
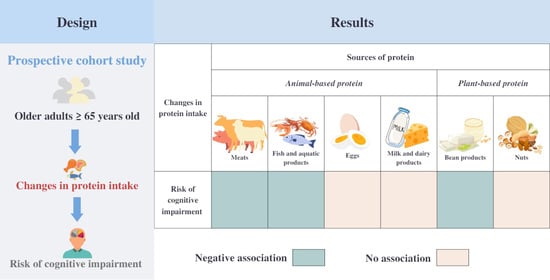
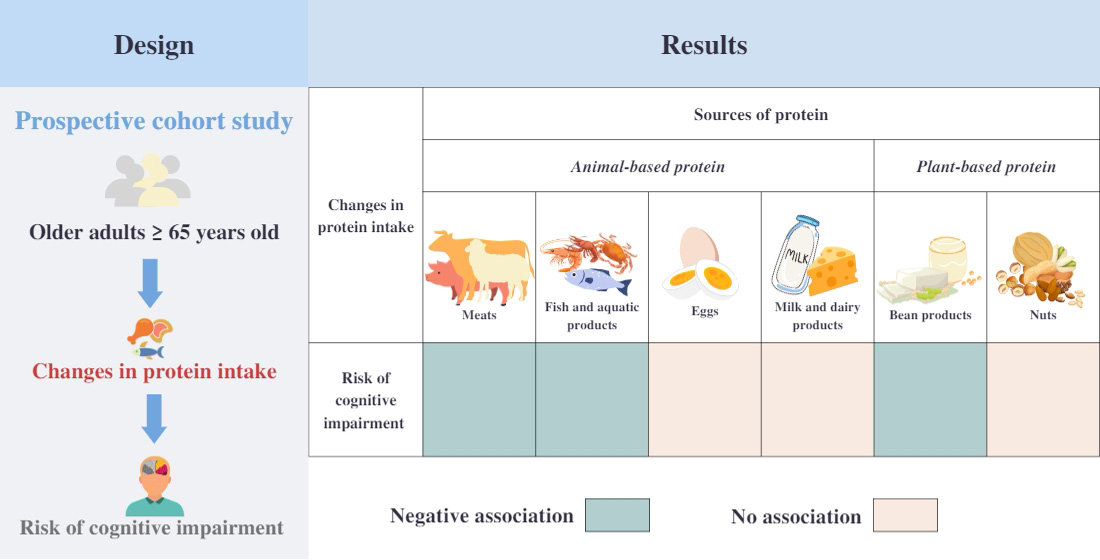
Association between Changes in Protein Intake and Risk of Cognitive Impairment: A Prospective Cohort Study


Abstract
1. Introduction
2. Materials and Methods
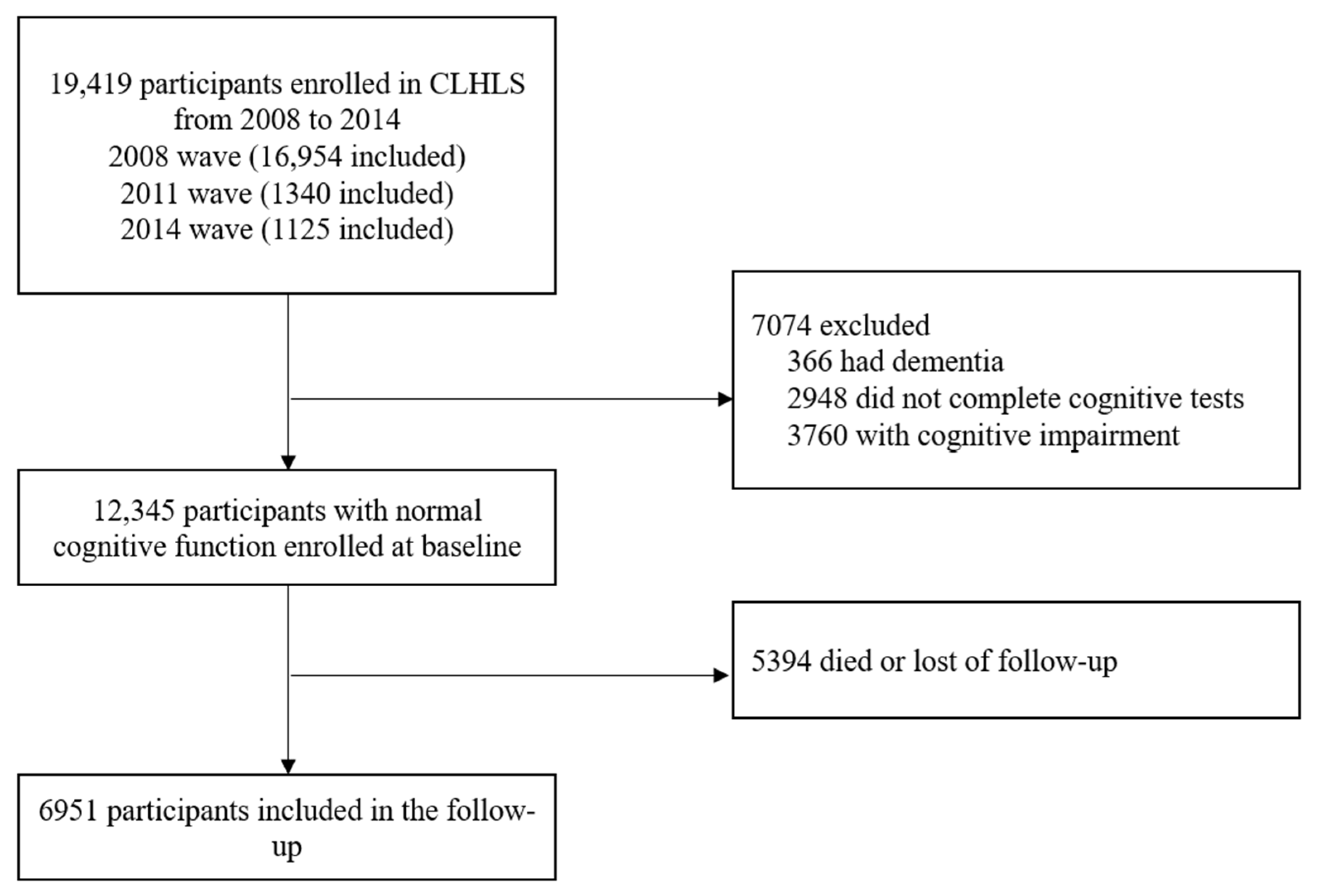
2.1. Study Design, Participants and Procedures
2.2. Measurement of Protein Intake
2.3. Cognitive Assessment
2.4. Covariates
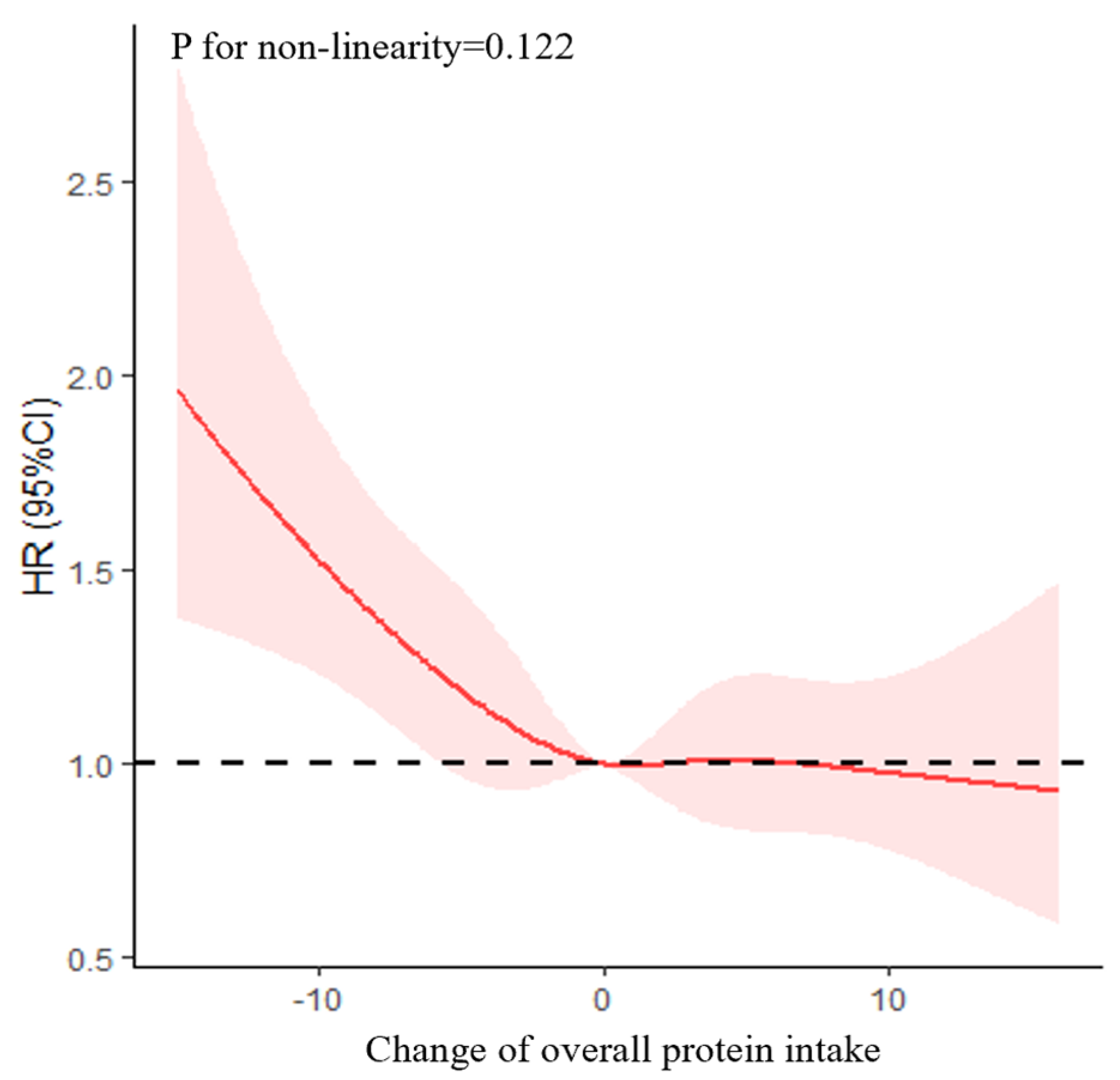
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Dementia. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 28 November 2022).
- Alzheimer’s Disease International. Dementia Statistics. 2019. Available online: https://www.alz.co.uk/research/statistics (accessed on 28 November 2022).
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for cognitive impairment in older adults: Updated evidence report and systematic review for the US preventive services task force. JAMA 2020, 323, 764–785. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia. 2019. Available online: https://www.who.int/publications/i/item/risk-reduction-of-cognitive-decline-and-dementia (accessed on 9 December 2022).
- Chen, X.; Maguire, B.; Brodaty, H.; O’Leary, F. Dietary patterns and cognitive health in older adults: A systematic review. J. Alzheimer’s Dis. 2019, 67, 583–619. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Calvani, R.; Landi, F.; Picca, A.; Marzetti, E. Protein intake and cognitive function in older adults: A systematic review and meta-analysis. Nutr. Metab. Insights 2021, 14, 11786388211022373. [Google Scholar] [CrossRef] [PubMed]
- Wu, G. Dietary protein intake and human health. Food Funct. 2016, 7, 1251–1265. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Wang, W.; Zhang, D. Association between dietary protein intake and cognitive function in adults aged 60 years and older. J. Nutr. Health Aging 2020, 24, 223–229. [Google Scholar] [CrossRef]
- Gao, R.; Yang, Z.; Yan, W.; Du, W.; Zhou, Y.; Zhu, F. Protein intake from different sources and cognitive decline over 9 years in community-dwelling older adults. Front. Public Health 2022, 10, 1016016. [Google Scholar] [CrossRef]
- Richter, C.K.; Skulas-Ray, A.C.; Champagne, C.M.; Kris-Etherton, P.M. Plant protein and animal proteins: Do they differentially affect cardiovascular disease risk? Adv. Nutr. 2015, 6, 712–728. [Google Scholar] [CrossRef]
- Shang, X.; Scott, D.; Hodge, A.; English, D.R.; Giles, G.G.; Ebeling, P.R.; Sanders, K.M. Dietary protein from different food sources, incident metabolic syndrome and changes in its components: An 11-year longitudinal study in healthy community-dwelling adults. Clin. Nutr. 2017, 36, 1540–1548. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Association of changes in diet quality with total and cause-specific mortality. N. Engl. J. Med. 2017, 377, 143–153. [Google Scholar] [CrossRef]
- Xu, X.Y.; Wang, S.S.; Niu, L.; Leung, I.S.H.; Tian, Q.B. Association of leisure activity changes and reversion from mild cognitive impairment to normal cognitive function among older adults: A prospective cohort study. Front. Public Health 2022, 10, 1035762. [Google Scholar] [CrossRef] [PubMed]
- Yi, Z. Introduction to the Chinese Longitudinal Healthy Longevity Survey (CLHLS). In Healthy Longevity in China: Demographic, Socioeconomic, and Psychological Dimension; Yi, Z., Poston, D.L., Vlosky, D.A., Gu, D., Eds.; Springer: Dordrecht, The Netherlands, 2008; pp. 23–38. [Google Scholar]
- Zeng, Y.; Feng, Q.; Hesketh, T.; Christensen, K.; Vaupel, J.W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 2017, 389, 1619–1629. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.-H.; Huang, Z.-P.; Zhang, X.; He, L.; Willett, W.; Wang, J.-L.; Hasegawa, K.; Chen, J.-S. Reproducibility and validity of a Chinese food frequency questionnaire. Biomed. Environ. Sci. 2010, 23, 1–38. [Google Scholar] [CrossRef]
- Zhang, Y.; Jin, X.; Lutz, M.W.; Ju, S.-Y.; Liu, K.; Guo, G.; Zeng, Y.; Yao, Y. Interaction between APOE ε4 and dietary protein intake on cognitive decline: A longitudinal cohort study. Clin. Nutr. 2021, 40, 2716–2725. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Jia, X.; Wang, Z.; Huang, F.; Su, C.; Du, W.; Jiang, H.; Wang, H.; Wang, J.; Wang, F.; Su, W.; et al. A comparison of the Mini-Mental State Examination (MMSE) with the Montreal Cognitive Assessment (MoCA) for mild cognitive impairment screening in Chinese middle-aged and older population: A cross-sectional study. BMC Psychiatry 2021, 21, 485. [Google Scholar] [CrossRef]
- Zhang, Z.; Gu, D.; Hayward, M.D. Early life influences on cognitive impairment among oldest old Chinese. J. Gerontol. Ser. B 2008, 63, S25–S33. [Google Scholar] [CrossRef]
- Zhu, A.; Chen, H.; Shen, J.; Wang, X.; Li, Z.; Zhao, A.; Shi, X.; Yan, L.; Zeng, Y.; Yuan, C.; et al. Interaction between plant-based dietary pattern and air pollution on cognitive function: A prospective cohort analysis of Chinese older adults. Lancet Reg. Health West. Pac. 2022, 20, 100372. [Google Scholar] [CrossRef]
- Yi, Z.; Vaupel, J.W. Functional capacity and self–evaluation of health and life of oldest old in China. J. Soc. Issues 2002, 58, 733–748. [Google Scholar] [CrossRef]
- Xu, H.; Dupre, M.E.; Gu, D.; Wu, B. The impact of residential status on cognitive decline among older adults in China: Results from a longitudinal study. BMC Geriatr. 2017, 17, 107. [Google Scholar] [CrossRef]
- Herzog, A.R.; Wallace, R.B. Measures of cognitive functioning in the AHEAD Study. J. Gerontol. Ser. B 1997, 52B, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Cui, G.H.; Yao, Y.H.; Xu, R.F.; Tang, H.D.; Jiang, G.X.; Wang, Y.; Wang, G.; Chen, S.D.; Cheng, Q. Cognitive impairment using education-based cutoff points for CMMSE scores in elderly Chinese people of agricultural and rural Shanghai China. Acta Neurol. Scand. 2011, 124, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Qiu, C.; Zeng, Y.; Li, J. Leisure activities, education, and cognitive impairment in Chinese older adults: A population-based longitudinal study. Int. Psychogeriatr. 2017, 29, 727–739. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Dupre, M.E.; Qiu, L.; Zhou, W.; Zhao, Y.; Gu, D. Urban-rural differences in the association between access to healthcare and health outcomes among older adults in China. BMC Geriatr. 2017, 17, 151. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged: The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Gu, D.; Brown, B.L.; Qiu, L. Self-perceived uselessness is associated with lower likelihood of successful aging among older adults in China. BMC Geriatr. 2016, 16, 172. [Google Scholar] [CrossRef]
- Hou, Q.; Guan, Y.; Yu, W.; Liu, X.; Wu, L.; Xiao, M.; Lü, Y. Associations between obesity and cognitive impairment in the Chinese elderly: An observational study. Clin. Interv. Aging 2019, 14, 367–373. [Google Scholar] [CrossRef]
- Malloy, E.J.; Spiegelman, D.; Eisen, E.A. Comparing measures of model selection for penalized splines in Cox models. Comput. Stat. Data Anal. 2009, 53, 2605–2616. [Google Scholar] [CrossRef]
- Durrleman, S.; Simon, R. Flexible regression models with cubic splines. Stat. Med. 1989, 8, 551–561. [Google Scholar] [CrossRef]
- Glenn, J.M.; Madero, E.N.; Bott, N.T. Dietary protein and amino acid intake: Links to the maintenance of cognitive health. Nutrients 2019, 11, 1315. [Google Scholar] [CrossRef]
- Yeh, T.-S.; Yuan, C.; Ascherio, A.; Rosner, B.A.; Blacker, D.; Willett, W.C. Long-term dietary protein intake and subjective cognitive decline in US men and women. Am. J. Clin. Nutr. 2022, 115, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.A.; Chevalier, S.; Gougeon, R. Protein turnover and requirements in the healthy and frail elderly. J. Nutr. Health Aging 2006, 10, 272–283. [Google Scholar] [PubMed]
- Otsuka, R.; Kato, Y.; Nishita, Y.; Tange, C.; Tomida, M.; Nakamoto, M.; Imai, T.; Ando, F.; Shimokata, H. Age-related changes in energy intake and weight in community-dwelling middle-aged and elderly Japanese. J. Nutr. Health Aging 2016, 20, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE study group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Walrand, S.; Guillet, C.; Salles, J.; Cano, N.; Boirie, Y. Physiopathological mechanism of sarcopenia. Clin. Geriatr. Med. 2011, 27, 365–385. [Google Scholar] [CrossRef]
- Mazza, E.; Fava, A.; Ferro, Y.; Moraca, M.; Rotundo, S.; Colica, C.; Provenzano, F.; Terracciano, R.; Greco, M.; Foti, D.; et al. Impact of legumes and plant proteins consumption on cognitive performances in the elderly. J. Transl. Med. 2017, 15, 109. [Google Scholar] [CrossRef]
- Vallianou, N.G.; Bountziouka, V.P.; Georgousopoulou, E.; Evangelopoulos, A.A.; Bonou, M.S.; Vogiatzakis, E.D.; Barbetseas, J.D.; Avgerinos, P.C.; Panagiotakos, D.B. Influence of protein intake from haem and non-haem animals and plant origin on inflammatory biomarkers among apparently-healthy adults in Greece. J. Health Popul. Nutr. 2013, 31, 446–454. [Google Scholar] [CrossRef][Green Version]
- Roth, W.; Zadeh, K.; Vekariya, R.; Ge, Y.; Mohamadzadeh, M. Tryptophan metabolism and gut-brain homeostasis. Int. J. Mol. Sci. 2021, 22, 2973. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Feskanich, D.; Niu, C.; Dopfel, R.; Holmes, M.D.; Hankinson, S.E. Dietary correlates of urinary 6-sulfatoxymelatonin concentrations in the Nurses’ Health Study cohorts. Am. J. Clin. Nutr. 2009, 90, 975–985. [Google Scholar] [CrossRef]
- Dalile, B.; Kim, C.; Challinor, A.; Geurts, L.; Gibney, E.R.; Galdos, M.V.; La Fata, G.; Layé, S.; Mathers, J.C.; Vauzour, D.; et al. The EAT-Lancet reference diet and cognitive function across the life course. Lancet Planet. Health 2022, 6, e749–e759. [Google Scholar] [CrossRef]
- Hercberg, S.; Preziosi, P.; Briançon, S.; Galan, P.; Triol, I.; Malvy, D.; Roussel, A.-M.; Favier, A. A primary prevention trial using nutritional doses of antioxidant vitamins and minerals in cardiovascular diseases and cancers in a general population: The SU.VI.MAX study--design, methods, and participant characteristics. SUpplementation en VItamines et Minéraux AntioXydants. Control. Clin. Trials 1998, 19, 336–351. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.E.; Elias, M.F.; Dore, G.A.; Robbins, M.A. Relation between dairy food intake and cognitive function: The Maine-Syracuse Longitudinal Study. Int. Dairy J. 2012, 22, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Oktaviani, L.W.; Hsu, H.-C.; Chen, Y.-C. Effects of health-related behaviors and changes on successful aging among Indonesian older people. Int. J. Environ. Res. Public Health 2022, 19, 5952. [Google Scholar] [CrossRef] [PubMed]
- Ogata, S.; Tanaka, H.; Omura, K.; Honda, C.; Hayakawa, K. Association between intake of dairy products and short-term memory with and without adjustment for genetic and family environmental factors: A twin study. Clin. Nutr. 2016, 35, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Humayun, M.A.; Elango, R.; Ball, R.O.; Pencharz, P.B. Reevaluation of the protein requirement in young men with the indicator amino acid oxidation technique. Am. J. Clin. Nutr. 2007, 86, 995–1002. [Google Scholar] [CrossRef]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sport. Med. 2018, 52, 376–384. [Google Scholar] [CrossRef]
- Tarnopolsky, M. Protein requirements for endurance athletes. Nutrition 2004, 20, 662–668. [Google Scholar] [CrossRef]
- Wohlgemuth, K.J.; Arieta, L.R.; Brewer, G.J.; Hoselton, A.L.; Gould, L.M.; Smith-Ryan, A.E. Sex differences and considerations for female specific nutritional strategies: A narrative review. J. Int. Soc. Sport. Nutr. 2021, 18, 27. [Google Scholar] [CrossRef]
- Lin, Y.; Bolca, S.; Vandevijvere, S.; Van Oyen, H.; Van Camp, J.; De Backer, G.; Foo, L.H.; De Henauw, S.; Huybrechts, I. Dietary sources of animal and plant protein intake among Flemish preschool children and the association with socio-economic and lifestyle-related factors. Nutr. J. 2011, 10, 97. [Google Scholar] [CrossRef][Green Version]
- Khusun, H.; Februhartanty, J.; Anggraini, R.; Mognard, E.; Alem, Y.; Noor, M.I.; Karim, N.; Laporte, C.; Poulain, J.-P.; Monsivais, P.; et al. Animal and plant protein food sources in Indonesia differ across socio-demographic groups: Socio-cultural research in protein transition in Indonesia and Malaysia. Front. Nutr. 2022, 9, 762459. [Google Scholar] [CrossRef]
- Sobhani, S.R.; Eini-Zinab, H.; Rezazadeh, A. Socioeconomic Status and Changes in Iranian Household Food Basket Using National Household Budget and Expenditure Survey Data, 1991–2017. Iran. J. Public Health 2022, 51, 919–928. [Google Scholar] [CrossRef]
- van Praag, H. Exercise and the brain: Something to chew on. Trends Neurosci. 2009, 32, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Makino, K.; Lee, S.; Bae, S.; Shinkai, Y.; Chiba, I.; Shimada, H. Relationship between instrumental activities of daily living performance and incidence of mild cognitive impairment among older adults: A 48-month follow-up study. Arch. Gerontol. Geriatr. 2020, 88, 104034. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.-Y.; Yoon, H.-J.; Kim, H.; Choi, K.Y.; Lee, J.J.; Lee, K.H.; Seo, E.H. Reversion from mild cognitive impairment to normal cognition: False-positive error or true restoration thanks to cognitive control ability? Neuropsychiatr. Dis. Treat. 2019, 15, 3021–3032. [Google Scholar] [CrossRef] [PubMed]
- Jakes, R.W.; Day, N.E.; Luben, R.; Welch, A.; Bingham, S.; Mitchell, J.; Hennings, S.; Rennie, K.; Wareham, N.J. Adjusting for energy intake—What measure to use in nutritional epidemiological studies? Int. J. Epidemiol. 2004, 33, 1382–1386. [Google Scholar] [CrossRef]
- Rhee, J.J.; Cho, E.; Willett, W.C. Energy adjustment of nutrient intakes is preferable to adjustment using body weight and physical activity in epidemiological analyses. Public Health Nutr. 2014, 17, 1054–1060. [Google Scholar] [CrossRef]
- Halkjær, J.; Olsen, A.; Bjerregaard, L.J.; Deharveng, G.; Tjønneland, A.; Welch, A.A.; Crowe, F.L.; Wirfält, E.; Hellstrom, V.; Niravong, M.; et al. Intake of total, animal and plant proteins, and their food sources in 10 countries in the European Prospective Investigation into Cancer and Nutrition. Eur. J. Clin. Nutr. 2009, 63, S16–S36. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Cognitive Impairment | Normal | p Value | |
|---|---|---|---|---|
| Number of participants | 6951 | 1202 | 5749 | |
| Age in years | 79.7 ± 10.3 | 86.7 ± 9.4 | 78.2 ± 9.8 | <0.001 *** |
| Participants per age group | <0.001 *** | |||
| Younger elderly | 3521 (50.7) | 270 (22.5) | 3251 (56.5) | |
| Octogenarian | 2092 (30.1) | 444 (36.9) | 1648 (28.7) | |
| Nonagenarian and centenarian | 1338 (19.2) | 488 (40.6) | 850 (14.8) | |
| Male | 3456 (49.7) | 410 (34.1) | 3046 (53.0) | <0.001 *** |
| Years of schooling | 2.8 ± 5.0 | 1.5 (5.0) | 3.1 ± 5.0 | <0.001 *** |
| Urban residence | 2520 (36.3) | 391 (32.5) | 2129 (37.0) | 0.003 ** |
| Marital status | <0.001 *** | |||
| Married | 3554 (51.2) | 341 (28.4) | 3213 (56.0) | |
| Divorced/widowed/never | 3387 (48.8) | 2527 (44.0) | ||
| Economic status | 0.024 * | |||
| Favorable | 5889 (84.9) | 992 (82.7) | 4897 (85.3) | |
| Unfavorable | 1048 (15.1) | 207 (17.3) | 841 (14.7) | |
| Living pattern | <0.001 *** | |||
| Living with family members | 5665 (81.6) | 930 (77.4) | 4735 (82.5) | |
| Alone or at nursing home | 1276 (18.4) | 272 (22.6) | 1004 (17.5) | |
| ADL | 6.1 ± 0.6 | 6.2 (1.0) | 6.1 ± 0.5 | <0.001 *** |
| ADL disabled | 303 (4.4) | 100 (8.3) | 203 (3.5) | <0.001 *** |
| IADL | 10.1 ± 3.6 | 11.8 ± 4.5 | 13.1 ± 5.0 | <0.001 *** |
| IADL disabled | 2947 (42.4) | 786 (65.4) | 2161 (37.6) | <0.001 *** |
| Smoke at present | 1582 (22.8) | 178 (14.8) | 1404 (24.4) | <0.001 *** |
| Drink alcohol at present | 1451 (20.9) | 191 (15.9) | 1260 (21.9) | <0.001 *** |
| Exercise at present | 2343 (33.8) | 317 (26.4) | 2026 (35.4) | <0.001 *** |
| BMI (kg/m2) | 20.9 ± 3.5 | 20.1 ± 3.6 | 21.1 ± 3.4 | <0.001 *** |
| BMI group | <0.001 *** | |||
| Underweight | 1600 (23.0) | 377 (31.4) | 1223 (21.3) | |
| Normal | 3952 (56.9) | 670 (55.8) | 3282 (57.1) | |
| Overweight | 1393 (20.1) | 153 (12.8) | 1240 (21.6) | |
| Chronic disease | ||||
| Hypertension | 1633 (24.0) | 273 (23.3) | 1360 (24.1) | 0.573 |
| Diabetes | 208 (3.0) | 19 (1.6) | 189 (3.3) | 0.001 ** |
| Heart disease | 637 (9.3) | 85 (7.2) | 552 (9.8) | 0.007 ** |
| Stroke or CVD | 352 (5.1) | 51 (4.3) | 301 (5.3) | 0.191 |
| Cataract | 520 (7.6) | 111 (9.4) | 409 (7.2) | 0.011 * |
| Digestive system diseases | 336 (5.3) | 46 (4.2) | 290 (5.6) | 0.075 |
| Arthritis | 1440 (21.0) | 259 (21.9) | 1181 (20.8) | 0.410 |
| Parkinson’s disease | 22 (0.3) | 6 (0.5) | 16 (0.3) | 0.252 |
| Variables | HR (95% CI) | p Value |
|---|---|---|
| Age in years | 1.07 (1.06–1.09) | <0.001 *** |
| Sex | 0.030 * | |
| Female | [1] | |
| Male | 0.84 (0.71–0.98) | |
| Years of schooling | 0.93 (0.90–0.95) | <0.001 *** |
| Location of residence | 0.545 | |
| Rural | [1] | |
| Urban | 0.96 (0.84–1.10) | |
| Marital status | 0.001 ** | |
| Divorced/widowed/never | [1] | |
| Married | 0.75 (0.63–0.89) | |
| Economic status | 0.348 | |
| Unfavorable | [1] | |
| Favorable | 0.92 (0.78–1.09) | |
| Living pattern | 0.545 | |
| Alone or at nursing home | [1] | |
| Living with family members | 1.04 (0.89–1.23) | |
| ADL | 1.03 (0.96–1.11) | 0.402 |
| IADL | 1.03 (1.02–1.05) | <0.001 *** |
| BMI | 1.001 (0.998–1.004) | 0.638 |
| Smoke at present | 0.859 | |
| No | [1] | |
| Yes | 1.02 (0.84–1.10) | |
| Drink at present | 0.482 | |
| No | [1] | |
| Yes | 0.48 (0.78–1.12) | |
| Exercise at present | 0.053 | |
| No | [1] | |
| Yes | 0.87 (0.75–1.002) | |
| Hypertension | 0.270 | |
| No | [1] | |
| Yes | 0.92 (0.78–1.07) | |
| Diabetes | 0.701 | |
| No | [1] | |
| Yes | 0.91 (0.56–1.48) | |
| Heart disease | 0.701 | |
| No | [1] | |
| Yes | 0.95 (0.74–1.22) | |
| Stroke or CVD | 0.535 | |
| No | [1] | |
| Yes | 1.11 (0.80–1.28) | |
| Cataract | 0.899 | |
| No | [1] | |
| Yes | 1.02 (0.81–1.28) | |
| Digestive system diseases | 0.375 | |
| No | [1] | |
| Yes | 0.87 (0.63–1.19) | |
| Arthritis | 0.305 | |
| No | [1] | |
| Yes | 1.08 (0.93–1.26) | |
| Parkinson’s disease | 0.799 | |
| No | [1] | |
| Yes | 1.11 (0.49–2.51) | |
| Change in overall protein intake | 0.98 (0.97–0.99) | 0.001 ** |
| HR (95% CI) | p Value | |
|---|---|---|
| Animal-based protein | ||
| Model 1 | 0.98 (0.97–0.99) | 0.005 ** |
| Model 2 | 0.98 (0.96–0.99) | 0.002 ** |
| Model 3 | 0.98 (0.96–0.99) | 0.003 ** |
| Meats | ||
| Model 1 | 0.95 (0.91–0.995) | 0.030 * |
| Model 2 | 0.95 (0.91–0.99) | 0.018 * |
| Model 3 | 0.95 (0.91–0.995) | 0.030 * |
| Fish and aquatic products | ||
| Model 1 | 0.95 (0.91–0.98) | 0.005 ** |
| Model 2 | 0.94 (0.91–0.98) | 0.003 ** |
| Model 3 | 0.94 (0.90–0.98) | 0.005 ** |
| Eggs | ||
| Model 1 | 0.96 (0.92–1.001) | 0.054 |
| Model 2 | 0.97 (0.93–1.01) | 0.093 |
| Model 3 | 0.96 (0.92–1.001) | 0.052 |
| Milk and dairy products | ||
| Model 1 | 0.997 (0.96–1.03) | 0.843 |
| Model 2 | 0.99 (0.96–1.03) | 0.728 |
| Model 3 | 0.99 (0.95–1.03) | 0.592 |
| Plant-based protein | ||
| Model 1 | 0.96 (0.94–0.99) | 0.007 ** |
| Model 2 | 0.96 (0.94–0.99) | 0.008 ** |
| Model 3 | 0.96 (0.93–0.99) | 0.010 * |
| Bean products | ||
| Model 1 | 0.96 (0.93–0.995) | 0.023 * |
| Model 2 | 0.96 (0.93–0.99) | 0.020 * |
| Model 3 | 0.96 (0.92–0.996) | 0.031 * |
| Nuts | ||
| Model 1 | 0.97 (0.93–1.01) | 0.096 |
| Model 2 | 0.97 (0.93–1.01) | 0.106 |
| Model 3 | 0.98 (0.93–1.02) | 0.250 |
| Overall Protein | Animal-Based Protein | Plant-Based Protein | ||||||
|---|---|---|---|---|---|---|---|---|
| No of Converters/Person Years | Conversion Rate | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | ||||||||
| Younger elderly | 270/22,534 | 7.7 | 0.98 (0.96–1.01) | 0.135 | 0.98 (0.95–1.02) | 0.280 | 0.96 (0.91–1.01) | 0.128 |
| Octogenarian | 444/10,083 | 21.2 | 0.97 (0.95–0.99) | 0.001 ** | 0.96 (0.94–0.98) | 0.001 ** | 0.96 (0.92–1.004) | 0.073 |
| Nonagenarian and centenarian | 488/5004 | 36.5 | 0.99 (0.97–1.01) | 0.225 | 0.99 (0.96–1.01) | 0.291 | 0.98 (0.93–1.02) | 0.323 |
| Sex | ||||||||
| Male | 410/18,938 | 11.9 | 0.97 (0.95–0.99) | 0.005 ** | 0.96 (0.94–0.99) | 0.009 ** | 0.96 (0.91–1.003) | 0.064 |
| Female | 792/18,698 | 22.7 | 0.99 (0.97–1.001) | 0.052 | 0.98 (0.97–1.002) | 0.076 | 0.98 (0.95–1.01) | 0.172 |
| Location of residence | ||||||||
| Urban | 391/13,582 | 15.5 | 0.98 (0.96–1.003) | 0.095 | 0.98 (0.96–0.99) | 0.011 * | 0.98 (0.94–1.03) | 0.480 |
| Rural | 811/24,060 | 18.3 | 0.98 (0.97–0.99) | 0.003 ** | 0.98 (0.95–1.002) | 0.076 | 0.96 (0.93–0.99) | 0.021 * |
| Economic status | ||||||||
| Favorable | 992/31,977 | 16.8 | 0.98 (0.97–0.99) | 0.001 ** | 0.98 (0.96–0.99) | 0.005 ** | 1.02 (0.95–1.09) | 0.619 |
| Unfavorable | 207/5575 | 19.8 | 0.99 (0.96–1.02) | 0.543 | 0.98 (0.94–1.02) | 0.281 | 0.96 (0.93–0.99) | 0.010 * |
| Living pattern | ||||||||
| Living with family members | 930/31,157 | 16.4 | 0.98 (0.97–0.99) | 0.001 ** | 0.97 (0.96–0.99) | 0.003 ** | 0.97 (0.94–0.99) | 0.019 * |
| Alone or at nursing home | 272/6443 | 21.3 | 0.99 (0.96–1.02) | 0.489 | 0.99 (0.95–1.02) | 0.495 | 0.99 (0.93–1.05) | 0.699 |
| Exercise at present | ||||||||
| Yes | 317/13,284 | 13.5 | 0.999 (0.98–1.02) | 0.962 | 0.997 (0.97–1.03) | 0.825 | 1.01 (0.96–1.06) | 0.792 |
| No | 883/24,289 | 19.3 | 0.97 (0.96–0.99) | <0.001 *** | 0.97 (0.95–0.99) | 0.001 ** | 0.95 (0.92–0.99) | 0.004 ** |
| IADL disabled | ||||||||
| Yes | 786/13,379 | 26.7 | 0.98 (0.97–0.99) | 0.005 ** | 0.98 (0.96–0.995) | 0.014 * | 0.96 (0.93–0.996) | 0.031 * |
| No | 416/24,258 | 10.4 | 0.98 (0.96–1.001) | 0.061 | 0.98 (0.95–1.003) | 0.078 | 0.97 (0.93–1.02) | 0.230 |
| BMI | ||||||||
| Underweight | 377/8144 | 23.6 | 0.97 (0.95–0.99) | 0.005 ** | 0.96 (0.94–0.99) | 0.005 ** | 0.96 (0.91–1.01) | 0.147 |
| Normal | 670/21,617 | 17.0 | 0.99 (0.97–1.003) | 0.127 | 0.99 (0.97–1.01) | 0.243 | 0.98 (0.94–1.01) | 0.156 |
| Overweight | 153/7870 | 11.0 | 0.98 (0.94–1.01) | 0.149 | 0.96 (0.92–1.01) | 0.114 | 0.98 (0.91–1.05) | 0.524 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, X.; Yin, Y.; Niu, L.; Yang, X.; Du, X.; Tian, Q. Association between Changes in Protein Intake and Risk of Cognitive Impairment: A Prospective Cohort Study. Nutrients 2023, 15, 2. https://doi.org/10.3390/nu15010002
Xu X, Yin Y, Niu L, Yang X, Du X, Tian Q. Association between Changes in Protein Intake and Risk of Cognitive Impairment: A Prospective Cohort Study. Nutrients. 2023; 15(1):2. https://doi.org/10.3390/nu15010002
Chicago/Turabian StyleXu, Xinyi, Yueheng Yin, Li Niu, Xinxin Yang, Xinru Du, and Qingbao Tian. 2023. "Association between Changes in Protein Intake and Risk of Cognitive Impairment: A Prospective Cohort Study" Nutrients 15, no. 1: 2. https://doi.org/10.3390/nu15010002
APA StyleXu, X., Yin, Y., Niu, L., Yang, X., Du, X., & Tian, Q. (2023). Association between Changes in Protein Intake and Risk of Cognitive Impairment: A Prospective Cohort Study. Nutrients, 15(1), 2. https://doi.org/10.3390/nu15010002