
Sugar Reduction Initiatives in the Eastern Mediterranean Region: A Systematic Review

 ,
,  ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Seeking Supplementary Information
2.5. Analysis
3. Results
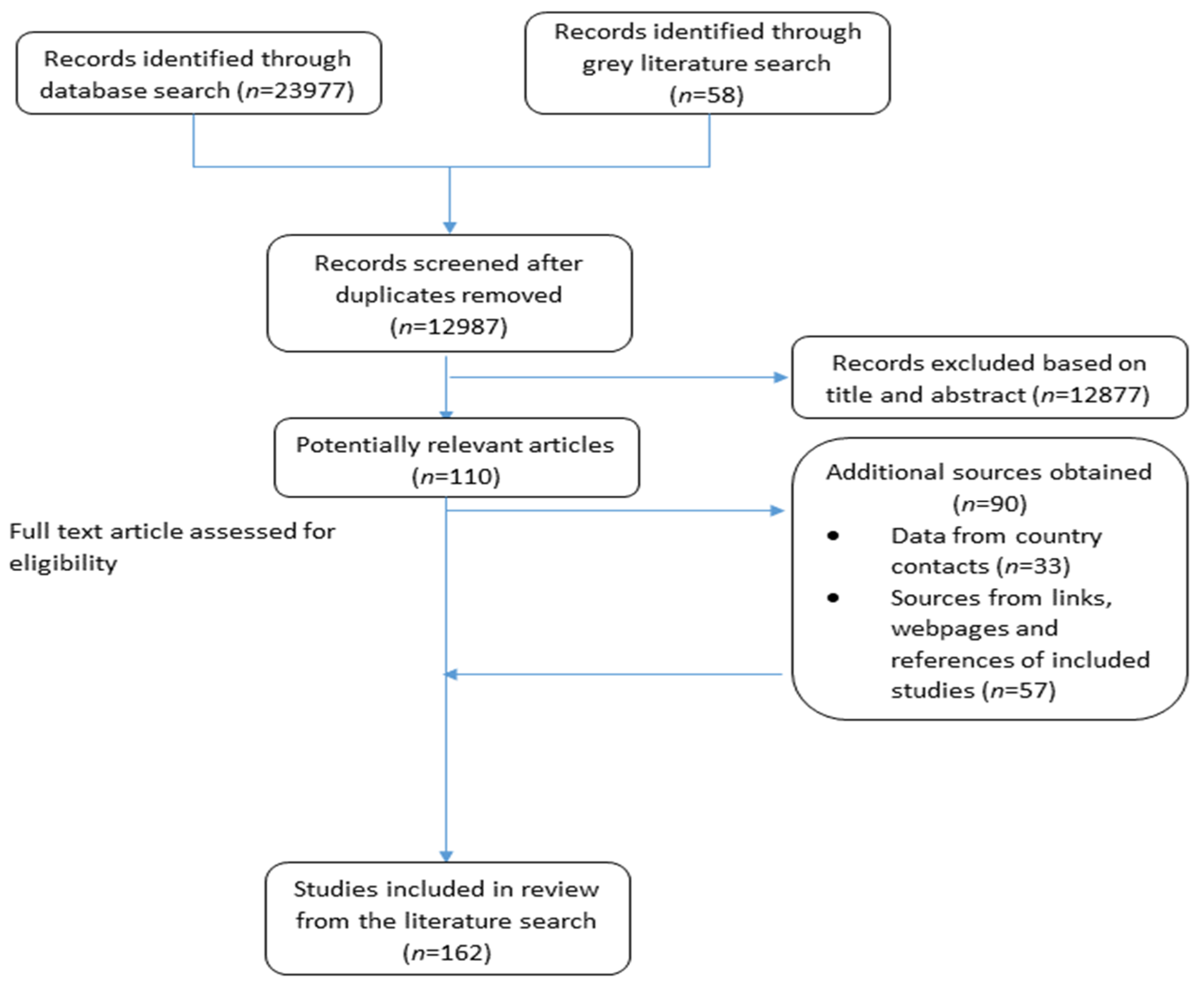
3.1. Search Results
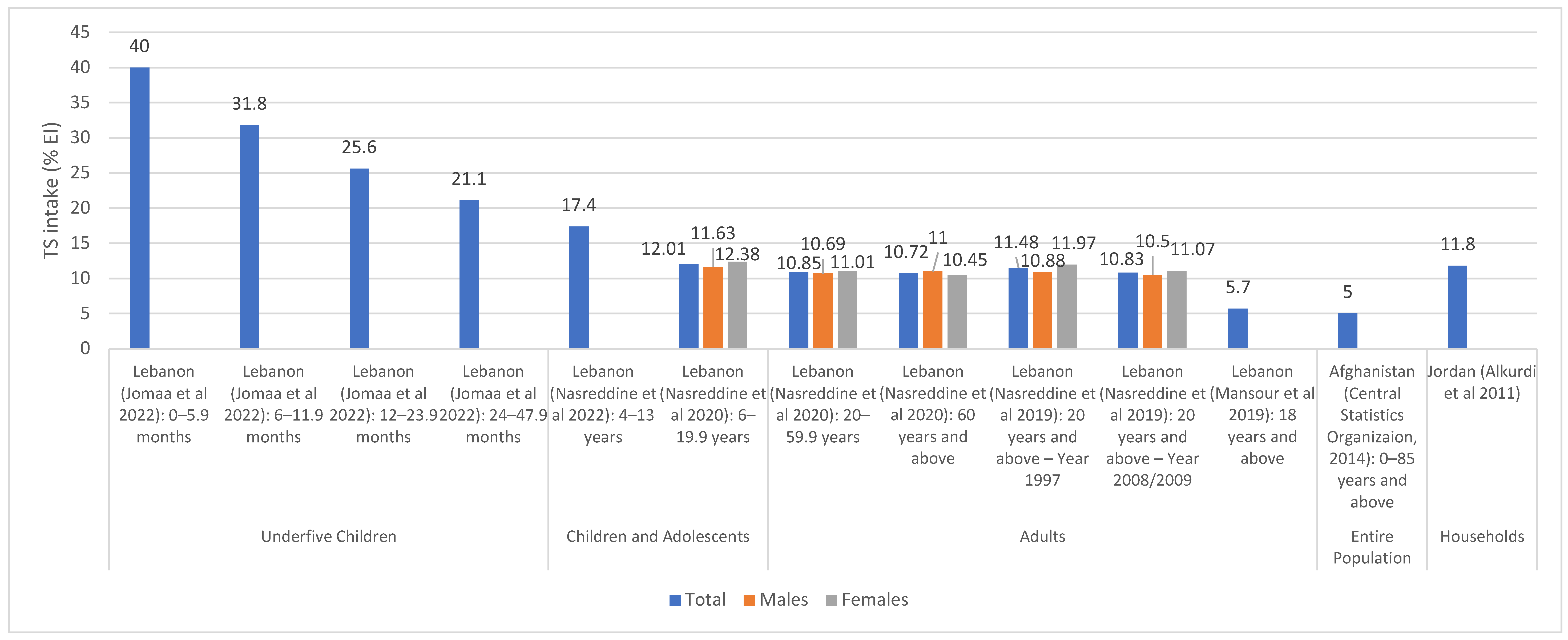
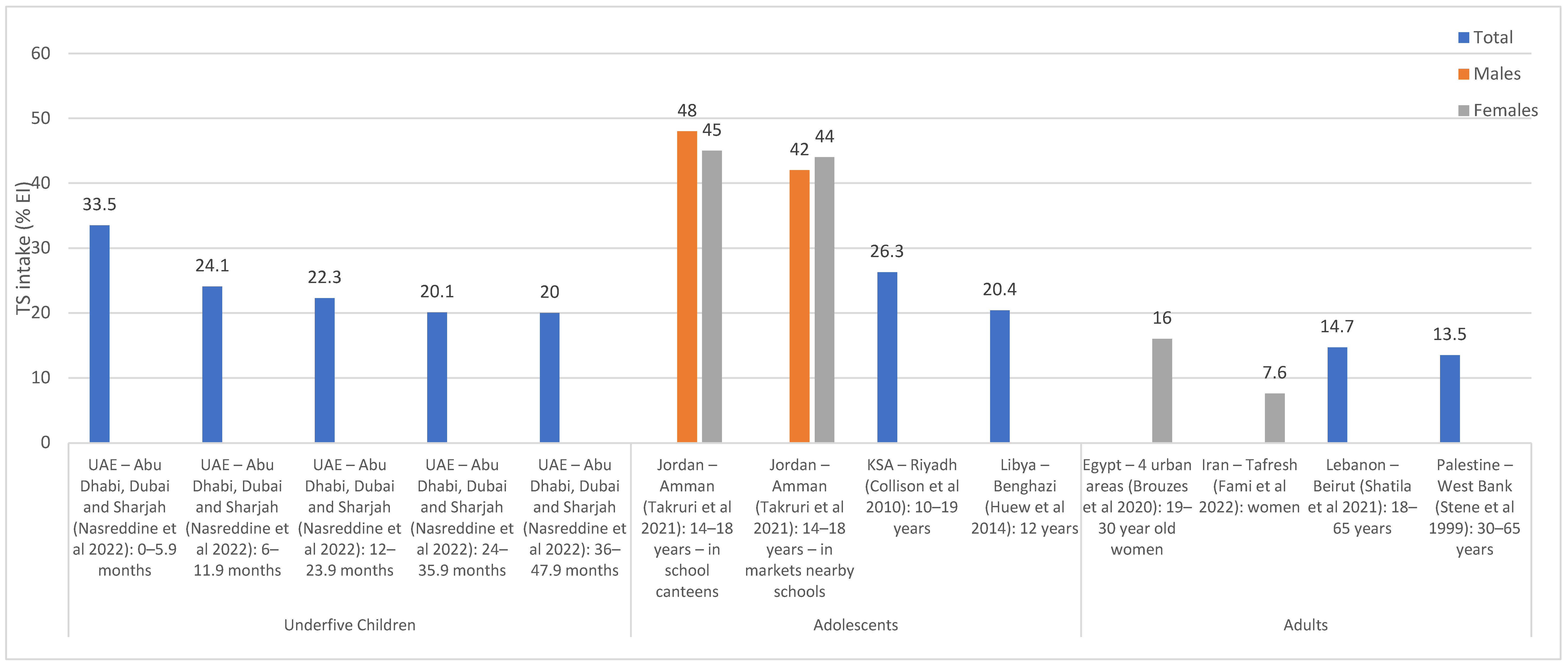
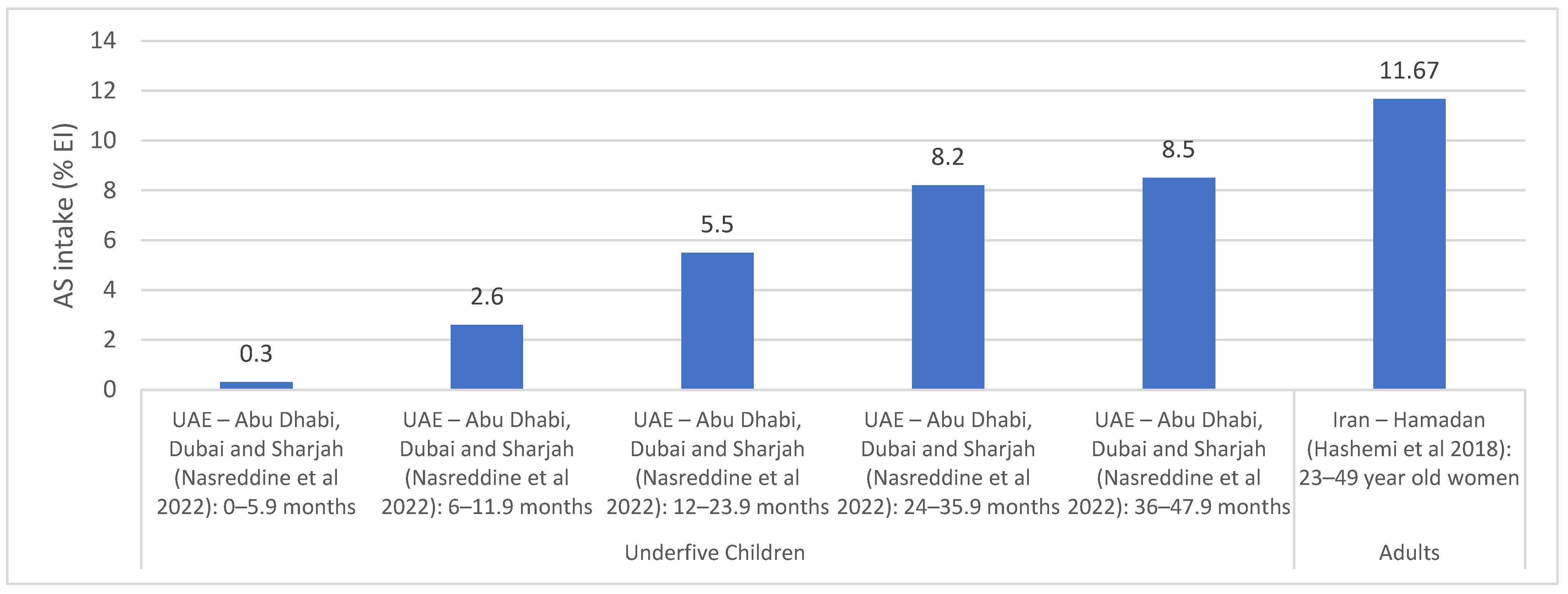
3.2. Assessment of Sugar Intake
3.3. Compliance/Adherence to Sugar Recommendations
3.4. Assessment of Sugar Levels in Food and Sugar-Related KAB
3.5. Countries with National Sugar Reduction Initiatives
3.6. Leadership and Strategic Approach
3.7. Implementation Strategies
3.7.1. Taxation, Elimination of Subsidies and Regulation of Marketing
3.7.2. Food Product Reformulation, Consumer Education, Labelling and Interventions in Specific Settings
3.8. Monitoring and Evaluation
3.9. Impact Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sugar | sugar* OR sucrose OR syrup* OR beverage* OR cola OR drink* OR soda OR sweet* OR chocolate* OR “ice cream*” OR candy OR candies OR cookie* OR jam OR confectioner* OR confectionar* OR cake* OR jelly OR jellies OR pastries OR pastry OR biscuit* OR bakery OR bakeries OR juice* OR honey OR pie OR pies OR dessert* OR cacao OR jam OR “chewing gum*” OR liquorice* OR marmalade* OR SSB OR cereal* OR smoothies OR milkshake* OR molasses OR fructose OR glucose |
| AND | |
| Reduction OR Intake | (reduce* OR reduction* OR reducing OR decreas* OR limit OR limits OR limitation* OR limiting OR restrict* OR reformulat* OR low*) OR (consumption OR consuming OR consume OR consumes OR intake* OR food* OR nutrition OR diet* OR source*) |
| AND | |
| Strategy/policy | standard* OR polic* OR initiative* OR tax* OR program* OR regulation* OR strateg* OR guideline* OR practice* OR legislat* OR action* OR plan OR plans OR intervention* OR law* OR campaign* OR marketing OR advertise* OR label* OR incentive* OR ban* OR recommendation* OR subsidy OR subsidies OR fiscal OR levy OR levies OR levied OR price* OR pricing OR excise* OR fee OR fees OR fine OR fines OR cost* |
| AND | |
| EMR | Afghan* OR Bahrain* OR Iran* OR Persia* OR Iraq* OR Jordan* OR Kuwait* OR Lebanon* OR Lebanese OR Libya* OR Oman* OR Palestin* OR Gaza* OR “West Bank” OR Qatar* OR Saud* OR KSA OR Syria* OR Tunis* OR “United Arab Emirate*” OR UAE OR Djibouti* OR Egypt* OR Morocc* OR Pakistan* OR Somal* OR Sudan* OR Yemen* OR Levant* OR “East* Mediterranean” OR Gulf OR GCC OR Arab OR Arabia OR Arabs OR EMR OR “Middle East*” OR MENA OR “North* Africa*” OR “East* Africa*” OR “Near East*” OR “Abu Dhabi” OR Dubai OR Ajman OR Fujaira* OR Sharja* OR *Khaima* OR *Qaiwain OR *Quwain |
References
- Sibai, A.M.; Nasreddine, L.; Mokdad, A.H.; Adra, N.; Tabet, M.; Hwalla, N. Nutrition transition and cardiovascular disease risk factors in Middle East and North Africa countries: Reviewing the evidence. Ann. Nutr. Metab. 2010, 57, 193–203. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Nutrition transition and the global diabetes epidemic. Curr. Diab. Rep. 2015, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Marinho, A.R.; Severo, M.; Correia, D.; Lobato, L.; Vilela, S.; Oliveira, A.; Ramos, E.; Torres, D.; Lopes, C.; Consortium, I.-A. Total, added and free sugar intakes, dietary sources and determinants of consumption in Portugal: The National Food, Nutrition and Physical Activity Survey (IAN-AF 2015–2016). Public Health Nutr. 2019, 23, 869–881. [Google Scholar] [CrossRef] [PubMed]
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A. Sugar in infants, children and adolescents: A position paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.; Latulippe, M.E.; Ayoob, K.; Slavin, J. The confusing world of dietary sugars: Definitions, intakes, food sources and international dietary recommendations. Food Funct. 2012, 3, 477–486. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/bitstream/handle/10665/149782/9789241549028_eng.pdf;jsessionid=77485E8F53EB13D8F39A95ECC0E89A9B?sequence=1 (accessed on 3 October 2022).
- Mesana, M.; Hilbig, A.; Androutsos, O.; Cuenca-Garcia, M.; Dallongeville, J.; Huybrechts, I.; De Henauw, S.; Widhalm, K.; Kafatos, A.; Nova, E. Dietary sources of sugars in adolescents’ diet: The HELENA study. Eur. J. Nutr. 2018, 57, 629–641. [Google Scholar] [CrossRef]
- Ruiz, E.; Rodriguez, P.; Valero, T.; Ávila, J.M.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Dietary intake of individual (free and intrinsic) sugars and food sources in the Spanish population: Findings from the ANIBES study. Nutrients 2017, 9, 275. [Google Scholar] [CrossRef]
- Alexy, U.; Sichert-Hellert, W.; Kersting, M. Associations between intake of added sugars and intakes of nutrients and food groups in the diets of German children and adolescents. Br. J. Nutr. 2003, 90, 441–447. [Google Scholar] [CrossRef][Green Version]
- Marshall, T.A.; Eichenberger Gilmore, J.M.; Broffitt, B.; Stumbo, P.J.; Levy, S.M. Diet quality in young children is influenced by beverage consumption. J. Am. Coll. Nutr. 2005, 24, 65–75. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; Berger, A. Added sugars drive nutrient and energy deficit in obesity: A new paradigm. Open Heart 2016, 3, e000469. [Google Scholar] [CrossRef] [PubMed]
- Arnone, D.; Chabot, C.; Heba, A.-C.; Kökten, T.; Caron, B.; Hansmannel, F.; Dreumont, N.; Ananthakrishnan, A.N.; Quilliot, D.; Peyrin-Biroulet, L. Sugars and gastrointestinal health. Clin. Gastroenterol. Hepatol. 2021, 20, 1912–1924.e7. [Google Scholar] [CrossRef]
- Ludwig, R.; Schmidt, L.; Brindis, C. Public health: The toxic truth about sugar. Nature 2011, 482, 27–29. [Google Scholar]
- Malik, V.S.; Hu, F.B. Sugar-sweetened beverages and health: Where does the evidence stand? Am. J. Clin. Nutr. 2011, 94, 1161–1162. [Google Scholar] [CrossRef]
- Liu, H.; Liu, Y.; Shi, M.; Zhou, Y.; Zhao, Y.; Xia, Y. Meta-analysis of sugar-sweetened beverage intake and the risk of cognitive disorders. J. Affect. Disord. 2022, 313, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Libuda, L.; Kersting, M. Soft drinks and body weight development in childhood: Is there a relationship? Curr. Opin Clin. Nutr. Metab. Care 2009, 12, 596–600. [Google Scholar] [CrossRef]
- Ambrosini, G.L.; Johns, D.J.; Northstone, K.; Emmett, P.M.; Jebb, S.A. Free sugars and total fat are important characteristics of a dietary pattern associated with adiposity across childhood and adolescence. J. Nutr. 2015, 146, 778–784. [Google Scholar] [CrossRef]
- Welsh, J.A.; Sharma, A.; Cunningham, S.A.; Vos, M.B. Consumption of added sugars and indicators of cardiovascular disease risk among US adolescents. Circulation 2011, 123, 249–257. [Google Scholar] [CrossRef]
- Kondaki, K.; Grammatikaki, E.; Jiménez-Pavón, D.; De Henauw, S.; Gonzalez-Gross, M.; Sjöstrom, M.; Gottrand, F.; Molnar, D.; Moreno, L.A.; Kafatos, A. Daily sugar-sweetened beverage consumption and insulin resistance in European adolescents: The HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr. 2013, 16, 479–486. [Google Scholar] [CrossRef]
- Sheiham, A.; James, W. Diet and dental caries: The pivotal role of free sugars reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef]
- US Department of Health and Human Services and US Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th Edition. 2015. Available online: https://health.gov/our-work/nutrition-physical-activity/dietary-guidelines/previous-dietary-guidelines/2015 (accessed on 3 October 2022).
- EFSAPanel on Nutrition, N.F.; Allergens, F.; Turck, D.; Bohn, T.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; et al. Tolerable upper intake level for dietary sugars. EFSA J. 2022, 20, e07074. [Google Scholar]
- Rippe, J.M.; Sievenpiper, J.L.; Lê, K.-A.; White, J.S.; Clemens, R.; Angelopoulos, T.J. What is the appropriate upper limit for added sugars consumption? Nutr. Rev. 2017, 75, 18–36. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.K.; Appel, L.J.; Brands, M.; Howard, B.V.; Lefevre, M.; Lustig, R.H.; Sacks, F.; Steffen, L.M.; Wylie-Rosett, J. Dietary sugars intake and cardiovascular health: A scientific statement from the American Heart Association. Circulation 2009, 120, 1011–1020. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Eastern Mediterranean. Policy Statement and Recommended Actions for Lowering Sugar Intake and Reducing Prevalence of Type 2 Diabetes and Obesity in the Eastern Mediterranean Region. 2016. Available online: https://applications.emro.who.int/dsaf/EMROPUB_2016_en_18687.pdf (accessed on 3 October 2022).
- World Health Organization Regional Office for the Eastern Mediterranean. Strategy on Nutrition for the Eastern Mediterranean Region 2020–2030; World Health Organization Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/330059/9789290222996-eng.pdf?sequence=1&isAllowed=y (accessed on 4 October 2022).
- World Health Organization Regional Office for the Eastern Mediterranean. Regional Framework for Action on Obesity Prevention 2019–2023; World Health Organization Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/325833/EMROPUB_2019_en_22319.pdf?sequence=1&isAllowed=y (accessed on 4 October 2022).
- Santos, J.A.; Tekle, D.; Rosewarne, E.; Flexner, N.; Cobb, L.; Al-Jawaldeh, A.; Kim, W.J.; Breda, J.; Whiting, S.; Campbell, N. A systematic review of salt reduction initiatives around the world: A midterm evaluation of progress towards the 2025 global non-communicable diseases salt reduction target. Adv. Nutr. 2021, 12, 1768–1780. [Google Scholar] [CrossRef] [PubMed]
- Al-Jawaldeh, A.; Taktouk, M.; Chatila, A.; Naalbandian, S.; Al-Thani, A.-A.M.; Alkhalaf, M.M.; Almamary, S.; Barham, R.; Baqadir, N.M.; Binsunaid, F.F. Salt reduction initiatives in the Eastern Mediterranean Region and evaluation of progress towards the 2025 global target: A systematic review. Nutrients 2021, 13, 2676. [Google Scholar] [CrossRef] [PubMed]
- Al-Jawaldeh, A.; Taktouk, M.; Chatila, A.; Naalbandian, S.; Abdollahi, Z.; Ajlan, B.; Al Hamad, N.; Alkhalaf, M.M.; Almamary, S.; Alobaid, R. A systematic review of trans fat reduction initiatives in the Eastern Mediterranean Region. Front. Nutr. 2021, 8, 771492. [Google Scholar] [CrossRef]
- World Health Organization. Fiscal Policies to Promote Healthy Diets: Policy Brief; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240049543 (accessed on 12 September 2022).
- Knowledge for Policy-European Commission. Implemented Policies to Address Sugars Intake. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/sugars-sweeteners-10_en (accessed on 20 September 2022).
- Krieger, J.; Bleich, S.N.; Scarmo, S.; Ng, S.W. Sugar-sweetened beverage reduction policies: Progress and promise. Annu. Rev. Public Health 2021, 42, 439–461. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; Vanderlee, L. Effect of formulation, labelling, and taxation policies on the nutritional quality of the food supply. Curr. Nutr. Rep. 2019, 8, 240–249. [Google Scholar] [CrossRef]
- Gharib, N.; Rasheed, P. Energy and macronutrient intake and dietary pattern among school children in Bahrain: A cross-sectional study. Nutr. J. 2011, 10, 12. [Google Scholar] [CrossRef]
- Nasreddine, L.; Hwalla, N.; Al Zahraa Chokor, F.; Naja, F.; O’Neill, L.; Jomaa, L. Food and nutrient intake of school-aged children in Lebanon and their adherence to dietary guidelines and recommendations. BMC Public Health 2022, 22, 922. [Google Scholar] [CrossRef] [PubMed]
- Jomaa, L.; Hamamji, S.; Kharroubi, S.; Diab-El-Harakeh, M.; Chokor, F.A.; Nasreddine, L. Dietary intakes, sources, and determinants of free sugars amongst Lebanese children and adolescents: Findings from two national surveys. Eur. J. Nutr. 2021, 60, 2655–2669. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Chamieh, M.C.; Ayoub, J.; Hwalla, N.; Sibai, A.M.; Naja, F. Sex disparities in dietary intake across the lifespan: The case of Lebanon. Nutr. J. 2020, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- Hamamji, S.E. Intakes and Sources of Fat, Free Sugars and Salt among Lebanese Children and Adolescents. Master’s Thesis, American University of Beirut, Beirut, Lebanon, 2018. [Google Scholar]
- Nasreddine, L.; Ayoub, J.J.; Hachem, F.; Tabbara, J.; Sibai, A.M.; Hwalla, N.; Naja, F. Differences in dietary intakes among Lebanese adults over a decade: Results from two national surveys 1997–2008/2009. Nutrients 2019, 11, 1738. [Google Scholar] [CrossRef] [PubMed]
- Mansour, M.; Tamim, H.; Nasreddine, L.; El Khoury, C.; Hwalla, N.; Chaaya, M.; Farhat, A.; Sibai, A.M. Prevalence and associations of behavioural risk factors with blood lipids profile in Lebanese adults: Findings from WHO STEPwise NCD cross-sectional survey. BMJ Open 2019, 9, 9. [Google Scholar] [CrossRef]
- Ministry of Health-Sudan; World Health Organization. Sudan STEPwise Survey for Non-Communicable Disease Risk Factors 2016 Report. 2016. Available online: https://www.who.int/ncds/surveillance/steps/Sudan_STEPwise_SURVEY_final_2016.pdf?ua=1 (accessed on 12 September 2022).
- Central Statistics Organization. The National Risk and Vulnerability Assessment 2011–2012 (Afghanistan Living Conditions Survey); Afghanistan, 2014. Available online: https://www.humanitarianresponse.info/en/operations/afghanistan/assessment/national-risk-and-vulnerability-assessment-20112012 (accessed on 12 September 2022).
- Eini-Zinab, H.; Sobhani, S.R.; Rezazadeh, A. Designing a healthy, low-cost and environmentally sustainable food basket: An optimisation study. Public Health Nutr. 2020, 24, 1952–1961. [Google Scholar] [CrossRef]
- Alkurd, R.A.; Fares, M.A.A.; Takruri, H.R. Trends of the intakes of energy, macronutrients and their food sources in Jordan. Saudi Soc. Food Nutr. J. 2022, 6, 40–54. [Google Scholar]
- Government of Pakistan. Household Integrated Economic Survey (HIES) 2018-19; Pakistan Bureau of Statistics: Islamabad, Pakistan, 2020; Available online: https://phkh.nhsrc.pk/sites/default/files/2021-07/Household%20Integrated%20Economic%20Survey%20Pakistan%202018-19.pdf (accessed on 12 September 2022).
- Naeeni, M.M.; Jafari, S.; Fouladgar, M.; Heidari, K.; Farajzadegan, Z.; Fakhri, M.; Karami, P.; Omidi, R. Nutritional knowledge, practice, and dietary habits among school children and adolescents. Int. J. Prev. Med. 2014, 5, S171–S178. [Google Scholar] [CrossRef]
- Montazerifar, F.; Karajibani, M.; Dashipour, A.R. Evaluation of dietary intake and food patterns of adolescent girls in sistan and baluchistan province, Iran. Funct. Foods Health Dis. 2012, 2, 62–71. [Google Scholar] [CrossRef]
- Thana’Y, A.; Tayyem, R.F.; Takruri, H.R. Nutrient Intakes among Jordanian Adolescents Based on Gender and Body Mass Index. Int. J. Child Health Nutr. 2020, 9, 9–16. [Google Scholar]
- Collison, K.S.; Zaidi, M.Z.; Subhani, S.N.; Al-Rubeaan, K.; Shoukri, M.; Al-Mohanna, F.A. Sugar-sweetened carbonated beverage consumption correlates with BMI, waist circumference, and poor dietary choices in school children. BMC Public Health 2010, 10, 234. [Google Scholar] [CrossRef]
- Huew, R.; Maguire, A.; Waterhouse, P.; Moynihan, P. Nutrient intake and dietary patterns of relevance to dental health of 12-year-old Libyan children. Public Health Nutr. 2014, 17, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Brouzes, C.M.C.; Darcel, N.; Tome, D.; Dao, M.C.; Bourdet-Sicard, R.; Holmes, B.A.; Lluch, A. Urban Egyptian Women Aged 19-30 Years Display Nutrition Transition-Like Dietary Patterns, with High Energy and Sodium Intakes, and Insufficient Iron, Vitamin D, and Folate Intakes. Curr. Dev. Nutr. 2020, 4, 10. [Google Scholar] [CrossRef]
- Fami, H.S.; Veerabhadraiah, V.; Nath, K.G. Nutritional status of rural women in relation to their participation in mixed farming in the Tafresh area of Iran. Food Nutr. Bull. 2002, 23, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Stene, L.C.M.; Giacaman, R.; Abdul-Rahim, H.; Husseini, A.; Norum, K.R.; Holmboe-Ottesen, G. Food consumption patterns in a Palestinian West Bank population. Eur. J. Clin. Nutr. 1999, 53, 953–958. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Awadi, S.; Rawashdeh, S.; Talafha, M.; Bani-Issa, J.; Alkadiri, M.A.S.; Al Zoubi, M.S.; Hussein, E.; Fattah, F.A.; Bashayreh, I.H.; Al-Saghir, M. Impact of COVID-19 pandemic on the Jordanian eating and nutritional habits. Heliyon 2022, 8, e09585. [Google Scholar]
- Jomaa, L.; Hwalla, N.; Chokor, F.A.Z.; Naja, F.; O’Neill, L.; Nasreddine, L. Food consumption patterns and nutrient intakes of infants and young children amidst the nutrition transition: The case of Lebanon. Nutr. J. 2022, 21, 34. [Google Scholar] [CrossRef]
- Benjelloun, S. Nutrition transition in Morocco. Public Health Nutr. 2002, 5, 135–140. [Google Scholar] [CrossRef]
- Nasreddine, L.M.; Naja, F.A.; Hwalla, N.C.; Ali, H.I.; Mohamad, M.N.; Chokor, F.A.Z.S.; Chehade, L.N.; O’Neill, L.M.; Kharroubi, S.A.; Ayesh, W.H. Total Usual Nutrient Intakes and Nutritional Status of United Arab Emirates Children (< 4 Years): Findings from the Feeding Infants and Toddlers Study (FITS) 2021. Curr. Dev. Nutr. 2022, 6, nzac080. [Google Scholar]
- Takruri, H.; ALjaraedah, T.; Tayyem, R. Food and nutrient intakes from school canteens and markets nearby schools among students aged 14-18 in Jordan. Nutr. Food Sci. 2021, 52, 391–402. [Google Scholar] [CrossRef]
- Shatila, H.; Baroudi, M.; El Sayed Ahmad, R.; Chehab, R.; Forman, M.R.; Abbas, N.; Faris, M.; Naja, F. Impact of Ramadan fasting on dietary intakes among healthy adults: A year-round comparative study. Front. Nutr. 2021, 8, 689788. [Google Scholar] [CrossRef]
- Aoun, R.; Chokor, F.A.Z.; Taktouk, M.; Nasrallah, M.; Ismaeel, H.; Tamim, H.; Nasreddine, L. Dietary fructose and its association with the metabolic syndrome in Lebanese healthy adults: A cross-sectional study. Diabetol. Metab. Syndr. 2022, 14, 29. [Google Scholar] [CrossRef]
- Shahinfar, H.; Safabakhsh, M.; Mansouri, S.; Djafarian, K.; Clark, C.C.T.; Shab-Bidar, S. Association of dietary energy density with cardiometabolic risk factors and metabolic syndrome in Tehranian older adults. J. Cardiovasc. Thorac. Res. 2020, 12, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, S.Z.; Vahidinia, A.; Hazavehei, S.M.M.; Karimi-Shahanjarini, A.; Poorolajal, J.; Erfani, H.; Entezari, M.H.; Eskandari, Z.; Shababadi, S. Nutrient intake and unhealthy dietary pattern of Iranian women: A cross sectional study. Prog. Nutr. 2018, 20, 106–118. [Google Scholar]
- Aounallah-Skhiri, H.; Traissac, P.; El-Ati, J.; Eymard-Duvernay, S.; Landais, E.; Achour, N.; Delpeuch, F.; Romdhane, H.B.; Maire, B. Nutrition transition among adolescents of a south-Mediterranean country: Dietary patterns, association with socioeconomic factors, overweight and blood pressure. A cross-sectional study in Tunisia. Nutr. J. 2011, 10, 38. [Google Scholar] [CrossRef]
- Nasreddine, L.; Hwalla, N.; Sibai, A.; Hamzé, M.; Parent-Massin, D. Food consumption patterns in an adult urban population in Beirut, Lebanon. Public Health Nutr. 2006, 9, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Naja, F.; Sibai, A.M.; Helou, K.; Adra, N.; Hwalla, N. Trends in nutritional intakes and nutrition-related cardiovascular disease risk factors in Lebanon: The need for immediate action. J. Med. Liban 2014, 62, 83–91. [Google Scholar] [CrossRef]
- Abassi, M.M.; Sassi, S.; El Ati, J.; Gharbia, H.B.; Delpeuch, F.; Traissac, P. Gender inequalities in diet quality and their socioeconomic patterning in a nutrition transition context in the Middle East and North Africa: A cross-sectional study in Tunisia. Nutr. J. 2019, 18, 18. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation, Geneva, 28 January–1 February 2002; World Health Organization: Geneva, Switzerland, 2003; Available online: https://apps.who.int/iris/bitstream/handle/10665/42665/WHO_TRS_916.pdf?sequence=1&isAllowed=y (accessed on 2 October 2022).
- Murphy, S.P.; Guenther, P.M.; Kretsch, M.J. Using the dietary reference intakes to assess intakes of groups: Pitfalls to avoid. J. Am. Diet. Assoc. 2006, 10, 1550–1553. [Google Scholar] [CrossRef]
- Mumena, W.A. Consumption of free sugar predicts nutrient intake of Saudi children. Front. Nutr. 2021, 8, 782853. [Google Scholar] [CrossRef]
- Mirmiran, P.; Hosseini-Esfahani, F.; Jessri, M.; Mahan, L.K.; Shiva, N.; Azizi, F. Does Dietary Intake by Tehranian Adults Align with the 2005 Dietary Guidelines for Americans? Observations from the Tehran Lipid and Glucose Study. J. Heatlh Popul. Nutr. 2011, 29, 39–52. [Google Scholar] [CrossRef]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A. Added sugars and cardiovascular disease risk in children: A scientific statement from the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef]
- World Health Organization. Healthy Diet. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 2 October 2022).
- Khoshtinat, K.; Koohy-Kamaly, P.; Komeili-Fanood, R.; Sohrabvandi, S.; Khosravi-Darani, K.; Mohammadi, M.; Zand-Rajabi, H.; Tavakoli, E.; Salehi, M.; Bahramian, G. Comparative study of salt, total fat and sugar contents of mayonnaise and salad dressings from the Iranian market in 2017 and 2019. East. Mediterr. Health J. 2021, 27, 452–458. [Google Scholar] [CrossRef]
- Aloudat, M.; Papp, A.; Magyar, N.; Sarkadi, L.S.; Lugasi, A. Nutritional Value of Traditional and Modern Meals: Jordan and Hungary. Acta Aliment. 2020, 49, 491–497. [Google Scholar] [CrossRef]
- Al-Jawaldeh, A.; Hoteit, M.; Zoghbi, E.; Al Iskandarani, M.; Rady, A.; Shankiti, I.; Matta, J. Nutritional value of the Middle Eastern diet: Analysis of total sugar, salt, and iron in Lebanese traditional dishes. F1000Research 2020, 9, 1254. [Google Scholar]
- Hoteit, M.; Zoghbi, E. Food Composition Data: Traditional Dishes, Arabic Sweets, and Market Foods. 2021. Available online: http://luwebxx.ul.edu.lb/en/food-composition-data-traditional-dishes-arabic-sweets-and-market-foods (accessed on 5 September 2022).
- Hoteit, M.; Zoghbi, E.; Rady, A.; Shankiti, I.; Al-Jawaldeh, A. Development of a Lebanese food exchange system based on frequently consumed Eastern Mediterranean traditional dishes and Arabic sweets. F1000Research 2021, 10, 12. [Google Scholar] [CrossRef]
- AbuKhader, M.M. Examining the amounts of added sugars and saturated fatty acids recorded on the nutrition panels of snack foods for young children. Prog. Nutr. 2018, 20, 570–577. [Google Scholar]
- World Health Organization. Summary Report on the Regional Meeting to Standardize and Update Food Composition Tables, Reflecting Sugar, Trans Fat, Saturated Fat and Salt Contents, Rabat, Morocco, 20–22 September 2016; World Health Organization. Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2016; Available online: https://apps.who.int/iris/handle/10665/251837 (accessed on 16 September 2022).
- Hadian, Z.; Mousavikhaneghah, A. Sugar, fat, saturated and trans fatty acid contents in Iranian cereal-based baked products. Food Sci. Technol. 2021, 42. [Google Scholar] [CrossRef]
- Wahab, R.A. Food Label Use and Awareness of Nutritional Information Among Consumers in Bahrain: An Exploratory Study. KnE Life Sci. 2018, 26–36. [Google Scholar] [CrossRef]
- Hasan Saad, F. Safe Use of Salt, Sugar and Fats for the Rural Women in Some Villages of Kafr El-sheikh Governorate. Agric. Econ. Soc. Sci. 2021, 12, 669–681. [Google Scholar]
- Rad, M.; Shahravan, A.; Haghdoost, A.A. The dietary patterns of 12-year-old children and their awareness about the effect of diet on oral health in Iran. J. Oral Health Oral Epidemiol. 2017, 6, 102–109. [Google Scholar]
- Rahnama, R.; Rampal, L.; Lye, M.S.; Sidik, S.M.; Abedi, P. Diet knowledge and behaviors related to prevention of obesity among students aged 11 to 15 years in Shiraz, Iran. Iran. Red Crescent Med. J. 2017, 19, e15730. [Google Scholar] [CrossRef]
- Saeidlou, S.N.; Babaei, F.; Ayremlou, P. Nutritional Knowledge, Attitude and Practice of North West Households in Iran: Is Knowledge likely to Become Practice? Maedica 2016, 11, 286–295. [Google Scholar] [PubMed]
- Ahadi, Z.; Heshmat, R.; Sanaei, M.; Shafiee, G.; Ghaderpanahi, M.; Homami, M.R.; Salehi, F.; Abdollahi, Z.; Azemati, B.; Larijani, B. Knowledge, attitude and practice of urban and rural households towards principles of nutrition in Iran: Results of NUTRIKAP survey. J. Diabetes Metab. Disord 2014, 13, 100. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Azadbakht, L.; Azizi, F. Dietary behaviour of Tehranian adolescents does not accord with their nutritional knowledge. Public Health Nutr. 2007, 10, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Rajab, L.D.; Petersen, P.E.; Bakaeen, G.; Hamdan, M.A. Oral health behaviour of schoolchildren and parents in Jordan. Int. J. Paediatr. Dent. 2002, 12, 168–176. [Google Scholar] [CrossRef]
- Mumena, W.A. Maternal Knowledge, Attitude and Practices toward Free Sugar and the Associations with Free Sugar Intake in Children. Nutrients 2021, 13, 4403. [Google Scholar] [CrossRef] [PubMed]
- Gehad, M.S.; Ali, F.A.; Thamir, M.A. Energy drinks and population health: Consumption pattern and adverse effects among Saudi population. BMC Public Health 2019, 19, 1539. [Google Scholar]
- Mumena, W.A.; Alamri, A.A.; Mahrous, A.A.; Alharbi, B.M.; Almohaimeed, J.S.; Hakeem, M.I.; Kutbi, H.A. Knowledge, attitudes, and practices toward added sugar consumption among female undergraduate students in Madinah, Saudi Arabia: A cross-sectional study. Nutrition 2020, 79-80, 6. [Google Scholar] [CrossRef]
- Hakim, N.A. Diabetes awareness and dietary habits of non-diabetic females in private universities in Jeddah city; Saudi Arabia. Prog. Nutr. 2020, 22, 9. [Google Scholar]
- Sultan, A.A.; Al Saleem, S.A.; Osman, A.A.M.; Mostafa, O.A. Knowledge and Prevalence of Energy Drinks Consumption among King Khalid University Female Students. World Fam. Med. 2020, 18, 4–17. [Google Scholar] [CrossRef]
- Alshammary, F.; Aljohani, F.A.; Alkhuwayr, F.S.; Siddiqui, A.A. Measurement of parents’ knowledge toward oral health of their children: An observational study from Hail, Saudi Arabia. J. Contemp. Dental. Pract. 2019, 20, 801–805. [Google Scholar]
- Alrasheedi, A.A. Prevalence and reasons for consumption of energy drinks among adolescents and young adults in Jeddah, Saudi Arabia. Glob. J. Health Sci. 2016, 9, 23–28. [Google Scholar] [CrossRef]
- Quadri, F.A.; Hendriyani, H.; Pramono, A.; Jafer, M. Knowledge, attitudes and practices of sweet food and beverage consumption and its association with dental caries among schoolchildren in Jazan, Saudi Arabia. East Mediter. Health J. 2015, 21, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Aluqmany, R.; Mansoor, R.; Saad, U.; Abdullah, R.; Ahamd, A. Consumption of energy drinks among female secondary school students, Almadinah Almunawwarah, Kingdom of Saudi Arabia, 2011. J. Taibah Univ. Med. Soc. 2013, 8, 60–65. [Google Scholar] [CrossRef][Green Version]
- Wyne, A.H.; Chohan, A.N.; Al-Dosari, K.; Al-Dokheil, M. Oral health knowledge and sources of information among male Saudi school children. Odontostomatol. Trop. 2004, 27, 22–26. [Google Scholar]
- Wyne, A.H.; Al-Ghorabi, B.M.; Al-Asiri, Y.A.; Khan, N.B. Caries prevalence in Saudi primary schoolchildren of Riyadh and their teachers’ oral health knowledge, attitude and practices. Saudi Med. J. 2002, 23, 77–81. [Google Scholar] [PubMed]
- Al-Othaimeen, A.; Osman, A.K.; Al Orf, S. Prevalence of nutritional anaemia among primary school girls in Riyadh City, Saudi Arabia. Int. J. Food Sci. Nutr. 1999, 50, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health-Kuwait. Eastern Mediterranean Approach for Control of Non Communicable Diseases. Survey for Risk Factors for Chronic Non Communicable Diseases. 2015. Available online: https://extranet.who.int/ncdsmicrodata/index.php/catalog/472/related-materials (accessed on 16 September 2022).
- Rahman, A.A. A Theory-Based Exploration of Adding Sugar to Beverages in Lebanese Public School Children. Doctoral Thesis, University of Strathclyde, Glasgow, UK, 2016. [Google Scholar]
- Ministry of Health-Morocco. Enquête Nationale sur les Facteurs de Risque Communs des Maladies Non Transmissibles 2017–2018: Rapport. 2017. Available online: https://extranet.who.int/ncdsmicrodata/index.php/catalog/544/related-materials (accessed on 16 September 2022).
- Chalgoum, N.B.; Koubaa, A.A.; Dahmen, H.; Kochbati, A. Nutritional practices of young children. Tunis. Med. 2009, 87, 786–789. [Google Scholar]
- Manickavasagan, A.; Al-Mahdouri, A.A.; Al-Mufargi, A.M.S.; Al-Souti, A.; Al-Mezeini, A.S.M.; Essa, M.M. Healthy eating knowledge among college students in Muscat: A self reported survey. Pak. J. Nutr. 2014, 13, 397–403. [Google Scholar] [CrossRef]
- Al Riyami, A.; Al Hadabi, S.; Abd El Aty, M.A.; Al Kharusi, H.; Morsi, M.; Jaju, S. Nutrition knowledge, beliefs and dietary habits among elderly people in Nizwa, Oman: Implications for policy. East Mediter. Health J. 2010, 16, 859–867. [Google Scholar] [CrossRef]
- Ministry of National Health Services Regulations and Coordination-Pakistan. National Views on Sugar Sweetened Beverages in Pakistan-2021 Opinion Poll; Pakistan Health Research Council-Ministry of National Health Services, Regulations and Coordination: Islamabad, Pakistan, 2021; Available online: https://panah.org.pk/publication/national-views-on-ssbs-in-pakistan-2021-opinion-poll/ (accessed on 16 September 2022).
- Luqman, M.; Hussain, R.; Yaseen, M.; Mehmood, M.U.; Asghar, I.; Saleem, U. Comparative Analysis of Dietary Intake Patterns of Rural and Urban Communities of Southern Punjab, Pakistan. Sarhad J. Agric. 2021, 37, 128–135. [Google Scholar] [CrossRef]
- Tanvir, S.; Sajjad, S.; Roshan, R. Awareness levels of prevention of cardiac diseases in general population of rawalpindi and requirement of health education. Public Health 2018, 157, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.; Saeeda, R.; Mudassar, I. Knowledge, attitude and practice regarding oral health among secondary school students of Azad Kashmir, Pakistan. Pakistan J. Public Health 2018, 8, 32–36. [Google Scholar]
- Sayed, S.A. A cross-sectional study on eating habits and food related beliefs and knowledge in university students of Karachi, Pakistan. Pak. J. Public Health 2012, 2, 36–42. [Google Scholar]
- Zuhaid, M.; Zahir, K.K.; Diju, I.U. Knowledge and perceptions of diabetes in urban and semi urban population of Peshawar, Pakistan. J. Ayub. Med. Coll. Abbottabad. 2012, 24, 105–108. [Google Scholar] [PubMed]
- Hussain, M.; Kiani, T.T.; Ghafoor, A.; Qadir, G. Role of genetic interactions in the inheritance of grain protein, tryptophan and lysine percentage in maize (Zea mays L.) under contrasting water regimes. J. Anim. Plant Sci. 2016, 26, 1002–1011. [Google Scholar]
- Hoteit, M.; Yazbeck, N.; Al-Jawaldeh, A.; Obeid, C.; Fattah, H.A.; Ghader, M.; Mohsen, H. Assessment of the knowledge, attitudes and practices of Lebanese shoppers towards food labeling: The first steps in the Nutri-score roadmap. F1000Research 2022, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health-Islamic Republic of Afghanistan. National Health Policy 2015–2020. 2015. Available online: https://www.acbar.org/upload/1493096331346.pdf (accessed on 15 September 2022).
- Buse, K.; Wafa, A.; Sadika, A.; Bui Phuong, L.; Haroun, C.; Minakshi, D.; Anam, F.; Sayad, H.; Akber Pradhan, N.; Iqbal, A.; et al. The state of diet-related NCD policies in Afghanistan, Bangladesh, Nepal, Pakistan, Tunisia and Vietnam: A comparative assessment that introduces a “policy cube” approach. Health Policy Plan 2020, 35, 503–521. [Google Scholar] [CrossRef]
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Action Plan for Control and Prevention of Non Communicable Diseases (2019–2030)-Bahrain. 2019. Available online: https://extranet.who.int/nutrition/gina/en/node/40324 (accessed on 15 September 2022).
- Al-Jawaldeh, A.; Hammerich, A.; Doggui, R.; Engesveen, K.; Lang, K.; McColl, K. Implementation of who recommended policies and interventions on healthy diet in the countries of the Eastern Mediterranean Region: From policy to action. Nutrients 2020, 12, 3700. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Eastern Mediterranean. Nutrition: Success stories. Available online: http://www.emro.who.int/nutrition/resources/success-stories.html (accessed on 15 September 2022).
- World Health Organization. Bahrain: NCD Joint Programming Mission: 15–17 May 2017; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/275763/WHO-NMH-NMA-18.90-eng.pdf?sequence=1&isAllowed=y (accessed on 15 September 2022).
- Al-Jawaldeh, A.; El-Mallah, C.; Obeid, O. Regional policies on sugar intake reduction at population levels to address obesity in the eastern Mediterranean. JSM Nutr. Disord. 2018, 2, 1006–1022. [Google Scholar]
- Sdralevich, M.C.A.; Sab, M.; Zouhar, M.Y.; Albertin, M.G. Subsidy Reform in the Middle East and North Africa: Recent Progress and Challenges Ahead; International Monetary Fund: Washington, DC, USA, 2014. [Google Scholar]
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Egypt National Multisectoral Action Plan for Prevention and Control of Noncommunicable Diseases (EgyptMAP-NCD). 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/25915 (accessed on 16 September 2022).
- Iqbal, F. Sustaining Gains in Poverty Reduction and Human Development in the Middle East and North Africa; World Bank Publications: Washington DC, USA, 2006. [Google Scholar]
- Abachizadeh, K.; Ostovar, A.; Pariani, A.; Raeisi, A. Banning advertising unhealthy products and services in Iran: A one-decade experience. Risk Manag. Healthc. Policy 2020, 13, 965. [Google Scholar] [CrossRef]
- Omidvar, N.; Al-Jawaldeh, A.; Amini, M.; Babashahi, M.; Abdollahi, Z.; Ranjbar, M. Food marketing to children in Iran: Regulation that needs further regulation. Curr. Res. Nutr. Food Sci. J. 2021, 9, 722–744. [Google Scholar] [CrossRef]
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Strategy for the Prevention and Control of Non-Communicable Diseases 2018–2022-Iraq. 2018. Available online: https://extranet.who.int/nutrition/gina/en/node/40323 (accessed on 16 September 2022).
- World Health Organization Regional Office for the Eastern Mediterranean. Country Cooperation Strategy for WHO and Oman 2021–2025; World Health Organization: Cairo, Egypt, 2021; Available online: https://applications.emro.who.int/docs/9789290228493-eng.pdf?ua=1 (accessed on 16 September 2022).
- Al-Awwad, N.J.; Ayoub, J.; Barham, R.; Sarhan, W.; Al-Holy, M.; Abughoush, M.; Al-Hourani, H.; Olaimat, A.; Al-Jawaldeh, A. Review of the Nutrition Situation in Jordan: Trends and Way Forward. Nutrients 2021, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Bin Sunaid, F.F.; Al-Jawaldeh, A.; Almutairi, M.W.; Alobaid, R.A.; Alfuraih, T.M.; Bin Saidan, F.N.; Alraqea, A.S.; Almutairi, L.A.; Bin Duhaim, A.N.; Alsaloom, T.A. Saudi Arabia’s healthy food strategy: Progress & hurdles in the 2030 road. Nutrients 2021, 13, 2130. [Google Scholar] [PubMed]
- Saudi Food and Drug Authority. Healthy Food Strategy. Vision 2030; SFDA: Riyadh, Saudi Arabia, 2018; Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/SAU_2017_SFDA-HealthyFoodStrategy.pdf (accessed on 16 September 2022).
- Alsukait, R.; Bleich, S.; Wilde, P.; Singh, G.; Folta, S. Sugary drink excise tax policy process and implementation: Case study from Saudi Arabia. Food Policy 2020, 90, 10. [Google Scholar] [CrossRef]
- General Authority of Zakat and Tax. Sin Taxation 2019; General Authority of Zakat and Tax: Riyadh, Saudi Arabia, 2019. [Google Scholar]
- Alhareky, M.; Bedi, S.; AlMulhim, A.; El Tantawi, M.; Farooqi, F.A.; AlHumaid, J. Impact of Sugar Tax on Sugar-sweetened Beverage Consumption among Saudi Schoolchildren. Oral Health Prev. Dent. 2021, 19, 189–194. [Google Scholar] [PubMed]
- Al-Jawaldeh, A.; Megally, R. Impact evaluation of soft drink taxes as part of nutrition policies in Gulf Cooperation Council countries: Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and United Arab Emirates. F1000Research 2021, 9, 1287. [Google Scholar] [CrossRef]
- Ministry of Finance-Lebanon. Wheat and Bread Subsidies 2007–2011. 2012. Available online: http://www.finance.gov.lb/en-us/Finance/Rep-Pub/DRI-MOF/Thematic%20Reports//Thematic%20Report%20Wheat%20subsidy%20Final%202.pdf (accessed on 30 August 2022).
- Consumers Lebanon. Proper Nutrition. Available online: http://consumerslebanon.org/Propernutrition (accessed on 30 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Stratégie Nationale Multisectorielle de Prévention et de Contrôle des Maladies Non Transmissibles 201–2029–Morocco. 2019. Available online: https://extranet.who.int/nutrition/gina/en/node/39426 (accessed on 30 August 2022).
- Belkhadir, J.; Brahimi, M.; Aguenaou, H.; Heikel, J.; El Berri, H.; Belakhal, L.; Mazzi, F.G.; Benabed, K. Taxation of Beverages and Sweetened Products in Morocco: A Major Achievement and a model to Follow in the Mena region. J. Med. Surg. Res. 2020, 7, 817–820. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Eastern Mediterranean. Maroc-Au Maroc, les Députés de la Chambre des Représentants Votent une Augmentation de 50% de la taxe sur les Boissons Sucrées. Available online: http://www.emro.who.int/fr/mor/morocco-infocus/au-maroc-les-deputes-de-la-chambre-des-representants-font-augmenter-de-50-la-taxe-sur-les-boissons-sucrees.html#:~:text=Il%20s’agit%20d’une,de%20sucre%20par%20100%20ml (accessed on 31 August 2022).
- Ministry of Health-Morocco. Programme National de Nutrition. 2019. Available online: https://www.sante.gov.ma/Documents/2019/06/Programme%20National%20de%20Nutrition.pdf (accessed on 31 August 2022).
- El Hourri, A. PLF2020. La “Taxe Sucre” Revient Dans les Debats Parlementaires. Available online: https://medias24.com/2019/11/07/plf2020-la-taxe-sucre-revient-dans-les-debats-parlementaires/ (accessed on 31 August 2022).
- Moroccan League for the Fight against Diabetes. Debate on Tax on High Sugar Products in Moroccan Parliament. Available online: http://www.lmlcd.com/index.php/taxe-sur-les-produits-tres-sucres-menu/english (accessed on 24 October 2022).
- Le Matin. PLF 2023: Une Nouvelle Taxe sur les Produits Contenant du Sucre. Available online: https://lematin.ma/express/2022/plf-2023-nouvelle-taxe-produits-contenant-sucre/382185.html (accessed on 15 November 2022).
- Challenge. PLF 2023. Les Principaux Amendements de la Première Partie Adoptés à la Chambre des Représentants. Available online: https://www.challenge.ma/plf-2023-les-principaux-amendements-de-la-premiere-partie-adoptes-a-la-chambre-des-representants-249306/ (accessed on 15 November 2022).
- Institut Marocain de Normalisation. Normalisation. Available online: https://www.imanor.gov.ma/ (accessed on 15 November 2022).
- Parlement de Maroc. La Chambre des Représentants adopte à la Majorité des Voix le Projet de loi de Finances 2023. Available online: https://www.chambredesrepresentants.ma/fr/actualites/la-chambre-des-representants-adopte-la-majorite-des-voix-le-projet-de-loi-de-finances (accessed on 15 November 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Oman Ministerial decree No. 112/2019 On Determining the Value and Types of Selective Goods and the Category of Tax Levied on Each. 2019. Available online: https://extranet.who.int/nutrition/gina/en/node/38194 (accessed on 31 August 2022).
- Ministry of Health-Oman; World Health Organization. National Nutrition Strategy and Framework for Action 2020–2030; Ministry of Health-Oman: Muscat, Oman; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Plan for the Prevention and Control of Chronic Non-Communicable Diseases 2016–2025-Oman. 2016. Available online: https://extranet.who.int/nutrition/gina/en/node/39383 (accessed on 31 August 2022).
- Mahmood, F. Subsidy on Export of Sugar. In State Bank of Pakistan. Available online: https://www.sbp.org.pk/epd/2015/FECL5.htm (accessed on 16 August 2022).
- Pakistan National Heart Association. Anti Sugary Drinks Campaign. Available online: https://panah.org.pk/sector/anti-sugary-drinks-campaign/ (accessed on 11 September 2022).
- Ministry of Health-Palestine. National Health Strategy 2017–2022; Assistant Deputy of Planning Affairs; General Directorate of Health Policies and Planning: 2017. Available online: https://site.moh.ps/Content/Books/OhV2yDbK3NBuMaBgzXrM13Tgf5Ek46VMsINeNQ9CvdRJ68xSIueheN_CUmin4TqPtVNgd7v3aBpOzbD57AZWl5OPlGu6RsGzmnu3mNE745Rr5.pdf (accessed on 17 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Qatar National Nutrition and Physical Activity Action Plan 2017–2022. 2017. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/QAT_2017_Action%20Plan%202017-2022-FINAL.pdf (accessed on 17 August 2022).
- General Tax Authority. Establishment of General Tax Authority. Available online: https://gta.gov.qa/en/establishment-of-general-tax-authority/ (accessed on 16 June 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Stratégie Nationale Multisectorielle de Prévention et Contrôle des Maladies Non Transmissibles (MNT)-Tunisia. 2018. Available online: https://extranet.who.int/nutrition/gina/en/node/39424 (accessed on 17 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Plan to Combat Childhood Obesity United Arab Emirates-UAE. 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/39385 (accessed on 18 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Plan for Prevention and Response For Noncommunicable Diseases State of United Arab Emirates. 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/38165 (accessed on 18 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Action Plan in Nutrition-UAE. 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/37425 (accessed on 18 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-The National Plan for Prevention and Response to NCDs 2017–2021-UAE. 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/40336 (accessed on 18 August 2022).
- Federal Tax Authority-UAE. Excise Tax. Available online: https://u.ae/en/information-and-services/finance-and-investment/taxation/excise-tax (accessed on 12 August 2022).
- Klaus-Stefan, E.; Choueiri, N.; Sobolev, Y.; Walliser, J. Republic of Yemen: Selected Issues; International Monetary Fund: Washington, DC, USA, 2001. [Google Scholar]
- Food and Agriculture Organization of the United Nations; Ministry of Public Health; Ministry of Agriculture Irrigation and Livestock; Ministry of Education. National Food-Based Dietary Guidelines for Afghans; Food and Agriculture Organization of the United Nations: Kabul, Afghanistan, 2016; Available online: https://www.fao.org/3/i5283e/i5283e.pdf (accessed on 19 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Food Canteen List for the Academic year 2016–2017-Bahrain; Public Health Directorate, Nutrition Section: 2016. Available online: https://extranet.who.int/nutrition/gina/en/node/63348 (accessed on 19 August 2022).
- World Health Organization Regional Office for the Eastern Mediterranean. Implementing the WHO Recommendations on the Marketing of Food and Non-Alcoholic Beverages to Children in the Eastern Mediterranean Region; World Health Organization: Cairo, Egypt, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/328213/EMROPUB_2018_2248_en.pdf?sequence=1&isAllowed=y (accessed on 20 June 2022).
- World Action on Salt Sugar and Health. World Action-Middle East: Iran. Available online: https://www.worldactiononsalt.com/worldaction/middle-east/iran/ (accessed on 20 June 2022).
- Ministry of Health and Medical Education. Food-Based Dietary Guidelines-Iran. 2015. Available online: https://www.fao.org/nutrition/education/food-dietary-guidelines/regions/countries/iran/en/ (accessed on 19 August 2022).
- Moslemi, M.; Kheirandish, M.; Mazaheri, R.N.F.; Hosseini, H.; Jannat, B.; Mofid, V.; Moghaddam, A.; Karimian, N. National food policies in the Islamic Republic of Iran aimed at control and prevention of noncommunicable diseases. East Mediterr. Health J. 2020, 26, 1556–1564. [Google Scholar] [CrossRef]
- Zargaraan, A.; Dinarvand, R.; Hosseini, H. Nutritional traffic light labeling and taxation on unhealthy food products in Iran: Health policies to prevent non-communicable diseases. Iran. Red Crescent. Med. J. 2017, 19, e57874. [Google Scholar]
- Hajifaraji, M.; Abdollahi, Z. The Challenges and Successes of Salt, Sugar and Fat Reduction Program to Prevent Ncds (Iran Experiences); Karger: Basel, Switzerland, 2017. [Google Scholar]
- Al-Jawaldeh, A.; Rayner, M.; Julia, C.; Elmadfa, I.; Hammerich, A.; McColl, K. Improving nutrition information in the eastern Mediterranean region: Implementation of front-of-pack nutrition labelling. Nutrients 2020, 12, 330. [Google Scholar] [CrossRef]
- Edalati, S.; Omidvar, N.; Haghighian Roudsari, A.; Ghodsi, D.; Zargaraan, A. Development and implementation of nutrition labelling in Iran: A retrospective policy analysis. Int. J. Health Plan. Manag. 2020, 35, e28–e44. [Google Scholar] [CrossRef]
- Ministry of Health and Medical Education. National Guidelines for Healthy Nutrition Canteen in Schools; Ministry of Health and Medical Education: Tehran, Iran, 2017. [Google Scholar]
- Babashahi, M.; Omidvar, N.; Joulaei, H.; Zargaraan, A.; Zayeri, F.; Veisi, E.; Doustmohammadian, A.; Kelishadi, R. Scrutinize of healthy school canteen policy in Iran’s primary schools: A mixed method study. BMC Public Health 2021, 21, 1566. [Google Scholar] [CrossRef]
- United Nations-Jordan. Policy Brief: Healthy Diets for All in Jordan. 2021. Available online: https://jordan.un.org/sites/default/files/202204/Policy%20Brief%20_Healthy%20Diets%20for%20All%20in%20Jordan%20_%20April%202022_0.pdf (accessed on 1 September 2022).
- Ministry of Health-Jordan. Low Salt, Low Sugar, Low Saturated and Trans Fat Consumption Guideline for Health Care Providers for Training of Trainees (TOT) and Pamphlet for Consumers; Ministry of Health: Amman, Jordan, 2015. [Google Scholar]
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-2012 Health Requirements for School Canteens and Foods Allowed and Prohibited to Be Sold for the Year 2012-Jordan. 2012. Available online: https://extranet.who.int/nutrition/gina/en/node/63351 (accessed on 1 September 2022).
- Ministry of Health-Jordan. Food-Based Dietary Guidelines for Jordanians; Nutrition Department: Amman, Jordan, 2020. Available online: https://www.moh.gov.jo/EchoBusV3.0/SystemAssets/PDFs/Jordan%20Guide%20Book_Website.pdf (accessed on 1 September 2022).
- Ministry of Health-KSA. Dietary Guidelines for Saudis: The Healthy Food Palm; General Directorate of Nutrition: Ministry of Health, 2012. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Documents/final%20english%20%20%D8%A7%D9%84%D9%83%D8%AA%D8%A7%D8%A8%20%D8%A7%D9%84%D8%B9%D9%84%D9%85%D9%8A%20%D8%A5%D9%86%D8%AC%D9%84%D9%8A%D8%B2%D9%8A.pdf (accessed on 1 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-A guide for Healthy Food Terms and Conditions in Government Subsistence Purchase Contracts-KSA. 2019. Available online: https://extranet.who.int/nutrition/gina/en/node/40344 (accessed on 1 September 2022).
- Moussa, H. Food and Agricultural Import Regulations and Standards Country Report, 1st ed.; United States Department of Agriculture Foreign Agriculture Service and Global Agriculture Information Network: Washington, DC, USA, 2020. [Google Scholar]
- Saudi Food and Drug Authority (SFDA). FD 5001: Fresh Juices, Mixes and Beverages, Sold at Juice Stores, Restaurants and Cafes; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2019. [Google Scholar]
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). An Initiative to Promote Public Health through Food in the Work Environment. 2019. Available online: https://extranet.who.int/nutrition/gina/en/node/41574 (accessed on 1 September 2022).
- Saudi Food and Drug Authority. SFDA.FD 42: Traffic Light Labeling; Saudi Food and Drug Authority: Al Hittin, Saudi Arabia, 2018. [Google Scholar]
- The Public Authority for Food and Nutrition-Kuwait. The Case for Investment in Prevention and Control of Non-Communicable Diseases in Kuwait; The Public Authority for Food and Nutrition: Sabah Al Salem, Kuwait, 2020. [Google Scholar]
- GCC Standardization Organization. GSO 2233:2012-Requirements of Nutritional Labeling. 2012. Available online: https://www.gso.org.sa/store/standards/GSO:589563/GSO%202233:2012?lang=en (accessed on 1 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Strategy for the Prevention and Response to Chronic Noncommunicable Diseases in the State of Kuwait 2017–2025. 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/40355 (accessed on 1 September 2022).
- American University of Beirut. Food-Based Dietary Guidelines-Lebanon; Faculty of Agricultural and Food Sciences: Beirut, Lebanon, 2013; Available online: https://www.aub.edu.lb/fafs/nfsc/Documents/FBDG%20English%20Version.pdf (accessed on 2 September 2022).
- LIBNOR. General Standard for the Labelling of Prepackaged Foods-NL 206:2017. 2017. Available online: http://www.libnor.gov.lb/CatalogDetails.aspx?id=6389&language=en (accessed on 2 September 2022).
- LIBNOR. Guidelines for Use of Nutrition and Health Claims-NL 661:2017. 2017. Available online: http://www.libnor.gov.lb/CatalogDetails.aspx?id=6391&language=en (accessed on 2 September 2022).
- National Center for Disease Control. Dietary Guidelines for Chronic Diseases in Libya. 2021. Available online: https://ncdc.org.ly/Ar/ (accessed on 2 September 2022).
- Ministry of Health-Morocco. National Health Plan 2025. 2018. Available online: http://www.draatafilalet.ma/images/Publications-pdf/Plan-de-sant%C3%A9-2025.pdf (accessed on 2 September 2022).
- Office National de Sécurité Sanitaire des Produits Alimentaires. Réglementation: Étiquetage des Produits Alimentaires. Available online: http://www.onssa.gov.ma/fr/reglementation-etiquetage-des-produits-alimentaires (accessed on 31 August 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Dietary and Health Guidelines for the Preparation of Menus in School Canteens and Boarding Schools-Morocco. 2013. Available online: https://extranet.who.int/nutrition/gina/en/node/63353 (accessed on 19 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Dietary and Health Guidelines for the Preparation of Menus at the Level of University Residences and Boarding Schools of Higher Education Establishments-Morocco. 2013. Available online: https://extranet.who.int/nutrition/gina/en/node/66522 (accessed on 19 September 2022).
- S.A. Boissons Sucrées: Vers une Augmentation de la Taxe au Maroc. Available online: https://www.bladi.net/taxe-boissons-sucrees-maroc,91129.html (accessed on 31 August 2022).
- Taybouta, R. La Taxation du Sucre Remise sur la Table de L’exécutif. Available online: https://www.lopinion.ma/La-taxation-du-sucre-remise-sur-la-table-de-l-Executif_a24799.html (accessed on 31 August 2022).
- Aguenaou, H.; El Ammari, L.; Bigdeli, M.; El Hajjab, A.; Lahmam, H.; Labzizi, S.; Gamih, H.; Talouizte, A.; Serbouti, C.; El Kari, K. Comparison of appropriateness of Nutri-Score and other front-of-pack nutrition labels across a group of Moroccan consumers: Awareness, understanding and food choices. Arch. Public Health 2021, 79, 71. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health-Oman. The Omani Guide to Healthy Eating; Department of Nutrition: Muscat, Oman, 2009; Available online: https://www.fao.org/3/as845e/as845e.pdf (accessed on 19 September 2022).
- Government of Pakistan and Food and Agriculture Organization of the United Nations. Pakistan Dietary Guidelines for Better Nutrition; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy; Ministry of Planning Development and Reform, Government of Pakistan: Islamabad, Pakistan, 2019.
- Al-Jawaldeh, A.; Jabbour, J. Marketing of Food and Beverages to Children in the Eastern Mediterranean Region: A Situational Analysis of the Regulatory Framework. Front. Nutr. 2022, 9, 868937. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health-Palestine. Food-Based Dietary Guidelines-Palestine. 2021. Available online: https://www.moh.gov.ps/portal/ (accessed on 2 September 2022).
- World Action on Salt Sugar and Health. World Action-Middle East: Qatar. Available online: https://www.worldactiononsalt.com/worldaction/middle-east/qatar/ (accessed on 17 June 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-List of Food Items in School Canteens-Qatar. 2016. Available online: https://extranet.who.int/nutrition/gina/en/node/63352 (accessed on 16 June 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Food Safety and Health Guide-Qatar. 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/57256 (accessed on 16 June 2022).
- Qatar University. QU Launches ‘Smart Start Campaign’ to Promote Child Health Awareness for Second Year Running. Available online: http://www.qu.edu.qa/newsroom/Qatar-University/QU-launches-%E2%80%98Smart-Start-Campaign%E2%80%99-to-promote-child-health-awareness-for-second-year-running (accessed on 16 June 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Guidance for Supervisors of School Canteens for the Academic Year 2018–2019-Qatar. 2018. Available online: https://extranet.who.int/nutrition/gina/en/node/57257 (accessed on 16 June 2022).
- Supreme Council of Health. Food-Based Dietary Guidelines-Qatar; Public Health Department: Doha, Qatar, 2015; Available online: https://www.fao.org/nutrition/education/food-dietary-guidelines/regions/countries/qatar/en/ (accessed on 16 June 2022).
- Ministry of Health and Human Services-Federal Republic of Somalia. Somalia Nutrition Strategy 2020–2025. 2020. Available online: https://www.unicef.org/somalia/media/1756/file/Somalia-nutrition-strategy-2020-2025.pdf (accessed on 17 June 2022).
- Ministry of Health-Sudan. National Nutrition Strategic Plan 2014–2025. 2014. Available online: https://scalingupnutrition.org/wp-content/uploads/2016/08/4.-Sudan-National_nutrition_strategic_Plan.pdf (accessed on 17 June 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Arrêté des Ministres du Commerce et de L’artisanat, de la Santé Publique, de L’industrie, de L’énergie et des Petites et Moyennes Entreprises du 3 Septembre 2008, Relatif à L’étiquetage et la Présentation des Denrées Alimentaires Préemballées-Tunisia. 2008. Available online: https://extranet.who.int/nutrition/gina/en/node/25405 (accessed on 17 June 2022).
- Abu Dhabi Quality and Conformity Council. Specification for Using Weqaya Food Program (ADS13/2018); Abu Dhabi Quality and Conformity Council: Abu Dhabi, United Arab Emirates, 2015. Available online: https://qcc.gov.ae//media/Project/QCC/QCC/Documents/Quality-Infrastructure-Documents/Abu-Dhabi-Specification/Abu-DhabiSpecifications/ADS-13---Specification-for-using-Wegaya-Food-program.pdf (accessed on 15 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Guideline to Healthy and Nutritious Food Practices in School Canteens-Dubai. 2011. Available online: https://extranet.who.int/nutrition/gina/en/node/63349 (accessed on 15 September 2022).
- Ministry of Health and Prevention. Food-Based Dietary Guidelines-united Arab Emirates; Ministry of Health and Prevention: 2019. Available online: https://www.fao.org/nutrition/education/food-dietary-guidelines/regions/countries/united-arab-emirates/en/ (accessed on 15 September 2022).
- Ministry of Community Development-UAE. National Program for Happiness and Wellbeing Launches Nutrition Labelling Policy. Available online: https://www.hw.gov.ae/en/news/to-promote-healthy-lifestyle-and-wellbeing-in-the-uae-national-program-for-happiness-and-wellbeing-launches-nutrition-labelling-policy (accessed on 15 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-School Canteen Guidelines of the Emirate of Abu Dhabi. 2011. Available online: https://extranet.who.int/nutrition/gina/en/node/63350 (accessed on 15 September 2022).
- Department of Health-Abu Dhabi. DOH Guideline for Vending Machines and Retail Items in Health Care Facilities. 2021. Available online: https://www.doh.gov.ae/-/media/83D7717CABB142A69721665A3A7D5526.ashx (accessed on 15 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-the National Strategy and Plan of Action Against Diabetes, Hypertension, Dyslipidemia And Obesity in Jordan-Jordan. 2015. Available online: https://extranet.who.int/nutrition/gina/en/node/25926 (accessed on 16 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Obesity Control Program-KSA. 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/39427 (accessed on 16 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-National Executive Plan for NCDs (2014–2025)-KSA. 2014. Available online: https://extranet.who.int/nutrition/gina/en/node/41465 (accessed on 16 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-The National Strategy for Healthy Food and Physical Activity 2015–2025-KSA. 2015. Available online: https://extranet.who.int/nutrition/gina/en/node/39384 (accessed on 16 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-KSA National Strategy for Diet and Physical Activity for the Years 2014–2025-KSA. 2014. Available online: https://extranet.who.int/nutrition/gina/en/node/40059 (accessed on 16 September 2022).
- World Health Organization Global Database on the Implementation of Nutrition Action (GINA). Policy-Prevention des Maladies Non Transmissibles: Plan d’action multisectoriel pour la Promotion d’un Mode de vie sain 2015–2020-Morocco. 2015. Available online: https://extranet.who.int/nutrition/gina/en/node/36194 (accessed on 16 September 2022).
- World Health Organization Regional Office for the Eastern Mediterranean. Nutrient Profile Model for the Marketing of Food and Non-Alcoholic Beverages to Children in the WHO Eastern Mediterranean Region; World Health Organization Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2017; Available online: https://apps.who.int/iris/bitstream/handle/10665/255260/EMROPUB_2017_en_19632.pdf?sequence=1&isAllowed=y (accessed on 20 October 2022).
- Babashahi, M.; Omidvar, N.; Joulaei, H.; Zargaraan, A.; Veisi, E.; Kelishadi, R. Food Products with the Child-Targeted Packaging in Food Stores around Primary Schools in Tehran, Iran. J. Prev. 2022, 43, 513–527. [Google Scholar] [CrossRef] [PubMed]
- Al-Awwad, N.J.; Al-Sayyed, H.F.; Safi, H.; Al-Bosta, S.M.; Al-Zawawi, S. Highlights on the Labels of Packaged Foods Sold in Jordanian Market from A Cross-Sectional Study. Curr. Res. Nutr. Food Sci. 2021, 9, 770. [Google Scholar] [CrossRef]
- Aldubayan, K.; Murimi, M. Compliance with school nutrition policy in Saudi Arabia: A quantitative study. East Mediterr. Health J. 2019, 25, 230–238. [Google Scholar] [CrossRef]
- Mokari-Yamchi, A.; Omidvar, N.; Zarandi, M.T.; Eini-Zinab, H. The Effects of Food Taxes and Subsidies on Promoting Healthier Diets in Iranian Households. Front. Nutr. 2022, 9, 917932. [Google Scholar] [CrossRef]
- Jalloun, R.A.; Qurban, M.A. The impact of taxes on soft drinks on adult consumption and weight outcomes in Medina, Saudi Arabia. Hum. Nutr. Metab. 2022, 27, 200139. [Google Scholar] [CrossRef]
- Alsukait, R.; Wilde, P.; Bleich, S.; Singh, G.; Folta, S. Impact of Saudi Arabia’s sugary drink tax on prices and purchases. Curr. Dev. Nutr. 2019, 3, nzz034.P10-066-19. [Google Scholar] [CrossRef]
- Megally, R.; Al-Jawaldeh, A. Impact of sin taxes on consumption volumes of sweetened beverages and soft drinks in Saudi Arabia. F1000Research 2021, 9, 1117. [Google Scholar] [CrossRef] [PubMed]
- Story, M.T.; Duffy, E. Supporting healthy eating: Synergistic effects of nutrition education paired with policy, systems, and environmental changes. In Nutrition Education: Strategies for Improving Nutrition and Healthy Eating in Individuals and Communities; Karger Publishers: Basel, Switzerland, 2020; pp. 69–81. [Google Scholar]
- Hyseni, L.; Bromley, H.; Kypridemos, C.; O’Flaherty, M.; Lloyd-Williams, F.; Guzman-Castillo, M.; Pearson-Stuttard, J.; Capewell, S. Systematic review of dietary trans-fat reduction interventions. Bull. World Health Organ. 2017, 95, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Tomaino, L.; Dernini, S.; Berry, E.M.; Lairon, D.; Ngo de la Cruz, J.; Bach-Faig, A.; Donini, L.M.; Medina, F.-X.; Belahsen, R. Updating the mediterranean diet pyramid towards sustainability: Focus on environmental concerns. Int. J. Environ. Res. Public Health 2020, 17, 8758. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.L.; Raheem, D.; Ramos, F.; Carrascosa, C.; Saraiva, A.; Raposo, A. Highlights of current dietary guidelines in five continents. Int. J. Environ. Res. Public Health 2021, 18, 2814. [Google Scholar] [CrossRef]
- World Health Organization. Global Nutrition Policy Review 2016–2017: Country Progress in Creating Enabling Policy Environments for Promoting Healthy Diets and Nutrition; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/publications/i/item/9789241514873 (accessed on 20 October 2022).
- Epel, E.S.; Hartman, A.; Jacobs, L.M.; Leung, C.; Cohn, M.A.; Jensen, L.; Ishkanian, L.; Wojcicki, J.; Mason, A.E.; Lustig, R.H.; et al. Association of a Workplace Sales Ban on Sugar-Sweetened Beverages With Employee Consumption of Sugar-Sweetened Beverages and Health. JAMA Intern. Med. 2020, 180, 9–16. [Google Scholar] [CrossRef]
- World Health Organization. Global Action plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/bitstream/handle/10665/94384/?sequence=1 (accessed on 20 October 2022).
- Mantilla Herrera, A.M.; Crino, M.; Erskine, H.E.; Sacks, G.; Ananthapavan, J.; Mhurchu, C.N.; Lee, Y.Y. Cost-effectiveness of product reformulation in response to the health star rating food labelling system in Australia. Nutrients 2018, 10, 614. [Google Scholar] [CrossRef]
- Griffith, R.; O’Connell, M.; Smith, K. The importance of product reformulation versus consumer choice in improving diet quality. Economica 2017, 84, 34–53. [Google Scholar] [CrossRef]
- Spiteri, M.; Soler, L.-G. Food reformulation and nutritional quality of food consumption: An analysis based on households panel data in France. Eur. J. Clin. Nutr. 2018, 72, 228–235. [Google Scholar] [CrossRef]
- Combris, P.; Enderli, G.; Gauvreau, C. Public and private actions for improving the nutritional quality of foods: Impacts and limits. Cah. Nutr. Diététique 2014, 49, 22–31. [Google Scholar] [CrossRef]
- Briggs, A.D.; Mytton, O.T.; Kehlbacher, A.; Tiffin, R.; Elhussein, A.; Rayner, M.; Jebb, S.A.; Blakely, T.; Scarborough, P. Health impact assessment of the UK soft drinks industry levy: A comparative risk assessment modelling study. Lancet Public Health 2017, 2, e15–e22. [Google Scholar] [CrossRef] [PubMed]
- Morley, B.C.; Niven, P.H.; Dixon, H.G.; Swanson, M.G.; McAleese, A.B.; Wakefield, M.A. Controlled cohort evaluation of the LiveLighter mass media campaign’s impact on adults’ reported consumption of sugar-sweetened beverages. BMJ Open 2018, 8, e019574. [Google Scholar] [CrossRef] [PubMed]
- Farley, T.A.; Halper, H.S.; Carlin, A.M.; Emmerson, K.M.; Foster, K.N.; Fertig, A.R. Mass media campaign to reduce consumption of sugar-sweetened beverages in a rural area of the United States. Am. J. Public Health 2017, 107, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Penalvo, J.L.; Del Gobbo, L.; Silva, J.; Michaelson, M.; O’Flaherty, M.; Capewell, S.; Spiegelman, D.; Danaei, G.; Mozaffarian, D. The prospective impact of food pricing on improving dietary consumption: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0172277. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Countdown to 2023: WHO Report on Global Trans-Fat Elimination 2019; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/331300/9789241516440-eng.pdf?sequence=1&isAllowed=y (accessed on 21 October 2022).
- Bucher Della Torre, S.; Moullet, C.; Jotterand Chaparro, C. Impact of Measures Aiming to Reduce Sugars Intake in the General Population and Their Implementation in Europe: A Scoping Review. Int. J. Public Health 2022, 111, 1604108. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Module 1: Review. How-to guide for landscape assessment and roadmap development for elimination of trans fats. In REPLACE Trans Fat: An Action Package to Eliminate Industrially Produced Trans-Fatty Acids; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/docs/default-source/replace-transfat/replace-module-1-re.pdf?sfvrsn=1885eaed_2 (accessed on 21 October 2022).
- Hussain, M.; Perna, S.; Mandeel, Q.; Naser, J.; Alalwan, T. Awareness and Consumption Pattern of Energy Drinks Among Bahraini Youth. Bahrain Med. Bull. 2021, 43, 423–430. [Google Scholar]





| Country | Taxation | Subsidies | Marketing Regulations |
|---|---|---|---|
| Afghanistan | Name of initiative: National Health Policy 2015–2020 | - | - |
| Year: 2015 | |||
| Leadership: Led by the government (MOPH) | |||
| Approach and target: Taxation on drinks with AS will be considered (not adopted) [117,118]. | |||
| Bahrain | Name of initiative: National Action Plan for control and prevention of Non communicable diseases (2019–2030) | Name of initiative: NCD Joint Programming Mission | Name of initiative: National Action Plan for control and prevention of Non communicable diseases (2019–2030) |
| Year: 2019 | Year: 2017 | Year: 2019 | |
| Leadership: Led by the government (MOH) | Leadership: Led by the government (MOH) | Leadership: Led by the government (MOH) | |
| Approach and target: Mandatory: Taxation on energy drinks and carbonated beverages [119]; reaching 100% on energy drinks and 50% on SSBs [120,121]. | Approach and target: Remove subsidies on locally produced juices (not adopted) [122]. | Approach: Policies to reduce the impact of marketing of foods and nonalcoholic beverages high in FS, on children (not adopted) [119]. | |
| Djibouti | - | Name of initiative: Sugar subsidies law | - |
| Year: NA | |||
| Leadership: NA | |||
| Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,124]. | |||
| Egypt | Name of initiative: National Multisectoral Action Plan for Prevention and Control of Noncommunicable Diseases | Name of initiative: Sugar subsidies law | - |
| Year: 2017 | Year: NA | ||
| Leadership: Led by the government (MOHAP) | Leadership: NA | ||
| Approach and target: Taxation on SSBs to reduce sugar consumption (not adopted) [125]. | Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,124]. | ||
| Iran | Name of initiative: Sweetened beverage tax | Name of initiative: Sugar subsidies law | Name of initiative: 5th national development plan (2011–2016) |
| Year: NA | Year: NA | Year: 2011 | |
| Leadership: NA | Leadership: NA | Leadership: Led by the government | |
| Approach and target: Tax of 10% on local soft drinks and 15% on imported ones; to reach 20% on SSBs [120]. | Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,126]. | Approach: Marketing foods with AS is forbidden. Soft drinks and 19 unhealthy food products (such as edible ice products, toffee and candy) have been banned [127,128]. | |
| Iraq | - | - | Name of initiative: National strategy for the prevention and control of non-communicable diseases 2018–2022 |
| Year: 2018 | |||
| Leadership: Led by the government (MOH, Ministry of Justice and the parliament) | |||
| Approach and target: Limiting the marketing of food items that are high in monosaccharides, to children [129]. | |||
| Jordan | - | Name of initiative: Sugar subsidies law | Name of initiative: National Framework of Action on Obesity Prevention in Jordan 2018–2023 |
| Year: NA | Year: 2019 | ||
| Leadership: NA | Leadership: Led by the government (MOH), in collaboration with Jordan Food and Drug Administration, Jordan Standards and Metrology Organization, Ministry of Education, Amman Municipality, Ministry of Youth, Ministry of Industry and Trade, the Royal Medical Services, Ministry of Planning and the University of Jordan | ||
| Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,124]. | Approach: Mandatory: Restrict marketing of foods high in sugar [121,130,131]. | ||
| KSA | Name of Initiative: Sin Taxation | - | - |
| Year: 2017 | |||
| Leadership: Led by the government (SFDA) | |||
| Approach and target: Mandatory: Taxation was imposed by the General Authority of Zakat, Tax and Customs (GZAT) as of 2017; Enforcement of a flat tax (in 2019) of 50% on SSBs, including carbonated drinks, juices, and dairy products and 120% on energy drinks. In 2018, an additional 5% taxation was implemented on beverages [120,121,132,133,134,135,136]. | |||
| Kuwait | Name of initiative: Taxation | - | - |
| Year: 2020 | |||
| Leadership: Led by the GCC Standardization Organization | |||
| Approach and target: Implementing excise tax on SSBs (50% on carbonated beverages and 100% on energy drinks) [137]. | |||
| Lebanon | - | Name of initiative: Sugar subsidies law | Name of initiative: NA |
| Year: NA | Year: NA | ||
| Leadership: NA | Leadership: Led by Consumers Lebanon | ||
| Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,138]. | Approach: Advocacy with the Association of Lebanese Artists to refrain from participation in the creation of advertisements that promote foods high in sugar [139]. | ||
| Morocco | Name of initiative: National Multisectoral Strategy for the Prevention and Control of Non-Communicable Diseases 2019–2029 | Name of initiative: Sugar subsidies law | Name of initiative: National Nutrition Program; National Multisectoral Strategy for the Prevention and Control of Non-Communicable Diseases 2019–2029 |
| Year: 2019 | Year: NA | Year: 2019 | |
| Leadership: Led by the government (MOH) and General Directorate of Customs and parliament | Leadership: Led by the parliament | Leadership: Led by the government (MOH) | |
| Approach and target: Tax on SSBs are 50% [120,140]; the soda tax was adopted by the Moroccan Parliament in the 2019 finance bill [141,142]. | Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,124]. | Approach: Regulate the marketing of high-sugar products [140,143]. | |
| Name of initiative: Progressive taxation | |||
| Year: 2020 | |||
| Leadership: Led by the government (Ministry of Finance) and parliament | |||
| Approach and target: A progressive taxation on sugary drinks in proportion to the quantity of AS (threshold of 5 g/100 mL) [144]. | |||
| Name of initiative: Excise tax | |||
| Year: 2022 | |||
| Leadership: Led by the government (MOH) and parliament | |||
| Approach and target: The sugar tax has been adopted by the moroccan parliament in the 2023 finance bill (11 November 2023). It includes processed products containing sugar such as cookies, industrial pastry, wafers, breakfast cereals, cereal bars, dairy products, drink yogurt, milk desserts, sweetened condensed milk, chocolates, confectionery [145,146,147,148,149]. | |||
| Oman | Name of initiative: Oman Ministerial decree No. 112/2019 on determining the value and types of selective goods and the category of tax levied on each | Name of initiative: National plan for the prevention and control of chronic non-communicable diseases 2016–2025 | Name of initiative: National plan for the prevention and control of chronic non-communicable diseases 2016–2025 |
| Year: 2019 | Year: 2016 | Year: 2016 | |
| Leadership: Led by the government (Ministry of Finance) | Leadership: Led by the government (MOH) | Leadership: Led by the government (MOH) | |
| Approach and target: Mandatory: Taxation on SSBs (fruit juices and nectars, energy drinks, canned and prepared coffee and tea beverages) and carbonated beverages; 100% for energy drinks and 50% for soft drinks; to be increased to 100% for SSBs [150,151]. | Approach and target: Gradually shift subsidization from sugars and unhealthy fats to healthy foods instead–to reach 100% by 2025 (not adopted) [152]. | Approach: Prevent marketing of non-healthy food for children by 2025 (not implemented) [152]. | |
| Name of initiative: Policy statement for sugar reduction | |||
| Year: 2022 | |||
| Leadership: Led by the government (MOH) | |||
| Approach and target: Voluntary: Meetings with companies have been conducted during the months of July and October 2022; Taxation on high-sugar products (needs to be finalized). | |||
| Pakistan | Name of initiative: National Action Plan for Reduction of Dietary Risks of NCDs for Pakistan | Name of initiative: Sugar subsidies law | Name of initiative: NA |
| Year: 2022 (Planned) | Year: NA | Year: NA | |
| Leadership: Led by the government (Ministry of National Health Services, Regulation and Coordination), in collaboration with the WHO | Leadership: NA | Leadership: Led by the Punjab Food Authority | |
| Approach and target: Will be mandatory for all foods and snacks (bakery products, breakfast cereals, desserts, puddings and ice cream, SSBs, biscuits and cakes, ultra-processed foods): Approach includes taxation for high sugar products. | Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,153]. | Approach and target: Marketing of energy drinks has been banned in the geographic limits of the province. | |
| Information provided by the NFP | Information provided by the NFP | ||
| Name of initiative: Saving Youth from Sugar-sweetened Beverages through Education, Media, and Advocacy (SYSTEM) | |||
| Year: 2020 | |||
| Leadership: Pakistan National Heart Association; in collaboration with MOH, MOF, Federal Board of Revenue and other policy makers | |||
| Approach and target: Advocate for SSB taxation [154]. | |||
| Palestine | Name of initiative: NA | - | Name of initiative: National Health Strategy 2017–2022 |
| Year: 2022 | Year: 2017 | ||
| Leadership: Led by the government (Ministry of Finance and Planning) | Leadership: Led by the government (MOH) in cooperation with all health sector stakeholders | ||
| Approach and target: Planned taxation on carbonated beverages, energy drinks, sweetened juices and juice concentrates. | Approach: Planned mandatory technical instructions regulating the marketing of foods containing high sugar content (planned; not implemented yet) [155]. | ||
| Information provided by the NFP | |||
| Qatar | Name of initiative: Qatar National Nutrition and Physical Activity Action Plan 2017–2022 | Name of initiative: Qatar National Nutrition and Physical Activity Action Plan 2017–2022 | Name of initiative: Qatar National Nutrition and Physical Activity Action Plan 2017–2022 |
| Year: 2017 | Year: 2017 | Year: 2017 | |
| Leadership: Led by the government (MOPH) | Leadership: Led by the government (MOPH) | Leadership: Led by the government (MOPH) | |
| Approach and target: Taxation to raise the price of sweetened soft drinks and beverages [156]. | Approach and target: Progressive elimination of any subsidies for sugar-rich food items [156]. | Approach: Restrict the marketing, advertising and sponsorship across all media (including digital) platforms for all sugar-rich foods and drinks to children and adults (not adopted); actions to limit price promotions on foods high in sugar in supermarkets, catering or street markets [156]. | |
| Name of Initiative: Establishment of General Tax Authority | |||
| Year: 2018 | |||
| Leadership: Led by the government (MOF) | |||
| Approach and target: Mandatory: Impose 100% tax on energy drinks and 50% tax on sugary drinks [120,157]. | |||
| Name of initiative: Taxation for high sugar products | |||
| Year: Planned | |||
| Leadership: Led by the government | |||
| Approach and target: Taxation on bakery products, desserts, SSBs, biscuits and cakes. | |||
| Information provided by the NFP | |||
| Sudan | - | Name of initiative: Sugar subsidies law | - |
| Year: NA | |||
| Leadership: NA | |||
| Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,124]. | |||
| Tunisia | Name of initiative: NA | Name of initiative: Sugar subsidies law | - |
| Year: 2014 | Year: NA | ||
| Leadership: Led by the government (Ministry of Commerce) | Leadership: NA | ||
| Approach and target: Prices of sugar have been increased first for the food industry and then for the consumer [158]. | Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,126]. | ||
| Name of initiative: National Obesity Control and Prevention | |||
| Year: 2017 | |||
| Leadership: Led by the government (Ministry of Commerce) with the cooperation of industries | |||
| Approach and target: Taxation on SSBs [118,120,158]. | |||
| UAE | Name of initiative: National Plan to Combat Childhood Obesity United Arab Emirates; National Plan for Prevention and Response For noncommunicable diseases; National Action Plan in Nutrition | Name of initiative: National Action Plan in Nutrition; National Plan for Prevention and Response to NCDs 2017–2021 | Name of initiative: National Plan to Combat Childhood Obesity United Arab Emirates |
| Year: 2017 | Year: 2017 | Year: 2017 | |
| Leadership: Led by the government (MOHAP–Department of Health Education and Promotion) | Leadership: Led by the government (MOHAP) | Leadership: Led by the government (MOHAP–Department of Health Education and Promotion) | |
| Approach and target: Implement taxes on SSBs according to the WHO guidance [159,160,161]. | Approach and targets: Government subsidies on high-sugar foods removed [161,162]. | Approach: Limit the consumption of foods and beverages high in sugar, to infants and young children through marketing regulations that are in line with the WHO recommendations (not adopted) [159]. | |
| Name of initiative: Cabinet Decision No. 52 of 2019 on Excise Goods, Excise Tax Rates and the Methods of Calculating the Excise Price | |||
| Year: 2019 | |||
| Leadership: Led by the government (Federal Tax Authority) | |||
| Approach and targets: 50% on carbonated beverages; 100% on energy drinks; 50% on any product with AS or other sweeteners [120,163]. | |||
| Yemen | - | Name of initiative: Sugar subsidies law | - |
| Year: NA | |||
| Leadership: NA | |||
| Approach: Eliminating food subsidies for sugar used in industries (pastries, candies, chocolate, sweets…) [123,164]. |
| Country | Product Reformulation | Consumer Education/Behavior Change | Labeling | Interventions in Specific Settings |
|---|---|---|---|---|
| Afghanistan | - | Name of initiative: National Health Policy 2015–2020 | - | - |
| Year: 2015 | ||||
| Leadership: Led by the government (MOPH) | ||||
| Approach: Promote health and highlight the risk of over consumption of foods high in sugar (not adopted) [117]. | ||||
| Name of initiative: Guideline to reduce sugar intake and avoid sweet carbonated beverages Year: 2016 | ||||
| Leadership: Led by the government (MOPH, Ministry of Agriculture, Irrigation and Livestock, and Ministry of Education, in collaboration with the WHO) | ||||
| Approach: Inclusion in FBDG [165]. | ||||
| Bahrain | Name of initiative: NCD Joint Programming Mission | - | - | Name of initiative: Food canteen list for the academic year 2016–2017 |
| Year: 2017 | Year: 2016 | |||
| Leadership: Led by the government (MOH) | Leadership: Led by the government (MOH) | |||
| Approach and target: Work on the law to reduce sugar in locally made juices (not adopted) [122]. | Approach: List of allowed and not allowed food items (which include some high sugar items such as fruit/nectar drinks, soft drinks, energy drinks, sweet biscuits, croissants, sweets and candies) | |||
| Setting: Schools [121,166,167]. | ||||
| Iran | Name of initiative: NA | Name of initiative: Guideline on the consumption of sugar, sweet foods and beverages, and soft drinks | Name of the Initiative: Nutritional Traffic Light labeling | Name of initiative: National Guidelines for Healthy School Canteen |
| Year: 2016 | Year: 2015 | Year: 2016 | Year: 2014 | |
| Leadership: Supreme Council for Health and Food Security | Leadership: Led by the government (Ministry of Health and Medical Education; with the involvement of the Tehran University of Medical Sciences; Iranian Nutrition Society; and the National Nutrition and Food Technology Research Institute, Tehran, as well as NGOs and the WHO EMRO | Leadership: Led by the government | Leadership: Led by the government (Ministry of Health and Medical Education in collaboration with MOH) | |
| Approach and target: Reformulate foods to reduce sugar primarily in drinks, by up to 10% [168]. | Approach: Inclusion in FBDG [169]. | Approach: Started in 2014 as voluntary; became mandatory in 2016; mandatory label that indicates the content of sugar in foods, as follows: Low (Green): less than or equal to 5 g per 100 g or less than or equal to 2.5 g per 100 mL Medium (Yellow): greater than 5 g to less than or equal to 22.5 g per 100 g, or greater than 2.5 g to less than or equal to 11.25 g per 100 mL High (Red): greater than 22.5 g per 100 g; greater than 11.25 g per 100 mL; greater than 27 g per serving [121,170,171,172,173,174]. | Approach: Prohibited the marketing of soft drinks and sweet biscuits; all schools should provide healthier food and drink options in school canteens | |
| Setting: Schools [167,175,176]. | ||||
| Name of initiative: Iran National Standard | Name of initiative: Educational campaigns for increasing awareness on salt and sugar, total fat and TFA reduction | |||
| Year: NA | Year: Annually since 2010 | |||
| Leadership: Led by the National Standard Organization | Leadership: Led by the government | |||
| Approach and target: Reducing the sugar content in biscuit products by 10% and in flavored milk from 8% to 6%. | Approach: Social marketing (e.g., campaigns), TV advertising and events. | |||
| Information provided by the NFP | Information provided by the NFP | |||
| Iraq | - | - | - | Name of initiative: National strategy for the prevention and control of non-communicable diseases 2018–2022 |
| Year: 2018 | ||||
| Leadership: Led by the government (MOH, Ministry of Education, Ministry of Youth and Sports and Ministry of Commerce) | ||||
| Approach: Limiting the marketing of food items and beverages that are high in monosaccharides, to children in the school setting | ||||
| Setting: Schools [129]. | ||||
| Jordan | Name of initiative: National Framework of Action on Obesity Prevention in Jordan 2018–2023 | Name of initiative: Low salt, low sugar, low saturated and trans fat consumption guideline for health care providers for training of trainers (TOT) and pamphlet for consumers | - | Name of initiative: Health requirements for school canteens and foods allowed and prohibited to be sold for the year 2012 |
| Year: 2019 | Year: 2015 | Year: 2012 | ||
| Leadership: Led by the government (MOH), in collaboration with Jordan Food and Drug Administration, Jordan Standards and Metrology Organization, Ministry of Education, Amman Municipality, Ministry of Youth, Ministry of Industry and Trade, the Royal Medical Services, Ministry of Planning and the University of Jordan Approach and target: Food reformulation regulations to reduce sugar, guided by WHO recommendations [121,131,177]. | Leadership: Led by the government (MOH) | Leadership: Led by the government (Ministry of Education) | ||
| Approach: Awareness and education [178]. | Approach: Food items have been prohibited from being sold at school canteens; they include soft drinks of all kinds, drinks containing sugar, candies, chocolates, lollipops, ice cream, biscuits of all kinds and prepackaged cakes | |||
| Setting: Schools [167,179]. | ||||
| Name of initiative: Guideline for low consumption of salt, sugar, saturated fat and trans fat | Name of initiative: NA | |||
| Year: 2020 | Year: NA | |||
| Leadership: Led by the government | Leadership: Led by the government (MOH), and the army sector | |||
| Approach: Inclusion in FBDG [180]. | Approach: Reduce sugars in menus served to the workers and patients at hospitals | |||
| Setting: Hospitals [177]. | ||||
| KSA | Name of initiative: Healthy Food Strategy, vision 2030 | Name of initiative: Guideline for low consumption of sugar | Name of initiative: A guide for healthy food terms and conditions in government subsistence purchase contracts | Name of initiative: A guide for healthy food terms and conditions in government subsistence purchase contracts |
| Year: 2018 | Year: 2012 | Year: 2019 | Year: 2019 | |
| Leadership: Led by the government (SFDA) | Leadership: Led by the government (MOH) | Leadership: Led by the government (SFDA) | Leadership: Led by the government (SFDA) | |
| Approach and target: Mandatory: Reduce the sugar content in food products by spreading awareness among food manufacturers and importers [133]. | Approach: Inclusion in the Dietary Guidelines for Saudis-The Healthy Food Palm [181]. | Approach: Nutrition labels ought to include TS and AS. Nutrition claims should be as follows: (1) “low in sugar” for products that do not contain more than 5 g of sugars per 100 g of solid food or more than 2.5 g of sugars per 100 mL of liquids; (2) “sugar-free” for products that do not contain more than 0.5 g of sugars per 100 g or per 100 mL; (3) “no added sugars” for products that do not contain any added monosaccharides or disaccharides or any other sweetener; (4) “reduced sugar” for products that contain the same amount of energy or less energy as compared to similar products [120,132,173,182,183] | Approach: Implementing healthy food terms and conditions: (1) select products that contain no AS or products that are low in AS as per the SFDA.FD 2233/2018; (2) replace chocolates with granola, fruits, unsalted nuts; (3) replace carbonated drinks with water, 100% fruit juices, milk low in fat; (4) offer sweets that are low in energy such as low-fat zabadi | |
| Setting: Governmental settings (hospitals, universities, military) [182]. | ||||
| Name of Initiative: SFDA.FD 5001: Fresh juices, mixes and beverages, sold at juice stores, restaurants and cafes | Name of initiative: An initiative to promote public health through food in the work environment | |||
| Year: Issued in 2019 and enforced in 2020 | Year: 2019 | |||
| Leadership: Led by the government (SFDA) | Leadership: General Authority for Food and Medicine | |||
| Approach and target: (1) Regulate the nutrient composition in fresh juices, nectars and fruit drinks and their display on products; (2) Encourage food and beverage establishments (restaurants, hotels, coffee shops, juice shops and supermarkets that sell juices) to withhold adding sugars to fresh juices, nectars and fruit drinks [184]. | Approach: In addition to those mentioned by the “Guide for healthy food terms and conditions in government subsistence purchase contracts”, (1) prohibit the provision of carbonated beverages; (2) offer fresh juices rather than artificial juices or nectar; (3) avoid adding sugars to fresh juices; (4) Place the following claim on sugar packets “The WHO recommends a maximum of 50 g of sugar per person per day | |||
| Setting: Public and private work environment [185]. | ||||
| Name of initiative: SFDA.FD 42 “Traffic light labeling” | Name of initiative: NA | |||
| Year: 2019 | Year: NA | |||
| Leadership: Led by the government (SFDA) | Leadership: NA | |||
| Approach: Voluntary for all food categories Low (Green): less than or equal to 5 g per 100 g Medium (Orange): greater than 5 g to less than or equal to 22.5 g per 100 g High (Red): greater than 22.5 g per 100 g; greater than 27 g per serving [182,186]. | Approach: Prohibited the marketing of soft drinks and sweet biscuits | |||
| Setting: Schools [167]. | ||||
| Kuwait | Name of initiative: Sugar reduction initiative | Name of initiative: Kuwait Food Based Dietary Guidelines | Name of initiative: Labeling technical regulation (Requirements of Nutritional Labeling GSO 2233/2012) | Name of initiative: The Case for Investment in Prevention and Control of Non-Communicable Diseases in Kuwait |
| Year: 2016 | Year: 2022 | Year: 2012 | Year: 2020 | |
| Leadership: Led by the government (Community Nutrition Promotion Sector (CNPS) of Public Authority for Food and Nutrition (PAFN)), on behalf of the Kuwait MOH, in partnership with the WHO and the food industries | Leadership: Led by the government | Leadership: Led by the GCC Standardization Organization | Leadership: Led by the FNA on behalf of the Kuwait MOH, in partnership with the WHO and the food industries | |
| Approach and target: Voluntary: The Community Nutrition Promotion Sector has approached six local manufacturers of fruit juices and SSBs in August 2016 with an aim to reduce the AS in their products. The producers have shown great support to gradually reduce the sugar content in the nectars and drinks considering that they are the main source of FS intake among children and adults [187]. The sugar reduction initiative included biscuits and cakes as well. | Approach: Consumer awareness and education (being finalized). | Approach: Mandatory: Nutrition labeling of all prepackaged food products except for raw products such as fresh fruits, vegetables, meat and fish (including % of daily intake) [188]. | Approach: Motivate food industries, via a collaboration between the Community Nutrition Promotion Sector and the Ministry of Education, in order to improve the school canteen food options, so that only the Nectar products with reduced sugar content are allowed into the school canteens | |
| Setting: Schools [187]. | ||||
| Information provided by the NFP | ||||
| Name of initiative: National strategy for the prevention and response to chronic noncommunicable diseases in the State of Kuwait 2017–2025 | Name of initiative: Nutrition and health education programs | Name of initiative: National Committee for Nutrition promotion of school children | ||
| Year: 2017 | Year: NA | Year: 2021 | ||
| Leadership: Led by the government | Leadership: Led by the government | Leadership: Led by the PAFN | ||
| Approach and target: Reduction of free and AS content in foods and beverages (not adopted) [189]. | Approach: Mass and social media awareness programs (campaigns, events). | Approach: Voluntary guidelines, education and procurement policy | ||
| Setting: Schools. | ||||
| Information provided by the NFP | Information provided by the NFP | |||
| Name of initiative: Implementing the FOPL | Name of initiative: Obesity Prevention Project | |||
| Year: 2018 | Year: 2022 | |||
| Leadership: Led by the government | Leadership: Led by the PAFN | |||
| Approach: Voluntary: Traffic Light labeling standard (Proposal submitted and awaiting approval from related technical committee). | Approach: Voluntary guidelines, education and procurement policy | |||
| Setting: Schools. | ||||
| Information provided by the NFP | Information provided by the NFP | |||
| Name of initiative: NA | ||||
| Year: NA | ||||
| Leadership: NA | ||||
| Approach: Prohibited the marketing of soft drinks and sweet biscuits | ||||
| Setting: Schools [167]. | ||||
| Lebanon | - | Name of initiative: Guideline to limit the intake of sugar, especially AS from sweetened foods and beverages | Name of initiative: General Standard for the Labeling of Pre-packaged Foods (NL 206:2017) and Guidelines for Use of Nutrition and Health Claims (NL 661:2017) | Name of initiative: NA |
| Year: 2013 | Year: 2017 | Year: NA | ||
| Leadership: Led by the American University of Beirut | Leadership: Led by the government | Leadership: NA | ||
| Approach: Inclusion in FBDG [190]. | Approach: Mandatory sugar claims for all food categories, whenever applicable [191,192]. | Approach: Prohibited the marketing of soft drinks and sweet biscuits | ||
| Setting: Schools [167]. | ||||
| Libya | - | Name of initiative: Guideline for reducing the consumption of foods high in AS | - | - |
| Year: 2020 | ||||
| Leadership: Led by the National Center for Disease Control | ||||
| Approach: Inclusion in the Dietary Guidelines for Chronic Diseases [193]. | ||||
| Morocco | Name of initiative: National Health Plan 2025 | Name of initiative: National Health Plan 2025 | Name of initiative: Labeling of food products (n°6684 of 21/06/2018) | Name of initiative: Dietary and health guidelines for the preparation of menus in school canteens and boarding schools |
| Year: 2018 | Year: 2018 | Year: 2018 | Year: 2013 | |
| Leadership: Led by the government (MOH) | Leadership: Led by the government (MOH) | Leadership: Led by the government (Ministry of Agriculture and MOH) | Leadership: Led by the government (MOH) | |
| Approach and target: Encourage the food industry to lower the sugar levels in their products [194]. | Approach and target: Encourage citizens, in particular children and poor populations, to consume less sugary products, less taxed, cheaper and healthier products [194]. | Approach: Mandatory: Labeling of food products with sugar and percentage of daily intake. Voluntary: FOPL (awaiting implementation) [195]. | Approach: Limiting the availability of the following foods: jams, candies, chocolates, cookies, cakes, ice cream, sweet breads, croissants, pancakes, cornflakes containing AS, flavored water, soft drinks and sodas, sweetened tea, coffee and infusions | |
| Setting: Schools, boarding schools and universities (not adopted) [196,197]. | ||||
| A proposal was developed in 2022 to set standards for agri-food products (Biscuits, pastries, milk and dairy products, cereals, confectionery, chocolate, candy, chewing gum, prepared broths, prepared soups, syrups, sauces, fruit juices (nectar, drinks), flavored drinks) regarding their sugar concentrations. Standards are being finalized and the draft for the finance law will be executed by 2023. The reduction will be mandatory as of year 2025 for all foods and beverages, with a reduction of 25% in AS content in processed foods as compared to year 2022. The reduction in sugar content will be as follows: 50% for dairy desserts, 20% for yogurt drinks, 40% for sweetened condensed milk, 40% for cookies, 29% for confectionery, 34% for chocolates and 33% for jam [198,199]. | ||||
| Name of initiative: National Nutrition Program | Name of initiative: Nutri-score | Name of initiative: National Multisectoral Strategy for the Prevention and Control of Non-Communicable Diseases 2019–2029 | ||
| Year: 2019 | Year: 2023; legislative decree being finalized | Year: 2019 | ||
| Leadership: Led by the government (MOH) | Leadership: Led by the government (MOH) and WHO | Leadership: Led by the government (MOH) and General Directorate of Customs | ||
| Approach: Promote healthy nutrition throughout the lifecycle by reducing the consumption of sugar-rich foods and beverages [143]. | Aproach: Voluntary [200]. | Approach: Setting sugar standards and procurement policy, and providing education and voluntary guidelines | ||
| Setting: Schools [140]. | ||||
| Oman | Name of initiative: National plan for the prevention and control of chronic non-communicable diseases 2016–2025 | Name of initiative: Guideline for low consumption of sugar | Name of initiative: GSO standard for Labeling of Prepackaged Food Stuffs (GSO 9/2013 (E)) | Name of initiative: National plan for the prevention and control of chronic non-communicable diseases 2016–2025; National Nutrition Strategy and Framework for Action 2020–2030 |
| Year: 2016 | Year: 2009; being updated in 2022 | Year: 2013 | Year: 2016 and 2020 respectively | |
| Leadership: Led by the government (MOH) | Leadership: Led by the government | Leadership: Led by the GCC Standardization Organization | Leadership: Led by the government (MOH) | |
| Approach and target: Encourage manufacturers to produce small-sized portions of food products that are high in sugars (not adopted) [152]. | Approach: Inclusion in FBDG [201]. | Approach: Mandatory for all food categories: Labeling for prepacked food with detailed ingredients and nutritive value of the food, as well as percentage of daily intake (this includes TS). | Approach: Food and beverages that are high in sugar have been prohibited from being sold at schools | |
| Setting: Schools [151,152,167]. | ||||
| Information provided by the NFP | ||||
| Name of initiative: Policy statement for sugar reduction | Name of initiative: Promoting healthier lifestyle and wellbeing | Name of initiative: Implementing Nutrient Profile in School | ||
| Year: 2022 | Year: 2021 | Year: NA (planned) | ||
| Leadership: Led by the government (MOH) | Leadership: Led by the WHO and government (MOH) | Leadership: Led by the government | ||
| Approach and target: Voluntary: Product reformulation (for instance, sugar in SSBs to be reduced by 20% by 2025) (planned) | Approach: awareness aimed at reducing the consumption of unhealthy food high in sugar, as well as other components (planned) [130]. | Approach: Providing education and voluntary guidelines | ||
| Setting: Schools. | ||||
| Information provided by the NFP | Information provided by the NFP | |||
| Name of initiative: National Nutrition Campaign | ||||
| Year: 2022–2023 | ||||
| Leadership: Led by the government, in collaboration with the WHO, FAO and Aljisr Foundation | ||||
| Approach: An awareness campaign for the community to reduce sugar, salt and unhealthy fat; through social marketing, TV advertisements, events, lectures for community (online and in person), videos, social media posts, posters, messages in the public transport, etc. | ||||
| Information provided by the NFP | ||||
| Pakistan | Name of initiative: National Action Plan for Reduction of Dietary Risks of NCDs for Pakistan | Name of initiative: Guideline to reduce sugar intake, and limit intake of soft drinks, confectionaries, bakery products and commercial fruit drinks | Name of initiative: National Action Plan for Reduction of Dietary Risks of NCDs for Pakistan | Name of initiative: NA |
| Year: 2022 (Planned) | Year: 2019 | Year: 2022 (Planned) | Year: NA | |
| Leadership: Led by the government (Ministry of National Health Services, Regulation and Coordination), in collaboration with the WHO | Leadership: Led by the government (Ministry of Planning, Development and Reform) and FAO UN | Leadership: Led by the government (Ministry of National Health Services, Regulation and Coordination); in collaboration with the WHO | Leadership: Led by Provincial Food Authorities of Punjab, Sindh, KP and Balochistan | |
| Approach and target: Mandatory for all foods and snacks (bakery products, breakfast cereals, desserts, puddings and ice cream, SSBs, biscuits and cakes, ultra-processed foods): Approach includes: (1) targets for sugar levels in foods and snacks and (2) revision of standards through Pakistan Standards and Quality Control Authority and Provincial Food Authorities. | Approach: Inclusion in Pakistan Dietary Guidelines for Better Nutrition [202]. | Approach: Warning labels; Mandatory for certain food categories such as “foods high in sugar”. | Approach: Restrictions on availability of SSBs and energy drinks, and foods high in sugar/ultra-processed foods, in schools/educational institutions; traffic lights have been introduced (foods in red category are not allowed in the premises of the school and within the 100-m radius of the educational institutions, similarly the availability and consumption of food in green category is encouraged in the premises of the school) | |
| Setting: Schools/educational institutions [203]. | ||||
| Information provided by the NFP | Information provided by the NFP | |||
| Name of initiative: Saving Youth from Sugar-sweetened Beverages through Education, Media, and Advocacy (SYSTEM) | ||||
| Year: 2020 | ||||
| Leadership: Pakistan National Heart Association (NGO) working closely with several government Ministries and key institutions | ||||
| Approach: Anti sugary drinks campaign through social marketing, events and media advocacy [154]. | ||||
| Name of initiative: National Action Plan for Reduction of Dietary Risks of NCDs for Pakistan | ||||
| Year: 2022 (Planned) | ||||
| Leadership: Led by the government (Ministry of National Health Services, Regulation and Coordination); in collaboration with the WHO | ||||
| Approach: Multisectoral approach; awareness raising. | ||||
| Information provided by the NFP | ||||
| Palestine | Name of initiative: National Health Strategy 2017–2022 | Name of initiative: National Health Strategy 2017–2022 | - | Name of initiative: NA |
| Year: 2017 | Year: 2017 | Year: NA | ||
| Leadership: Led by the government (MOH) in cooperation with all health sector stakeholders | Leadership: Led by the government (MOH) in cooperation with all health sector stakeholders | Leadership: NA | ||
| Approach and target: Mandatory technical instructions to reduce sugar in food products (to be endorsed and applied by 90%) (planned) [155]. | Approach: Raising awareness to help reduce the consumption of sugar in line with the WHO (planned) [155]. | Approach: Prohibited the marketing of soft drinks and sweet biscuits in schools | ||
| Setting: Schools [167]. | ||||
| Name of initiative: Guideline for reduction of sugary foods and beverages, specifically AS | ||||
| Year: 2021 | ||||
| Leadership: Led by the government (MOH) | ||||
| Approach: Inclusion in FBDG [204]. | ||||
| Qatar | Name of initiative: Qatar National Nutrition and Physical Activity Action Plan 2017–2022 | Name of initiative: Start now campaign | Name of initiative: Food safety and health guide | |
| Year: 2017 | Year: 2017 | Year: 2016 | ||
| Leadership: Led by the government (MOPH) | Leadership: Led by the government (MOPH) | Leadership: Led by the government (Ministry of Education and Higher Education Department of Health and Safety) | ||
| Approach and target: Progressive reformulation of sugar-rich drinks and foods (not adopted) [156]. | Approach: Encourages the consumption of wholegrains, vegetables, fish and chicken, and discourages foods high in salt, sugar and fat [205]. | Approach: EI from TS in school meals should be limited to 35% (or 17.5 g) per person | ||
| Setting: Schools (not adopted) [206,207]. | ||||
| Name of initiative: Initiative to reduce fat, sugar and salt consumption in Qatar | Name of Initiative: Smart Start Campaign | Name of initiative: Guidance for supervisors of school canteens for the academic year 2018–2019 | ||
| Year: 2019 | Year: 2019 | Year: 2018 | ||
| Leadership: Led by the government (MOPH) | Leadership: Qatar University | Leadership: Led by the government (Ministry of Education and Higher Education Department of Health and Safety) | ||
| Approach: Voluntary: Approach done through meetings with the food industries (dairy beverages, bread, pastries, baked goods, bottled juices) to reformulate their products and reduce the amount of sugar used during manufacturing. | Approach: Promotes the importance of physical and psychological health of children aged 3–6 years; included sugar awareness on the dangers of excess sugar intake [208]. | Approach: Food items prohibited from being sold at schools; they include desserts and sweets (jellies, lollipops, chewing gum), carbonated beverages, ice cream, chocolates, energy drinks, milk and yogurt that contain more than 22 g and 30 g of sugar/240 mL, | ||
| Setting: Schools [167,206,207,209]. | ||||
| Information provided by the NFP | ||||
| Name of initiative: Initiative to reduce fat, sugar and salt consumption in Qatar | Name of initiative: Food & Beverage Guidelines; School Canteen Guidelines; Educational sessions in schools and workplaces | |||
| Year: 2019 | Year: Ongoing | |||
| Leadership: Led by the government (MOPH) | Leadership: Led by the government (MOPH) | |||
| Approach: Social marketing (e.g., campaigns, TV advertising (conducted TV and radio interviews), events. | Approach: Education, procurement policy, voluntary guidelines. School Canteen Guidelines are mandatory in governmental schools | |||
| Setting: Schools, hospitals, workplace. | ||||
| Information provided by the NFP | Information provided by the NFP | |||
| - | Name of initiative: Guideline for low consumption of sugar | - | ||
| Year: 2015 | ||||
| Leadership: Led by the Supreme Council of Health | ||||
| Approach: Inclusion in FBDG [210]. | ||||
| Somalia | Name of Initiative: Somalia Nutrition Strategy (2020–2025) | - | ||
| Year: Target by 2025 | ||||
| Leadership: Ministry of Health and Human Services, Federal Republic of Somalia | ||||
| Approach and Target: Providing comprehensive and routine nutritional assessment and counseling services to adolescents at communities, schools and health facilities with the goal of reducing the intake of FS in children and adult meals and reducing the consumption of SSBs [211]. | ||||
| Sudan | - | Name of initiative: National Nutrition Strategic Plan 2014–2025 | - | - |
| Year: 2014 | ||||
| Leadership: Led by the government (MOH) | ||||
| Approach: Promote nutritional knowledge and appropriate attitudes and practices of caregivers towards food, social and dietary customs, family/child care and feeding practices; promote low sugar intake among the public (not adopted) [212]. | ||||
| Tunisia | Name of initiative: National Obesity Control and Prevention | - | Name of initiative: NA | - |
| Year: 2017 | Year: 2008 | |||
| Leadership: Led by the government (Ministry of Commerce) with the cooperation of industries | Leadership: Led by the government (Ministry of Commerce and Crafts) | |||
| Approach and target: Reduction of sugar content in beverages, milk and milk products [118,120,158]. | Approach: The amount of sugar should be indicated on the label. Nutrition claims indicating “sugar-free” should not contain more than 0.5 g of sugars per 100 g or per 100 mL (not adopted) [213]. | |||
| UAE | Name of initiative: National Action Plan in Nutrition; National Plan for Prevention and Response to NCDs 2017–2021 | Name of initiative: National Plan to Combat Childhood Obesity United Arab Emirates | Name of initiative: Weqaya Food Program (ADS13/2018)–health logo scheme in Abu Dhabi | Name of initiative: Guideline to Healthy and Nutritious Food Practices in School Canteens–Dubai |
| Year: 2017 | Year: 2017 | Year: 2015 | Year: 2011 | |
| Leadership: Led by the government (MOHAP) | Leadership: Led by the government (MOHAP–Department of Health Education and Promotion) | Leadership: Led by Abu Dhabi Quality and Conformity Council | Leadership: Led by Dubai Municipality–Dubai Health Authority | |
| Approach and targets: Regulation of the maximum limit of sugar in SSBs (8 g/100 mL i.e., 2 teaspoons) (in process of submission to Higher Authorities for endorsement) [161,162]. | Approach: Limit the consumption of foods and beverages high in sugar among infants and young children by providing guidance and support to caregivers regarding foods to be avoided (such as sugar- sweetened milks, fruit juices or energy-dense and nutrient poor foods) (not adopted) [159]. | Approach: Voluntary: Logo on foods/dishes or meals should meet certain AS levels in meals/takeaway food, children’s meals, or takeaway food and individual food items [173,214]. | Approach: Guideline provided to the school canteens and staff regarding foods that are not allowed (soft drinks, energy drinks, all types of fruit drinks, milk and yogurt with artificial flavors, chewing gum, candies, sweets, chocolates). Moreover, AS content should not exceed 6% in food preparations and sugars should be limited to 2% of daily recommended allowance in packaged products | |
| Setting: Schools (not adopted) [215]. | ||||
| Name of initiative: Guideline for low consumption of sugar | Name of initiative: National Program for Happiness and Wellbeing | Name of initiative: School Canteen Guidelines of the Emirate of Abu Dhabi | ||
| Year: 2019 | Year: 2020 | Year: 2011 | ||
| Leadership: Led by the government (MOHAP), in collaboration with other health authorities, government-related sectors, academia and municipalities | Leadership: Led by the government (MOH and the Standards and Metrology Organization) | Leadership: Abu Dhabi Education Council, Abu Dhabi Food Control Authority and Health Authority | ||
| Approach: Inclusion in FBDG [216]. | Approach: Voluntary FOP traffic light labeling for sugar levels in prepackaged foods; to become mandatory in 2022 [173,217]. | Approach: TS and AS of products offered in schools should not exceed 35% of the product’s weight | ||
| Setting: Schools (not adopted) [218]. | ||||
| Name of initiative: National Plan to Combat Childhood Obesity United Arab Emirates | ||||
| Year: 2017 | ||||
| Leadership: Led by the government (MOHAP–Department of Health Education and Promotion) | ||||
| Approach: Eliminate the provision and sale of unhealthy foods (SSBs and energy-dense, nutrient-poor foods) | ||||
| Setting: Schools (not adopted) [159]. | ||||
| Name of initiative: National Action Plan in Nutrition | ||||
| Year: 2017 | ||||
| Leadership: Led by the government (MOHAP) | ||||
| Approach: Reduce sugar consumption | ||||
| Setting: Prisons, juvenile centers, police and military schools, army forces, geriatric home cares and their canteen [161]. | ||||
| Name of initiative: Department of Health Guideline for Vending Machines and Retail Items in Health Care Facilities–Abu Dhabi | ||||
| Year: 2021 | ||||
| Leadership: Led by the government (Department of Health) | ||||
| Approach: A healthy vending machine should not contain foods high in AS (soft drinks, sports drinks, energy drinks, chocolates except for dark, sugar candies); packed snacks should not exceed 35% of total weight from sugar (i.e., a maximum of 20 g of TS) | ||||
| Setting: Health care facilities [219]. |
| Country | National Strategy and/or Action Plan |
|---|---|
| Jordan | Reduction of FS intake in the population, specifically among children and adolescents, to <10% of EI–2015 (MOH) (National Strategy And Plan Of Action Against Diabetes, Hypertension, Dyslipidemia And Obesity in Jordan) (not adopted) [220] |
| KSA | Reduction of monosaccharides consumption by 10% in the coming 10 years (an average of 1% per year)–2017 (MOH) (National Obesity Control Program) (not adopted) [221] and 2014 (Government of KSA) (National Executive Plan for NCDs 2014–2025) (not adopted) [222] |
| Reduction in consumption of products rich in sugars to less than 10% of total EI and to less than 5% for more health benefits–2015 (MOH) (National Strategy for Healthy Food and Physical Activity 2015–2025) (not adopted) [223] and 2014 (Government of KSA) (KSA National Strategy for Diet and Physical Activity for the Years 2014–2025) (not adopted) [224] | |
| Morocco | Reduction in population sugar intake–2015 (MOH) (Prevention of NCDs: Multisectoral Action Plan for a Healthy Lifestyle 2015–2020) [225] |
| Oman | Reduction in sugar intake by 20% by 2025 (MOH) (National Nutrition Strategy) (Information provided by the NFP) |
| Reduction in population sugar intake, gradually to reach 100% by 2025–2016 (MOCI) (National plan for the prevention and control of chronic non-communicable diseases 2016–2025) [152] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Jawaldeh, A.; Taktouk, M.; Naalbandian, S.; Aguenaou, H.; Al Hamad, N.; Almamary, S.; Al-Tamimi, H.A.; Alyafei, S.A.; Barham, R.; Hoteit, M.; et al. Sugar Reduction Initiatives in the Eastern Mediterranean Region: A Systematic Review. Nutrients 2023, 15, 55. https://doi.org/10.3390/nu15010055
Al-Jawaldeh A, Taktouk M, Naalbandian S, Aguenaou H, Al Hamad N, Almamary S, Al-Tamimi HA, Alyafei SA, Barham R, Hoteit M, et al. Sugar Reduction Initiatives in the Eastern Mediterranean Region: A Systematic Review. Nutrients. 2023; 15(1):55. https://doi.org/10.3390/nu15010055
Chicago/Turabian StyleAl-Jawaldeh, Ayoub, Mandy Taktouk, Sally Naalbandian, Hassan Aguenaou, Nawal Al Hamad, Salima Almamary, Hend Ali Al-Tamimi, Salah Abdulla Alyafei, Rawhieh Barham, Maha Hoteit, and et al. 2023. "Sugar Reduction Initiatives in the Eastern Mediterranean Region: A Systematic Review" Nutrients 15, no. 1: 55. https://doi.org/10.3390/nu15010055
APA StyleAl-Jawaldeh, A., Taktouk, M., Naalbandian, S., Aguenaou, H., Al Hamad, N., Almamary, S., Al-Tamimi, H. A., Alyafei, S. A., Barham, R., Hoteit, M., Hussain, M., Massad, H., & Nasreddine, L. (2023). Sugar Reduction Initiatives in the Eastern Mediterranean Region: A Systematic Review. Nutrients, 15(1), 55. https://doi.org/10.3390/nu15010055