Association between Different Types of Plant-Based Diets and Dyslipidemia in Middle-Aged and Elderly Chinese Participants


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Physical Examination and Biochemical Assays
2.3. Definition of Diagnostic Criteria and Related Indicators
2.4. Assessment of PDI Score
2.5. Assessment of Covariates
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Samples
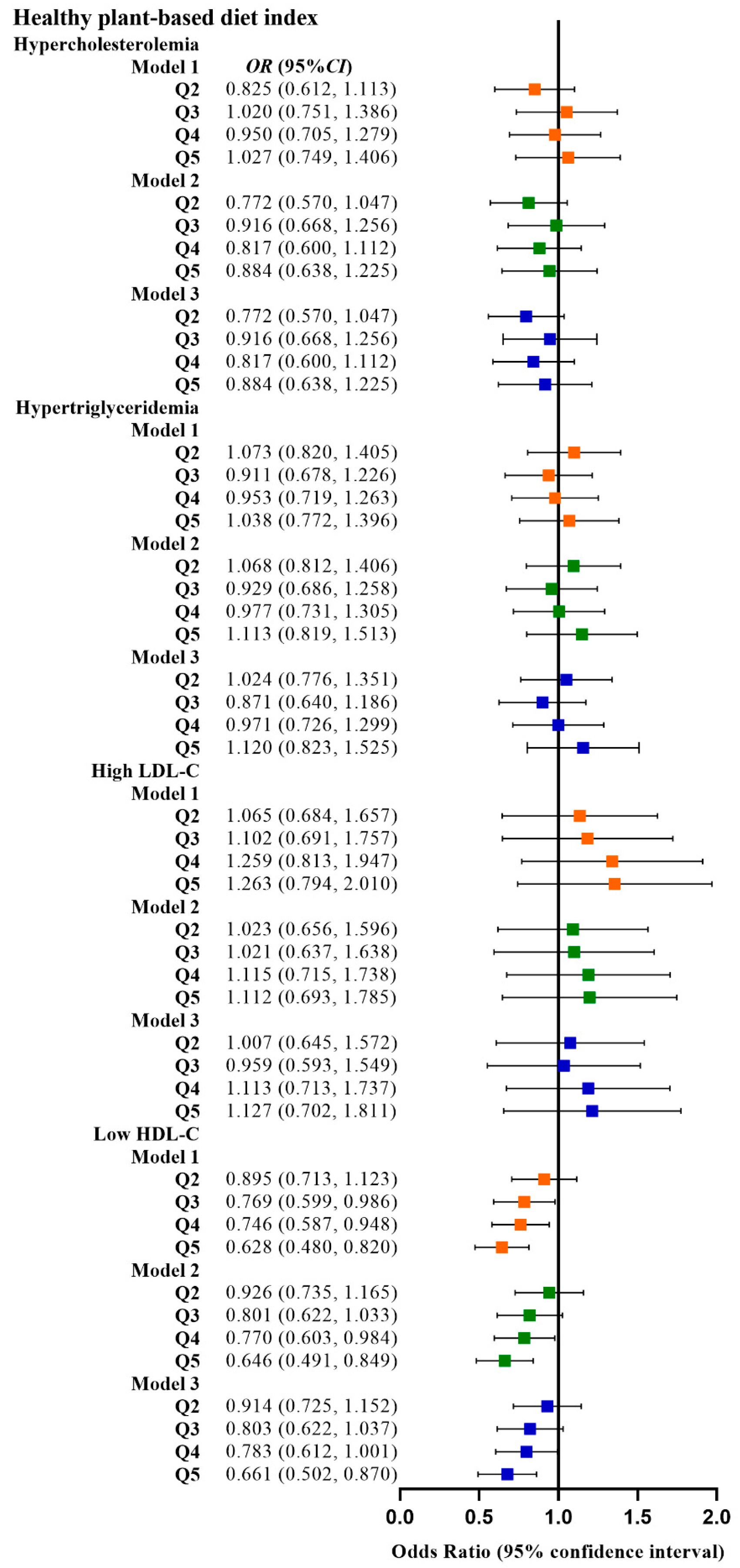
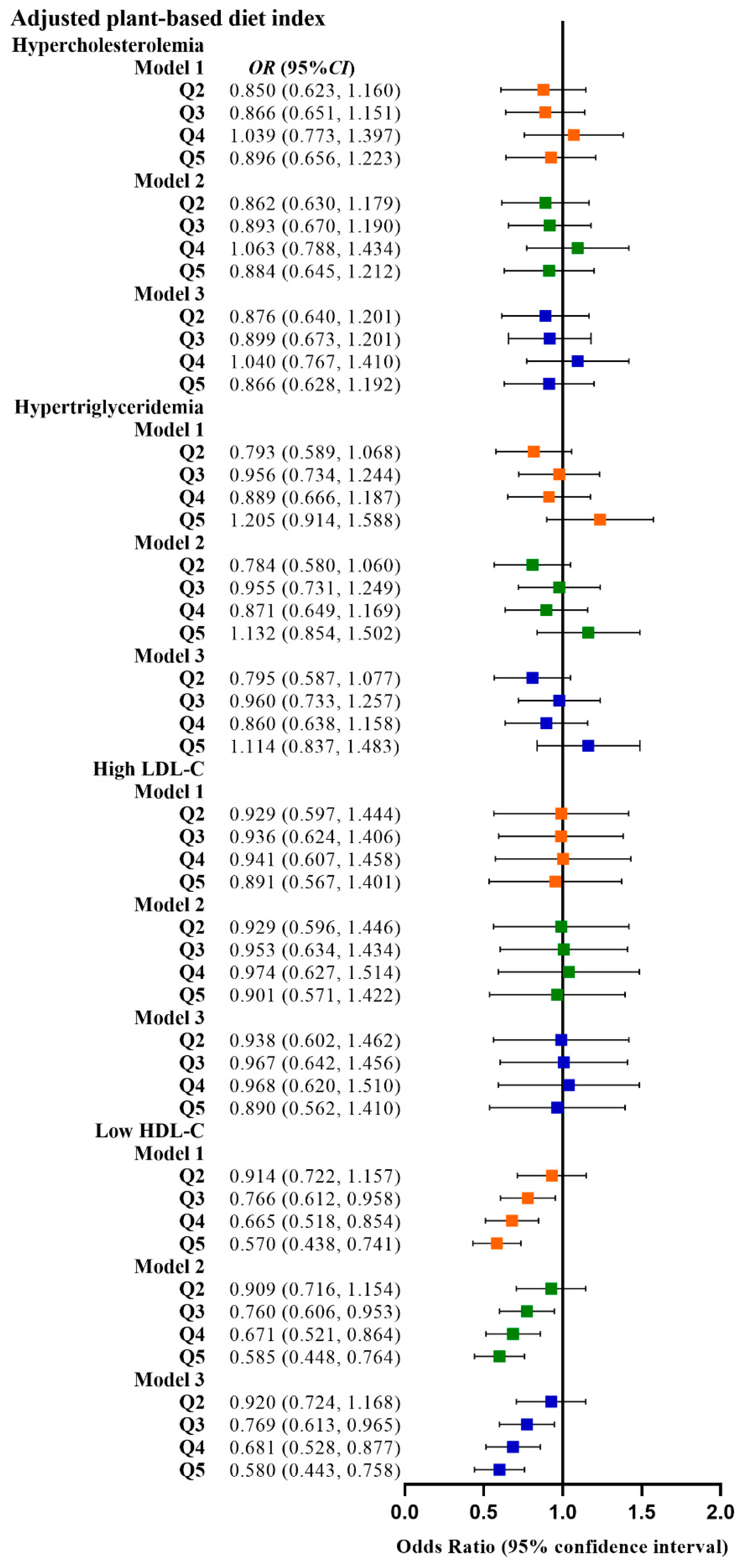
3.2. Correlation between PDI and Dyslipidemia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kopin, L.; Lowenstein, C. Dyslipidemia. Ann. Intern. Med. 2017, 167, ITC81–ITC96. [Google Scholar] [CrossRef] [PubMed]
- Sandesara, P.B.; Virani, S.S.; Fazio, S.; Shapiro, M.D. The Forgotten Lipids: Triglycerides, Remnant Cholesterol, and Atherosclerotic Cardiovascular Disease Risk. Endocr. Rev. 2019, 40, 537–557. [Google Scholar] [CrossRef] [PubMed]
- Atar, D.; Jukema, J.W.; Molemans, B.; Taub, P.R.; Goto, S.; Mach, F.; CerezoOlmos, C.; Underberg, J.; Keech, A.; Tokgözoğlu, L.; et al. New cardiovascular prevention guidelines: How to optimally manage dyslipidaemia and cardiovascular risk in 2021 in patients needing secondary prevention? Atherosclerosis 2021, 319, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhang, H.; Lu, J.; Ding, Q.; Li, X.; Wang, X.; Sun, D.; Tan, L.; Mu, L.; Liu, J.; et al. Prevalence of Dyslipidemia and Availability of Lipid-Lowering Medications Among Primary Health Care Settings in China. JAMA Netw. Open 2021, 4, e2127573. [Google Scholar] [CrossRef] [PubMed]
- Pirillo, A.; Casula, M.; Olmastroni, E.; Norata, G.D.; Catapano, A.L. Global epidemiology of dyslipidaemias. Nat. Rev. Cardiol. 2021, 18, 689–700. [Google Scholar] [CrossRef]
- Pirillo, A.; Norata, G.D.; Catapano, A.L. Worldwide Changes in Total Cholesterol and Non-HDL-Cholesterol Trends Indicate Where the Challenges Are for the Coming Years. Clin. Chem. 2021, 67, 30–32. [Google Scholar] [CrossRef]
- Du, H.; Shi, Q.; Song, P.; Pan, X.; Yang, X.; Chen, L.; He, Y.; Zong, G.; Zhu, Y.; Su, B.; et al. Global Burden Attributable to High Low-Density Lipoprotein-Cholesterol From 1990 to 2019. Front. Cardiovasc. Med. 2022, 9, 903126. [Google Scholar] [CrossRef]
- Kim, S.A.; Shin, S. Dietary Patterns and the Risk of Dyslipidemia in Korean Adults: A Prospective Cohort Study Based on the Health Examinees (HEXA) Study. J. Acad. Nutr. Diet 2021, 121, 1242–1257.e1242. [Google Scholar] [CrossRef]
- Song, S.; Paik, H.Y.; Park, M.; Song, Y. Dyslipidemia patterns are differentially associated with dietary factors. Clin. Nutr. 2016, 35, 885–891. [Google Scholar] [CrossRef]
- Wallace, T.C.; Bailey, R.L.; Blumberg, J.B.; Burton-Freeman, B.; Chen, C.O.; Crowe-White, K.M.; Drewnowski, A.; Hooshmand, S.; Johnson, E.; Lewis, R.; et al. Fruits, vegetables, and health: A comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake. Crit. Rev. Food Sci. Nutr. 2020, 60, 2174–2211. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Levin, S.M.; Barnard, N.D. Association between plant-based diets and plasma lipids: A systematic review and meta-analysis. Nutr. Rev. 2017, 75, 683–698. [Google Scholar] [CrossRef]
- Wang, F.; Zheng, J.; Yang, B.; Jiang, J.; Fu, Y.; Li, D. Effects of Vegetarian Diets on Blood Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2015, 4, e002408. [Google Scholar] [CrossRef]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Cardiovascular Disease Prevention: All Plant Foods Are Not Created Equal. Curr. Atheroscler. Rep. 2019, 21, 18. [Google Scholar] [CrossRef]
- Wang, F.; Ugai, T.; Haruki, K.; Wan, Y.; Akimoto, N.; Arima, K.; Zhong, R.; Twombly, T.S.; Wu, K.; Yin, K.; et al. Healthy and unhealthy plant-based diets in relation to the incidence of colorectal cancer overall and by molecular subtypes. Clin. Transl. Med. 2022, 12, e893. [Google Scholar] [CrossRef]
- Haslam, D.E.; Peloso, G.M.; Herman, M.A.; Dupuis, J.; Lichtenstein, A.H.; Smith, C.E.; McKeown, N.M. Beverage Consumption and Longitudinal Changes in Lipoprotein Concentrations and Incident Dyslipidemia in US Adults: The Framingham Heart Study. J. Am. Heart Assoc. 2020, 9, e014083. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef]
- Wang, F.; Baden, M.Y.; Guasch-Ferré, M.; Wittenbecher, C.; Li, J.; Li, Y.; Wan, Y.; Bhupathiraju, S.N.; Tobias, D.K.; Clish, C.B.; et al. Plasma metabolite profiles related to plant-based diets and the risk of type 2 diabetes. Diabetologia 2022, 65, 1119–1132. [Google Scholar] [CrossRef]
- Chen, B.; Zeng, J.; Qin, M.; Xu, W.; Zhang, Z.; Li, X.; Xu, S. The Association between Plant-Based Diet Indices and Obesity and Metabolic Diseases in Chinese Adults: Longitudinal Analyses From the China Health and Nutrition Survey. Front. Nutr. 2022, 9, 881901. [Google Scholar] [CrossRef]
- Pereira, P.M.; Vicente, A.F. Meat nutritional composition and nutritive role in the human diet. Meat Sci. 2013, 93, 586–592. [Google Scholar] [CrossRef]
- NW, S.; AJ, F.; JP, H.; WC, M. Modeling the Contribution of Meat to Global Nutrient Availability. Front. Nutr. 2022, 9, 766796. [Google Scholar]
- Mohanty, B.P.; Mahanty, A.; Ganguly, S.; Mitra, T.; Karunakaran, D.; Anandan, R. Nutritional composition of food fishes and their importance in providing food and nutritional security. Food Chem. 2019, 293, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, D.A.; Durrant, C.; Elliott, J.; Givens, D.I.; Lovegrove, J.A. Diets containing the highest levels of dairy products are associated with greater eutrophication potential but higher nutrient intakes and lower financial cost in the United Kingdom. Eur. J. Nutr. 2020, 59, 895–908. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Dinu, M.; Pagliai, G.; Cesari, F.; Gori, A.M.; Sereni, A.; Becatti, M.; Fiorillo, C.; Marcucci, R.; Casini, A. Low-Calorie Vegetarian Versus Mediterranean Diets for Reducing Body Weight and Improving Cardiovascular Risk Profile: CARDIVEG Study (Cardiovascular Prevention with Vegetarian Diet). Circulation 2018, 137, 1103–1113. [Google Scholar] [CrossRef]
- Termannsen, A.D.; Clemmensen, K.K.B.; Thomsen, J.M.; Norgaard, O.; Diaz, L.J.; Torekov, S.S.; Quist, J.S.; Faerch, K. Effects of vegan diets on cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2022, 23, e13462. [Google Scholar] [CrossRef]
- Rees, K.; Al-Khudairy, L.; Takeda, A.; Stranges, S. Vegan dietary pattern for the primary and secondary prevention of cardiovascular diseases. Cochrane Database Syst. Rev. 2021, 2, CD013501. [Google Scholar] [CrossRef]
- Tao, L.; Tian, T.; Liu, L.; Zhang, Z.; Sun, Q.; Sun, G.; Dai, J.; Yan, H. Cohort profile: The Xinjiang Multiethnic Cohort (XMC) study. BMJ Open 2022, 12, e048242. [Google Scholar] [CrossRef]
- Joint Committee for Developing Chinese guidelines on Prevention and Treatment of Dyslipidemia in Adults. Guidelines for the prevention and treatment of dyslipidemia in Chinese adults (2016 revision). Chin. Circ. J. 2016, 31, 937–953. [Google Scholar]
- Martin, C.; Zhang, Y.; Tonelli, C.; Petroni, K. Plants, diet, and health. Annu. Rev. Plant Biol. 2013, 64, 19–46. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Chen, Z.; Drouin-Chartier, J.P.; Li, Y.; Baden, M.Y.; Manson, J.E.; Willett, W.C.; Voortman, T.; Hu, F.B.; Bhupathiraju, S.N. Changes in Plant-Based Diet Indices and Subsequent Risk of Type 2 Diabetes in Women and Men: Three U.S. Prospective Cohorts. Diabetes Care 2021, 44, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Malik, V.; Rimm, E.B.; Sacks, F.; Willett, W.; Hu, F.B. Changes in intake of plant-based diets and weight change: Results from 3 prospective cohort studies. Am. J. Clin. Nutr. 2019, 110, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.J.; Mangels, A.R.; American Dietetic, A. Position of the American Dietetic Association: Vegetarian diets. J. Am. Diet Assoc. 2009, 109, 1266–1282. [Google Scholar] [PubMed]
- Tong, T.Y.N.; Appleby, P.N.; Bradbury, K.E.; Perez-Cornago, A.; Travis, R.C.; Clarke, R.; Key, T.J. Risks of ischaemic heart disease and stroke in meat eaters, fish eaters, and vegetarians over 18 years of follow-up: Results from the prospective EPIC-Oxford study. BMJ 2019, 366, l4897. [Google Scholar] [CrossRef]
- Derbyshire, E. Could we be overlooking a potential choline crisis in the United Kingdom? BMJ Nutr. Prev. Health 2019, 2, 86–89. [Google Scholar] [CrossRef]
- Chazelas, E.; Srour, B.; Desmetz, E.; Kesse-Guyot, E.; Julia, C.; Deschamps, V.; Druesne-Pecollo, N.; Galan, P.; Hercberg, S.; Latino-Martel, P.; et al. Sugary drink consumption and risk of cancer: Results from NutriNet-Sante prospective cohort. BMJ 2019, 366, l2408. [Google Scholar] [CrossRef]
- Lee, K.; Kim, H.; Rebholz, C.M.; Kim, J. Association between Different Types of Plant-Based Diets and Risk of Dyslipidemia: A Prospective Cohort Study. Nutrients 2021, 13, 220. [Google Scholar] [CrossRef]
- Cabrera, M.C.; Saadoun, A. An overview of the nutritional value of beef and lamb meat from South America. Meat Sci. 2014, 98, 435–444. [Google Scholar] [CrossRef]
- Rehault-Godbert, S.; Guyot, N.; Nys, Y. The Golden Egg: Nutritional Value, Bioactivities, and Emerging Benefits for Human Health. Nutrients 2019, 11, 684. [Google Scholar] [CrossRef]
- Al-Shaar, L.; Satija, A.; Wang, D.D.; Rimm, E.B.; Smith-Warner, S.A.; Stampfer, M.J.; Hu, F.B.; Willett, W.C. Red meat intake and risk of coronary heart disease among US men: Prospective cohort study. BMJ 2020, 371, m4141. [Google Scholar] [CrossRef]
- Zheng, Y.; Li, Y.; Satija, A.; Pan, A.; Sotos-Prieto, M.; Rimm, E.; Willett, W.C.; Hu, F.B. Association of changes in red meat consumption with total and cause specific mortality among US women and men: Two prospective cohort studies. BMJ 2019, 365, l2110. [Google Scholar] [CrossRef]
- Chinese Nutrition Society. Dietary Guidelines for Chinese Residents: 2022; People’s Medical Publishing House: Beijing, China, 2022. [Google Scholar]
- Rohrmann, S.; Linseisen, J. Processed meat: The real villain? Proc. Nutr. Soc. 2016, 75, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef] [PubMed]
- Mateș, L.; Popa, D.S.; Rusu, M.E.; Fizeșan, I.; Leucuța, D. Walnut Intake Interventions Targeting Biomarkers of Metabolic Syndrome and Inflammation in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2022, 11, 1412. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.S.; Sarker, M.Z.; Ferdosh, S.; Akanda, M.J.; Easmin, M.S.; Bt Shamsudin, S.H.; Bin Yunus, K. Phytosterols and their extraction from various plant matrices using supercritical carbon dioxide: A review. J. Sci. Food Agric. 2015, 95, 1385–1394. [Google Scholar] [CrossRef]
- Van Hung, P. Phenolic Compounds of Cereals and Their Antioxidant Capacity. Crit. Rev. Food Sci. Nutr. 2016, 56, 25–35. [Google Scholar] [CrossRef]
- Chávez-Santoscoy, R.A.; Gutiérrez-Uribe, J.A.; Serna-Saldívar, S.O. Effect of Flavonoids and Saponins Extracted from Black Bean (Phaseolus vulgaris L.) Seed Coats as Cholesterol Micelle Disruptors. Plant Foods Hum. Nutr. 2013, 68, 416–423. [Google Scholar] [CrossRef]
- Chen, Z.F.; Zhao, B.; Tang, X.Y.; Li, W.; Zhu, L.L.; Tang, C.S.; DU, J.B.; Jin, H.F. Hydrogen sulfide regulates vascular endoplasmic reticulum stress in apolipoprotein E knockout mice. Chin. Med. J. 2011, 124, 3460–3467. [Google Scholar]
- Kjlbk, L.; Lorenzen, J.K.; Larsen, L.H.; Astrup, A. Calcium intake and the associations with faecal fat and energy excretion, and lipid profile in a free-living population. J. Nutr. Sci. 2017, 6, e50. [Google Scholar] [CrossRef]
- Huo Yung Kai, S.; Bongard, V.; Simon, C.; Ruidavets, J.B.; Arveiler, D.; Dallongeville, J.; Wagner, A.; Amouyel, P.; Ferrieres, J. Low-fat and high-fat dairy products are differently related to blood lipids and cardiovascular risk score. Eur. J. Prev. Cardiol. 2014, 21, 1557–1567. [Google Scholar]
- Trichia, E.; Luben, R.; Khaw, K.T.; Wareham, N.J.; Imamura, F.; Forouhi, N.G. The associations of longitudinal changes in consumption of total and types of dairy products and markers of metabolic risk and adiposity: Findings from the European Investigation into Cancer and Nutrition (EPIC)-Norfolk study, United Kingdom. Am. J. Clin. Nutr. 2020, 111, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Hustad, K.S.; Rundblad, A.; Ottestad, I.; Christensen, J.J.; Holven, K.B.; Ulven, S.M. Comprehensive lipid and metabolite profiling in healthy adults with low and high consumption of fatty fish: A cross-sectional study. Br. J. Nutr. 2021, 125, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.H.; Amar, M.; Sorokin, A.V.; Troendle, J.; Courville, A.B.; Sampson, M.; Playford, M.P.; Yang, S.; Stagliano, M.; Ling, C.; et al. Supplementation with saury oil, a fish oil high in omega-11 monounsaturated fatty acids, improves plasma lipids in healthy subjects. J. Clin. Lipidol. 2020, 14, 53–65.e2. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
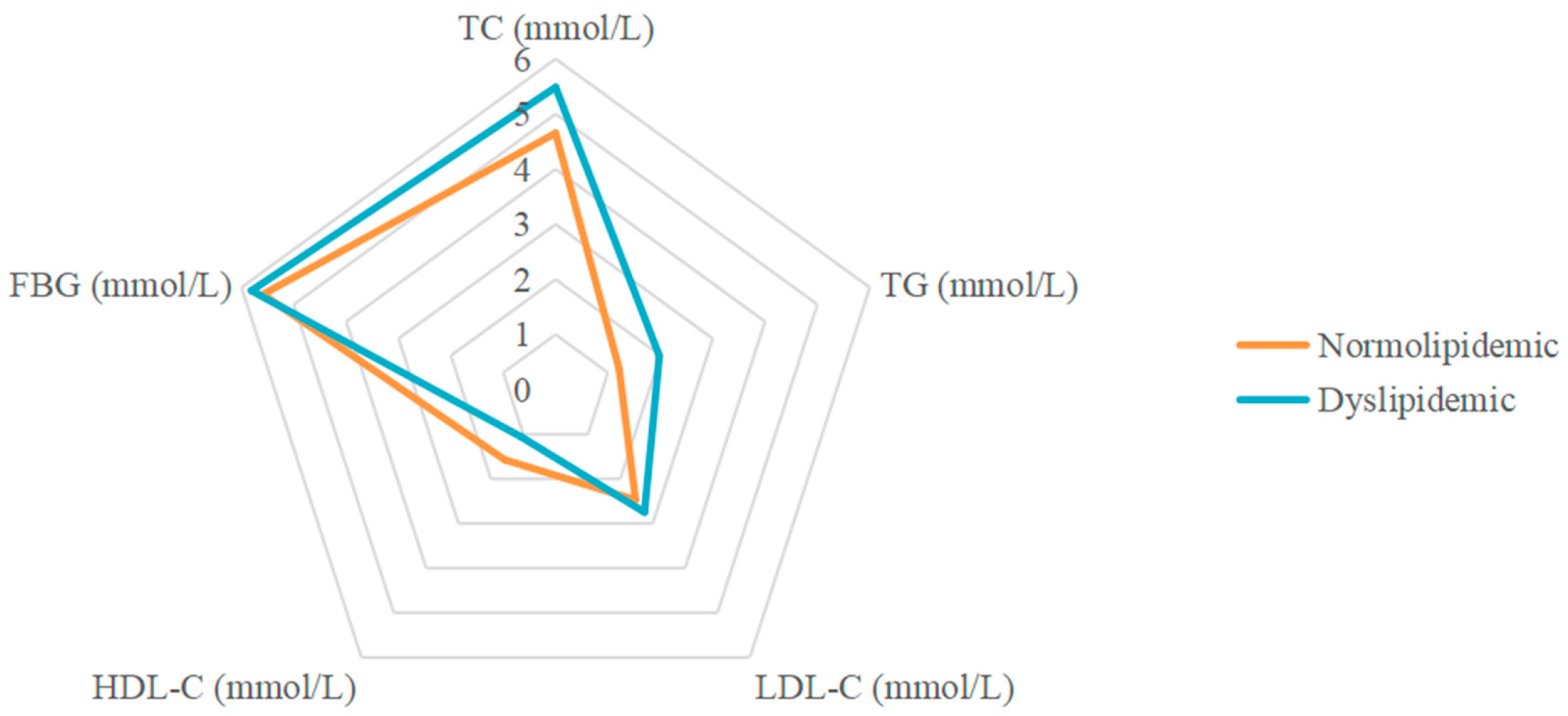
| Dyslipidemic Participants (n = 1501) | Normolipidemic Participants (n = 2595) | p-Value | |
|---|---|---|---|
| Sex, n (%) | 0.010 | ||
| Male | 714 (47.6) | 1126 (43.4) | |
| Female | 787 (52.4) | 1469 (56.6) | |
| Age (years) | 51.42 ± 10.16 | 51.04 ± 10.19 | 0.247 |
| Ethnicity, n (%) | <0.001 | ||
| Han | 182 (12.1) | 337 (13.0) | |
| Hui | 516 (34.4) | 745 (28.7) | |
| Uygur | 282 (18.8) | 914 (35.2) | |
| Kazak | 489 (32.6) | 550 (21.2) | |
| other | 32 (2.1) | 49 (1.9) | |
| Body mass index (kg/m2) | 26.80 ± 4.14 | 26.14 ± 4.30 | <0.001 |
| Socio-economic status, n (%) | 0.254 | ||
| Low | 846 (56.4) | 1451 (55.9) | |
| Medium | 619 (41.2) | 1100 (42.4) | |
| High | 36 (2.4) | 44 (1.7) | |
| Marriage | 0.519 | ||
| Married | 1331 (88.7) | 2318 (89.3) | |
| Other | 170 (11.3) | 277 (10.7) | |
| Smoking status, n (%) | 0.114 | ||
| Never | 1135 (75.6) | 2030 (78.2) | |
| Occasionally | 30 (2.0) | 55 (2.1) | |
| Every day | 336 (22.4) | 510 (19.7) | |
| Alcohol drinking, n (%) | 0.322 | ||
| Never | 1250 (83.3) | 2207 (85.0) | |
| Occasionally | 230 (15.3) | 355 (13.7) | |
| Weekly | 21 (1.4) | 33 (1.3) | |
| Physical activity, n (%) | 0.531 | ||
| Never | 1237 (82.4) | 2119 (81.7) | |
| Occasionally | 211 (14.1) | 366 (14.1) | |
| Weekly | 53 (3.5) | 110 (4.2) | |
| FPG (mmol/L) | 5.81 ± 2.05 | 5.59 ± 1.40 | <0.001 |
| TC (mmol/L) | 5.49 ± 1.66 | 4.65 ± 0.79 | <0.001 |
| TG (mmol/L) | 1.98 ± 1.48 | 1.21 ± 0.46 | <0.001 |
| LDL-C (mmol/L) | 2.75 ± 1.37 | 2.47 ± 0.53 | <0.001 |
| HDL-C (mmol/L) | 1.06 ± 0.90 | 1.57 ± 0.49 | <0.001 |
| TC/HDL-C (M (P25, P75)) | 4.89 (3.87, 15.50) | 3.09 (2.56, 3.59) | <0.001 |
| LDL-C/HDL-C ((P25, P75)) | 2.62 (1.98, 5.58) | 1.66 (1.32, 1.95) | <0.001 |
| AIP (M (P25, P75)) | 0.33 (0.06, 0.62) | −0.11 (−0.28, 0.03) | <0.001 |
| Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | |
| Overall plant-based diet index | ||||||||||
| Model 1 | 1 (Reference) | 0.865 (0.710, 1.055) | 0.152 | 0.787 (0.648, 0.955) | 0.015 | 0.801 (0.662, 0.969) | 0.022 | 0.835 (0.680, 1.025) | 0.085 | |
| Model 2 | 1 (Reference) | 0.864 (0.708, 1.055) | 0.152 | 0.784 (0.645, 0.953) | 0.015 | 0.794 (0.655, 0.962) | 0.018 | 0.832 (0.676, 1.023) | 0.080 | |
| Model 3 | 1 (Reference) | 0.855 (0.699, 1.046) | 0.128 | 0.780 (0.641, 0.949) | 0.013 | 0.799 (0.659, 0.970) | 0.023 | 0.825 (0.670, 1.017) | 0.071 | |
| Healthful plant-based diet index | ||||||||||
| Model 1 | 1 (Reference) | 0.961 (0.795, 1.162) | 0.681 | 0.874 (0.713, 1.072) | 0.197 | 0.906 (0.746, 1.102) | 0.324 | 0.894 (0.725, 1.102) | 0.293 | |
| Model 2 | 1 (Reference) | 0.964 (0.796, 1.169) | 0.712 | 0.885 (0.719, 1.089) | 0.248 | 0.899 (0.737, 1.098) | 0.297 | 0.890 (0.718, 1.103) | 0.288 | |
| Model 3 | 1 (Reference) | 0.941 (0.776, 1.142) | 0.540 | 0.867 (0.703, 1.069) | 0.181 | 0.893 (0.731, 1.092) | 0.272 | 0.893 (0.720, 1.109) | 0.306 | |
| Unhealthful plant-based diet index | ||||||||||
| Model 1 | 1 (Reference) | 1.068 (0.871, 1.309) | 0.528 | 1.047 (0.859, 1.277) | 0.649 | 1.187 (0.976, 1.444) | 0.086 | 1.019 (0.838, 1.240) | 0.847 | |
| Model 2 | 1 (Reference) | 1.067 (0.869, 1.310) | 0.536 | 1.068 (0.873, 1.305) | 0.524 | 1.233 (1.010, 1.505) | 0.039 | 1.065 (0.871, 1.302) | 0.541 | |
| Model 3 | 1 (Reference) | 1.036 (0.842, 1.275) | 0.736 | 1.058 (0.864, 1.296) | 0.584 | 1.208 (0.988, 1.477) | 0.065 | 1.042 (0.851, 1.277) | 0.689 | |
| Adjusted plant-based diet index | ||||||||||
| Model 1 | 1 (Reference) | 0.836 (0.684, 1.020) | 0.077 | 0.864 (0.719, 1.038) | 0.119 | 0.760 (0.622, 0.929) | 0.007 | 0.752 (0.614, 0.923) | 0.006 | |
| Model 2 | 1 (Reference) | 0.838 (0.686, 1.025) | 0.085 | 0.873 (0.725, 1.050) | 0.149 | 0.771 (0.630, 0.944) | 0.012 | 0.752 (0.612, 0.925) | 0.007 | |
| Model 3 | 1 (Reference) | 0.854 (0.697, 1.045) | 0.125 | 0.881 (0.731, 1.061) | 0.182 | 0.770 (0.628, 0.945) | 0.012 | 0.748 (0.607, 0.921) | 0.006 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Li, Y.; Liu, Y.; Zhang, H.; Qiao, T.; Chu, L.; Luo, T.; Zhang, Z.; Dai, J. Association between Different Types of Plant-Based Diets and Dyslipidemia in Middle-Aged and Elderly Chinese Participants. Nutrients 2023, 15, 230. https://doi.org/10.3390/nu15010230
Wang L, Li Y, Liu Y, Zhang H, Qiao T, Chu L, Luo T, Zhang Z, Dai J. Association between Different Types of Plant-Based Diets and Dyslipidemia in Middle-Aged and Elderly Chinese Participants. Nutrients. 2023; 15(1):230. https://doi.org/10.3390/nu15010230
Chicago/Turabian StyleWang, Lu, Yuanyuan Li, Yan Liu, Huanwen Zhang, Tingting Qiao, Lei Chu, Tao Luo, Zewen Zhang, and Jianghong Dai. 2023. "Association between Different Types of Plant-Based Diets and Dyslipidemia in Middle-Aged and Elderly Chinese Participants" Nutrients 15, no. 1: 230. https://doi.org/10.3390/nu15010230
APA StyleWang, L., Li, Y., Liu, Y., Zhang, H., Qiao, T., Chu, L., Luo, T., Zhang, Z., & Dai, J. (2023). Association between Different Types of Plant-Based Diets and Dyslipidemia in Middle-Aged and Elderly Chinese Participants. Nutrients, 15(1), 230. https://doi.org/10.3390/nu15010230