
Comparison of the 24 h Dietary Recall of Two Consecutive Days, Two Non-Consecutive Days, Three Consecutive Days, and Three Non-Consecutive Days for Estimating Dietary Intake of Chinese Adult

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection and Measurements
2.3. Dietary Intake Assessment
2.4. Data Sets
2.5. Statistical Analysis
3. Results
3.1. Subjects’ Characteristics
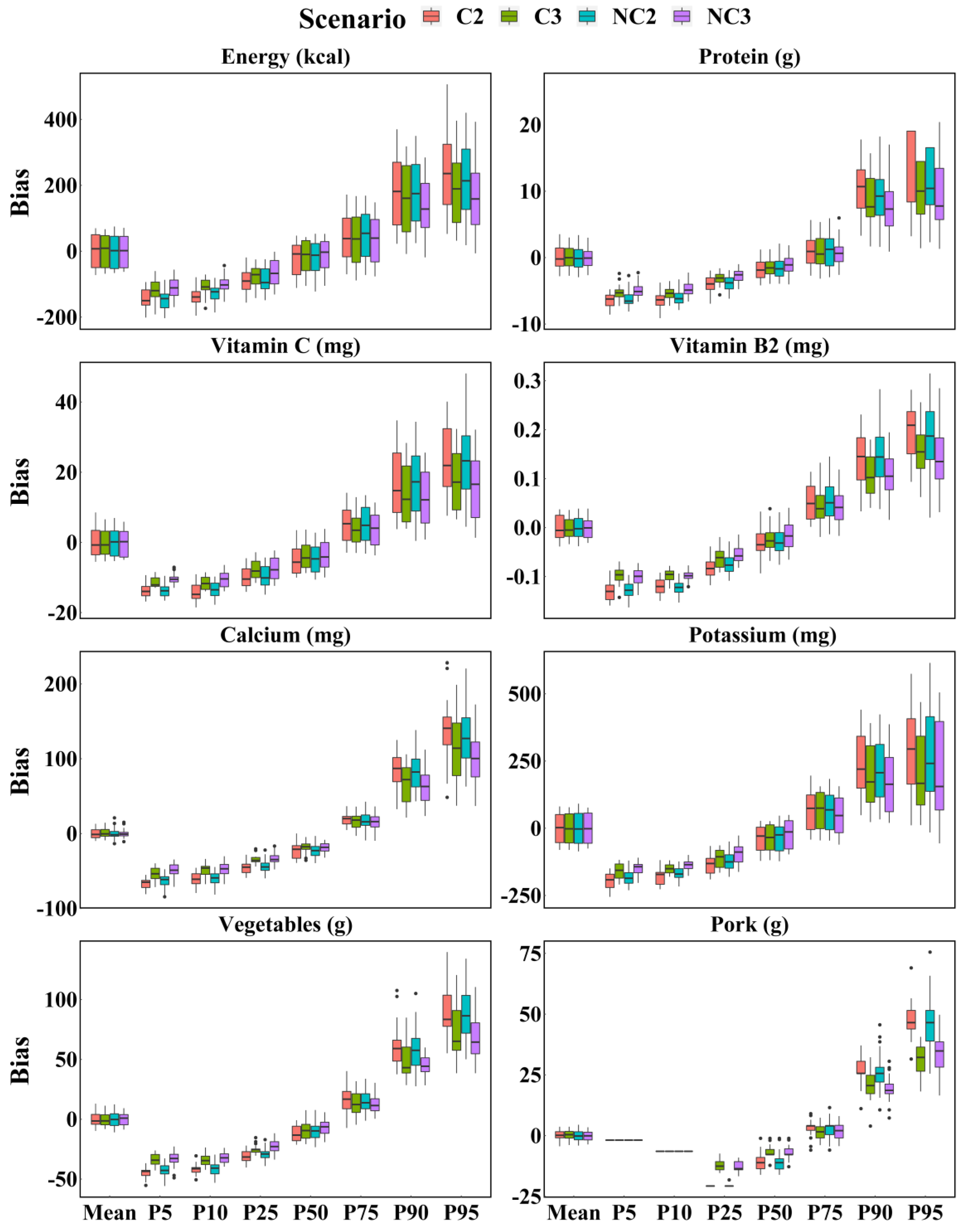
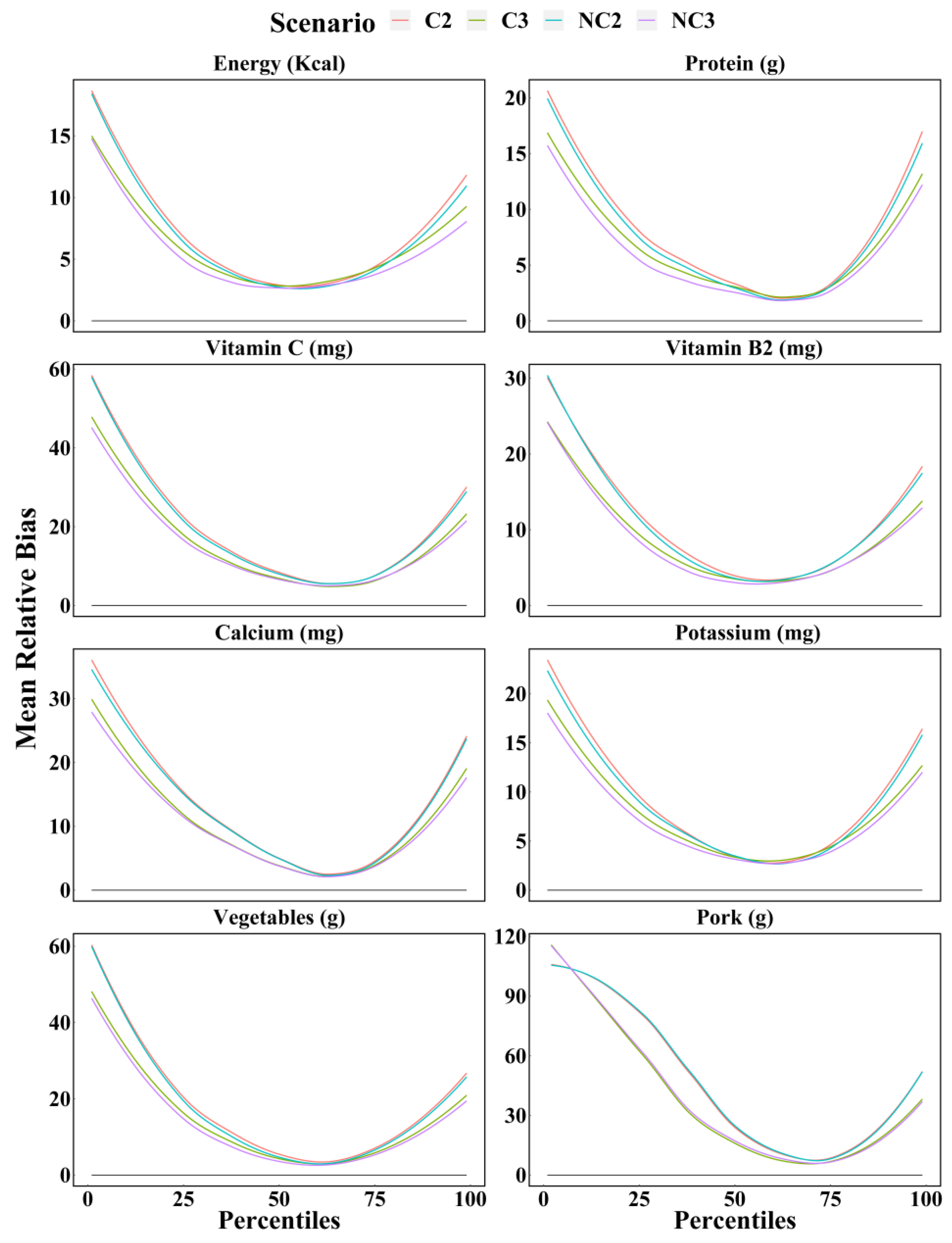
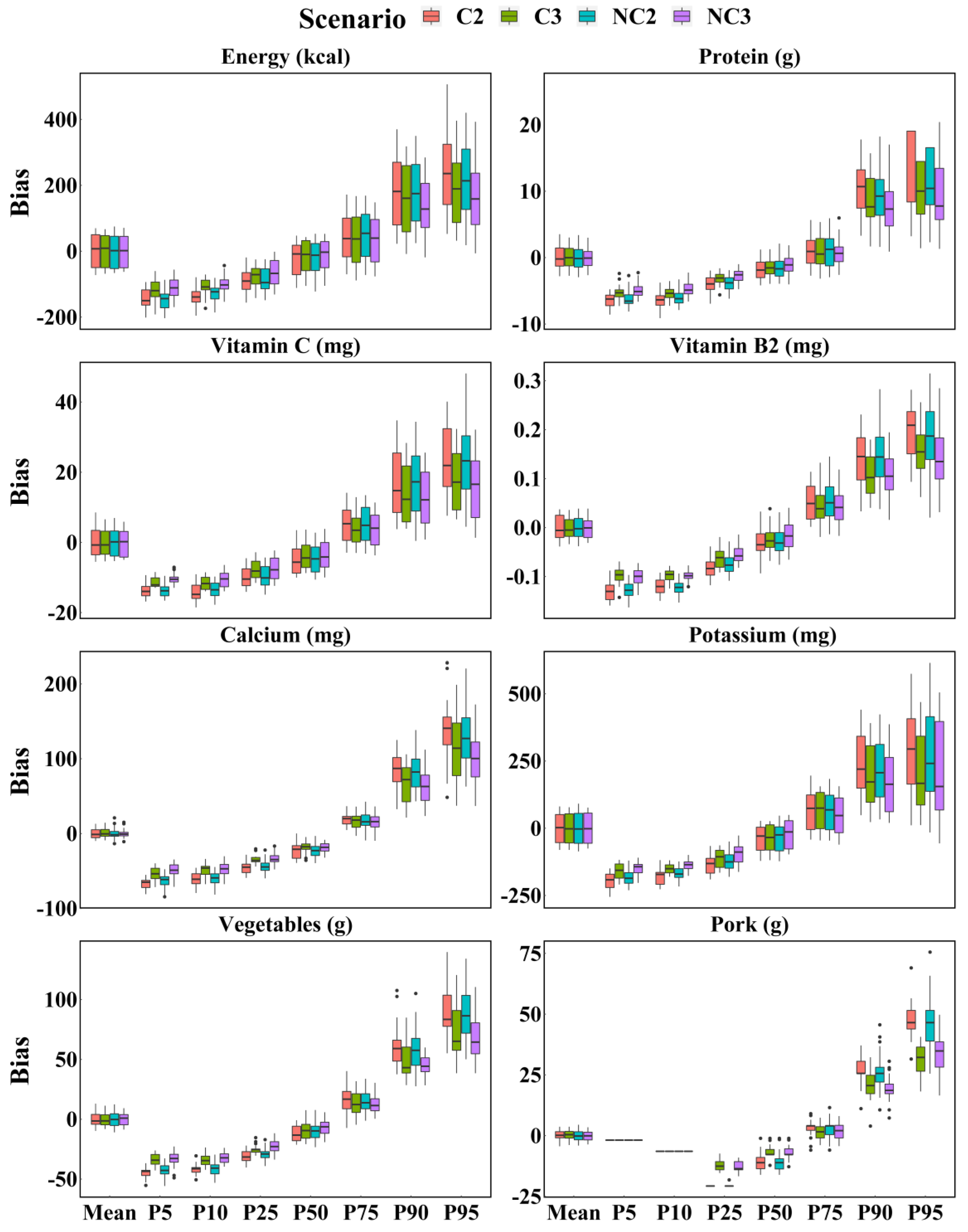
3.2. Comparison of Four Scenarios Based on WPM Method
3.3. Equivalence Testing between Scenario C3 and NC2
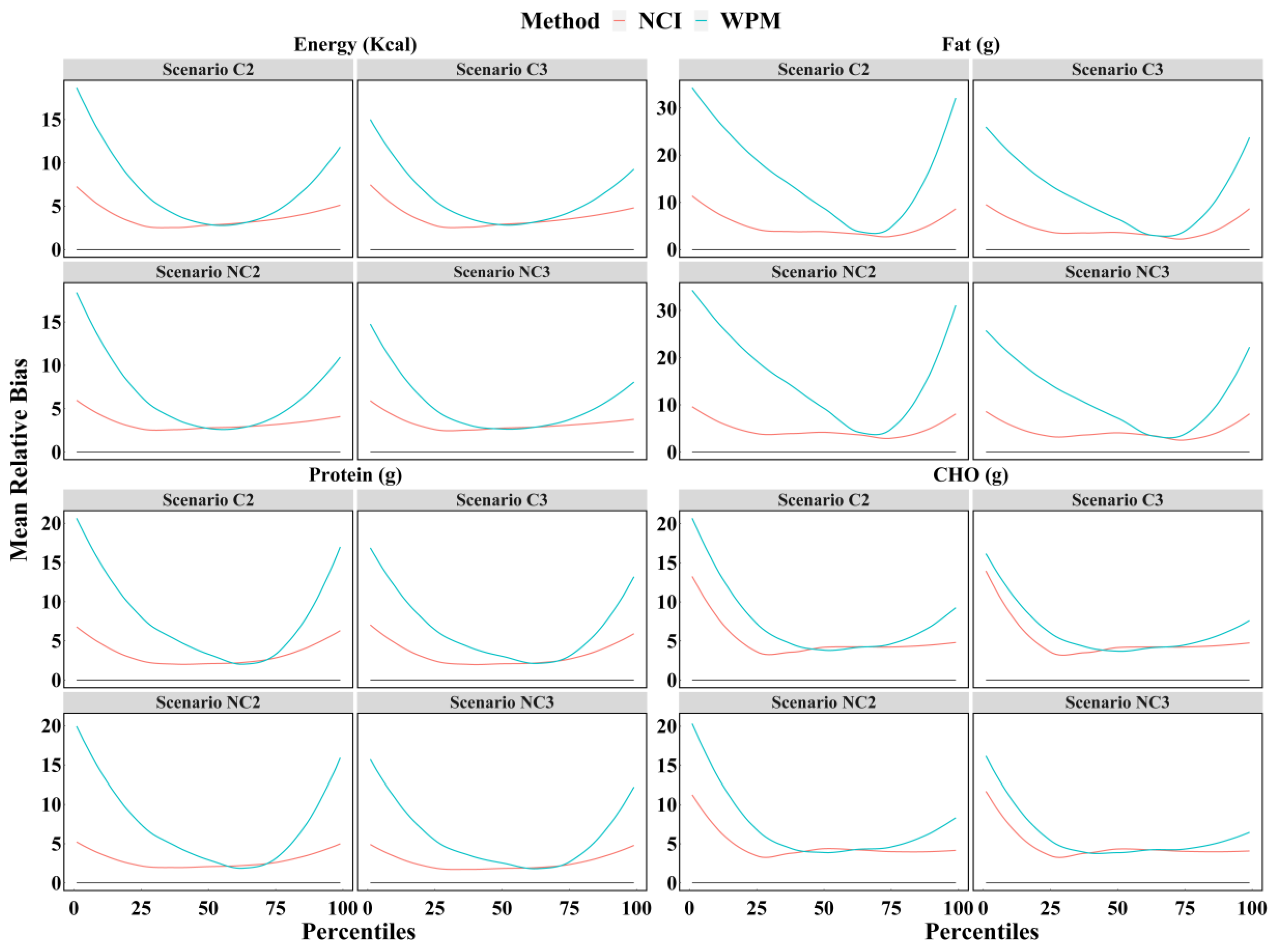
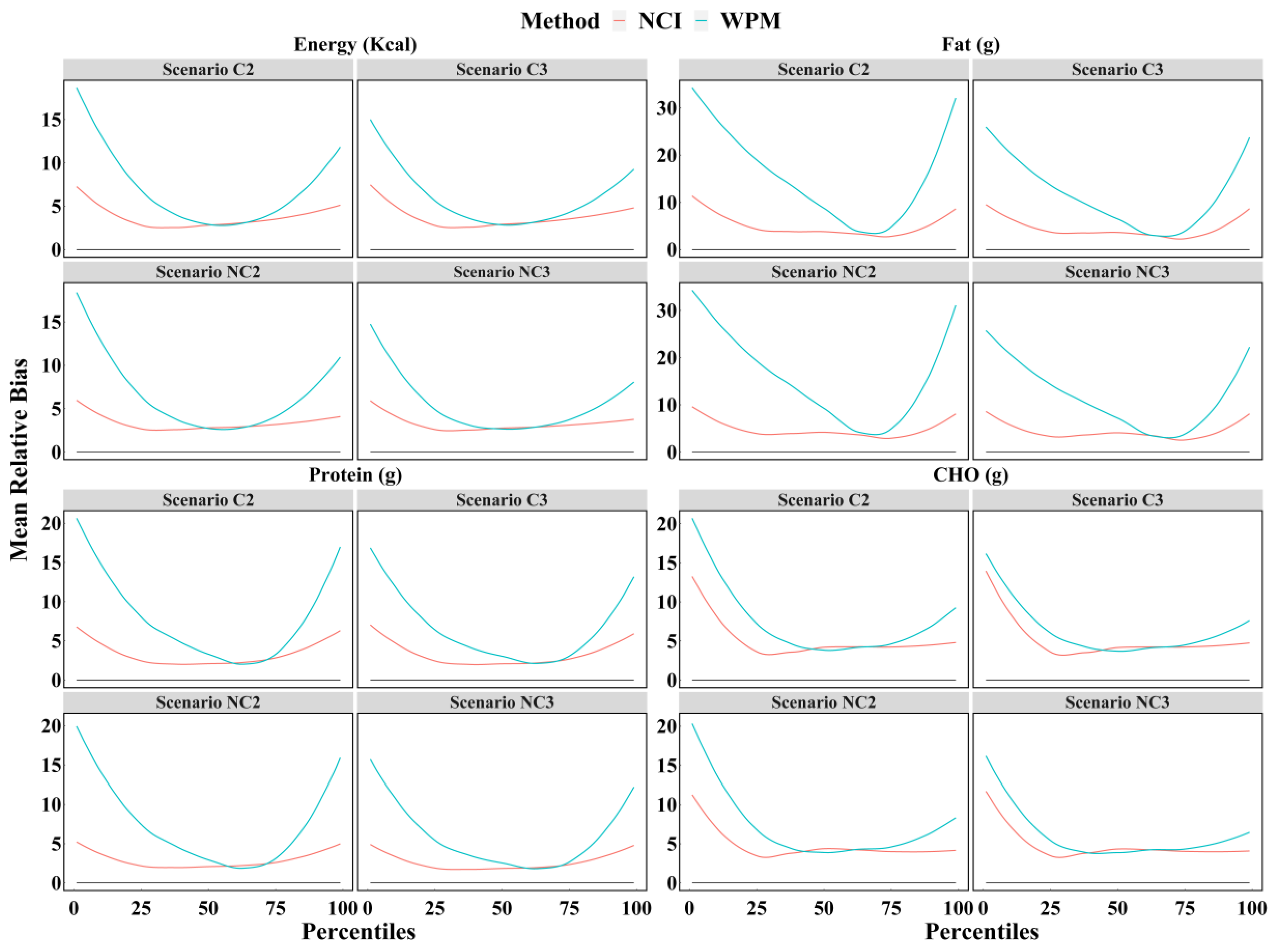
3.4. Comparison of Four Scenarios between WPM and NCI Method
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Majem, L.; Roman, B.; Estruch, R. Scientific evidence of interventions using the Mediterranean diet: A systematic review. Nutr. Rev. 2006, 64, S27–S47. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M.; Perez-Rodrigo, C.; Lopez-Sobaler, A.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 31 (Suppl. 3), 38–45. [Google Scholar] [CrossRef]
- Perez Rodrigo, C.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Food frequency questionnaires. Nutr. Hosp. 2015, 31 (Suppl. 3), 49–56. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- National Center for Health Statistics. National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 5 July 2021).
- Canada, H. Reference Guide to Understanding and Using the Data—2015 Canadian Community Health Survey—Nutrition. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-nutrition-surveillance/health-nutrition-surveys/canadian-community-health-survey-cchs/ (accessed on 9 February 2022).
- Yu, D.; Zhao, L.; Zhao, W. Status and trends in consumption of grains and dietary fiber among Chinese adults (1982–2015). Nutr. Rev. 2020, 78, 43–53. [Google Scholar] [CrossRef]
- Castell, G.S.; Serra-Majem, L.; Ribas-Barba, L. What and how much do we eat? 24-hour dietary recall method. Nutr. Hosp. 2015, 31 (Suppl. 3), 46–48. [Google Scholar] [CrossRef]
- Walter, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Basiotis, P.P.; Welsh, S.O.; Cronin, F.J.; Kelsay, J.L.; Mertz, W. Number of days of food intake records required to estimate individual and group nutrient intakes with defined confidence. J. Nutr. 1987, 117, 1638–1641. [Google Scholar] [CrossRef]
- Luo, H.; Dodd, K.W.; Arnold, C.D.; Engle-Stone, R. A New Statistical Method for Estimating Usual Intakes of Nearly-Daily Consumed Foods and Nutrients through Use of Only One 24-hour Dietary Recall. J. Nutr. 2019, 149, 1667–1673. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Australian Health Survey: Nutrition FirstResultsFoodsand Nutrients, 2011–2012. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/0D6B1FE95EAB8FF3CA257CD2001CA113?opendocument (accessed on 15 January 2021).
- Castellanos-Gutierrez, A.; Rodriguez-Ramirez, S.; Bromage, S.; Fung, T.T.; Li, Y.; Bhupathiraju, S.N.; Deitchler, M.; Willett, W.; Batis, C. Performance of the Global Diet Quality Score with Nutrition and Health Outcomes in Mexico with 24-h Recall and FFQ Data. J. Nutr. 2021, 151, 143S–151S. [Google Scholar] [CrossRef]
- Jung, S.; Park, S.; Kim, J.Y. Comparison of dietary share of ultra-processed foods assessed with a FFQ against a 24-h dietary recall in adults: Results from KNHANES 2016. Public Health Nutr. 2022, 25, 1166–1175. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.L.; He, L.; Zhao, L.Y.; Guo, Q.Y.; Yu, D.M.; Ju, L.H.; Fang, H.Y. The Status of Dietary Energy and Nutrients Intakes among Chinese Elderly Aged 80 and Above: Data from the CACDNS 2015. Nutrients 2021, 13, 1622. [Google Scholar] [CrossRef] [PubMed]
- Larkin, F.A.; Metzner, H.L.; Guire, K.E. Comparison of three consecutive-day and three random-day records of dietary intake. J. Am. Diet. Assoc. 1991, 91, 1538–1542. [Google Scholar] [CrossRef]
- El Lozy, M. Dietary variability and its impact on nutritional epidemiology. J. Chronic Dis. 1983, 36, 237–249. [Google Scholar] [CrossRef]
- Morgan, K.J.; Johnson, S.R.; Goungetas, B. Variability of food intakes. An analysis of a 12-day data series using persistence measures. Am. J. Epidemiol. 1987, 126, 326–335. [Google Scholar] [CrossRef]
- St George, S.M.; Van Horn, M.L.; Lawman, H.G.; Wilson, D.K. Reliability of 24-Hour Dietary Recalls as a Measure of Diet in African-American Youth. J. Acad. Nutr. Diet. 2016, 116, 1551–1559. [Google Scholar] [CrossRef]
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.X. Chinese Food Composition Table; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Freese, J.; Pricop-Jeckstadt, M.; Heuer, T.; Clemens, M.; Boeing, H.; Knuppel, S.; Nothlings, U. Determinants of consumption-day amounts applicable for the estimation of usual dietary intake with a short 24-h food list. J. Nutr. Sci. 2016, 5, e35. [Google Scholar] [CrossRef] [Green Version]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef] [Green Version]
- Walker, E.; Nowacki, A.S. Understanding equivalence and noninferiority testing. J. Gen. Intern. Med. 2011, 26, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Wable Grandner, G.; Dickin, K.; Kanbur, R.; Menon, P.; Rasmussen, K.M.; Hoddinott, J. Assessing statistical similarity in dietary intakes of women of reproductive age in Bangladesh. Matern. Child Nutr. 2021, 17, e13086. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhao, L.; Zhang, J.; Yang, Z.; Yang, L.; Huang, J.; Fang, H.; Guo, Q.; Xu, X.; Ju, L.; et al. China Nutrition and Health Surveys (1982–2017). China CDC Wkly 2021, 3, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Capita, R.; Alonso-Calleja, C. Differences in reported winter and summer dietary intakes in young adults in Spain. Int. J. Food Sci. Nutr. 2005, 56, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, N.; Okuda, T.; Shinohara, H.; Yamasaki, R.S.; Hirano, N.; Kang, J.; Ogawa, M.; Nishi, N.N. Relationship between Seasonal Changes in Food Intake and Energy Metabolism, Physical Activity, and Body Composition in Young Japanese Women. Nutrients 2022, 14, 506. [Google Scholar] [CrossRef]
- Westerterp, K.R.; Plasqui, G.; Goris, A.H. Water loss as a function of energy intake, physical activity and season. Br. J. Nutr. 2005, 93, 199–203. [Google Scholar] [CrossRef] [Green Version]
- Tokudome, Y.; Imaeda, N.; Nagaya, T.; Ikeda, M.; Fujiwara, N.; Sato, J.; Kuriki, K.; Kikuchi, S.; Maki, S.; Tokudome, S. Daily, weekly, seasonal, within- and between-individual variation in nutrient intake according to four season consecutive 7 day weighed diet records in Japanese female dietitians. J. Epidemiol. 2002, 12, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Stote, K.S.; Radecki, S.V.; Moshfegh, A.J.; Ingwersen, L.A.; Baer, D.J. The number of 24 h dietary recalls using the US Department of Agriculture’s automated multiple-pass method required to estimate nutrient intake in overweight and obese adults. Public Health Nutr. 2011, 14, 1736–1742. [Google Scholar] [CrossRef] [Green Version]
- Carriquiry, A.L. Estimation of usual intake distributions of nutrients and foods. J. Nutr. 2003, 133, 601S–608S. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Olendzki, B.C.; Pagoto, S.L.; Hurley, T.G.; Magner, R.P.; Ockene, I.S.; Schneider, K.L.; Merriam, P.A.; Hebert, J.R. Number of 24-hour diet recalls needed to estimate energy intake. Ann. Epidemiol. 2009, 19, 553–559. [Google Scholar] [CrossRef] [Green Version]
- Huang, K.; Yu, D.; Guo, Q.; Yang, Y.; Wei, X.; Zhao, L.; Fang, H. Validation of the MSM and NCI Method for Estimating the Usual Intake of Nutrients and Food According to Four Seasons of Seven Consecutive Daily 24 Hour Dietary Recalls in Chinese Adults. Nutrients 2022, 14, 445. [Google Scholar] [CrossRef]
- Laureano, G.H.; Torman, V.B.; Crispim, S.P.; Dekkers, A.L.; Camey, S.A. Comparison of the ISU, NCI, MSM, and SPADE Methods for Estimating Usual Intake: A Simulation Study of Nutrients Consumed Daily. Nutrients 2016, 8, 166. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Northern | Southern |
|---|---|---|---|
| N | 595 (100%) | 324 (54.5%) | 271 (45.5%) |
| Age group (year) | |||
| 18–39 | 291 (48.9%) | 170 (52.5%) | 121 (44.6%) |
| 40–60 | 304 (51.1%) | 154 (47.5%) | 150 (55.4%) |
| Gender | |||
| Male | 285 (47.9%) | 154 (47.5%) | 131 (48.3%) |
| Female | 310 (52.1%) | 170 (52.5%) | 140 (51.7%) |
| Urban or Rural | |||
| Urban | 304 (51.1%) | 164 (50.6%) | 140 (51.7%) |
| Rural | 291 (48.9%) | 160 (49.4%) | 131 (48.3%) |
| Education level | |||
| Primary school or below | 34 (5.7%) | 11 (3.4%) | 23 (8.5%) |
| Middle school | 186 (31.3%) | 130 (40.1%) | 56 (20.7%) |
| High school and above | 375 (63%) | 183 (56.5%) | 192 (70.8%) |
| Household income level * | |||
| Low | 9 (1.5%) | 8 (2.5%) | 1 (0.4%) |
| Medium | 124 (20.8%) | 110 (34.0%) | 14 (5.2%) |
| High | 204 (34.3%) | 56 (17.2%) | 148 (54.5%) |
| Unclear | 258 (43.4%) | 150 (46.3%) | 108 (39.9%) |
| BMI (Kg/m2) | |||
| 18.5< | 13 (2.2%) | 4 (1.2%) | 9 (3.3%) |
| 18.5–23.9 | 300 (50.4%) | 143 (44.1%) | 157 (57.9%) |
| ≥24 | 282 (47.4%) | 177 (54.7%) | 105 (38.8%) |
| The number of 24 h recalls | |||
| 23 | 4 (0.7%) | 1 (0.3%) | 3 (1.1%) |
| 24 | 4 (0.7%) | 4 (1.2%) | 0 (0%) |
| 25 | 5 (0.8%) | 1 (0.3%) | 4 (1.5%) |
| 26 | 12 (2.0%) | 5 (1.5%) | 7 (2.6%) |
| 27 | 56 (9.4%) | 29 (9.0%) | 27 (10.0%) |
| 28 | 514 (86.4%) | 284 (87.7%) | 230 (84.8%) |
| Dietary Components | Parameter | True Value | Mean Bias (Mean Relative Bias %) | MSE | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| C2 | NC2 | C3 | NC3 | C2 | NC2 | C3 | NC3 | |||
| Protein (g) | Mean | 66.47 | −0.01 (−0.01) | 0.02 (0.03) | −0.04 (−0.06) | 0.03 (0.05) | 3.34 | 2.97 | 3.16 | 2.77 |
| P05 | 38.46 | −6.48 (16.84) | −6.31 (16.40) | −5.29 (13.75) | −4.93 (12.82) | 43.03 | 40.86 | 29.42 | 25.33 | |
| P10 | 43.48 | −6.42 (14.76) | −6.04 (13.88) | −5.36 (12.33) | −4.64 (10.67) | 42.73 | 37.34 | 29.73 | 22.72 | |
| P25 | 51.70 | −3.98 (7.69) | −3.84 (7.42) | −3.11 (6.01) | −2.72 (5.27) | 17.24 | 15.82 | 10.54 | 8.30 | |
| P50 | 63.66 | −1.78 (3.18) | −1.48 (2.78) | −1.53 (2.75) | −0.93 (2.34) | 5.56 | 4.33 | 4.28 | 3.01 | |
| P75 | 79.31 | 1.24 (2.68) | 1.06 (2.68) | 0.98 (2.56) | 0.69 (2.14) | 7.15 | 6.49 | 6.44 | 4.58 | |
| P90 | 91.21 | 10.33 (11.32) | 9.48 (10.39) | 8.46 (9.28) | 7.71 (8.45) | 124.67 | 107.60 | 87.89 | 75.06 | |
| P95 | 103.04 | 13.92 (13.51) | 11.79 (11.44) | 10.69 (10.38) | 9.26 (8.99) | 237.60 | 175.03 | 147.45 | 113.17 | |
| Zinc (mg) | Mean | 9.90 | −0.01 (−0.07) | 0 (0.04) | −0.01 (−0.14) | 0.01 (0.07) | 0.12 | 0.11 | 0.11 | 0.10 |
| P05 | 5.63 | −1.08 (19.13) | −1.03 (18.30) | −0.91 (16.19) | −0.85 (15.08) | 1.18 | 1.09 | 0.87 | 0.76 | |
| P10 | 6.17 | −0.87 (14.11) | −0.8 (12.89) | −0.72 (11.63) | −0.58 (9.33) | 0.79 | 0.67 | 0.54 | 0.39 | |
| P25 | 7.53 | −0.63 (8.42) | −0.58 (7.71) | −0.50 (6.66) | −0.42 (5.63) | 0.44 | 0.40 | 0.29 | 0.24 | |
| P50 | 9.31 | −0.19 (3.36) | −0.19 (2.87) | −0.12 (3.15) | −0.09 (2.62) | 0.13 | 0.11 | 0.13 | 0.09 | |
| P75 | 11.82 | 0.04 (2.98) | 0.08 (3.06) | 0.02 (2.93) | 0.03 (2.82) | 0.17 | 0.19 | 0.17 | 0.17 | |
| P90 | 14.06 | 1.16 (8.28) | 1.07 (7.61) | 0.98 (6.99) | 0.87 (6.21) | 1.86 | 1.54 | 1.36 | 1.08 | |
| P95 | 16.06 | 1.75 (10.89) | 1.52 (9.48) | 1.28 (8.1) | 1.13 (7.09) | 3.90 | 3.03 | 2.40 | 1.87 | |
| Vitamin C (mg) | Mean | 65.68 | −0.06 (−0.09) | 0.01 (0.01) | −0.21 (−0.31) | −0.03 (−0.04) | 15.88 | 16.13 | 14.30 | 15.65 |
| P05 | 28.59 | −13.71 (47.96) | −13.71 (47.97) | −11.32 (39.59) | −10.4 (36.37) | 191.38 | 191.45 | 130.65 | 110.08 | |
| P10 | 35.41 | −14.13 (39.91) | −13.44 (37.94) | −11.51 (32.49) | −10.53 (29.75) | 205.34 | 184.91 | 135.68 | 115.61 | |
| P25 | 45.32 | −9.88 (21.81) | −9.52 (21.00) | −7.72 (17.03) | −7.39 (16.31) | 105.04 | 99.41 | 66.08 | 65.57 | |
| P50 | 61.68 | −4.69 (8.59) | −4.75 (8.07) | −3.92 (7.31) | −3.60 (6.81) | 38.72 | 36.95 | 29.25 | 27.16 | |
| P75 | 80.23 | 4.98 (6.95) | 5.01 (6.84) | 3.85 (5.77) | 3.79 (5.98) | 50.78 | 50.25 | 36.61 | 35.68 | |
| P90 | 101.46 | 16.76 (16.52) | 16.64 (16.40) | 13.85 (13.65) | 12.98 (12.80) | 367.07 | 351.90 | 263.58 | 232.32 | |
| P95 | 120.30 | 24.08 (20.02) | 22.81 (18.96) | 17.59 (14.62) | 15.80 (13.14) | 680.31 | 619.95 | 377.94 | 334.97 | |
| Vegetables (g) | Mean | 221.59 | −0.17 (−0.08) | 0 (0) | −0.07 (−0.03) | 0.13 (0.06) | 45.31 | 38.12 | 36.83 | 28.34 |
| P05 | 92.77 | −44.38 (47.84) | −42.73 (46.07) | −33.69 (36.32) | −32.67 (35.22) | 1990.09 | 1853.40 | 1160.65 | 1096.74 | |
| P10 | 115.60 | −42.02 (36.35) | −41.91 (36.25) | −33.77 (29.21) | −32.45 (28.07) | 1785.84 | 1783.45 | 1165.28 | 1072.67 | |
| P25 | 152.07 | −31.18 (20.50) | −29.18 (19.19) | −25.29 (16.63) | −22.54 (14.82) | 998.71 | 872.37 | 653.75 | 531.96 | |
| P50 | 205.82 | −11.89 (5.78) | −9.93 (5.08) | −8.79 (4.96) | −6.71 (3.66) | 184.77 | 143.52 | 136.72 | 83.84 | |
| P75 | 276.24 | 16.40 (6.23) | 15.40 (5.60) | 12.80 (4.95) | 12.34 (4.47) | 419.00 | 308.78 | 283.12 | 208.32 | |
| P90 | 342.43 | 61.85 (18.06) | 58.61 (17.12) | 49.45 (14.44) | 44.5 (13.00) | 4146.79 | 3697.01 | 2717.41 | 2059.91 | |
| P95 | 394.86 | 88.21 (22.34) | 87.18 (22.08) | 72.94 (18.47) | 67.12 (17.00) | 8194.88 | 8082.75 | 5882.91 | 4812.53 | |
| Dietary Components | 90% Confidence Interval (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | P5 | P10 | P25 | P50 | P75 | P90 | P95 | |
| Energy | (−0.73, 0.77) * | (−4.19, −2.50) ** | (−2.60, −1.40) ** | (−1.44, −0.10) ** | (−0.94, 0.64) * | (−0.14, 1.76) ** | (−0.21, 1.88) ** | (0.40, 2.40) ** |
| Fat | (−1.00, −0.01) * | (−12.70, −9.96) *** | (−9.59, −7.59) *** | (−7.61, −6.01) *** | (−3.31, −2.05) ** | (−0.53, 0.86) * | (2.58, 4.39) ** | (1.95, 3.98) ** |
| Protein | (−0.55, 0.73) * | (−3.87, −2.29) ** | (−2.39, −1.15) ** | (−2.01, −0.98) ** | (−0.50, 0.64) * | (−0.60, 0.82) * | (0.00, 2.05) ** | (−0.32, 2.25) ** |
| CHO | (−0.77, 1.13) ** | (−4.00, −2.53) ** | (−3.26, −2.10) ** | (−1.43, 0.26) ** | (−0.58, 1.53) ** | (−0.34, 1.98) ** | (−0.23, 2.01) ** | (−0.70, 2.02) ** |
| Fiber | (−0.64, 0.66) * | (−8.25, −6.99) *** | (−5.13, −4.13) ** | (−4.32, −3.26) ** | (−1.99, −0.49) ** | (−0.05, 1.58) ** | (0.97, 2.71) ** | (2.64, 4.56) ** |
| Cholesterol | (−1.43, 0.49) ** | (−68.21, −54.79) | (−44.4, −36.58) | (−10.10, −6.30) *** | (−2.24, −0.07) ** | (−0.01, 1.71) ** | (1.81, 3.70) ** | (3.62, 5.91) ** |
| Calcium | (−0.50, 0.22) * | (−7.14, −4.58) ** | (−6.28, −4.16) ** | (−4.08, −2.78) ** | (−1.78, −0.74) ** | (−0.47, 0.53) * | (1.44, 3.21) ** | (0.78, 3.22) ** |
| Iron | (−1.34, 1.6) ** | (−4.14, −2.73) ** | (−2.84, −1.30) ** | (−2.80, −1.10) ** | (−2.58, −0.26) ** | (−1.70, 1.61) ** | (−1.02, 3.28) ** | (1.36, 6.83) ** |
| Zinc | (−0.65, 1.00) * | (−3.48, −1.56) ** | (−2.28, −0.58) ** | (−1.95, −0.29) ** | (−1.49, 0.08) ** | (−0.31, 1.44) ** | (−0.44, 1.61) ** | (0.18, 2.59) ** |
| Magnesium | (−0.66, 0.88) * | (−4.64, −2.89) ** | (−3.03, −1.70) ** | (−2.13, −0.87) ** | (−1.35, 0.16) ** | (−0.63, 1.24) ** | (0.59, 2.74) ** | (0.71, 3.18) ** |
| Sodium | (−0.87, 0.38) * | (−12.03, −7.48) *** | (−10.02, −7.13) *** | (−7.78, −6.23) *** | (−5.86, −4.55) ** | (−0.89, 0.67) * | (2.41, 4.68) ** | (3.43, 6.36) ** |
| Potassium | (−0.82, 0.84) * | (−3.88, −2.35) ** | (−2.30, −1.16) ** | (−1.58, −0.23) ** | (−0.71, 0.88) * | (−1.07, 0.60) ** | (−0.30, 1.94) ** | (0.45, 3.38) ** |
| Phosphorus | (−0.56, 0.80) * | (−3.61, −2.27) ** | (−2.45, −1.23) ** | (−1.20, 0.10) ** | (−0.44, 0.79) * | (−0.13, 1.33) ** | (−0.36, 1.78) ** | (−0.26, 1.82) ** |
| Vitamin A | (−2.43, 1.95) ** | (−17.22, −13.56) | (−13.69, −10.36) | (−8.56, −5.42) *** | (−5.65, −1.90) ** | (−4.07, 1.03) ** | (−0.72, 5.87) *** | (1.05, 7.36) ** |
| Vitamin C | (−1.16, 1.81) ** | (−16.40, −11.35) | (−10.16, −5.99) *** | (−6.67, −2.91) ** | (−3.05, 0.17) ** | (−0.07, 2.81) ** | (0.58, 4.25) ** | (2.08, 5.49) ** |
| Vitamin E | (−1.55, 0.89) ** | (−7.62, −5.56) *** | (−6.51, −4.58) ** | (−6.09, −3.73) ** | (−4.32, −1.65) ** | (−2.07, 0.69) ** | (1.18, 4.43) ** | (4.69, 8.18) ** |
| Vitamin B1 | (−0.48, 0.81) * | (−8.87, −6.87) *** | (−6.05, −4.60) ** | (−3.06, −1.46) ** | (−1.08, 0.63) ** | (0.03, 1.69) ** | (1.65, 3.46) ** | (0.99, 2.83) ** |
| Vitamin B2 | (−0.65, 0.51) * | (−3.70, −1.91) ** | (−4.87, −3.39) ** | (−2.35, −0.87) ** | (−1.25, 0.13) ** | (−0.17, 1.01) ** | (−0.1, 1.53) ** | (0.51, 2.31) ** |
| Vitamin B3 | (−0.60, 0.67) * | (−3.80, −2.13) ** | (−3.35, −1.92) ** | (−2.58, −1.36) ** | (−0.88, 0.20) * | (−0.60, 0.93) * | (−0.4, 1.57) ** | (0.63, 3.51) ** |
| Vitamin B9 | (−1.24, 0.53) ** | (−11.09, −8.39) *** | (−8.25, −6.41) *** | (−4.97, −3.01) ** | (−2.57, −0.45) ** | (−0.20, 1.78) ** | (0.44, 2.47) ** | (1.99, 4.48) ** |
| Wheat | (−0.54, 1.50) ** | (−99.85, −91.18) | (−25.27, −20.14) | (−6.03, −3.12) ** | (0.08, 2.27) ** | (0.74, 3.55) ** | (1.27, 3.80) ** | (0.61, 3.24) ** |
| Pork | (−1.99, 0.07) ** | - | - | (−102.83, −96.17) | (−15.3, −10.15) | (0.43, 2.53) ** | (2.59, 5.19) ** | (7.54, 10.49) *** |
| Vegetables | (−0.65, 0.72) * | (−17.45, −13.16) | (−11.50, −8.40) *** | (−3.92, −2.21) ** | (−1.45, 0.29) ** | (0.12, 1.67) ** | (1.32, 3.36) ** | (1.87, 4.22) ** |
| Milk | (−2.92, 2.39) ** | - | - | - | (−107.33, −92.67) | (−6.01, −0.11) *** | (0.75, 5.19) *** | (−1.46, −0.49) ** |
| Beans | (−2.33, 1.94) ** | - | (−114.93, −85.07) | (−30.10, −23.40) | (−9.45, −5.95) *** | (−4.97, −0.54) ** | (0.96, 6.46) *** | (8.39, 13.93) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, K.; Zhao, L.; Guo, Q.; Yu, D.; Yang, Y.; Cao, Q.; Yuan, X.; Ju, L.; Li, S.; Cheng, X.; et al. Comparison of the 24 h Dietary Recall of Two Consecutive Days, Two Non-Consecutive Days, Three Consecutive Days, and Three Non-Consecutive Days for Estimating Dietary Intake of Chinese Adult. Nutrients 2022, 14, 1960. https://doi.org/10.3390/nu14091960
Huang K, Zhao L, Guo Q, Yu D, Yang Y, Cao Q, Yuan X, Ju L, Li S, Cheng X, et al. Comparison of the 24 h Dietary Recall of Two Consecutive Days, Two Non-Consecutive Days, Three Consecutive Days, and Three Non-Consecutive Days for Estimating Dietary Intake of Chinese Adult. Nutrients. 2022; 14(9):1960. https://doi.org/10.3390/nu14091960
Chicago/Turabian StyleHuang, Kun, Liyun Zhao, Qiya Guo, Dongmei Yu, Yuxiang Yang, Qiuye Cao, Xiaolin Yuan, Lahong Ju, Shujuan Li, Xue Cheng, and et al. 2022. "Comparison of the 24 h Dietary Recall of Two Consecutive Days, Two Non-Consecutive Days, Three Consecutive Days, and Three Non-Consecutive Days for Estimating Dietary Intake of Chinese Adult" Nutrients 14, no. 9: 1960. https://doi.org/10.3390/nu14091960
APA StyleHuang, K., Zhao, L., Guo, Q., Yu, D., Yang, Y., Cao, Q., Yuan, X., Ju, L., Li, S., Cheng, X., Xu, X., & Fang, H. (2022). Comparison of the 24 h Dietary Recall of Two Consecutive Days, Two Non-Consecutive Days, Three Consecutive Days, and Three Non-Consecutive Days for Estimating Dietary Intake of Chinese Adult. Nutrients, 14(9), 1960. https://doi.org/10.3390/nu14091960