


Obesity Risk of Pediatric Central Nervous System Tumor Survivors: A Cross-Sectional Study
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
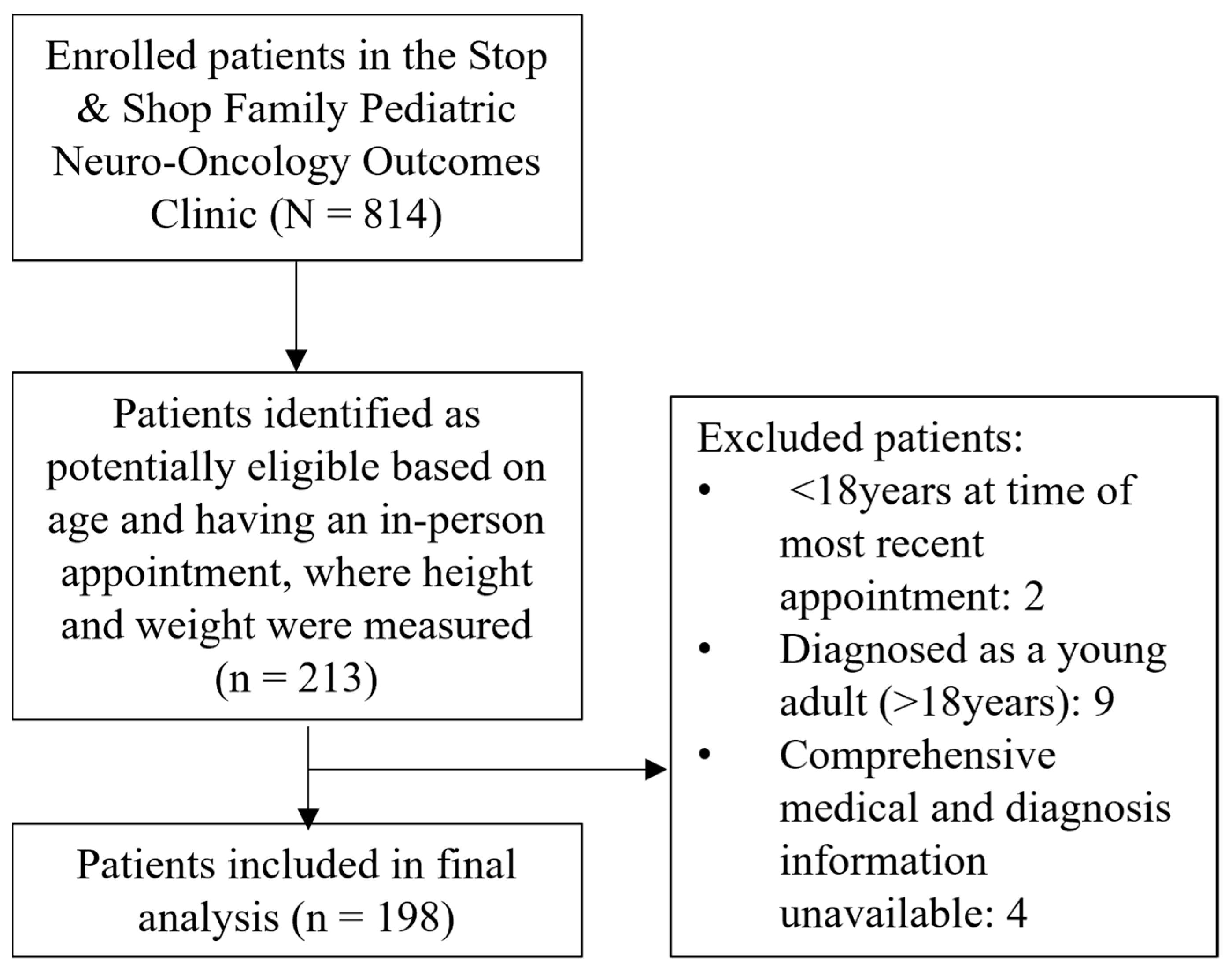
2.1. Study Design and Population
2.2. Data Collection
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Risk of Overweight and Obesity at Follow-Up
3.3. Underweight at Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Cancer Institute Surveillance Research Program. Cancer Stat Facts: Childhood Brain and Other Nervous System Cancer (Ages 0–19). 2022. Available online: https://seer.cancer.gov/statfacts/html/childbrain.html (accessed on 21 January 2023).
- Mertens, A.C.; Yasui, Y.; Neglia, J.P.; Potter, J.D.; Nesbit, M.E., Jr.; Ruccione, K.; Smithson, W.A.; Robison, L.L. Late mortality experience in five-year survivors of childhood and adolescent cancer: The Childhood Cancer Survivor Study. J. Clin. Oncol. 2001, 19, 3163–3172. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.J.; Little, M.P.; Winter, D.L.; Sugden, E.; Ellison, D.W.; Stiller, C.A.; Stovall, M.; Frobisher, C.; Lancashire, E.R.; Reulen, R.C.; et al. Population-based risks of CNS tumors in survivors of childhood cancer: The British Childhood Cancer Survivor Study. J. Clin. Oncol. 2010, 28, 5287–5293. [Google Scholar] [CrossRef] [PubMed]
- Dama, E.; Pastore, G.; Mosso, M.L.; Ferrante, D.; Maule, M.M.; Magnani, C.; Merletti, F. Late deaths among five-year survivors of childhood cancer. A population-based study in Piedmont Region, Italy. Haematologica 2006, 91, 1084–1091. [Google Scholar] [PubMed]
- Armstrong, G.T.; Liu, Q.; Yasui, Y.; Huang, S.; Ness, K.K.; Leisenring, W.; Hudson, M.M.; Donaldson, S.S.; King, A.A.; Stovall, M.; et al. Long-term outcomes among adult survivors of childhood central nervous system malignancies in the Childhood Cancer Survivor Study. J. Natl. Cancer Inst. 2009, 101, 946–958. [Google Scholar] [CrossRef]
- Stavinoha, P.L.; Askins, M.A.; Powell, S.K.; Pillay Smiley, N.; Robert, R.S. Neurocognitive and Psychosocial Outcomes in Pediatric Brain Tumor Survivors. Bioengineering 2018, 5, 73. [Google Scholar] [CrossRef]
- Warner, E.L.; Fluchel, M.; Wright, J.; Sweeney, C.; Boucher, K.M.; Fraser, A.; Smith, K.R.; Stroup, A.M.; Kinney, A.Y.; Kirchhoff, A.C. A population-based study of childhood cancer survivors’ body mass index. J. Cancer Epidemiol. 2014, 2014, 531958. [Google Scholar] [CrossRef]
- Meacham, L.R.; Gurney, J.G.; Mertens, A.C.; Ness, K.K.; Sklar, C.A.; Robison, L.L.; Oeffinger, K.C. Body mass index in long-term adult survivors of childhood cancer: A report of the Childhood Cancer Survivor Study. Cancer 2005, 103, 1730–1739. [Google Scholar] [CrossRef]
- van Schaik, J.; van Roessel, I.; Schouten-van Meeteren, N.; van Iersel, L.; Clement, S.C.; Boot, A.M.; Claahsen-van der Grinten, H.L.; Fiocco, M.; Janssens, G.O.; van Vuurden, D.G.; et al. High Prevalence of Weight Gain in Childhood Brain Tumor Survivors and Its Association With Hypothalamic-Pituitary Dysfunction. J. Clin. Oncol. 2021, 39, 1264–1273. [Google Scholar] [CrossRef]
- Moke, D.J.; Hamilton, A.S.; Chehab, L.; Deapen, D.; Freyer, D.R. Obesity and Risk for Second Malignant Neoplasms in Childhood Cancer Survivors: A Case-Control Study Utilizing the California Cancer Registry. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1612–1620. [Google Scholar] [CrossRef]
- Co-Reyes, E.; Li, R.; Huh, W.; Chandra, J. Malnutrition and obesity in pediatric oncology patients: Causes, consequences, and interventions. Pediatr. Blood Cancer 2012, 59, 1160–1167. [Google Scholar] [CrossRef]
- Brouwer, C.A.; Gietema, J.A.; Kamps, W.A.; de Vries, E.G.; Postma, A. Changes in body composition after childhood cancer treatment: Impact on future health status—A review. Crit. Rev. Oncol./Hematol. 2007, 63, 32–46. [Google Scholar] [CrossRef] [PubMed]
- Iniesta, R.R.; Paciarotti, I.; Brougham, M.F.; McKenzie, J.M.; Wilson, D.C. Effects of pediatric cancer and its treatment on nutritional status: A systematic review. Nutr. Rev. 2015, 73, 276–295. [Google Scholar] [CrossRef] [PubMed]
- Müller, H.L.; Emser, A.; Faldum, A.; Bruhnken, G.; Etavard-Gorris, N.; Gebhardt, U.; Oeverink, R.; Kolb, R.; Sörensen, N. Longitudinal study on growth and body mass index before and after diagnosis of childhood craniopharyngioma. J. Clin. Endocrinol. Metab. 2004, 89, 3298–3305. [Google Scholar] [CrossRef] [PubMed]
- Children’s Oncology Group. Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers. Version 5.0; Children’s Oncology Group: Monrovia, CA, USA, 2018; Available online: http://www.survivor-shipguidelines.org/ (accessed on 21 January 2023).
- Ellison-Barnes, A.; Johnson, S.; Gudzune, K. Trends in Obesity Prevalence Among Adults Aged 18 through 25 Years, 1976–2018. JAMA 2021, 326, 2073–2074. [Google Scholar] [CrossRef] [PubMed]
- Prasad, M.; Arora, B.; Chinnaswamy, G.; Vora, T.; Narula, G.; Banavali, S.; Kurkure, P. Nutritional status in survivors of childhood cancer: Experience from Tata Memorial Hospital, Mumbai. Indian J. Cancer 2015, 52, 219–223. [Google Scholar] [CrossRef]
- Hudson, M.M.; Oeffinger, K.C.; Jones, K.; Brinkman, T.M.; Krull, K.R.; Mulrooney, D.A.; Mertens, A.; Castellino, S.M.; Casillas, J.; Gurney, J.G.; et al. Age-dependent changes in health status in the Childhood Cancer Survivor cohort. J. Clin. Oncol. 2015, 33, 479–491. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Defining Adult Overweight & Obesity. 2022. Available online: https://www.cdc.gov/obesity/basics/adult-defining.html (accessed on 21 January 2023).
- The Global BMI Mortality Collaboration; Di Angelantonio, E.; Bhupathiraju, S.N.; Wormser, D.; Gao, P.; Kaptoge, S.; Berrington de Gonzalez, A.; Cairns, B.J.; Huxley, R.; Jackson, C.L.; et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 2016, 388, 776–786. [Google Scholar] [CrossRef]
- Wilson, C.L.; Liu, W.; Yang, J.J.; Kang, G.; Ojha, R.P.; Neale, G.A.; Srivastava, D.K.; Gurney, J.G.; Hudson, M.M.; Robison, L.L.; et al. Genetic and clinical factors associated with obesity among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort. Cancer 2015, 121, 2262–2270. [Google Scholar] [CrossRef]
- Lustig, R.H.; Post, S.R.; Srivannaboon, K.; Rose, S.R.; Danish, R.K.; Burghen, G.A.; Xiong, X.; Wu, S.; Merchant, T.E. Risk factors for the development of obesity in children surviving brain tumors. J. Clin. Endocrinol. Metab. 2003, 88, 611–616. [Google Scholar] [CrossRef]
- Gurney, J.G.; Kadan-Lottick, N.S.; Packer, R.J.; Neglia, J.P.; Sklar, C.A.; Punyko, J.A.; Stovall, M.; Yasui, Y.; Nicholson, H.S.; Wolden, S.; et al. Endocrine and cardiovascular late effects among adult survivors of childhood brain tumors: Childhood Cancer Survivor Study. Cancer 2003, 97, 663–673. [Google Scholar] [CrossRef]
- Wang, K.W.; Fleming, A.; Johnston, D.L.; Zelcer, S.M.; Rassekh, S.R.; Ladhani, S.; Socha, A.; Shinuda, J.; Jaber, S.; Burrow, S.; et al. Overweight, obesity and adiposity in survivors of childhood brain tumours: A systematic review and meta-analysis. Clin. Obes. 2018, 8, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Lek, N.; Prentice, P.; Williams, R.M.; Ong, K.K.; Burke, G.A.; Acerini, C.L. Risk factors for obesity in childhood survivors of suprasellar brain tumours: A retrospective study. Acta Paediatr. 2010, 99, 1522–1526. [Google Scholar] [CrossRef] [PubMed]
- Gurney, J.G.; Ness, K.K.; Stovall, M.; Wolden, S.; Punyko, J.A.; Neglia, J.P.; Mertens, A.C.; Packer, R.J.; Robison, L.L.; Sklar, C.A. Final height and body mass index among adult survivors of childhood brain cancer: Childhood cancer survivor study. J. Clin. Endocrinol. Metab. 2003, 88, 4731–4739. [Google Scholar] [CrossRef] [PubMed]
- Gance-Cleveland, B.; Linton, A.; Arbet, J.; Stiller, D.; Sylvain, G. Predictors of Overweight and Obesity in Childhood Cancer Survivors. J. Pediatr. Oncol. Nurs. 2020, 37, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.; Gettys, T.W.; Watson, P.; Wallace, P.; Ganaway, E.; Pan, Q.; Garvey, W.T. The metabolic significance of leptin in humans: Gender-based differences in relationship to adiposity, insulin sensitivity, and energy expenditure. J. Clin. Endocrinol. Metab. 1997, 82, 1293–1300. [Google Scholar] [CrossRef]
- Stierman, B.; Afful, J.; Carroll, M.D.; Chen, T.-C.; Davy, O.; Fink, S.; Fryar, C.D.; Gu, Q.; Hales, C.M.; Hughes, J.P. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes. In National Health Statistics Reports; National Center for Health Statistics (NCHS): Hyattsville, MD, USA, 2021. [Google Scholar]
- Mizuno, T.; Shu, I.W.; Makimura, H.; Mobbs, C. Obesity over the life course. Sci. Aging Knowl. Environ. 2004, 2004, re4. [Google Scholar] [CrossRef] [PubMed]
- Lustig, R.H. Hypothalamic obesity after craniopharyngioma: Mechanisms, diagnosis, and treatment. Front. Endocrinol. 2011, 2, 60. [Google Scholar] [CrossRef] [PubMed]
- Harz, K.J.; Müller, H.L.; Waldeck, E.; Pudel, V.; Roth, C. Obesity in patients with craniopharyngioma: Assessment of food intake and movement counts indicating physical activity. J. Clin. Endocrinol. Metab. 2003, 88, 5227–5231. [Google Scholar] [CrossRef]
- Cohen, J.; Collins, L.; Gregerson, L.; Chandra, J.; Cohn, R.J. Nutritional concerns of survivors of childhood cancer: A “First World” perspective. Pediatr. Blood Cancer 2020, 67 (Suppl. S3), e28193. [Google Scholar] [CrossRef]
- Hayek, S.; Gibson, T.M.; Leisenring, W.M.; Guida, J.L.; Gramatges, M.M.; Lupo, P.J.; Howell, R.M.; Oeffinger, K.C.; Bhatia, S.; Edelstein, K.; et al. Prevalence and Predictors of Frailty in Childhood Cancer Survivors and Siblings: A Report From the Childhood Cancer Survivor Study. J. Clin. Oncol. 2020, 38, 232–247. [Google Scholar] [CrossRef]
- van Roessel, I.; van Schaik, J.; Meeteren, A.; Boot, A.M.; der Grinten, H.L.C.; Clement, S.C.; van Iersel, L.; Han, K.S.; van Trotsenburg, A.S.P.; Vandertop, W.P.; et al. Body mass index at diagnosis of a childhood brain tumor; a reflection of hypothalamic-pituitary dysfunction or lifestyle? Support. Care Cancer 2022, 30, 6093–6102. [Google Scholar] [CrossRef] [PubMed]
- Karlage, R.E.; Wilson, C.L.; Zhang, N.; Kaste, S.; Green, D.M.; Armstrong, G.T.; Robison, L.L.; Chemaitilly, W.; Srivastava, D.K.; Hudson, M.M.; et al. Validity of anthropometric measurements for characterizing obesity among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort Study. Cancer 2015, 121, 2036–2043. [Google Scholar] [CrossRef] [PubMed]
- Runco, D.V.; Yoon, L.; Grooss, S.A.; Wong, C.K. Nutrition & Exercise Interventions in Pediatric Patients with Brain Tumors: A Narrative Review. J. Natl. Cancer Inst. Monogr. 2019, 2019, 163–168. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Total (N = 198; 100%) | Underweight (n = 8; 4.0%) | Healthy weight (n = 81; 40.9%) | Overweight (n = 53; 26.8%) | Obesity (n = 40; 20.2%) | Severe obesity (n = 16; 8.1%) | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Overweight or Obese vs. Not | Underweight vs. Not | |||||||
| Sex N (%) | ||||||||
| Male | 93 (47.0) | - | 32 (39.5) | 34 (64.2) | 20 (50.0) | 7 (43.8) | 0.006 | 0.007 |
| Female | 105 (53.0) | 8 (100.0) | 49 (60.5) | 19 (35.8) | 20 (50.0) | 9 (56.3) | ||
| Age Median [IQR] | ||||||||
| At diagnosis, years | 8 [4.0–12.0] | 6 [3.5–14.5] | 8 [5.0–13.0] | 8 [3.5–12.0] | 10 [5.0–12.8] | 5.5 [3.3–9.0] | 0.860 | 0.743 |
| At follow-up, years | 24.0 [20.0–28.0] | 20.5 [19.3–25.5] | 23.0 [20.0–27.0] | 24.0 [20.0–28.0] | 27.0 [20.3–32.8] | 25.0 [23.3–31.8] | 0.002 | 0.181 |
| Follow-up time, years (mean ± SD) | 16.5 ± 6.4 | 14.2 ± 6.3 | 15.1 ± 6.2 | 16.8 ± 5.6 | 17.9 ± 7.3 | 19.7 ± 6.2 | 0.005 | 0.323 |
| Race N (%) | ||||||||
| White | 167 (84.3) | 4 (50.0) | 70 (86.4) | 47 (88.7) | 31 (77.5) | 15 (93.8) | 0.698 | 0.022 |
| Black/African American | 8 (4.0) | 3 (37.5) | 3 (3.7) | 1 (1.9) | 1 (2.5) | - | ||
| Asian | 2 (1.0) | - | - | 2 (3.8) | - | - | ||
| Other or multiple races | 7 (3.5) | 1 (12.5) | 2 (2.5) | - | 4 (10.0) | - | ||
| Unknown | 14 (7.1) | - | 6 (7.4) | 3 (5.7) | 4 (10.0) | 1 (6.3) | ||
| Ethnicity N (%) | ||||||||
| Hispanic/Latino | 14 (7.1) | - | 6 (7.4) | 2 (3.8) | 4 (10.0) | 2 (12.5) | 1.000 | 0.229 |
| Not Hispanic/Latino | 132 (66.7) | 8 (100.0) | 46 (56.8) | 37 (69.8) | 28 (70.0) | 13 (81.3) | ||
| Unknown | 52 (26.3) | - | 29 (35.8) | 14 (26.4) | 8 (20.0) | 1 (6.3) | ||
| Insurance N (%) | ||||||||
| Medicaid/Mass Health | 78 (39.4) | 4 (50.0) | 24 (29.6) | 21 (39.6) | 21 (52.5) | 8 (50.0) | 0.109 | 0.760 |
| Private | 116 (58.6) | 4 (50.0) | 55 (67.9) | 31 (58.5) | 18 (45.0) | 8 (50.0) | ||
| Other | 4 (2.0) | - | 2 (2.5) | 1 (1.9) | 1 (2.5) | - | ||
| Tumor histology at primary diagnosis N (%) | ||||||||
| Low-grade glioma | 100 (50.5) | 6 (75.0) | 44 (54.3) | 25 (47.2) | 19 (47.5) | 6 (37.5) | 0.087 | 0.054 |
| Embryonal tumor | 40 (20.2) | - | 18 (22.2) | 11 (20.8) | 9 (22.5) | 2 (12.5) | ||
| Craniopharyngioma | 14 (7.1) | 1 (12.5) | 1 (1.2) | 2 (3.8) | 5 (12.5) | 5 (31.3) | ||
| Other | 44 (22.2) | 1 (12.5) | 18 (22.2) | 15 (28.3) | 7 (17.5) | 3 (18.8) | ||
| Primary tumor location N (%) | ||||||||
| Posterior fossa | 78 (39.4) | 3 (37.5) | 33 (40.7) | 22 (41.5) | 16 (40.0) | 4 (25.0) | 0.295 | 0.054 |
| Hypothalamus/optic pathway | 44 (22.2) | 1 (12.5) | 13 (16.0) | 9 (17.0) | 13 (32.5) | 8 (50.0) | ||
| Supratentorial | 62 (31.3) | 2 (25.0) | 30 (37.0) | 16 (30.2) | 11 (27.5) | 3 (18.8) | ||
| Cervicomedullary | 5 (2.5) | 2 (25.0) | 1 (1.2) | 1 (1.9) | - | 1 (6.3) | ||
| Spinal cord | 8 (4.0) | - | 4 (4.9) | 4 (7.5) | - | - | ||
| Tumor treatment N (%) | ||||||||
| Surgery | 179 (90.4) | 7 (87.5) | 74 (91.4) | 48 (90.6) | 36 (90.0) | 14 (87.5) | 1.000 | 0.561 |
| Chemotherapy | 102 (51.5) | 2 (25.0) | 48 (59.3) | 25 (47.2) | 19 (47.5) | 8 (50.0) | 0.255 | 0.160 |
| Radiotherapy | 104 (52.5) | 1 (12.5) | 36 (44.4) | 29 (54.7) | 26 (65.0) | 12 (75.0) | 0.007 | 0.028 |
| Presence of neurodevelopmental disorder N (%) | 46 (23.2) | 1 (12.5) | 16 (19.8) | 14 (26.4) | 12 (30.0) | 3 (18.8) | 0.239 | 0.684 |
| Presence of endocrine disorder N (%) | 83 (41.9) | 2 (25.0) | 29 (35.8) | 21 (39.6) | 22 (55.0) | 9 (56.3) | 0.083 | 0.472 |
| Stimulant use N (%) | 25 (12.6) | 1 (12.5) | 12 (14.8) | 7 (13.2) | 3 (7.5) | 2 (12.5) | 0.521 | 1.000 |
| Variable | Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| Males | 2.414 | 1.321–4.414 | 0.004 |
| Age at follow up | 1.103 | 1.037–1.173 | 0.002 |
| Craniopharyngioma | 5.764 | 1.197–27.751 | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, R.L.; Soja, J.; Yunker, A.G.; Uno, H.; Gordon, E.; Cooney, T.; Dieli-Conwright, C.M. Obesity Risk of Pediatric Central Nervous System Tumor Survivors: A Cross-Sectional Study. Nutrients 2023, 15, 2269. https://doi.org/10.3390/nu15102269
Wilson RL, Soja J, Yunker AG, Uno H, Gordon E, Cooney T, Dieli-Conwright CM. Obesity Risk of Pediatric Central Nervous System Tumor Survivors: A Cross-Sectional Study. Nutrients. 2023; 15(10):2269. https://doi.org/10.3390/nu15102269
Chicago/Turabian StyleWilson, Rebekah L., Jacqueline Soja, Alexandra G. Yunker, Hajime Uno, Erin Gordon, Tabitha Cooney, and Christina M. Dieli-Conwright. 2023. "Obesity Risk of Pediatric Central Nervous System Tumor Survivors: A Cross-Sectional Study" Nutrients 15, no. 10: 2269. https://doi.org/10.3390/nu15102269
APA StyleWilson, R. L., Soja, J., Yunker, A. G., Uno, H., Gordon, E., Cooney, T., & Dieli-Conwright, C. M. (2023). Obesity Risk of Pediatric Central Nervous System Tumor Survivors: A Cross-Sectional Study. Nutrients, 15(10), 2269. https://doi.org/10.3390/nu15102269