
Effects of a Theory-Based, Multicomponent eHealth Intervention for Obesity Prevention in Young Children from Low-Income Families: A Pilot Randomized Controlled Study



Abstract
1. Introduction
2. Materials and Methods
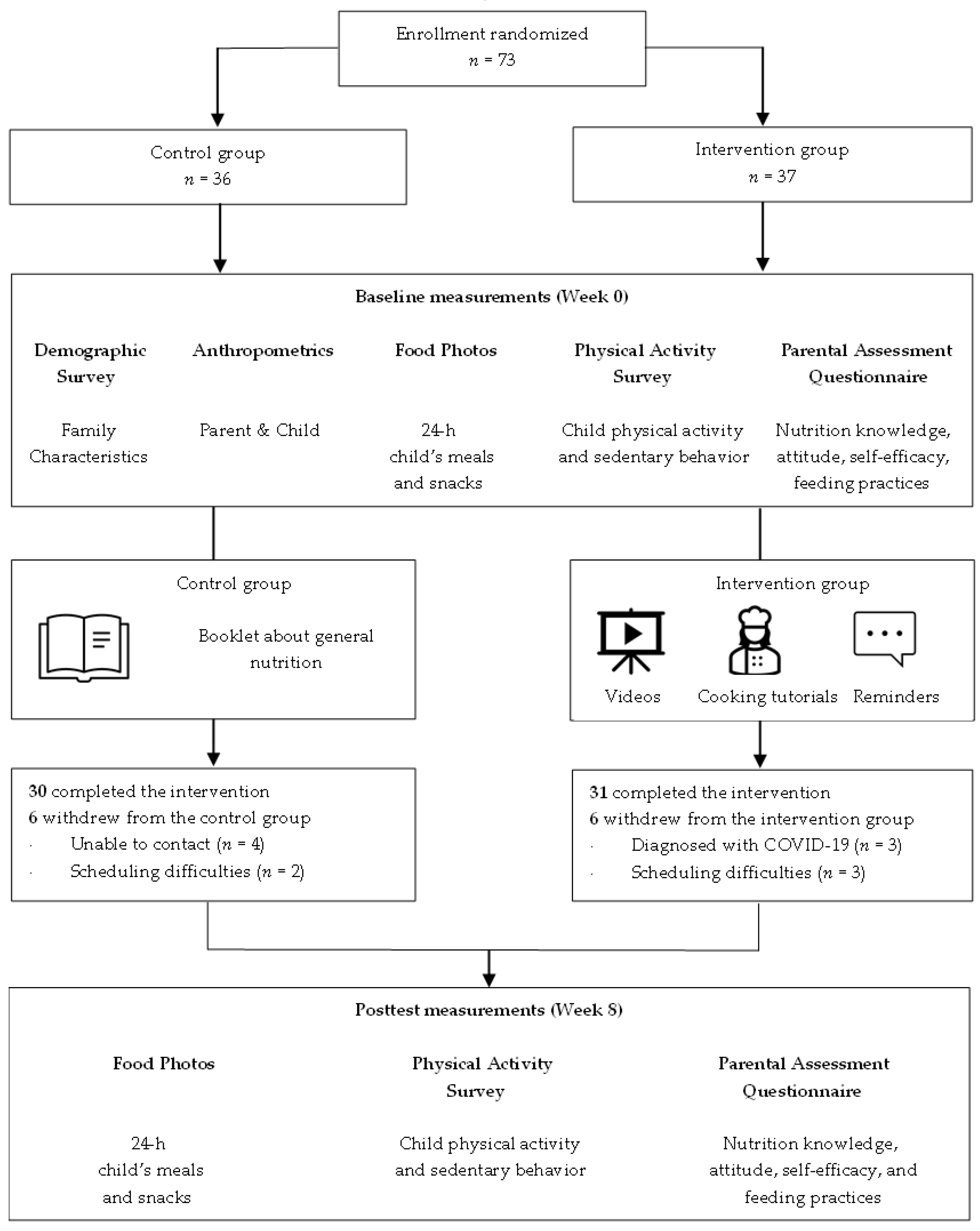
2.1. Research Design
2.2. Participants
2.3. Intervention Methods
2.4. Survey Items
2.4.1. Primary Evaluation Items
2.4.2. Secondary Evaluation Items
2.5. Statistical Analysis
3. Results
3.1. Background Characteristics
3.2. Results of Child Eating and Physical Activity Behaviors
3.3. Results of Parental Psychosocial Attributes and Feeding Practices
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Childhood Obesity Facts—Prevalence of Childhood Obesity in the United States. Available online: https://www.cdc.gov/obesity/data/childhood.html (accessed on 6 April 2023).
- Weaver, R.G.; Brazendale, K.; Hunt, E.; Sarzynski, M.A.; Beets, M.W.; White, K. Disparities in childhood overweight and obesity by income in the United States: An epidemiological examination using three nationally representative datasets. Int. J. Obes. 2019, 43, 1210–1222. [Google Scholar] [CrossRef]
- Yusuf, Z.I.; Dongarwar, D.; Yusuf, R.A.; Bell, M.; Harris, T.; Salihu, H.M. Social determinants of overweight and obesity among children in the United States. Int. J. Matern. Child AIDS 2020, 9, 22–33. [Google Scholar] [CrossRef]
- Huffman, F.G.; Kanikireddy, S.; Patel, M. Parenthood—A contributing factor to childhood obesity. Int. J. Env. Environ. Res. Public Health 2010, 7, 2800–2810. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Davison, K.K.; Birch, L.L. Childhood overweight: A contextual model and recommendations for future research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef]
- Hodder, R.K.; Stacey, F.G.; Wyse, R.J.; O’Brien, K.M.; Clinton-McHarg, T.; Tzelepis, F.; Nathan, N.K.; James, E.L.; Bartlem, K.M.; Sutherland, R.; et al. Interventions for increasing fruit and vegetable consumption in children aged five years and under. Cochrane Database Syst. Rev. 2017, 9, CD008552. [Google Scholar] [CrossRef]
- Stevens, J.; Kelleher, K.J.; Ward-Estes, J.; Hayes, J. Perceived barriers to treatment and psychotherapy attendance in child community mental health centers. Community Ment. Health J. 2016, 42, 449–458. [Google Scholar] [CrossRef]
- Spoth, R.; Redmond, C. Research on family engagement in preventive interventions: Toward improved use of scientific findings in primary prevention practice. J. Prim. Prev. 2000, 21, 267–284. [Google Scholar] [CrossRef]
- Kazdin, A.E.; Holland, L.; Crowley, M. Family experience of barriers to treatment and premature termination from child therapy. J. Consult. Clin. Psychol. 1997, 65, 453–463. [Google Scholar] [CrossRef]
- Zhen-Duan, J.; Engebretsen, B.; Laroche, H.H. Diet and physical activity changes among low-income families: Perspectives of mothers and their children. Int. J. Qual. Stud. Health Well-Being 2019, 14, 1. [Google Scholar] [CrossRef]
- Knowlden, A.; Sharma, M. One-year efficacy testing of enabling mothers to prevent pediatric obesity through web-based education and reciprocal determinism (EMPOWER) randomized control trial. Health Educ. Behav. 2016, 43, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Bakırcı-Taylor, A.L.; Reed, D.B.; McCool, B.; Dawson, J.A. mHealth Improved fruit and vegetable accessibility and intake in young children. J. Nutr. Educ. Behav. 2019, 51, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Luque, V.; Escribano, J.; Closa-Monasterolo, R.; Zaragoza-Jordana, M.; Ferré, N.; Grote, V.; Koletzko, B.; Totzauer, M.; Verduci, E.; ReDionigi, A.; et al. Unhealthy dietary patterns established in infancy track to mid-childhood: The EU childhood obesity project. J. Nutr. 2018, 148, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting styles, feeding styles, feeding practices, and weight status in 4–12 year-old children: A systematic review of the literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef]
- Blissett, J.; Haycraft, E.; Farrow, C. Inducing preschool children’s emotional eating: Relations with parental feeding practices. Am. J. Clin. Nutr. 2010, 92, 359–365. [Google Scholar] [CrossRef]
- Wolfenden, L.; Kypri, K.; Freund, M.; Hodder, R. Obtaining active parental consent for school-based research: A guide for researchers. Aust. N. Z. J. Public. Health 2009, 33, 270–275. [Google Scholar] [CrossRef]
- Enright, G.; Allman-Farinelli, M.; Redfern, J. Effectiveness of family-based behavior change interventions on obesity-related behavior change in children: A realist synthesis. Int. J. Env. Environ. Res. Public. Health 2020, 17, 4099. [Google Scholar] [CrossRef]
- Locke, E.A.; Latham, G.P. Building a practically useful theory of goal setting and task motivation. A 35-year odyssey. Am. Psychol. 2002, 57, 705–717. [Google Scholar] [CrossRef]
- Doran, G.T. There’s a S.M.A.R.T. way to write managements’s goals and objectives. Manag. Rev. 1981, 70, 35–36. [Google Scholar]
- Goulão, M.F.; Menedez, R.C. Learner Autonomy and self-regulation in eLearning. Procedia Soc. 2015, 174, 1900–1907. [Google Scholar] [CrossRef]
- Frid, H.; Adolfsson, E.T.; Rosenblad, A.; Nydahl, M. Agreement between different methods of measuring height in elderly patients. J. Hum. Nutr. Diet. 2013, 26, 504–511. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey: Anthropometry Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2017-2018/manuals/2017_Anthropometry_Procedures_Manual.pdf (accessed on 6 April 2023).
- Centers for Disease Control and Prevention. Measuring Children’s Height and Weight Accurately at Home. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/measuring_children.html (accessed on 6 April 2023).
- Grummer-Strawn, L.M.; Reinold, C.; Krebs, N.F.; Centers for Disease Control and Prevention (CDC). Use of world health organization and CDC growth charts for children aged 0–59 months in the United States. MMWR. Recommendations and reports: Morbidity and mortality weekly report. Recomm. Rep. 2010, 59, 1–15. Available online: https://www.cdc.gov/mmwr/pdf/rr/rr5909.pdf (accessed on 5 May 2023).
- Centers for Disease Control and Prevention. BMI Percentile Calculator for Child and Teen. 2021. Available online: https://www.cdc.gov/healthyweight/bmi/calculator.html (accessed on 5 May 2023).
- De Onis, M.; Lobstein, T. Defining obesity risk status in the general childhood population: Which cut-offs should we use? Int. J. Pediatr. Obes. 2010, 5, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Bingham, D.D.; Collings, P.J.; Clemes, S.A.; Costa, S.; Santorelli, G.; Griffiths, P.; Barber, S.E. Reliability and validity of the early years physical activity questionnaire (EY-PAQ). Sports 2016, 4, 30. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Agriculture; United States Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; US Government Publishing Office: Washington, DC, USA, 2020. Available online: https://www.dietaryguidelines.gov/ (accessed on 6 April 2023).
- United States Department of Health and Human Services. Physical Activity Guidelines for Americans Midcourse Report: Strategies to Increase Physical Activity among Youth 2012. Available online: https://health.gov/sites/default/files/2019-09/pag-mid-course-report-final.pdf (accessed on 6 April 2023).
- Wilson, A.; Magarey, A.; Mastersson, N. Reliability of questionnaires to assess the healthy eating and activity environment of a child’s home and school. J. Obes. 2013, 2013, 720368. [Google Scholar] [CrossRef]
- Horodynski, M.A.; Stommel, M. Nutrition education aimed at toddlers: An intervention study. Pediatr. Nurs. 2005, 31, 364–372. [Google Scholar]
- Musher-Eizenman, D.; Holub, S. Comprehensive feeding practices questionnaire: Validation of a new measure of parental feeding practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef] [PubMed]
- Hunsaker, S.L.; Jensen, C.D. Effectiveness of a parent health report in increasing fruit and vegetable consumption among preschoolers and kindergarteners. J. Nutr. Educ. Behav. 2017, 49, 380–386. [Google Scholar] [CrossRef]
- Ling, J.; Robbins, L.B.; Zhang, N.; Kerver, J.M.; Lyons, H.; Wieber, N.; Zhang, M. Using facebook in a healthy lifestyle intervention: Feasibility and preliminary efficacy. West. J. Nurs. Res. 2018, 40, 1818–1842. [Google Scholar] [CrossRef]
- Skouteris, H.; Hill, B.; McCabe, M.; Swinburn, B.; Busija, L. A parent-based intervention to promote healthy eating and active behaviours in pre-school children: Evaluation of the MEND 2-4 randomized controlled trial. Pediatr. Obes. 2016, 11, 4–10. [Google Scholar] [CrossRef]
- Ha, A.; Lonsdale, C.; Lubans, D.; Ng, F.; Ng, J. Improving children’s fundamental movement skills through a family-based physical activity program: Results from the “Active 1 + FUN” randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–99. [Google Scholar] [CrossRef]
- Pate, R.R.; Brown, W.H.; Pfeiffer, K.A.; Howie, E.K.; Saunders, R.P.; Addy, C.L.; Dowda, M. An intervention to increase physical activity in children: A randomized controlled trial with 4-year-olds in preschools. Am. J. Prev. Med. 2016, 51, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Downing, K.L.; Hnatiuk, J.A.; Hinkley, T.; Salmon, J.; Hesketh, K.D. Interventions to reduce sedentary behaviour in 0–5-year-olds: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sport. Med. 2018, 52, 314–321. [Google Scholar] [CrossRef]
- Barnett, T.A.; Kelly, A.S.; Young, D.R.; Perry, C.K.; Pratt, C.A.; Edwards, N.M.; Rao, G.; Vos, M.B.; American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; et al. Sedentary behaviors in today’s youth: Approaches to the prevention and management of childhood obesity: A Scientific Statement From the American Heart Association. Circulation 2018, 138, 142–159. [Google Scholar] [CrossRef] [PubMed]
- De Lepeleere, S.; De Bourdeaudhuij, I.; Cardon, G.; Verloigne, M. The effect of an online video intervention ‘Movie Models’ on specific parenting practices and parental self-efficacy related to children’s physical activity, screen-time and healthy diet: A quasi experimental study. BMC Public Health 2017, 17, 366. [Google Scholar] [CrossRef] [PubMed]
- Möhler, R.; Wartha, O.; Steinacker, J.M.; Szagun, B.; Kobel, S. Parental self-Efficacy as a predictor of children’s nutrition and the potential mediator effect between the health promotion program “join the healthy boat” and children’s nutrition. Int. J. Env. Environ.Res. Public Health 2020, 17, 9463. [Google Scholar] [CrossRef] [PubMed]
- Hammersley, M.L.; Okely, A.D.; Batterham, M.J.; Jones, R.A. An internet-based childhood obesity prevention program (Time2bHealthy) for parents of preschool-aged children: Randomized controlled trial. J. Med. Internet Res. 2019, 21, 11964. [Google Scholar] [CrossRef]
- Essery, E.V.; DiMarco, N.M.; Rich, S.S.; Nichols, D.L. Mothers of preschoolers report using less pressure in child feeding situations following a newsletter intervention. J. Nutr. Educ. Behav. 2008, 40, 110–115. [Google Scholar] [CrossRef]
- Harvey-Berino, J.; Rourke, J. Obesity prevention in preschool native-american children: A pilot study using home visiting. Obes. Res. 2003, 11, 606–611. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Session | Topic | Activity |
|---|---|---|
| 1 | What Does Healthy Eating Look Like for Children | |
| Introduction; food groups using MyPlate; trends and consequences of childhood obesity; portion sizes | Setting SMART goal | |
| 2 | Why Children Should Eat More Fruit | |
| Recommended fruit intake; health benefits of eating various fruit; tips on introducing new fruits to toddlers | Making healthy snacks using fruits | |
| 3 | Listening to Your Child’ Needs | |
| Importance of using responsive feeding practices; impact of growth and psychosocial development on child appetite; neophobia or rejection of foods | Preparing child meals using ‘My ChildPlate’ | |
| 4 | How to Practice Responsive Feeding | |
| Emotional, pressure, and restriction feeding practices; negative consequences of such practices in children; tips on shifting non-responsive to responsive feeding practices | Journaling on current feeding practices | |
| 5 | Vegetable Goals for Young Children | |
| Recommended vegetable intake; health benefits of eating adequate and various vegetables; tips on increasing vegetable intake at home; importance of parent modeling in eating vegetables | Making veggie stuffed pepper cups | |
| 6 | Active and Healthy Child | |
| Physical activity and screen viewing guidelines for toddlers; examples and strategies for increasing physical activity at home without equipment | Identifying negative consequences of child screen time | |
| 7 | Eating on A Budget | |
| Tips to shop on a budget for fruit and vegetables (both perishable and non-perishable items); importance of meal planning; utilizing leftovers | Making healthy tortilla pizza | |
| 8 | Informed Shopper | |
| Elements on food labels; health claims; serving size; what and how to read food labels | Reading food labels | |
| Characteristic | Full Sample | Intervention Group | Control Group | p-Value |
|---|---|---|---|---|
| Age (months) | 26.52 8.48 | 25.54 8.67 | 27.53 8.28 | 0.26 |
| Gender | 0.58 | |||
| Female | 41 (56.2%) | 19 (51.4%) | 13 (36.1%) | |
| Male | 32 (43.8%) | 18 (48.7%) | 23 (63.9%) | |
| Race | 0.48 | |||
| Biracial | 27 (36.9%) | 14 (37.8%) | 13 (36.1%) | |
| Hispanic | 17 (23.3%) | 10 (27.0%) | 6 (16.7%) | |
| Non-Hispanic White | 16 (21.9%) | 6 (16.2%) | 11 (30.6%) | |
| Black | 12 (16.4%) | 7 (18.9%) | 5 (13.9%) | |
| Native Hawaiian and other Pacific Islander | 1 (1.4%) | 0 | 1 (2.8%) | |
| BMI-for-age z score | 0.87 1.65 | 1.03 1.88 | 0.71 1.41 | 0.504 |
| Weight status | 0.50 | |||
| Healthy weight | 41 (56.2%) | 24 (64.9%) | 17 (47.2%) | |
| Obesity | 16 (21.9%) | 7 (18.9%) | 9 (25.0%) | |
| Overweight | 10 (13.7%) | 4 (10.8%) | 6 (16.7%) | |
| Underweight | 6 (8.2%) | 2 (5.4%) | 4 (11.1%) | |
| Relationship with child | 0.83 | |||
| Mother | 62 (84.9%) | 32 (86.5%) | 30 (83.3%) | |
| Father | 6 (8.2%) | 2 (5.4%) | 4 (11.1%) | |
| Foster mother | 4 (5.5%) | 2 (5.4%) | 2 (5.6%) | |
| Grandmother | 1 (1.4%) | 1 (2.7%) | 0 | |
| Parental educational attainment | 0.21 | |||
| High school | 22 (30.1%) | 14 (37.8%) | 8 (2.2%) | |
| One year of college | 13 (17.8%) | 6 (16.2%) | 7 (19.4%) | |
| Bachelor’s degree or equivalent | 10 (13.7%) | 6 (16.2%) | 3 (8.3%) | |
| Two years of college | 9 (12.3%) | 5 (13.5%) | 4 (11.1%) | |
| Some high school | 9 (12.3%) | 4 (10.8%) | 6 (16.7%) | |
| Three years of college | 5 (6.8%) | 2 (5.4%) | 3 (8.3%) | |
| Master’s degree | 5 (6.8%) | 0 | 5 (13.9%) | |
| Parental marital status | 0.47 | |||
| Never married | 36 (49.3%) | 19 (51.4%) | 17 (47.2%) | |
| Married | 25 (34.2%) | 14 (37.8%) | 11 (30.6%) | |
| Divorced | 7 (9.6%) | 2 (5.4%) | 5 (13.9%) | |
| Separated | 3 (4.1%) | 2 (5.4%) | 1 (2.8%) | |
| Engaged | 2 (2.7%) | 0 | 2 (5.6%) | |
| Yearly income ($) | 26,436.97 17,524.52 | 26,113.43 17,536.31 | 26,808.44 17,837.48 | 0.94 |
| Household income level | 0.91 | |||
| Very low income | 41 (56.1%) | 21 (56.8%) | 20 (5.6%) | |
| Low income | 10 (13.7%) | 6 (16.2%) | 4 (11.1%) | |
| Non-low income | 4 (5.5%) | 1 (2.7%) | 3 (8.3%) | |
| Not specify | 18 (24.7%) | 9 (24.3%) | 9 (25.0%) | |
| Parental BMI | 31.71 ± 8.34 | 29.95 ± 8.35 | 33.43 ± 8.07 | 0.03 |
| Parental weight status | 0.20 | |||
| Obesity | 34 (46.6%) | 21 (56.8%) | 13 (36.1%) | |
| Overweight | 25 (34.2%) | 11 (29.7%) | 14 (38.9%) | |
| Healthy weight | 14 (19.2%) | 5 (13.5%) | 9 (25.0%) |
| Variable | Control Group (n = 36) | Intervention Group (n = 37) | Between Groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline M [SD] | Posttest M [SD] | Change Score M [SD] | t [df] | p-Value | BaselineM [SD] | Posttest M [SD] | Change Score M [SD] | t [df] | p-Value | Change Score M [SD] | t [df] | p-Value | |
| Fruit intake (servings) | 0.47 [0.62] | 0.46 [0.75] | −0.016 [0.88] | −0.11 [21.54] | 0.92 | 0.57 [0.48] | 1.47 [0.54] | 0.91 [0.62] | 8.89 [30.31] | 6 × 10−10 | 0.89 [1.93] | 3.96 [24.69] | 0.00057 |
| Vegetable intake (servings) | 0.44 [0.47] | 0.27 [0.66] | −0.17 [0.74] | −1.40 [22.58] | 0.17 | 0.45 [0.52] | 0.98 [0.71] | 0.54 [0.69] | 4.74 [29.39] | 5 × 10−5 | 0.60 [1.64] | 3.10 [36.13] | 0.0037 |
| MVPA (minutes) | 61.23 [38.13] | 55.58 [39.00] | −5.65 [39.29] | −0.86 [23.88] | 0.4 | 59.79 [25.22] | 69.07 [29.01] | 9.28 [27.15] | 2.08 [27.23] | 0.047 | 10.13 [81.45] | 1.06 [22.52] | 0.29 |
| Sedentary behavior (minutes) | 208.38 [72.56] | 238.15 [93.21] | 29.78 [97.59] | 1.83 [21.66] | 0.08 | 238.33 [86.98] | 194.96 [74.92] | −43.38 [61.79] | −4.27 [30.34] | 0.00018 | −44.89 [191.86] | −2.00 [32.26] | 0.054 |
| Screen time (minutes) | 68.31 [48.58] | 89.45 [63.98] | 21.14 [49.12] | 2.58 [23.38] | 0.017 | 73.25 [34.74] | 45.78 [33.34] | −27.47 [30.87] | −5.41 [30.15] | 7 × 10−6 | −33.87 [121.67] | −2.37 [23.05] | 0.026 |
| Variable | Control Group (n = 36) | Intervention Group (n = 37) | Between Groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline M [SD] | Posttest M [SD] | Change Score M [SD] | t [df] | p-Value | Baseline M [SD] | Posttest M [SD] | Change Score M [SD] | t [df] | p-Value | Change Score M [SD] | t [df] | p-Value | |
| Nutrition knowledge | 11.11 [1.74] | 10.34 [2.58] | −0.77 [2.62] | −1.76 [22.13] | 0.093 | 10.89 [1.71] | 11.49 [2.50] | 0.60 [2.33] | 1.57 [30.43] | 0.13 | 0.92 [6.37] | 1.23 [29.99] | 0.23 |
| Attitude | 34.08 [6.83] | 33.18 [8.24] | −0.90 [6.63] | −0.82 [26.38] | 0.42 | 33.51 [5.65] | 36.20 [7.31] | 2.68 [5.94] | 2.74 [29.20] | 0.01 | 2.68 [16.14] | 1.42 [32.78] | 0.17 |
| Self-efficacy | 25.25 [5.16] | 24.19 [5.94] | −1.06 [5.08] | −1.25 [21.83] | 0.22 | 22.78 [5.02] | 27.35 [5.01] | 4.57 [4.66] | 5.96 [31.04] | 1 × 10−6 | 4.42 [12.94] | 2.92 [28.57] | 0.0068 |
| CFP | 132.19 [15.71] | 120.70 [17.99] | −11.50 [15.45] | −4.46 [21.87] | 0.002 | 123.19 [21.39] | 132.09 [18.07] | 8.90 [20.23] | 2.68 [30.30] | 0.012 | 13.69 [40.89] | 2.85 [37.46] | 0.0069 |
| Variable | Control Group (n = 36) | Intervention Group (n = 37) | Between Groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline M [SD] | Posttest M [SD] | Change Score M [SD] | t [df] | p-Value | Baseline M [SD] | Posttest M [SD] | Change Score M [SD] | t [df] | p-Value | Change Score M [SD] | t [df] | p-Value | |
| Responsive Feeding Practices | |||||||||||||
| Encouragement | 13.86 [2.29] | 13.79 [2.92] | −0.072 [2.24] | −0.19 [27.07] | 0.84 | 13.24 [2.36] | 15.20 [2.26] | 1.95 [2.56] | 4.63 [31.24] | 6 × 10−5 | 0.98 [5.98] | 1.39 [32.44] | 0.17 |
| Environment | 10.50 [3.20] | 10.65 [3.71] | 0.15 [2.89] | 0.30 [22.48] | 0.76 | 10.43 [3.45] | 11.53 [4.11] | 1.10 [4.34] | 1.54 [31.38] | 0.13 | 1.18 [9.31] | 1.08 [27.67] | 0.29 |
| Involvement | 7.69 [2.95] | 7.13 [3.59] | −0.56 [2.71] | −1.25 [26.70] | 0.22 | 6.27 [3.20] | 9.35 [3.45] | 3.08 [3.61] | 5.19 [27.20] | 2 × 10−5 | 2.16 [10.51] | 1.75 [19.04] | 0.096 |
| Modeling | 12.92 [4.03] | 12.44 [5.20] | −0.48 [3.31] | −0.86 [17.26] | 0.41 | 11.89 [3.44] | 13.76 [3.04] | 1.87 [2.39] | 4.75 [29.37] | 5 × 10−5 | 1.61 [6.60] | 2.09 [41.99] | 0.043 |
| Monitoring | 11.08 [4.20] | 12.61 [5.44] | 1.53 [5.28] | 1.74 [22.74] | 0.096 | 11.24 [4.41] | 12.10 [4.10] | 0.85 [4.95] | 1.05 [32.06] | 0.30 | −0.77 [11.04] | −0.60 [31.94] | 0.56 |
| Non-Responsive Feeding Practices | |||||||||||||
| Child control | 11.39 [3.56] | 10.11 [4.14] | −1.28 [3.76] | −2.04 [27.46] | 0.051 | 10.05 [2.86] | 10.60 [4.37] | 0.54 [3.86] | 0.85 [25.25] | 0.4 | 1.20 [9.47] | 1.08 [33.04] | 0.29 |
| Emotion regulation | 8.31 [2.54] | 8.80 [3.19] | 0.49 [2.95] | 1.00 [20.54] | 0.33 | 8.00 [2.33] | 9.17 [2.41] | 1.17 [2.64] | 2.69 [30.43] | 0.012 | 0.84 [6.21] | 1.16 [27.28] | 0.26 |
| Food as reward | 8.14 [2.50] | 7.12 [4.28] | −1.01 [4.22] | −1.44 [22.03] | 0.16 | 7.32 [2.84] | 9.29 [3.17] | 1.96 [3.28] | 3.65 [23.42] | 0.0013 | 2.23 [10.25] | 1.86 [24.05] | 0.075 |
| Pressure to eat | 7.44 [3.74] | 6.40 [4.60] | −1.04 [4.94] | −1.27 [24.54] | 0.22 | 7.19 [3.82] | 9.09 [3.41] | 1.90 [3.36] | 3.45 [31.99] | 0.0016 | 2.51 [11.80] | 1.82 [21.84] | 0.083 |
| Restriction for health | 6.89 [3.98] | 6.05 [4.87] | −0.84 [4.07] | −1.24 [21.78] | 0.23 | 6.57 [2.52] | 7.71 [4.24] | 1.14 [3.53] | 1.96 [27.85] | 0.06 | 1.98 [9.44] | 1.79 [31.17] | 0.083 |
| Restriction for weight | 26.53 [4.08] | 25.70 [5.72] | −0.82 [5.08] | −0.97 [20.20] | 0.34 | 23.78 [4.81] | 26.73 [6.55] | 2.95 [4.61] | 3.89 [29.61] | 0.00053 | 2.16 [13.39] | 1.38 [26.02] | 0.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Oldewage-Theron, W.; Dawson, J.A. Effects of a Theory-Based, Multicomponent eHealth Intervention for Obesity Prevention in Young Children from Low-Income Families: A Pilot Randomized Controlled Study. Nutrients 2023, 15, 2296. https://doi.org/10.3390/nu15102296
Lee H, Oldewage-Theron W, Dawson JA. Effects of a Theory-Based, Multicomponent eHealth Intervention for Obesity Prevention in Young Children from Low-Income Families: A Pilot Randomized Controlled Study. Nutrients. 2023; 15(10):2296. https://doi.org/10.3390/nu15102296
Chicago/Turabian StyleLee, Hyunjung, Wilna Oldewage-Theron, and John A. Dawson. 2023. "Effects of a Theory-Based, Multicomponent eHealth Intervention for Obesity Prevention in Young Children from Low-Income Families: A Pilot Randomized Controlled Study" Nutrients 15, no. 10: 2296. https://doi.org/10.3390/nu15102296
APA StyleLee, H., Oldewage-Theron, W., & Dawson, J. A. (2023). Effects of a Theory-Based, Multicomponent eHealth Intervention for Obesity Prevention in Young Children from Low-Income Families: A Pilot Randomized Controlled Study. Nutrients, 15(10), 2296. https://doi.org/10.3390/nu15102296