
Exercise Capacity, Iron Status, Body Composition, and Mediterranean Diet in Patients with Chronic Heart Failure

Abstract
1. Background
2. Materials and Methods
2.1. Study Design
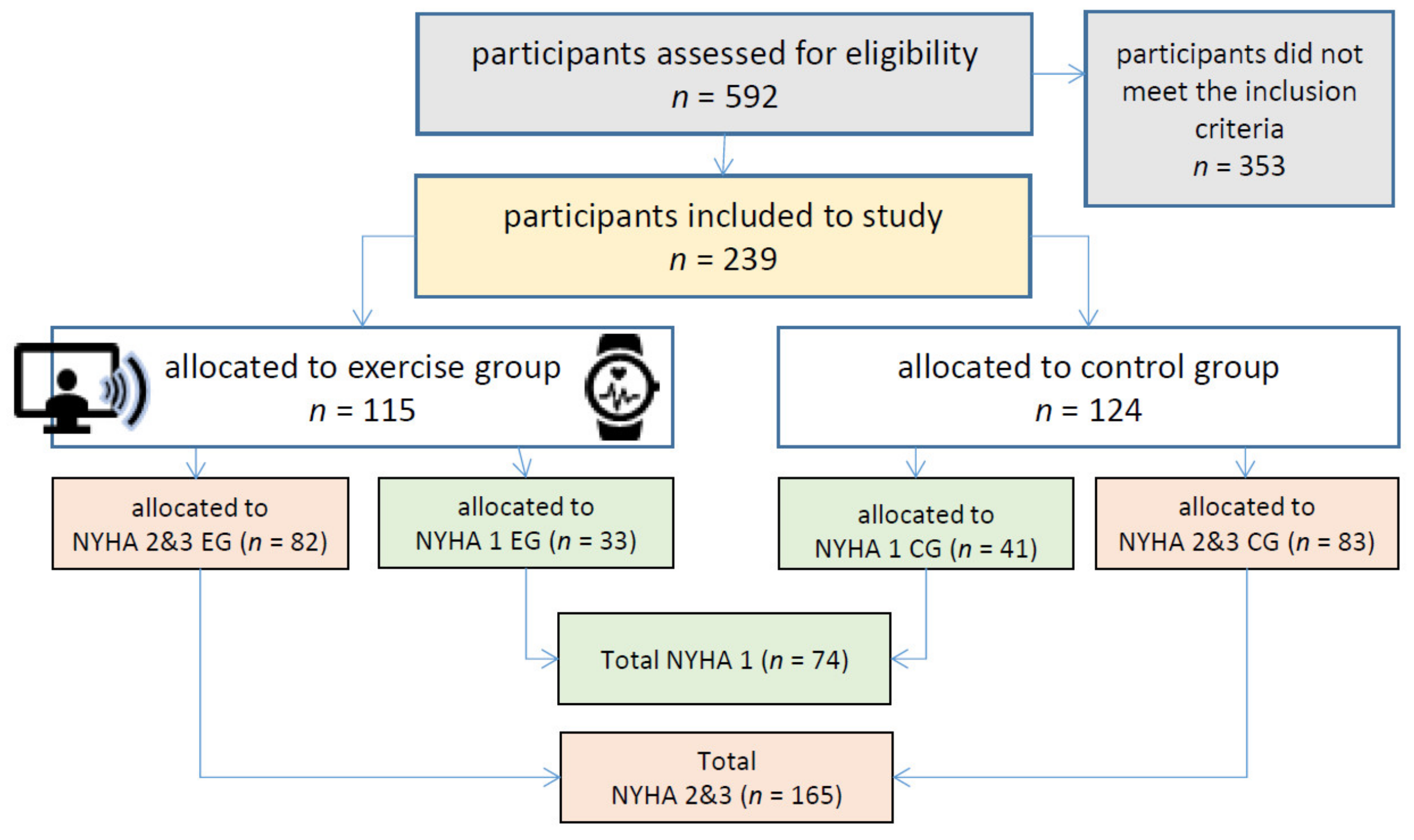
2.2. Subjects
2.3. Procedures
2.4. Statistical Analysis
3. Results
Participants’ Characteristics
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tanai, E.; Frantz, S. Pathophysiology of Heart Failure. In Comprehensive Physiology; John Wiley & Sons, Ltd.: New York, NY, USA, 2015; pp. 187–214. [Google Scholar]
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [PubMed]
- van Riet, E.E.; Hoes, A.W.; Limburg, A.; Landman, M.A.; van der Hoeven, H.; Rutten, F.H. Prevalence of unrecognized heart failure in older persons with shortness of breath on exertion. Eur. J. Heart Fail. 2014, 16, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Bundesärztekammer (BÄK); Kassenärztliche Bundesvereinigung (KBV); Arbeitsgemeinschaft der Wissenschaftli-Chen Medizinischen Fachgesellschaften (AWMF). Nationale Versorgungs Leitlinie Chronische Herzinsuffizienz Leitlinienreport; Springer: Berlin, Germany, 2018. [Google Scholar]
- American Heart Association. Heart Failure. 2022. Available online: https://www.heart.org/en/health-topics/heart-failure (accessed on 4 November 2022).
- Schwinger, R.H.G. Pathophysiology of heart failure. Cardiovasc. Diagn. Ther. 2021, 11, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, F.; Doust, J.; Mant, J.; Cowie, M.R. Diagnosis of heart failure in primary care. Heart 2010, 96, 1773–1777. [Google Scholar] [CrossRef] [PubMed]
- Hayhoe, B.; Kim, D.; Aylin, P.P.; Majeed, A.; Cowie, M.R.; Bottle, A. Adherence to guidelines in management of symptoms suggestive of heart failure in primary care. Heart 2018, 105, 678–685. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Corrado, D.; Drezner, J.; Halle, M.; Hansen, D.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behavior. 2020. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 3 July 2022).
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Ernährung e.V. Vollwertige Ernährung. 2022. Available online: https://www.dge.de/ernaehrungspraxis/vollwertige-ernaehrung/ (accessed on 4 November 2022).
- Mesías, M.; Seiquer, I.; Muñoz-Hoyos, A.; Galdó, G.; Navarro, M.P. The beneficial effect of Mediterranean dietary patterns on dietary iron utilization in male adolescents aged 11–14 years. Int. J. Food Sci. Nutr. 2009, 60 (Suppl. S7), 355–368. [Google Scholar] [CrossRef]
- Zbeida, M.; Goldsmith, R.; Shimony, T.; Vardi, H.; Naggan, L.; Shahar, D.R. Mediterranean diet and functional indicators among older adults in non-Mediterranean and Mediterranean countries. J. Nutr. Health Aging 2014, 18, 411–418. [Google Scholar] [CrossRef]
- Russell, S.D.; Saval, M.A.; Robbins, J.L.; Ellestad, M.H.; Gottlieb, S.S.; Handberg, E.; Zhou, Y.; Chandler, B. New York Heart Association functional class predicts exercise parameters in the current era. Am. Heart J. 2009, 158 (Suppl. S4), S24–S30. [Google Scholar] [CrossRef]
- American Heart Association. Classes of Heart Failure. 2017. Available online: https://www.heart.org/en/health-topics/heart-failure/what-is-heart-failure/classes-of-heart-failure (accessed on 7 November 2022).
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A. ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Rapp, D.; Scharhag, J.; Wagenpfeil, S.; Scholl, J. Reference values for peak oxygen uptake: Cross-Sectional analysis of cycle ergometry-based cardiopulmonary exercise tests of 10,090 adult German volunteers from the Prevention First Registry. BMJ Open 2018, 8, e018697. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Green, C.; Porter, C.B.; Bresnahan, D.R.; Spertus, J.A. Development and evaluation of the Kansas City Cardiomyopathy Questionnaire: A new health status measure for heart failure. J. Am. Coll. Cardiol. 2000, 35, 1245–1255. [Google Scholar] [CrossRef]
- Nowson, C.A.; Service, C.; Appleton, J.; Grieger, J.A. The impact of dietary factors on indices of chronic disease in older people: A systematic review. J. Nutr. Health Aging 2017, 22, 282–296. [Google Scholar] [CrossRef]
- Fitó, M.; Konstantinidou, V. Nutritional genomics and the Mediterranean diet’s effects on human cardiovascular health. Nutrients 2016, 8, 218. [Google Scholar] [CrossRef]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef]
- Finicelli, M.; Di Salle, A.; Galderisi, U.; Peluso, G. The Mediterranean Diet: An Update of the Clinical Trials. Nutrients 2022, 14, 2956. [Google Scholar] [CrossRef]
- Bianchi, V.E. Nutrition in chronic heart failure patients: A systematic review. Heart Fail. Rev. 2019, 25, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Avery, C.L.; Loehr, L.R.; Baggett, C.; Chang, P.P.; Kucharska-Newton, A.M.; Matsushita, K.; Rosamond, D.W.; Heiss, G. The population burden of heart failure attributable to modifiable risk factors: The ARIC (Atherosclerosis Risk in Communities) study. J. Am. Coll. Cardiol. 2012, 60, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Alkhatib, A.; Klonizakis, M. Effects of exercise training and Mediterranean diet on vascular risk reduction in post-menopausal women. Clin. Hemorheol. Microcirc. 2014, 57, 33–47. [Google Scholar] [CrossRef] [PubMed]
- Glass, S.; Dwyer, G.B.; American College of Sports Medicine. ACSM’s Metabolic Calculations Handbook; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2007. [Google Scholar]
- Jennings, A.; Tang, J.; Gillings, R.; Perfecto, A.; Dutton, J.; Speakman, J.; Fraser, W.D.; Nicoletti, C.; Berendsen, A.A.M.; De Groot, L.C.P.G.M.; et al. Changing from a Western to a Mediterranean-style diet does not affect iron or selenium status: Results of the New Dietary Strategies Addressing the Specific Needs of the Elderly Population for Healthy Aging in Europe (NU-AGE) 1-year randomized clinical trial in elderly Europeans. Am. J. Clin. Nutr. 2019, 111, 98–109. [Google Scholar]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. JAMA 2004, 292, 1440–1446. [Google Scholar] [CrossRef]
- McEwan, P.; Ponikowski, P.; Davis, J.A.; Rosano, G.; Coats, A.J.; Dorigotti, F.; O’Sullivan, D.; de Arellano, A.R.; Jankowska, E.A. Ferric carboxymaltose for the treatment of iron deficiency in heart failure: A multinational cost-effectiveness analysis utilising AFFIRM-AHF. Eur. J. Heart Fail. 2021, 23, 1687–1697. [Google Scholar] [CrossRef]
- Comín-Colet, J.; Rubio-Rodríguez, D.; Rubio-Terrés, C.; Enjuanes-Grau, C.; Gutzwiller, F.S.; Anker, S.D.; Ponikowski, P. A cost-effectiveness analysis of ferric carboxymaltose in patients with iron deficiency and chronic heart failure in Spain. Rev. Española Cardiol. 2015, 68, 846–851. [Google Scholar] [CrossRef]
- Calbet, J.A.; Lundby, C.; Koskolou, M.; Boushel, R. Importance of hemoglobin concentration to exercise: Acute manipulations. Respir. Physiol. Neurobiol. 2006, 151, 132–140. [Google Scholar] [CrossRef]
- Chopra, V.K.; Anker, S.D. Anaemia, iron deficiency and heart failure in 2020: Facts and numbers. ESC Heart Fail. 2020, 7, 2007–2011. [Google Scholar] [CrossRef]
- Loncar, G.; Obradovic, D.; Thiele, H.; von Haehling, S.; Lainscak, M. Iron deficiency in heart failure. ESC Heart Fail. 2021, 8, 2368–2379. [Google Scholar] [CrossRef]
- Anker, S.D.; Kirwan, B.-A.; van Veldhuisen, D.J.; Filippatos, G.; Comin-Colet, J.; Ruschitzka, F.; Lüscher, T.F.; Arutyunov, G.P.; Motro, M.; Mori, C.; et al. Effects of ferric carboxymaltose on hospitalisations and mortality rates in iron-deficient heart failure patients: An individual patient data meta-analysis. Eur. J. Heart Fail. 2017, 20, 125–133. [Google Scholar] [CrossRef]
- van Veldhuisen, D.J.; Ponikowski, P.; van der Meer, P.; Metra, M.; Böhm, M.; Doletsky, A.; Voors, A.A.; Roubert, B.; Zakin, L.; Cohen-Solal, A.; et al. Effect of ferric carboxymaltose on exercise capacity in patients with chronic heart failure and iron deficiency. Circulation 2017, 136, 1374–1383. [Google Scholar] [CrossRef]
- Jankowska, E.A.; Tkaczyszyn, M.; Suchocki, T.; Drozd, M.; von Haehling, S.; Doehner, W.; Banasiak, W.; Filippatos, G.; Anker, S.D.; Ponikowski, P. Effects of intravenous iron therapy in iron-deficient patients with systolic heart failure: A meta-analysis of randomized controlled trials. Eur. J. Heart Fail. 2016, 18, 786–795. [Google Scholar] [CrossRef]
- Anker, S.D.; Comin Colet, J.; Filippatos, G.; Willenheimer, R.; Dickstein, K.; Drexler, H.; Lüscher, T.F.; Bart, B.; Banasiak, W.; Niegowska, J.; et al. Ferric carboxymaltose in patients with heart failure and iron deficiency. N. Engl. J. Med. 2009, 361, 2436–2448. [Google Scholar] [CrossRef]
- Jacob, C.; Altevers, J.; Barck, I.; Hardt, T.; Braun, S.; Greiner, W. Retrospective analysis into differences in heart failure patients with and without iron deficiency or anaemia. ESC Heart Fail. 2019, 6, 840–855. [Google Scholar] [CrossRef]
- Malczewska, J.; Błach, W.; Stupnicki, R. The Effects of Physical Exercise on the Concentrations of Ferritin and Transferrin Receptor in Plasma of Female Judoists. Endoscopy 2000, 21, 175–179. [Google Scholar] [CrossRef]
- Jankowska, E.A.; Kasztura, M.; Sokolski, M.; Bronisz, M.; Nawrocka, S.; Oleśkowska-Florek, W.; Zymlinski, R.; Biegus, J.; Siwołowski, P.; Banasiak, W.; et al. Iron deficiency defined as depleted iron stores accompanied by unmet cellular iron requirements identifies patients at the highest risk of death after an episode of acute heart failure. Eur. Heart J. 2014, 35, 2468–2476. [Google Scholar] [CrossRef]
- Löllgen, H.; Leyk, D. Exercise testing in sports medicine. Deutsches Ärzteblatt Int. 2018, 115, 409. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| NYHA 1 | n | NYHA 2&3 | n | p-Value | |
|---|---|---|---|---|---|
| Sex (women/men) | 26/48 | 74 | 74/91 | 165 | 0.159 |
| Age (years) | 65 (36;81) | 74 | 68 (27;94) | 165 | 0.020 |
| Body weight (kg) | 79.2 (53.3;126.0) | 74 | 82.7 (45.3;153.0) | 165 | 0.175 |
| Body mass index [BMI (kg/m2)] | 25.2 (19.1;42.1) | 74 | 28.2 (17.2;52.3) | 165 | 0.001 |
| Body fat [FM (kg)] | 23.3 (6.1;53.8) | 53 | 27.7 (6.1;88.8) | 123 | 0.004 |
| Fat free mass [FFM (kg)] | 55.3 (41.1;79.5) | 53 | 55.4 (33.7;84.6) | 123 | 0.757 |
| Waist circumference (cm) | 96 ± 14 | 73 | 100 ± 14 | 160 | 0.019 |
| Hip circumference (cm) | 101 (85;129) | 70 | 105 (77;150) | 152 | 0.005 |
| Waist-to-hip-ratio | 0.93 ± 0.08 | 70 | 0.95 ± 0.09 | 152 | 0.212 |
| Exercise capacity (wattmax) | 130 (50;267) | 72 | 110 (50;217) | 147 | <0.001 |
| Relative exercise capacity (wattmax/kg) | 1.71 (0.67;2.98) | 72 | 1.28 (0.54;2.60) | 147 | <0.001 |
| Relative oxygen uptake [VO2max/kg (mL/min/kg)] | 21.2 (8.4;37.2) | 68 | 16.3 (9.0;29.5) | 138 | <0.001 |
| Individual aerobic lactate threshold [base lactate + 1.5 mmol/L (mmol/L)] | 2.57 (2.00;4.64) | 71 | 2.50 (2.00;5.42) | 147 | 0.359 |
| Ferritin [F(ng/mL)] | 129 (29;466) | 68 | 125 (10;1269) | 143 | 0.779 |
| CRP (mg/L) | 1.0 (0.6;9.5) | 72 | 1.3 (0.5;43.2) | 160 | 0.047 |
| Soluble transferrin receptor [sTfR(nmol/L)] | 30.4 (8.7;52.8) | 72 | 32.6 (12.8;115.0) | 156 | 0.042 |
| Transferrin saturation [TSF(%)] | 32 (16;62) | 73 | 29 (8;81) | 161 | 0.020 |
| Hemoglobin (g/dL) | 14.3 (11.3;17.3) | 72 | 13.9 (10.4;19.8) | 157 | 0.030 |
| Hematocrit (L/L) | 0.42 ± 0.04 | 72 | 0.41 ± 0.04 | 150 | 0.046 |
| NT-proBNP (ng/L) | 237 (50;1882) | 74 | 320 (36;1848) | 164 | 0.003 |
| KCCQ total score | 90.0 (59;100) | 68 | 73.0 (30;98) | 159 | <0.001 |
| KCCQ functional status score | 93.8 (65.4;100.0) | 68 | 78.6 (25.0;100.0) | 159 | <0.001 |
| KCCQ clinical summery score | 94.0 (57.5;100.0) | 68 | 73.8 (25.0;100.0) | 159 | <0.001 |
| KCCQ symptom scale | 96.9 (57.1;112.5) | 68 | 81.3 (21.9;100.0) | 159 | <0.001 |
| MDS total score | 6.0 (1;13) | 48 | 6.0 (0;13) | 118 | 0.331 |
| Secondary Diagnoses | % |
|---|---|
| Coronary artery disease | 73.2 |
| Hypertension | 68.7 |
| Hypercholesterolemia | 51.5 |
| Atrial fibrillation and other cardiac arrhythmia | 47.0 |
| Vitium cordis | 38.9 |
| History of cardiac support systems; transplants or implants | 38.4 |
| Chronic renal failure | 25.8 |
| Orthopedic impairment | 20.2 |
| Other diseases | 19.7 |
| Diabetes mellitus | 18.2 |
| Obesity | 13.1 |
| Other atherosclerotic diseases | 12.6 |
| Left bundle branch block | 6.6 |
| Malignoma | 5.6 |
| Thyroid disorder | 5.6 |
| Dilated cardiomyopathy | 5.1 |
| Chronic obstructive pulmonary disease and bronchial asthma | 5.1 |
| Pulmonary hypertension | 3.5 |
| Right bundle branch block | 3.5 |
| Neurological and psychiatric disorders | 3.5 |
| Hypertensive heart disease | 3.0 |
| Other cardiomyopathies | 3.0 |
| Normal Iron Status | n | Iron Deficiency | n | Anemia | n | p-Value | η² | |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 68 (30;83] | 109 | 65 (27;81) | 82 | 71 (34;94) | 25 | 0.309 | 0.01 |
| Weight (kg) | 87.8 (55.1;153.0) | 109 | 75.5 (53.2;120.2) | 82 | 72.3 (55.2;94.4) | 25 | 0.012 | 0.04 |
| Body mass index [BMI(kg/m2)] | 27.7 (19.2;52.3) | 109 | 27.3 (17.2;38.2) | 82 | 27.6 (19.0;46.6) | 25 | 0.173 | 0.02 |
| Body fat (kg) | 26.3 (8.9;88.8) | 81 | 27.6 (6.1;50.3) | 64 | 22.4 (7.8;52.4) | 16 | 0.536 | <0.01 |
| Fat free mass [FFM(kg)] | 56.4 (33.7;79.5) a | 81 | 50.4 (36.8;84.6) a | 64 | 58.4 (37.6;71.3) | 16 | 0.010 | 0.06 |
| Waist-to-hip-ratio (WHR) | 0.96 (0.75;1.15) | 102 | 0.92 (0.78;1.07) | 80 | 0.95 (0.69;1.10) | 23 | 0.035 | 0.03 |
| Exercise capacity (wattmax) | 120 (50;250) b | 104 | 110 (50;267) | 78 | 100 (50;160) b | 25 | 0.049 | 0.03 |
| Relative exercise capacity (watt/kg) | 1.45 (0.67;2.68) | 104 | 1.49 (0.54;2.98) c | 78 | 1.11 (0.57;2.60) c | 25 | 0.032 | 0.03 |
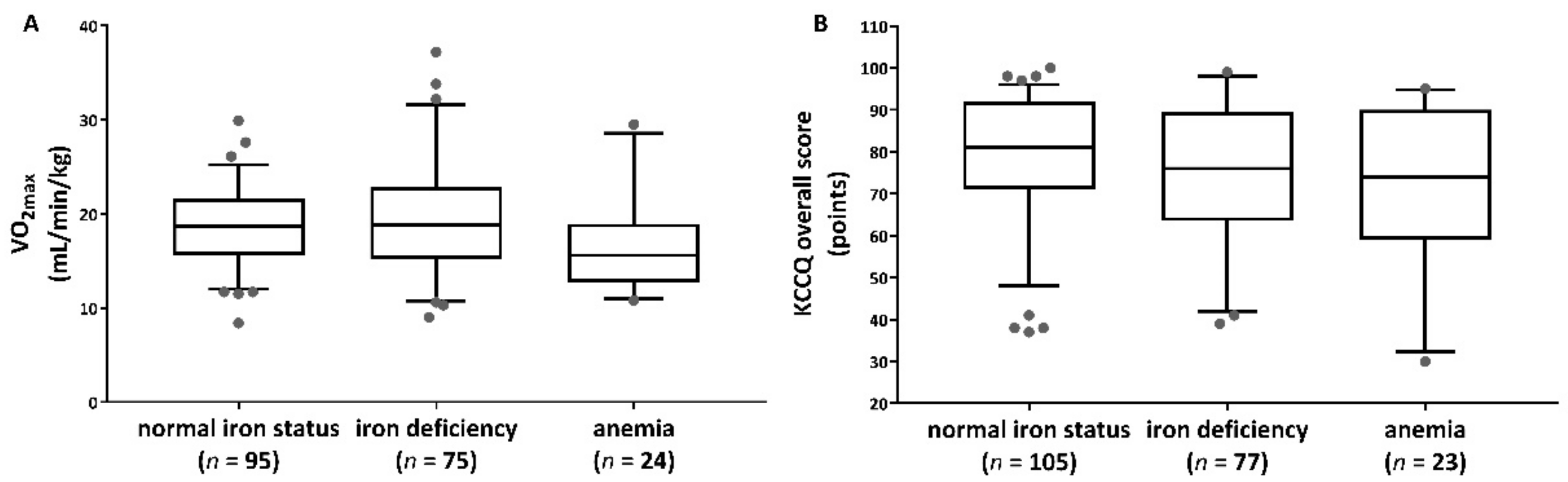
| Oxygen uptake [VO2max (mL/min)] | 1502 (761;2797) b | 95 | 1392 (721;3330) | 75 | 1351 (785;1881) b | 24 | 0.021 | 0.04 |
| Relative oxygen uptake [VO2max/kg (mL/min/kg)] | 18.55 ± 4.05 | 95 | 19.39 ± 5.86 c | 75 | 16.52 ± 4.80 c | 24 | 0.046 | 0.03 |
| Individual aerobic lactate threshold [base lactate + 1.5 mmol/L (mmol/L)] | 2.55 (2.00;5.42) | 104 | 2.49 (2.00;3.98) | 76 | 2.55 (2.06;3.39) | 24 | 0.494 | <0.01 |
| CRP (mg/L) | 1.2 (0.5;23.7) b, c | 109 | 1.0 (0.6;21.9) c | 82 | 2.9 (0.6;43.2) b, c | 24 | 0.002 | 0.06 |
| NT-proBNP (ng/L) | 283 (50;1335) | 109 | 251 (36;1882) | 82 | 335 (127;1304) | 25 | 0.951 | <0.01 |
| KCCQ total score | 81 (37;100) | 105 | 76 (39;99) | 77 | 74 (30;95) | 23 | 0.050 | 0.04 |
| KCCQ functional status score | 88 (34;100) | 104 | 80 (32;100) | 77 | 82 (25;100) | 25 | 0.040 | 0.03 |
| KCCQ clinical summery score | 85 (36;100) | 104 | 79 (37;100) | 77 | 74 (25;100) | 25 | 0.038 | 0.03 |
| KCCQ symptom scale | 89 (34;100) | 104 | 84 (28;113) | 77 | 78 (22;100) | 25 | 0.022 | 0.04 |
| MDS total score | 6 (2;13) | 79 | 6 (1;13) | 58 | 5 (0;10) | 17 | 0.702 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayerle, P.; Beyer, S.; Tegtbur, U.; Kück, M.; Adel, J.; Kwast, S.; Pökel, C.; Kerling, A.; Busse, M. Exercise Capacity, Iron Status, Body Composition, and Mediterranean Diet in Patients with Chronic Heart Failure. Nutrients 2023, 15, 36. https://doi.org/10.3390/nu15010036
Bayerle P, Beyer S, Tegtbur U, Kück M, Adel J, Kwast S, Pökel C, Kerling A, Busse M. Exercise Capacity, Iron Status, Body Composition, and Mediterranean Diet in Patients with Chronic Heart Failure. Nutrients. 2023; 15(1):36. https://doi.org/10.3390/nu15010036
Chicago/Turabian StyleBayerle, Pauline, Sebastian Beyer, Uwe Tegtbur, Momme Kück, John Adel, Stefan Kwast, Christoph Pökel, Arno Kerling, and Martin Busse. 2023. "Exercise Capacity, Iron Status, Body Composition, and Mediterranean Diet in Patients with Chronic Heart Failure" Nutrients 15, no. 1: 36. https://doi.org/10.3390/nu15010036
APA StyleBayerle, P., Beyer, S., Tegtbur, U., Kück, M., Adel, J., Kwast, S., Pökel, C., Kerling, A., & Busse, M. (2023). Exercise Capacity, Iron Status, Body Composition, and Mediterranean Diet in Patients with Chronic Heart Failure. Nutrients, 15(1), 36. https://doi.org/10.3390/nu15010036