
Changing Dietary Habits: The Impact of Urbanization and Rising Socio-Economic Status in Families from Burkina Faso in Sub-Saharan Africa

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
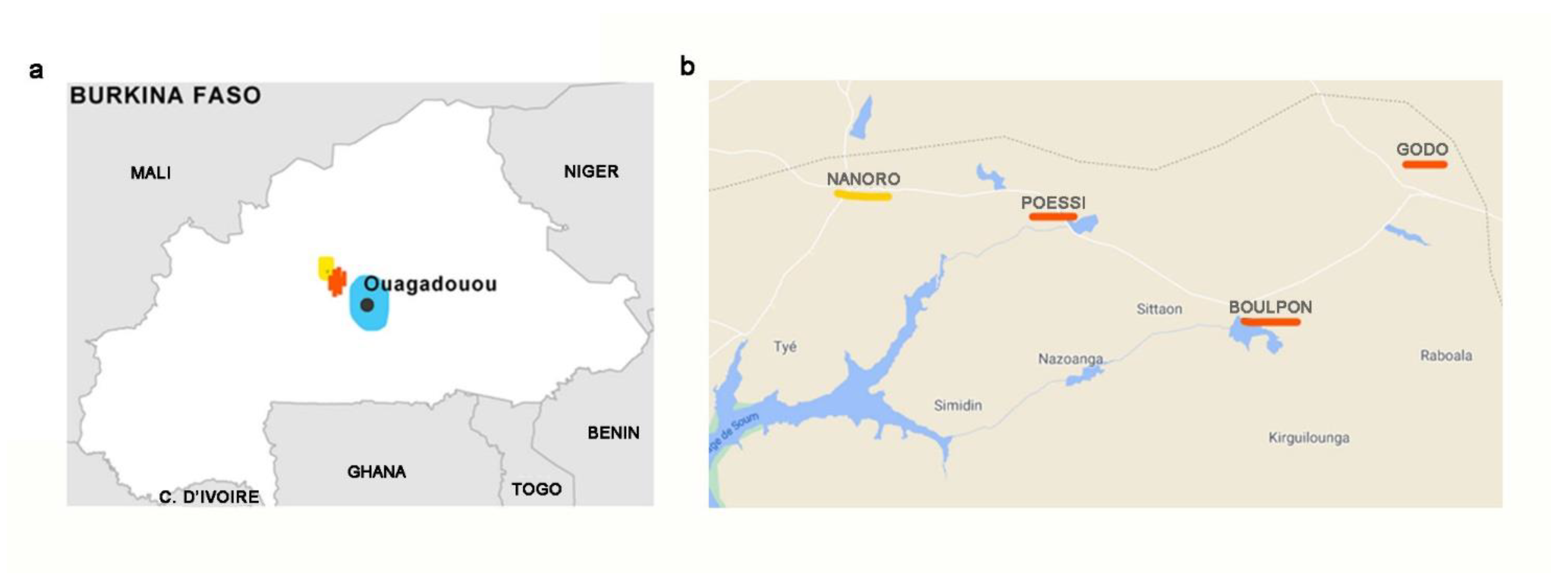
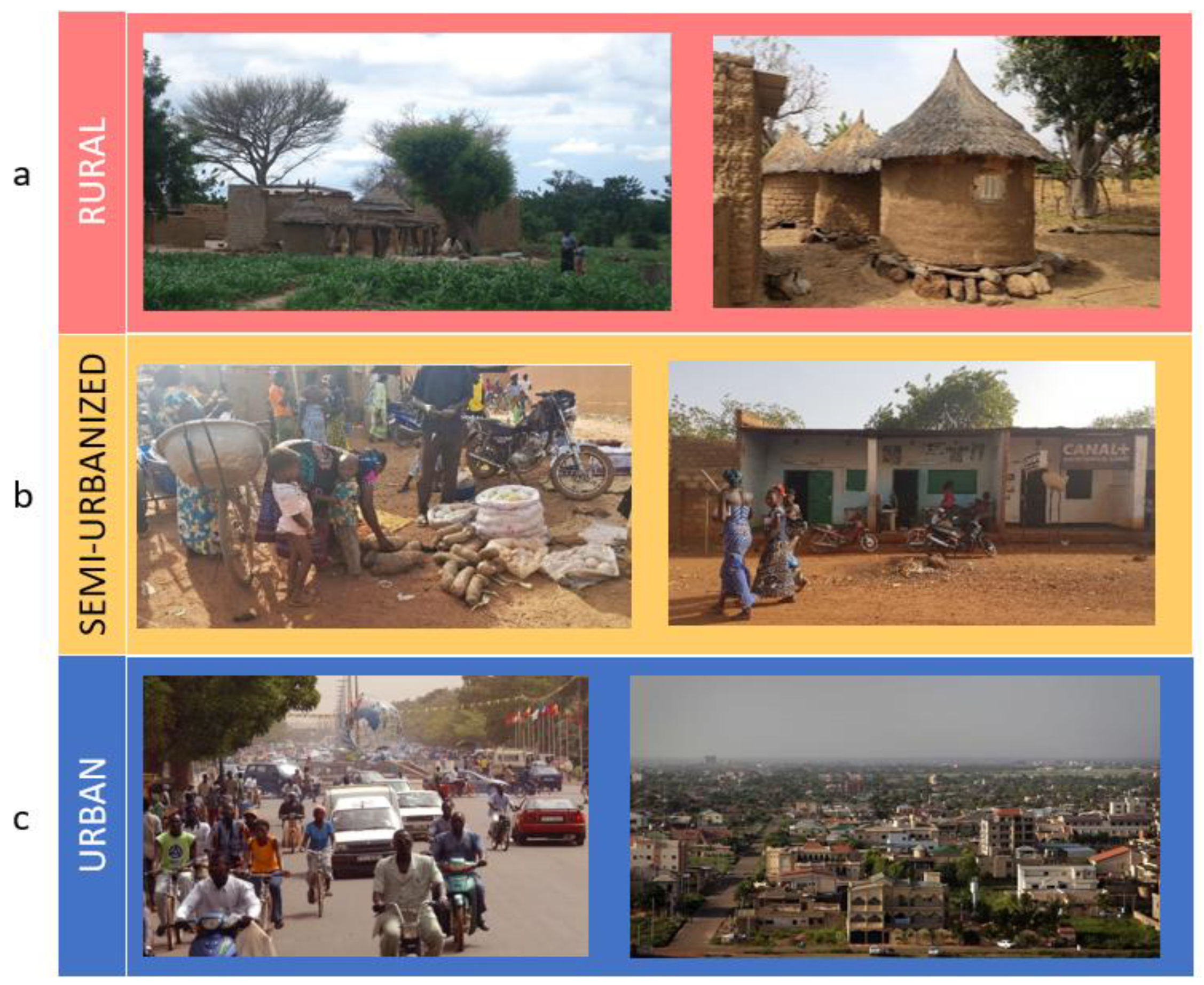
2.1. Characteristic of the Region, Setting and Study Population
- Rural cohort: 10 households (n = 54 individuals) living in the rural villages of Boulpon (n = 4 households), Godo (n = 3) and Poessi (n = 3).
- Semi-Urbanized cohort: 10 households (n = 55 individuals) from Nanoro.
- Urban cohort: 10 households (n = 50 individuals) living in the capital city of Ouagadougou selected among wealthy households.
2.2. Ethics
2.3. Data Collection and Nutritional Analyses
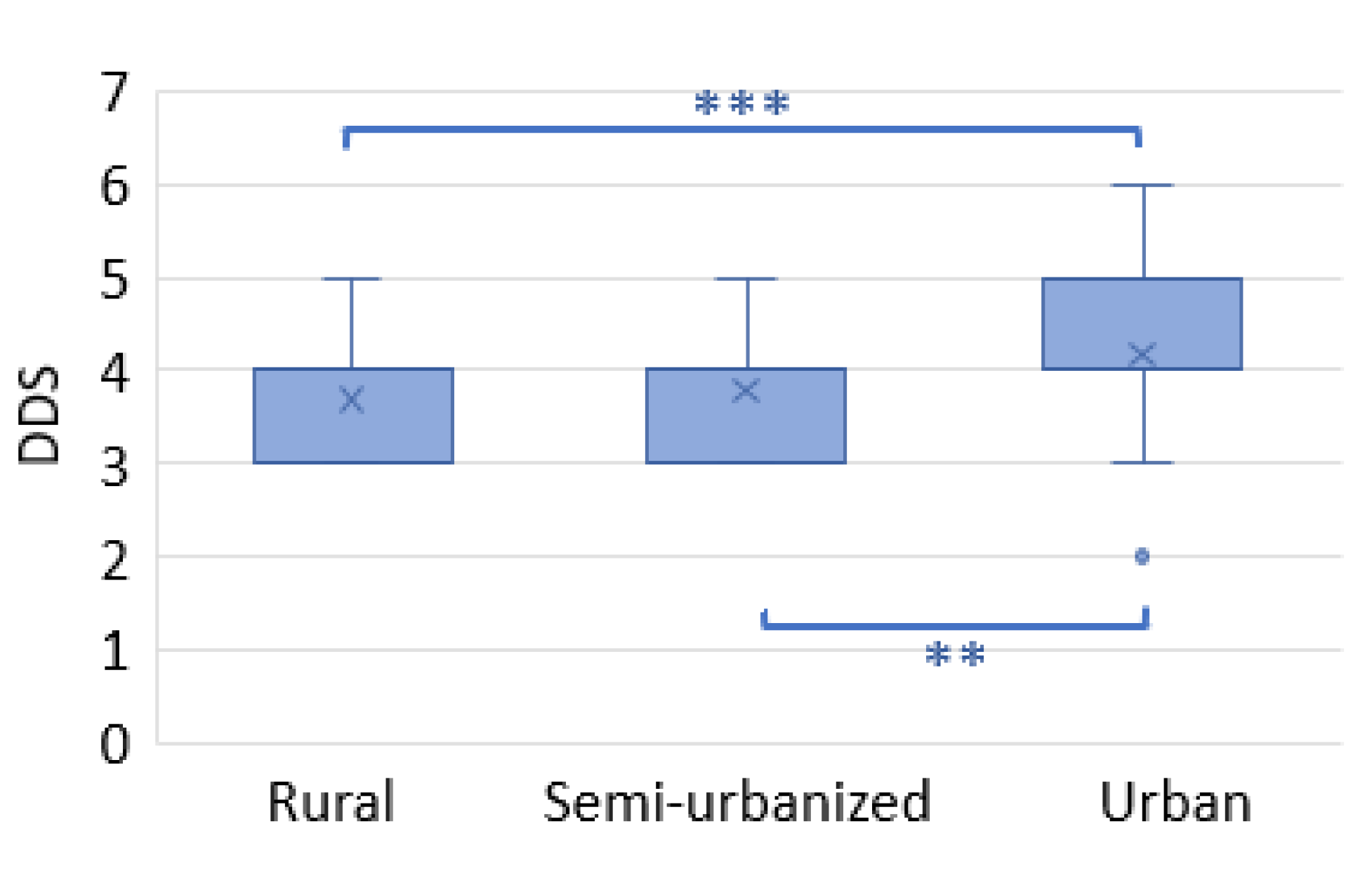
2.4. Dietary Diversity Score
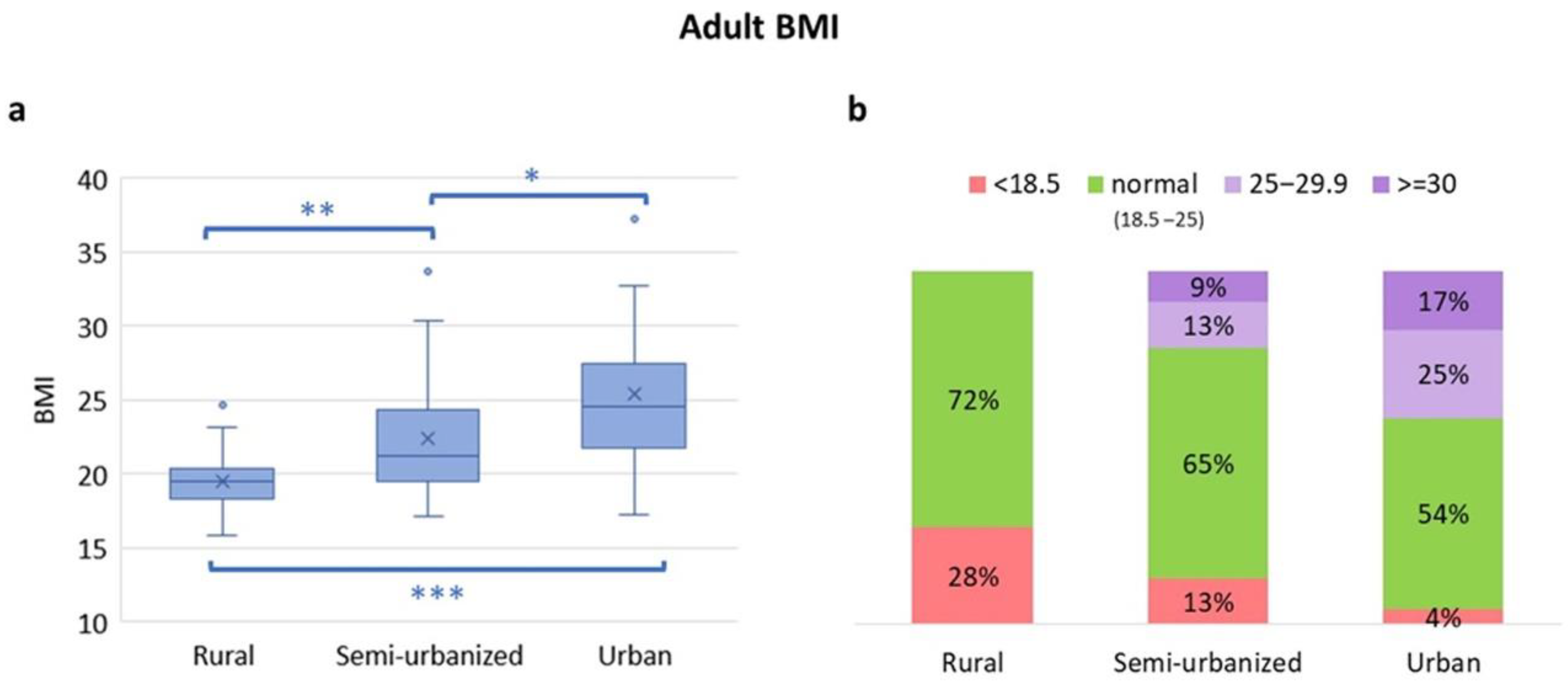
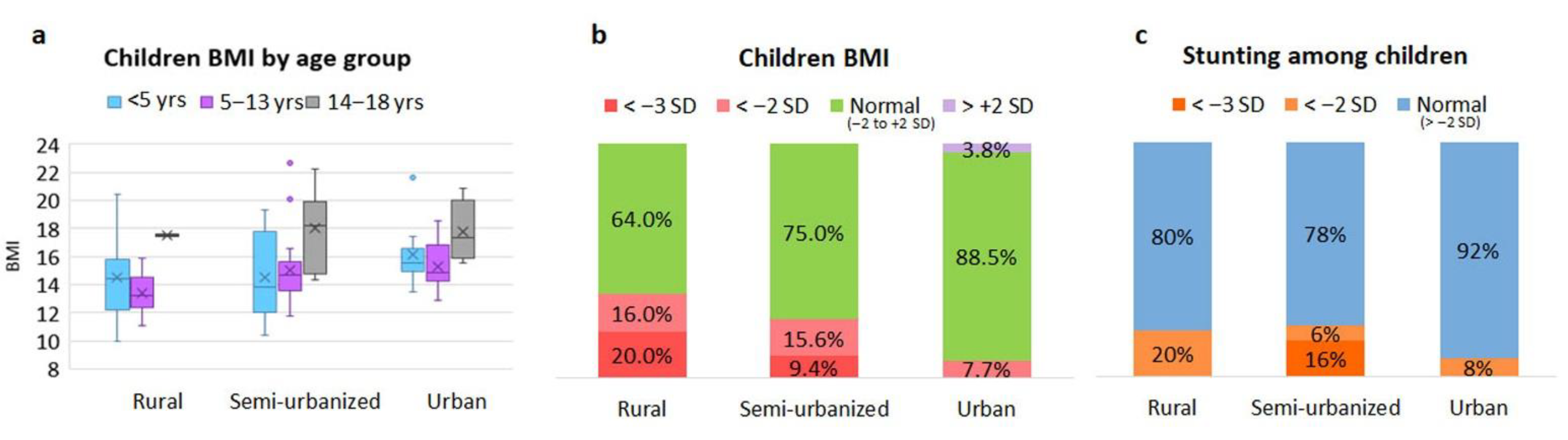
2.5. Anthropometry and Classification of Nutritional Status
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Three Burkinabè Cohorts
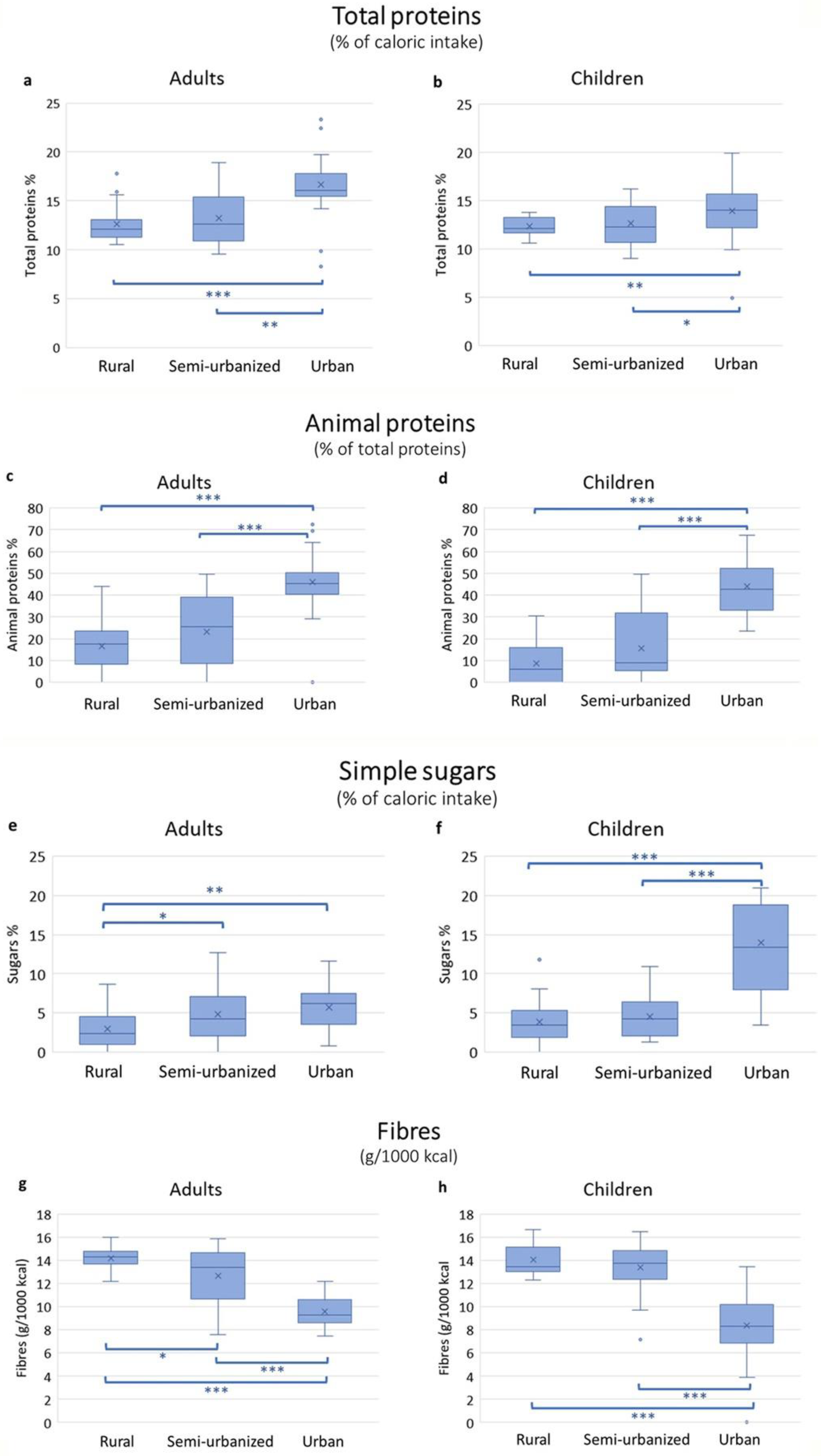
3.2. Energy and Macronutrient Intake Estimation Per Area
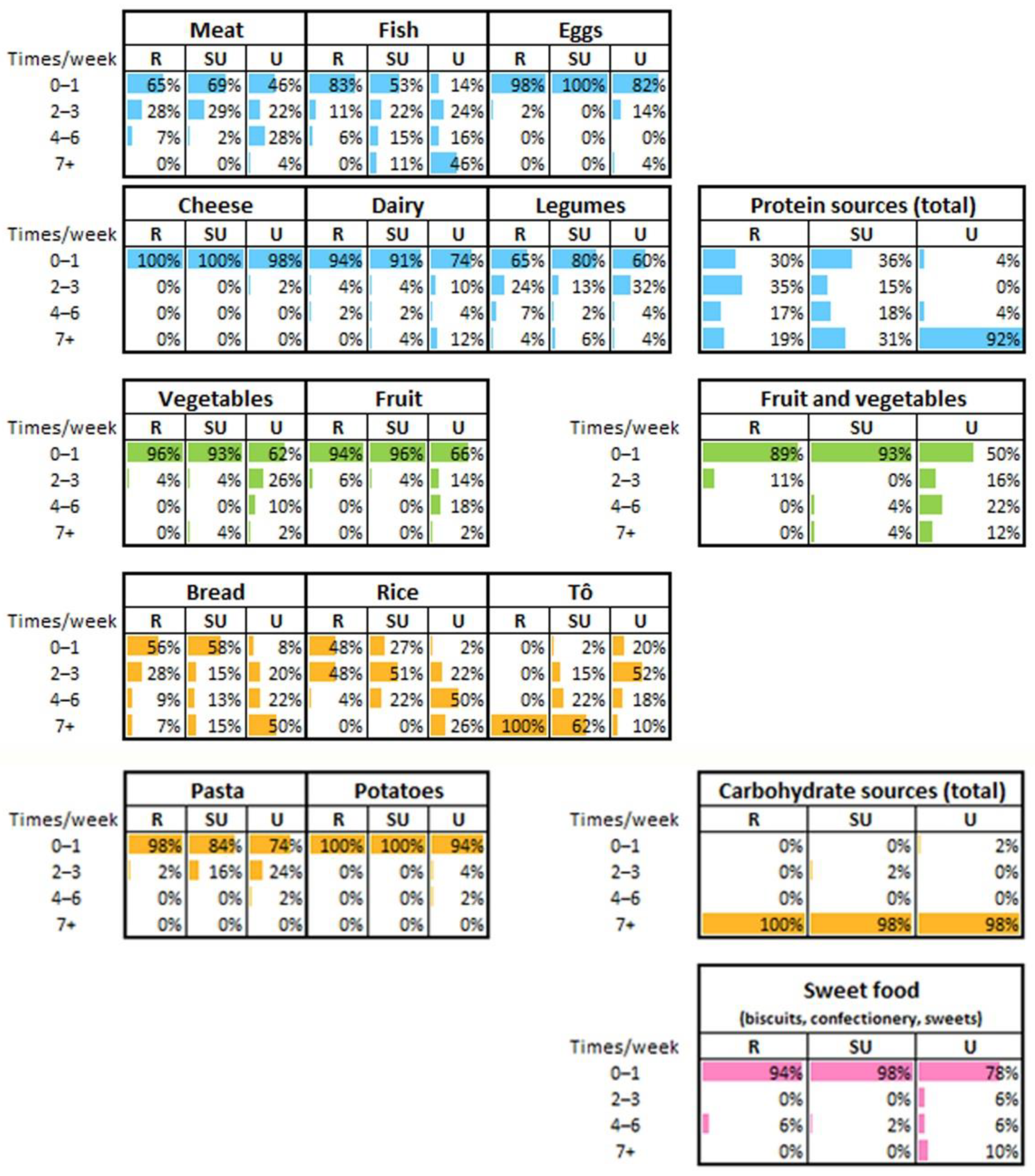
3.3. Food Frequency Consumption and Estimation of Dietary Diversity
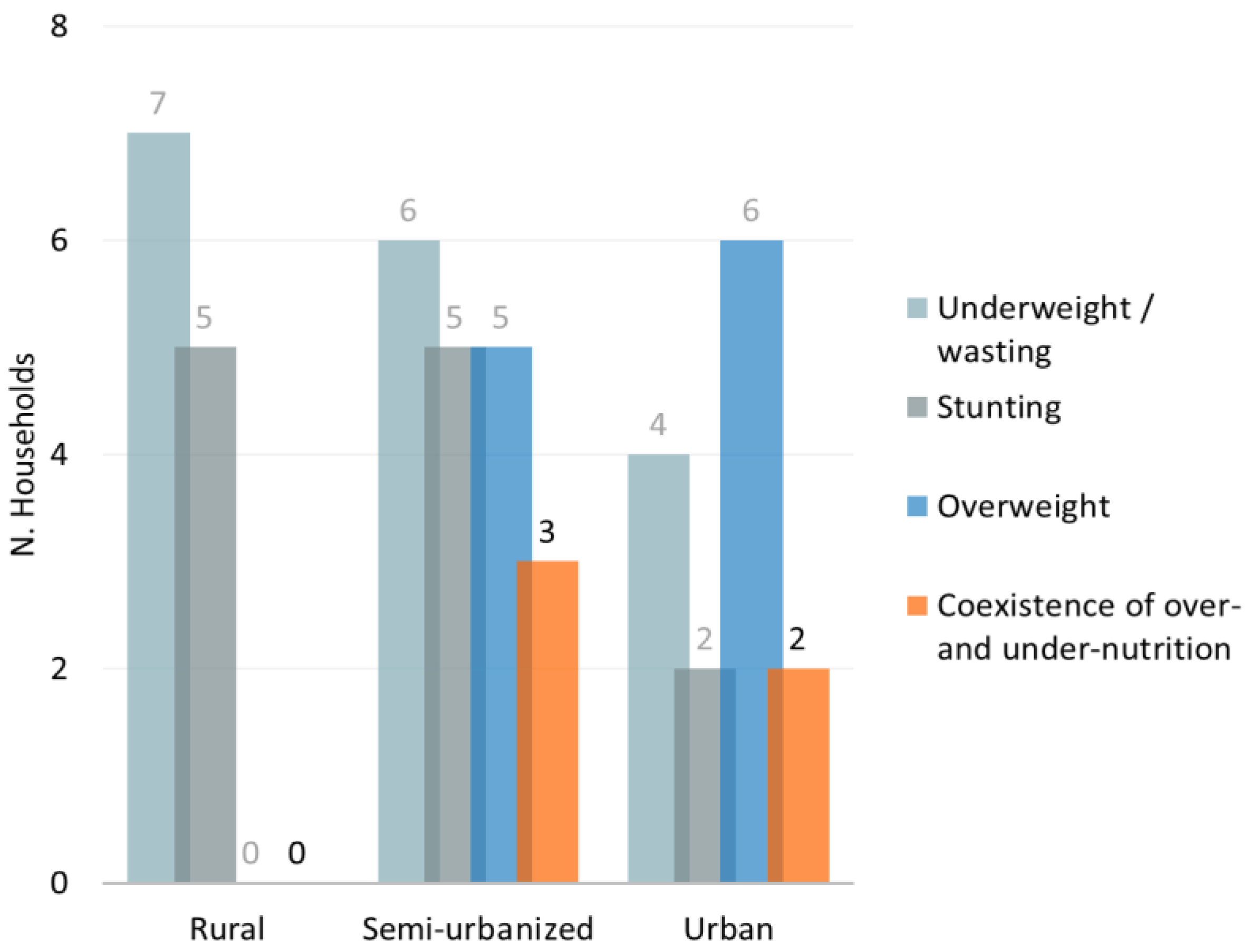
3.4. Nutritional Status Changes across the Cohorts
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Baker, P.; Machado, P.; Santos, T.; Sievert, K.; Backholer, K.; Hadjikakou, M.; Russell, C.; Huse, O.; Bell, C.; Scrinis, G.; et al. Ultra-processed foods and the nutrition transition: Global, regional and national trends, food systems transformations and political economy drivers. Obes. Rev. 2020, 21, e13126. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Popkin, B.M. The nutrition transition: New trends in the global diet. Nutr. Rev. 1997, 55, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. The nutrition transition: An overview of world patterns of change. Nutr. Rev. 2004, 62, S140–S143. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, G.; Nantel, G.; Shetty, P. Food and Agriculture Organization of the United Nations Globalization of food systems in developing countries: Impact on food security and nutrition. FAO Food Nutr. Pap. 2004, 83, 1–300. [Google Scholar]
- Ruel, M.T.; Garrett, J.L. Features of Urban Food and Nutrition Security and Considerations for Successful Urban Programming. Electron. J. Agric. Dev. Econ. 2004, 1, 242–271. [Google Scholar]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Now and then: The Global Nutrition Transition: The Pandemic of Obesity in Developing Countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Global Action Plan for the Prevention and Control of NCDs 2013–2020. Available online: https://www.who.int/publications-detail-redirect/9789241506236 (accessed on 18 August 2021).
- Cecchini, M.; Sassi, F.; Lauer, J.A.; Lee, Y.Y.; Guajardo-Barron, V.; Chisholm, D. Tackling of unhealthy diets, physical inactivity, and obesity: Health effects and cost-effectiveness. Lancet 2010, 376, 1775–1784. [Google Scholar] [CrossRef]
- Mendez, M.A.; Monteiro, C.A.; Popkin, B.M. Overweight exceeds underweight among women in most developing countries. Am. J. Clin. Nutr. 2005, 81, 714–721. [Google Scholar] [CrossRef] [Green Version]
- Global, Regional, and National Comparative Risk Assessment of 84 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016—The Lancet. Available online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)32366-8/fulltext (accessed on 18 August 2021).
- Frank, L.K.; Kröger, J.; Schulze, M.B.; Bedu-Addo, G.; Mockenhaupt, F.P.; Danquah, I. Dietary patterns in urban Ghana and risk of type 2 diabetes. Br. J. Nutr. 2014, 112, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Dake, F.A.A.; Thompson, A.L.; Ng, S.W.; Agyei-Mensah, S.; Codjoe, S.N.A. The Local Food Environment and Body Mass Index among the Urban Poor in Accra, Ghana. J. Urban Health 2016, 93, 438–455. [Google Scholar] [CrossRef] [Green Version]
- Kiawi, E.; Edwards, R.; Shu, J.; Unwin, N.; Kamadjeu, R.; Mbanya, J.C. Knowledge, attitudes, and behavior relating to diabetes and its main risk factors among urban residents in Cameroon: A qualitative survey. Ethn. Dis. 2006, 16, 503–509. [Google Scholar] [PubMed]
- Cockx, L.; Colen, L.; De Weerdt, J. From corn to popcorn? Urbanization and dietary change: Evidence from rural-urban migrants in Tanzania. World Dev. 2018, 110, 140–159. [Google Scholar] [CrossRef]
- Research Institute (IFPRI), I.F.P. Global Nutrition Report 2016 from Promise to Impact Ending Malnutrition by 2030; International Food Policy Research Institute: Washington, DC, USA, 2016. [Google Scholar] [CrossRef] [Green Version]
- Yach, D.; Hawkes, C.; Gould, C.L.; Hofman, K.J. The global burden of chronic diseases: Overcoming impediments to prevention and control. JAMA 2004, 291, 2616–2622. [Google Scholar] [CrossRef] [PubMed]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mudie, K.; Jin, M.M.; Tan; Kendall, L.; Addo, J.; Dos-Santos-Silva, I.; Quint, J.; Smeeth, L.; Cook, S.; Nitsch, R.; et al. Non-communicable diseases in sub-Saharan Africa: A scoping review of large cohort studies. J. Glob. Health 2019, 9, 020409. [Google Scholar] [CrossRef]
- Owino, V.O. Challenges and opportunities to tackle the rising prevalence of diet-related non-communicable diseases in Africa. Proc. Nutr. Soc. 2019, 78, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Juma, K.; Juma, P.; Shumba, C.; Otieno, P.; Asiki, G. Non-Communicable Diseases and Urbanization in African Cities: A Narrative Review. In Public Health in Developing Countries: Challenges and Opportunities; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- Bosu, W.K. An overview of the nutrition transition in West Africa: Implications for non-communicable diseases. Proc. Nutr. Soc. 2015, 74, 466–477. [Google Scholar] [CrossRef]
- De Filippo, C.; Cavalieri, D.; Di Paola, M.; Ramazzotti, M.; Poullet, J.B.; Massart, S.; Collini, S.; Pieraccini, G.; Lionetti, P. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc. Natl. Acad. Sci. USA 2010, 107, 14691–14696. [Google Scholar] [CrossRef] [Green Version]
- De Filippo, C.; Di Paola, M.; Ramazzotti, M.; Albanese, D.; Pieraccini, G.; Banci, E.; Miglietta, F.; Cavalieri, D.; Lionetti, P. Diet, Environments, and Gut Microbiota. A Preliminary Investigation in Children Living in Rural and Urban Burkina Faso and Italy. Front. Microbiol. 2017, 8, 1979. [Google Scholar] [CrossRef] [Green Version]
- Sié, A.; Tapsoba, C.; Dah, C.; Ouermi, L.; Zabre, P.; Bärnighausen, T.; Arzika, A.M.; Lebas, E.; Snyder, B.M.; Moe, C.; et al. Dietary diversity and nutritional status among children in rural Burkina Faso. Int. Health 2018, 10, 157–162. [Google Scholar] [CrossRef]
- Becquey, E.; Savy, M.; Danel, P.; Dabiré, H.B.; Tapsoba, S.; Martin-Prével, Y. Dietary patterns of adults living in Ouagadougou and their association with overweight. Nutr. J. 2010, 9, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Population Growth (annual %)—Burkina Faso | Data. Available online: https://data.worldbank.org/indicator/SP.POP.GROW?locations=BF (accessed on 20 August 2021).
- World Urbanization Prospects—Population Division—United Nations. Available online: https://population.un.org/wup/Publications/ (accessed on 18 August 2021).
- Derra, K.; Rouamba, E.; Kazienga, A.; Ouedraogo, S.; Tahita, M.C.; Sorgho, H.; Valea, I.; Tinto, H. Profile: Nanoro Health and Demographic Surveillance System. Int. J. Epidemiol. 2012, 41, 1293–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- INFOODS: FAO/INFOODS Databases. Available online: http://www.fao.org/infoods/infoods/tables-and-databases/faoinfoods-databases/en/ (accessed on 19 August 2021).
- FAO. Guidelines for Measuring Household and Individual Dietary Diversity. 2010. Available online: http://www.fao.org/docrep/014/i1983e/i1983e00.pdf (accessed on 18 November 2021).
- Kennedy, G.L.; Pedro, M.R.; Seghieri, C.; Nantel, G.; Brouwer, I. Dietary diversity score is a useful indicator of micronutrient intake in non-breast-feeding Filipino children. J. Nutr. 2007, 137, 472–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirmiran, P.; Azadbakht, L.; Esmaillzadeh, A.; Azizi, F. Dietary diversity score in adolescents—A good indicator of the nutritional adequacy of diets: Tehran lipid and glucose study. Asia. Pac. J. Clin. Nutr. 2004, 13, 56–60. [Google Scholar]
- Developing and Validating Simple Indicators of Dietary Quality and Energy Intake of Infants and Young Children in Developing Countries | Food and Nutrition Technical Assistance III Project (FANTA). Available online: https://www.fantaproject.org/research/indicators-dietary-quality-intake-children (accessed on 28 September 2021).
- Foote, J.A.; Murphy, S.P.; Wilkens, L.R.; Basiotis, P.P.; Carlson, A. Dietary variety increases the probability of nutrient adequacy among adults. J. Nutr. 2004, 134, 1779–1785. [Google Scholar] [CrossRef] [Green Version]
- Child Growth Standards. Available online: https://www.who.int/tools/child-growth-standards (accessed on 13 April 2022).
- de Onis, M.; Borghi, E.; Arimond, M.; Webb, P.; Croft, T.; Saha, K.; De-Regil, L.M.; Thuita, F.; Heidkamp, R.; Krasevec, J.; et al. Prevalence thresholds for wasting, overweight and stunting in children under 5 years. Public Health Nutr. 2019, 22, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 13 April 2022).
- Abdoul-latif, F.M.; Bassolé, I.H.; Bassolé, I.H.; Dicko, M.H.; Dicko, M.H. Proximate composition of traditional local sorghum beer “dolo” manufactured in Ouagadougou. Afr. J. Biotechnol. 2013, 12, 1517–1522. [Google Scholar] [CrossRef]
- EFSA (European Food Safety Authority) Scientific Opinion on Dietary Reference Values for Carbohydrates and Dietary Fibre. Available online: https://www.efsa.europa.eu/en/efsajournal/pub/1462 (accessed on 30 August 2021).
- Akoto, E.; Tambashe, B. Socioeconomic Inequalities in Infant and Child Mortality among Urban and Rural Areas in Sub-Saharan Africa. In Proceedings of the First seminar of the IUSSP Committee on Emerging Health Threats, Max Planck Institute for Demographic Research, Rostock, Germany, 19–21 June 2002. [Google Scholar]
- Fotso, J.-C. Urban-rural differentials in child malnutrition: Trends and socioeconomic correlates in sub-Saharan Africa. Health Place 2007, 13, 205–223. [Google Scholar] [CrossRef]
- Tusting, L.S.; Gething, P.W.; Gibson, H.S.; Greenwood, B.; Knudsen, J.; Lindsay, S.W.; Bhatt, S. Housing and child health in sub-Saharan Africa: A cross-sectional analysis. PLoS Med. 2020, 17, e1003055. [Google Scholar] [CrossRef] [Green Version]
- Hayase, Y.; Liaw, K.L. Factors on polygamy in sub-Saharan Africa: Findings based on the Demographic and Health Surveys. Dev. Econ. 1997, 35, 293–327. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, H.; Roser, M. Urbanization. Our World Data. June 2018. Available online: https://ourworldindata.org/urbanization (accessed on 13 April 2022).
- Cockx, L.; Liesbeth, C.; De Weerdt, J.; Gomez, Y.; Gomez y Paloma, S. Urbanization as a Driver of Changing Food Demand in Africa Evidence from Rural-Urban Migration in Tanzania; JRC Working Papers JRC107918; Joint Research Centre (Seville Site): Seville, Spain, 2019. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, M.D.; Walker, S.P.; Younger, N.M.; Bennett, F.I. Use of a food frequency questionnaire to assess diets of Jamaican adults: Validation and correlation with biomarkers. Nutr. J. 2011, 10, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arsenault, J.E.; Moursi, M.; Olney, D.K.; Becquey, E.; Ganaba, R. Validation of 24-h dietary recall for estimating nutrient intakes and adequacy in adolescents in Burkina Faso. Matern. Child. Nutr. 2020, 16, e13014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codjoe, S.N.A.; Okutu, D.; Abu, M. Urban Household Characteristics and Dietary Diversity: An Analysis of Food Security in Accra, Ghana. Food Nutr. Bull. 2016, 37, 202–218. [Google Scholar] [CrossRef] [Green Version]
- Ren, Y.; Castro Campos, B.; Peng, Y.; Glauben, T. Nutrition Transition with Accelerating Urbanization? Empirical Evidence from Rural China. Nutrients 2021, 13, 921. [Google Scholar] [CrossRef]
- Tan, J.; McKenzie, C.; Potamitis, M.; Thorburn, A.N.; Mackay, C.R.; Macia, L. The role of short-chain fatty acids in health and disease. Adv. Immunol. 2014, 121, 91–119. [Google Scholar] [CrossRef]
- Yatsunenko, T.; Rey, F.E.; Manary, M.J.; Trehan, I.; Dominguez-Bello, M.G.; Contreras, M.; Magris, M.; Hidalgo, G.; Baldassano, R.N.; Anokhin, A.P.; et al. Human gut microbiome viewed across age and geography. Nature 2012, 486, 222–227. [Google Scholar] [CrossRef]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [Green Version]
- Schnorr, S.L.; Candela, M.; Rampelli, S.; Centanni, M.; Consolandi, C.; Basaglia, G.; Turroni, S.; Biagi, E.; Peano, C.; Severgnini, M.; et al. Gut microbiome of the Hadza hunter-gatherers. Nat. Commun. 2014, 5, 3654. [Google Scholar] [CrossRef]
- Cho, I.; Blaser, M.J. The human microbiome: At the interface of health and disease. Nat. Rev. Genet. 2012, 13, 260–270. [Google Scholar] [CrossRef] [Green Version]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 27 August 2021).
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Seale, J.L.; Wahl, T.; Bai, J. The changing dietary patterns and health issues in China. China Agric. Econ. Rev. 2019, 11, 143–159. [Google Scholar] [CrossRef]
- Poskitt, E.M.E. Childhood obesity in low- and middle-income countries. Paediatr. Int. Child. Health 2014, 34, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Methven, E.; McDowell, Z.C.; Hacking, B.; Alexander, D.; Stewart, L.; Kelnar, C.J.H. Health consequences of obesity. Arch. Dis. Child. 2003, 88, 748–752. [Google Scholar] [CrossRef]
- Serdula, M.K.; Ivery, D.; Coates, R.J.; Freedman, D.S.; Williamson, D.F.; Byers, T. Do obese children become obese adults? A review of the literature. Prev. Med. 1993, 22, 167–177. [Google Scholar] [CrossRef]
- Rolland-Cachera, M.F.; Deheeger, M.; Bellisle, F.; Sempé, M.; Guilloud-Bataille, M.; Patois, E. Adiposity rebound in children: A simple indicator for predicting obesity. Am. J. Clin. Nutr. 1984, 39, 129–135. [Google Scholar] [CrossRef]
- Bickler, S.W.; Wang, A.; Amin, S.; Halbach, J.; Lizardo, R.; Cauvi, D.M.; De Maio, A. Urbanization in Sub-Saharan Africa: Declining Rates of Chronic and Recurrent Infection and Their Possible Role in the Origins of Non-communicable Diseases. World J. Surg. 2018, 42, 1617–1628. [Google Scholar] [CrossRef]
- Ministere de la Sante, Secretariat General Burkina Faso|Enquête nutritionnelle dans les communautés et sites d’accueil—Rapid SMART—2019|HumanitarianResponse. Available online: https://www.humanitarianresponse.info/en/op%C3%A9rations/burkina-faso/document/burkina-faso-enqu%C3%AAte-nutritionnelle-dans-les-communaut%C3%A9s-et-sites-d (accessed on 30 August 2021).
- Wells, J.C.; Sawaya, A.L.; Wibaek, R.; Mwangome, M.; Poullas, M.S.; Yajnik, C.S.; Demaio, A. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet 2020, 395, 75–88. [Google Scholar] [CrossRef]
- The Double Burden of Malnutrition Case Studies from Six Developing Countries. Available online: https://www.fao.org/3/a0442e/a0442e03.htm (accessed on 14 January 2022).
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef]
- Doak, C.M.; Adair, L.S.; Bentley, M.; Monteiro, C.; Popkin, B.M. The dual burden household and the nutrition transition paradox. Int. J. Obes. 2005, 29, 129–136. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rural (R) n. (%) | Semi-Urbanized (SU) n. (%) | Urban (U) n. (%) | |
|---|---|---|---|
| Participants (n = 159) | 54 (34.0) | 55 (34.6) | 50 (31.4) |
| Fathers/mothers (n = 26/40) | 8 (30.8)/19 (47.5) | 9 (34.6)/11 (27.5) | 9 (34.6)/10 (25.0) |
| Offspring (n = 93) | 27 (29.0) | 35 (37.6) | 31 (33.4) |
| Children Males/females (n = 44/49) | 14 (31.8)/13 (26.5) | 16 (36.4)/19 (38.8) | 14 (31.8)/17 (34.7) |
| Age distribution (years) | |||
| <5 (n = 27) | 11 (40.7) | 6 (22.3) | 10 (37.0) |
| 5–13 (n = 43) | 12 (27.9) | 19 (44.2) | 12 (27.9) |
| 14–18 (n = 13) | 2 (15.4) | 7 (53.8) | 4 (30.8) |
| >18–77 (n = 76) | 29 (38.1) | 23 (30.3) | 24 (31.6) |
| Parents/caregivers (n = 66) | 27 (40.9) | 20 (30.3) | 19 (28.8) |
| Religion of Parents/caregiver | |||
| Muslim | 6 (22.2) | 7 (35) | 8 (42.1) |
| Christian Catholic | 7 (25.9) | 5 (25) | 9 (47.4) |
| Christian Protestant | 2 (7.5) | 6 (30) | 2 (10.5) |
| Traditional (animist) | 12 (44.4) | 2 (10) | 0 (0) |
| Education level of parents/caregivers | |||
| Males | |||
| No school education | 8 (100) | 7 (77.8) | 1 (11.1) |
| Primary school | 0 (0) | 0 (0) | 3 (33.3) |
| Intermediate | 0 (0) | 1 (11.1) | 3 (33.3) |
| High or more | 0 (0) | 1 (11.1) | 2 (22.2) |
| Females | |||
| No school education | 18 (94.7) | 9 (81.8) | 0 (0) |
| Primary school | 1 (5.3) | 2 (18.2) | 2 (20) |
| Intermediate | 0 (0) | 0 (0) | 6 (60) |
| High or more | 0 (0) | 0 (0) | 2 (20) |
| Occupation of parents/caregivers | |||
| Males | |||
| Manual worker | 8 (100) | 8 (88.9) | 4 (44.4) |
| Professional | 0 (0) | 1 (11.1) | 4 (44.4) |
| Retired | 0 (0) | 0 (0) | 1 (11.2) |
| Females | |||
| Housewife/farmer | 19 (100) | 11 (100) | 4 (40) |
| Student | 0 (0) | 0 (0) | 1 (10) |
| Manual worker | 0 (0) | 0 (0) | 1 (10) |
| Professional | 0 (0) | 0 (0) | 4 (40) |
| School attendance among children at school age (6–16 y) | |||
| Attending | 0 (0) | 21 (100) | 12 (85.7) |
| Habitual alcohol consumption (parents/caregivers) | |||
| Alcoholic fermented products (e.g., dolo) | 16 (55.2) | 4 (17.4) | 3 (12.5) |
| Alcoholic beverages (beer, wine, spirits) | 2 (6.9) | 0 (0) | 8 (33.3) |
| Smoking (parents/caregivers) | |||
| Smoking habit | 0 (0) | 1 (4.3) | 1 (4.2) |
| Means of transport of adults (>18 y) | |||
| Walk and/or bike | 26 (89.7) | 16 (69.6) | 8 (33.3) |
| Scooter and/or car | 3 (10.3) | 7 (30.4) | 16 (66.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casari, S.; Di Paola, M.; Banci, E.; Diallo, S.; Scarallo, L.; Renzo, S.; Gori, A.; Renzi, S.; Paci, M.; de Mast, Q.; et al. Changing Dietary Habits: The Impact of Urbanization and Rising Socio-Economic Status in Families from Burkina Faso in Sub-Saharan Africa. Nutrients 2022, 14, 1782. https://doi.org/10.3390/nu14091782
Casari S, Di Paola M, Banci E, Diallo S, Scarallo L, Renzo S, Gori A, Renzi S, Paci M, de Mast Q, et al. Changing Dietary Habits: The Impact of Urbanization and Rising Socio-Economic Status in Families from Burkina Faso in Sub-Saharan Africa. Nutrients. 2022; 14(9):1782. https://doi.org/10.3390/nu14091782
Chicago/Turabian StyleCasari, Silene, Monica Di Paola, Elena Banci, Salou Diallo, Luca Scarallo, Sara Renzo, Agnese Gori, Sonia Renzi, Monica Paci, Quirijn de Mast, and et al. 2022. "Changing Dietary Habits: The Impact of Urbanization and Rising Socio-Economic Status in Families from Burkina Faso in Sub-Saharan Africa" Nutrients 14, no. 9: 1782. https://doi.org/10.3390/nu14091782
APA StyleCasari, S., Di Paola, M., Banci, E., Diallo, S., Scarallo, L., Renzo, S., Gori, A., Renzi, S., Paci, M., de Mast, Q., Pecht, T., Derra, K., Kaboré, B., Tinto, H., Cavalieri, D., & Lionetti, P. (2022). Changing Dietary Habits: The Impact of Urbanization and Rising Socio-Economic Status in Families from Burkina Faso in Sub-Saharan Africa. Nutrients, 14(9), 1782. https://doi.org/10.3390/nu14091782