2015, 13, 481–497. [Google Scholar] [CrossRef]
- Dev, R.; Del Fabbro, E.; Schwartz, G.G.; Hui, D.; Palla, S.L.; Gutierrez, N.; Bruera, E. Preliminary report: Vitamin D deficiency in advanced cancer patients with symptoms of fatigue or anorexia. Oncologist 2011, 16, 1637–1641. [Google Scholar] [CrossRef]
- Stone, C.A.; Kenny, R.A.; Healy, M.; Walsh, J.B.; Lawlor, P.G. Vitamin D depletion: Of clinical significance in advanced cancer? Support. Care Cancer 2011, 19, 865–867. [Google Scholar] [CrossRef]
- Abbas, S.; Linseisen, J.; Slanger, T.; Kropp, S.; Mutschelknauss, E.J.; Flesch-Janys, D.; Chang-Claude, J. Serum 25-hydroxyvitamin D and risk of post-menopausal breast cancer--results of a large case-control study. Carcinogenesis 2008, 29, 93–99. [Google Scholar] [CrossRef]
- Ahonen, M.H.; Tenkanen, L.; Teppo, L.; Hakama, M.; Tuohimaa, P. Prostate cancer risk and prediagnostic serum 25-hydroxyvitamin D levels (Finland). Cancer Causes Control. 2000, 11, 847–852. [Google Scholar] [CrossRef]
- Gorham, E.D.; Garland, C.F.; Garland, F.C.; Grant, W.B.; Mohr, S.B.; Lipkin, M.; Newmark, H.L.; Giovannucci, E.; Wei, M.; Holick, M.F. Vitamin D and prevention of colorectal cancer. J. Steroid Biochem. Mol. Biol. 2005, 97, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Park, W.H.; Seol, J.G.; Kim, E.S.; Jung, C.W.; Lee, C.C.; Binderup, L.; Koeffler, H.P.; Kim, B.K.; Lee, Y.Y. Cell cycle arrest induced by the vitamin D(3) analog EB1089 in NCI-H929 myeloma cells is associated with induction of the cyclin-dependent kinase inhibitor p27. Exp. Cell Res. 2000, 254, 279–286. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Anand, A.; Singh, S.; Sonkar, A.A.; Husain, N.; Singh, K.R.; Singh, S.; Kushwaha, J.K. Expression of vitamin D receptor and vitamin D status in patients with oral neoplasms and effect of vitamin D supplementation on quality of life in advanced cancer treatment. Contemp. Oncol. 2017, 21, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Arem, H.; Weinstein, S.J.; Horst, R.L.; Virtamo, J.; Yu, K.; Albanes, D.; Abnet, C.C. Serum 25-Hydroxyvitamin D and Risk of Oropharynx and Larynx Cancers in Finnish Men. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Bektas-Kayhan, K.; Unur, M.; Yaylim-Eraltan, I.; Ergen, H.A.; Toptas, B.; Hafiz, G.; Karadeniz, A.; Isbir, T. Association of Vitamin D Receptor Taq I Polymorphism and Susceptibility to Oral Squamous Cell Carcinoma. In Vivo 2010, 24, 755–759. [Google Scholar]
- Dudding, T.; Johansson, M.; Thomas, S.J.; Brennan, P.; Martin, R.M.; Timpson, N.J. Assessing the causal association between 25-hydroxyvitamin D and the risk of oral and oropharyngeal cancer using Mendelian randomization. Int. J. Cancer 2018, 143, 1029–1036. [Google Scholar] [CrossRef]
- Giovannucci, E.; Liu, Y.; Willett, W.C. Cancer incidence and mortality and vitamin D in Black and White male health professionals. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2467–2472. [Google Scholar] [CrossRef]
- Grimm, M.; Alexander, D.; Munz, A.; Hoffmann, J.; Reinert, S. Is 1,25-dihydroxyvitamin D-3 receptor expression a potential Achilles’ heel of CD44+oral squamous cell carcinoma cells? Target. Oncol. 2013, 8, 189–201. [Google Scholar] [CrossRef]
- Grimm, M.; Cetindis, M.; Biegner, T.; Lehman, M.; Munz, A.; Teriete, P.; Reinert, S. Serum vitamin D levels of patients with oral squamous cell carcinoma (OSCC) and expression of vitamin D receptor in oral precancerous lesions and OSCC. Med. Oral. Patol. Oral. Y Cir. Bucal 2015, 20, E188–E195. [Google Scholar] [CrossRef]
- Lipworth, L.; Rossi, M.; McLaughlin, J.K.; Negri, E.; Talamini, R.; Levi, F.; Franceschi, S.; La Vecchia, C. Dietary vitamin D and cancers of the oral cavity and esophagus. Ann. Oncol. 2009, 20, 1576–1581. [Google Scholar] [CrossRef] [PubMed]
- Malodobra-Mazur, M.; Paduch, A.; Lebioda, A.; Konopacka, M.; Rogolinski, J.; Szymczyk, C.; Wierzgon, J.; Maciejewski, A.; Chmielik, E.; Jonkisz, A.; et al. VDR gene single nucleotide polymorphisms and their association with risk of oral cavity carcinoma. Acta Biochim. Pol. 2012, 59, 627–630. [Google Scholar] [CrossRef] [PubMed]
- Negri, E.; Franceschi, S.; Bosetti, C.; Levi, F.; Conti, E.; Parpinel, M.; La Vecchia, C. Selected micronutrients and oral and pharyngeal cancer. Int. J. Cancer 2000, 86, 122–127. [Google Scholar] [CrossRef]
- Nuszkiewicz, J.; Czuczejko, J.; Maruszak, M.; Pawłowska, M.; Woźniak, A.; Małkowski, B.; Szewczyk-Golec, K. Parameters of Oxidative Stress, Vitamin D, Osteopontin, and Melatonin in Patients with Lip, Oral Cavity, and Pharyngeal Cancer. Oxid. Med. Cell. Longev. 2021, 2021, 2364931. [Google Scholar] [CrossRef] [PubMed]
- Udeabor, S.E.; Albejadi, A.M.; Al-Shehri, W.A.K.; Onwuka, C.I.; Al-Fathani, S.Y.; Al Nazeh, A.A.; Aldhahri, S.F.; Alshahrani, F.A. Serum levels of 25-hydroxy-vitamin D in patients with oral squamous cell carcinoma: Making a case for chemoprevention. Clin. Exp. Dent. Res. 2020, 6, 428–432. [Google Scholar] [CrossRef]
- Young, M.R.I.; Levingston, C.; Johnson, S.D. Cytokine and Adipokine Levels in Patients with Premalignant Oral Lesions or in Patients with Oral Cancer Who Did or Did Not Receive 1 alpha,25-Dihydroxyvitamin D-3 Treatment upon Cancer Diagnosis. Cancers 2015, 7, 1109–1124. [Google Scholar] [CrossRef] [PubMed]
- Zeljic, K.; Supic, G.; Radak, M.S.; Jovic, N.; Kozomara, R.; Magic, Z. Vitamin D receptor, CYP27B1 and CYP24A1 genes polymorphisms association with oral cancer risk and survival. J. Oral. Pathol. Med. 2012, 41, 779–787. [Google Scholar] [CrossRef]
- Zhang, H.; Lu, H.; Shrestha, C.; Feng, Y.; Li, Y.; Peng, J.; Li, Y.; Xie, Z. In serum, higher parathyroid hormone but not lower vitamin D is associated with oral squamous cell carcinoma. Curr. Oncol. 2015, 22, E259–E263. [Google Scholar] [CrossRef]
- van Ginkel, P.R.; Yang, W.; Marcet, M.M.; Chow, C.C.; Kulkarni, A.D.; Darjatmoko, S.; Lindstrom, M.J.; Lokken, J.; Bhattacharya, S.; Albert, D.M. 1 alpha-Hydroxyvitamin D2 inhibits growth of human neuroblastoma. J. Neurooncol. 2007, 85, 255–262. [Google Scholar] [CrossRef]
- Maturana-Ramirez, A.; Aitken-Saavedra, J.; Guevara-Benitez, A.L.D.; Espinoza-Santander, I. Hypovitaminosis D, oral potentially malignant disorders, and oral squamous cell carcinoma: A systematic review. Med. Oral. Patol. Oral. Y Cir. Bucal 2022, 27, E135–E141. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, W.; Li, D.; Yin, X.; Zhang, X.; Olsen, N.; Zheng, S.G. Vitamin D and chronic diseases. Aging Dis. 2017, 8, 346. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Gandini, S.; Mullie, P. A Systematic Review: Influence of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Concentration. J. Clin. Endocrinol. Metab. 2012, 97, 2606–2613. [Google Scholar] [CrossRef] [PubMed]
- Laczmanski, L.; Laczmanska, I.; Lwow, F. Association of select vitamin D receptor gene polymorphisms with the risk of tobacco-related cancers—A meta-analysis. Sci. Rep. 2019, 9, 16026. [Google Scholar] [CrossRef]
- Yuan, L.; Ni, J. The association between tobacco smoke exposure and vitamin D levels among US general population, 2001-2014: Temporal variation and inequalities in population susceptibility. Environ. Sci. Pollut. Res. Int. 2022, 29, 32773–32787. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Criteria Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Outcome |
|
|
| Study design |
|
|
| Participant characteristics |
|
|
| Electronic Databases | Search Strategies | Extent of Search | Number of Articles |
|---|---|---|---|
| Medline www.ncbi.nlm.nih.gov/sites/entrez (Accessed on 20 July 2022) | ((Vitamin D) OR (Vitamin D2) OR (Vitamin D3) OR (Calcidiol) OR (Calcitriol) OR (Ergocalciferol) OR (Cholecalciferol) OR (25-hydroxyvitamin D) OR (25(OH)D) OR (Vit D) OR (Vit D2) OR (Vit D3)) AND ((Oral Cancer*) OR (Mouth Cancer*) OR (Oral Neoplasm*) OR (Mouth Neoplasm*) OR (Oral Carcinoma*) OR (Mouth Carcinoma*) OR (Oral Malignancy) OR (Oral malignancies) OR (Mouth Malignancy) OR (Mouth Malignancies) OR (Oral Tumor*) OR (Mouth Tumor*)) | In all fields | 1035 |
| Web of Science https://clarivate.com/webofsciencegroup/solutions/web-of-science/ (Accessed on 20 July 2022) | (((((((((((ALL=(Vitamin D)) OR ALL=(Vitamin D2)) OR ALL=(Vitamin D3)) OR ALL=(Vit D)) OR ALL=(Vit D2)) OR ALL=(Vit D3)) OR ALL=(Calcitriol)) OR ALL=(Calcidiol)) OR ALL=(Ergocalciferol)) OR ALL=(Cholecalciferol)) OR ALL=(25-hydroxyvitamin)) OR ALL=(25(OH)D) AND (((((((((((ALL=(Oral Cancer*)) OR ALL=(Mouth cancer*)) OR ALL=(Oral Neoplasm*)) OR ALL=(Mouth Neoplasm*)) OR ALL=(Oral Carcinoma*)) OR ALL=(Mouth Carcinoma*)) OR ALL=(Mouth Malignancy)) OR ALL=(Mouth Malignancies)) OR ALL=(Oral Malignancy)) OR ALL=(Oral malignancies)) OR ALL=(Oral Tumor*)) OR ALL=(Mouth Tumor*) | In all fields | 1532 |
| Science Direct http://www.sciencedirect.com (Accessed on 20 July 2022) | (“Vitamin D” OR “Vitamin D2” OR “Vitamin D3”) AND (“Oral Cancer” OR “Oral Neoplasm” OR “Oral Carcinoma” OR “Oral Malignancy” OR “Oral Tumor”) | Search filtered by article type inclusion/exclusion criteria | 332 |
| Wiley Online Library http://onlinelibrary.wiley.com (Accessed on 20 July 2022) | (“Vitamin D” OR “Vitamin D2” OR “Vitamin D3” OR “Calcidiol” OR “Calcitriol” OR “Ergocalciferol” OR “Cholecalciferol” OR “25-hydroxyvitamin D” OR “25(OH)D” OR “Vit D” OR “Vit D2” OR “Vit D3”) AND (“Oral Cancer*” OR “Mouth Cancer*” OR “Oral Neoplasm*” OR “Mouth Neoplasm*” OR “Oral Carcinoma*” OR “Mouth Carcinoma*” OR “Oral Malignancy” OR “Oral malignancies” OR “Mouth Malignancy” OR “Mouth Malignancies” OR “Oral Tumor*” OR “Mouth Tumor*”) | Anywhere | 421 |
| Scopus www.scopus.com (Accessed on 20 July 2022) | ((Adults) OR {Vitamin D2} OR {Vitamin D3} OR {Calcidiol} OR {Calcitriol} OR {Ergocalciferol} OR {Cholecalciferol} OR {25-hydroxyvitamin D} OR {25(OH)D} OR {Vit D} OR {Vit D2} OR {Vit D3}) AND ({Oral Cancer*} OR {Mouth Cancer*} OR {Oral Neoplasm*} OR {Mouth Neoplasm*} OR {Oral Carcinoma*} OR {Mouth Carcinoma*} OR {Oral Malignancy} OR {Oral malignancies} OR {Mouth Malignancy} OR {Mouth Malignancies} OR {Oral Tumor*} OR {Mouth Tumor*}) | No limits | 28 |
| Google Scholar www.scholar.google.com (Accessed on 20 July 2022) | ((Vitamin D) OR (Vitamin D2) OR (Vitamin D3) OR (Calcidiol) OR (Calcitriol) OR (Ergocalciferol) OR (Cholecalciferol) OR (25-hydroxyvitamin D) OR (25(OH)D) OR (Vit D) OR (Vit D2) OR (Vit D3)) AND ((Oral Cancer*) OR (Mouth Cancer*) OR (Oral Neoplasm*) OR (Mouth Neoplasm*) OR (Oral Carcinoma*) OR (Mouth Carcinoma*) OR (Oral Malignancy) OR (Oral malignancies) OR (Mouth Malignancy) OR (Mouth Malignancies) OR (Oral Tumor*) OR (Mouth Tumor*)) | All fields | 13,300—results from first 40 pages were included = 405 |
| Ovid database http://ovidsp.ovid.com/autologin.html (Accessed on 20 July 2022) | ((Vitamin D) OR (Vitamin D2) OR (Vitamin D3) OR (Calcidiol) OR (Calcitriol) OR (Ergocalciferol) OR (Cholecalciferol) OR (25-hydroxyvitamin D) OR (Vit D) OR (Vit D2) OR (Vit D3)) AND ((Oral Cancer*) OR (Mouth Cancer*) OR (Oral Neoplasm*) OR (Mouth Neoplasm*) OR (Oral Carcinoma*) OR (Mouth Carcinoma*) OR (Oral Malignancy) OR (Oral malignancies) OR (Mouth Malignancy) OR (Mouth Malignancies) OR (Oral Tumor*) OR (Mouth Tumor*)) | All fields | 120 |
| ProQuest http://search.proquest.com/ (Accessed on 20 July 2022) | (((Vitamin D) OR (Vitamin D2) OR (Vitamin D3) OR (Calcidiol) OR (Calcitriol) OR (Ergocalciferol) OR (Cholecalciferol) OR (25-hydroxyvitamin D)) AND ((Oral Cancer) OR (Mouth Cancer) OR (Oral Neoplasm) OR (Mouth Neoplasm) OR (Oral Carcinoma) OR (Mouth Carcinoma) OR (Oral Malignancy) OR (Oral Tumor) OR (Mouth Tumor))) | -Abstract -English language | 31 |
| Cochrane Library http://onlinelibrary.wiley.com/cochranelibrary/ (Accessed on 20 July 2022) | “Vitamin D” OR “Vitamin D2” OR “Vitamin D3” OR “Calcidiol” OR “Calcitriol” OR “Ergocalciferol” OR “Cholecalciferol” OR “25-hydroxyvitamin D” OR “25(OH)D” OR “Vit D” OR “Vit D2” OR “Vit D3” AND “Oral Cancer*” OR “Mouth Cancer*” OR “Oral Neoplasm*” OR “Mouth Neoplasm*” OR “Oral Carcinoma*” OR “Mouth Carcinoma*” OR “Oral Malignancy” OR “Oral malignancies” OR “Mouth Malignancy” OR “Mouth Malignancies” OR “Oral Tumor*” OR “Mouth Tumor*” | No limits | 2 |
| Author (Year) | Country | Study Type/Design | Study Population | Results Summary | Category |
|---|---|---|---|---|---|
| Anand at el. (2017) [27] | India | Prospective/Cohort | Total cases: N = 87; 69 male, 18 female; mean age of 43 (32–53) * years | Vitamin D supplementation reduced treatment-related toxicities. | Treatment |
| Controls: N = 95; matched gender; median age of 49 (35–62) years | |||||
| Arem et al. (2011) [28] | Finland | Prospective/Case–control | Total cases: N = 182 male; median age of 57 (53–61) * years | Did not show an association between serum 25(OH)D and risk of head and neck cancers. | Prevention |
| Controls: N = 182 male; 57 (53–61) * | |||||
| Bektas-Kayhan et al. (2010) [29] | Turkey | Prospective/Case–control | Total cases: N = 64; 43 male, 21 female; median age of 55 (42–69) years | VDR Tt genotype was linked to an increased risk of OSCC. | Prevention |
| Controls: N = 87; 45 male, 42 female; median age of 57 (44–70) years | VDR gene influences susceptibility to OSCC. | ||||
| Dudding et al. (2018) [30] | United Kingdom | Retrospective/Cohort | Total cases: N = 5133; 3798 male, 1335 female; age N/A | Found no clinically relevant protective effect of 25OHD on oral cancers; supplementation unlikely to be beneficial/ | Prevention |
| Control: N = 5984; 3882 male, 2102 female; age N/A | |||||
| Giovannucci et al. (2006) [31] | United States | Prospective/Case–control | Total cases: N = 51 males; aged 40–75 years | Investigated the association of multiple determinants of vitamin D exposure to cancer risk and found a statistically significant inverse association. | Prevention |
| Controls: N/A | |||||
| Grimm et al. (2013) [32] | Germany | Retrospective/Case–control | Total cases: N = 191; 145 male, 46 female; ~60 years of age | Low VDR expression is associated with tumor recurrence, and low VDR expression is an independent prognostic factor. | Prevention, Treatment |
| Controls: N = 10; gender N/A; age N/A | |||||
| Grimm et al. (2015) [33] | Germany | Retrospective/Case–control | Total cases: N = 42; 24 male, 18 female; age N/A | Serum vitamin D levels correlated with apoptosis induction of VDR+ cells in oral precancerous lesions; OSCC by natural or synthetic vitamin D compounds could be useful for chemoprevention. | Prevention |
| Controls: N = 5; gender N/A; age N/A | |||||
| Lipworth et al. (2009) [34] | Italy | Prospective/Case–control | Total cases: N = 804 cases; 658 male, 146 female; median age of 58 (22–78) years | Observed inverse associations between dietary vitamin D intake and risk and oral cancer, which were most pronounced among current heavy smokers. | Prevention |
| Controls: N = 743; 593 male, 150 female; median age of 60 (36–77) years | |||||
| Małodobra-Mazur et al. (2012) [35] | Poland | Prospective/Cohort | Total cases: N = 73; 48 male, 25 female; median age of 58 (27–83) years | Provided evidence for the genetic association between the specific VDR gene polymorphism and the occurrence and risk of oral cavity cancer. | Prevention |
| Controls: N = 100 male; age N/A | |||||
| Negri et al. (2000) [36] | Italy | Retrospective/Case–control | Total cases: N = 344; 274 male, 70 female with oral cancer and N = 410; 364 male, 46 female, with pharyngeal cancer; median age of 57 (22–77) years | Dietary vitamin D was inversely associated with oral cancer risk. | Prevention |
| Controls: N = 1.775; 1.254 male, 521 female; median age of 57 (20–78) years | |||||
| Nuszkiewicz et al. (2021) [37] | Poland | Prospective/Case–control | Total cases: N = 45; 29 male, 16 female; median age 57–71 years | Vitamin D deficiency and disturbed oxidant–antioxidant homeostasis are more common in oral cancer patients. | Prevention |
| Controls: N = 25; 11 male, 14 female; median age 55 (54–57) years | |||||
| Udeabor et al. (2020) [38] | Saudi Arabia | Prospective/Case–control | Total cases: N = 51; 22 male, 29 female; median 59 (46–72) years | Found an association between vitamin D deficiency and OSCC risk, especially in levels below 25 ng/mL | Prevention |
| Controls: N = 113; 36 male, 77 female; median age of 49 (33–65) years | |||||
| Young et al. (2015) [39] | United States | Prospective/Clinical trial | Total cases: N = 61; 40 male, 21 female; age range 46–72 years | Treatment with vitamin D in patients with head and neck cancers helped maintain normal immune reactivity. | Treatment |
| Controls: N = 30; 19 male, 11 female; mean age of 59 (48–70) years | |||||
| Zeljic et al. (2012) [40] | Serbia | Prospective/Case–control | Total cases: N = 110; 81 male, 29 female; mean age of ~60 years | Found a significant decrease in oral cancer risk in VDR heterozygote AG of CYP24A1 gene compared with wild-type AA genotype. | Prevention |
| Controls (matched): N = 122 | VDR FokI polymorphism was associated with decreased survival and could be an independent prognostic marker. | ||||
| Zhang et al. (2015) [41] | China | Prospective/Case–control | Total cases: N = 70; 62 male, 8 female; median age 51 (40–63) years | Serum vitamin D was not significantly different between the OSCC cases and the controls. | Prevention |
| Controls: N = 70; 62 male, 8 female; median age 53 (42–64) years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, M.; Almpani, K.; Thao, B.; Sudweeks, K.; Lipsky, M.S. Vitamin D in the Prevention and Treatment of Oral Cancer: A Scoping Review. Nutrients 2023, 15, 2346. https://doi.org/10.3390/nu15102346
Hung M, Almpani K, Thao B, Sudweeks K, Lipsky MS. Vitamin D in the Prevention and Treatment of Oral Cancer: A Scoping Review. Nutrients. 2023; 15(10):2346. https://doi.org/10.3390/nu15102346
Chicago/Turabian StyleHung, Man, Konstantinia Almpani, Bao Thao, Kaili Sudweeks, and Martin S. Lipsky. 2023. "Vitamin D in the Prevention and Treatment of Oral Cancer: A Scoping Review" Nutrients 15, no. 10: 2346. https://doi.org/10.3390/nu15102346
APA StyleHung, M., Almpani, K., Thao, B., Sudweeks, K., & Lipsky, M. S. (2023). Vitamin D in the Prevention and Treatment of Oral Cancer: A Scoping Review. Nutrients, 15(10), 2346. https://doi.org/10.3390/nu15102346