
Children’s and Parents’ Marburg Sugar Index (MSI) Values: Are They Comparable?

 ,
,  ,
,
Abstract
:
1. Introduction
- Children’s responses in regard to CNB and those of their parents correlate.
- The sugar indices are correlated with the caries experience.
2. Study Population and Methods
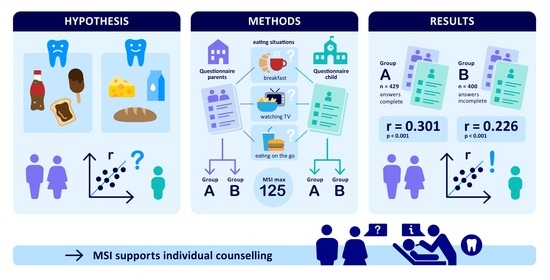
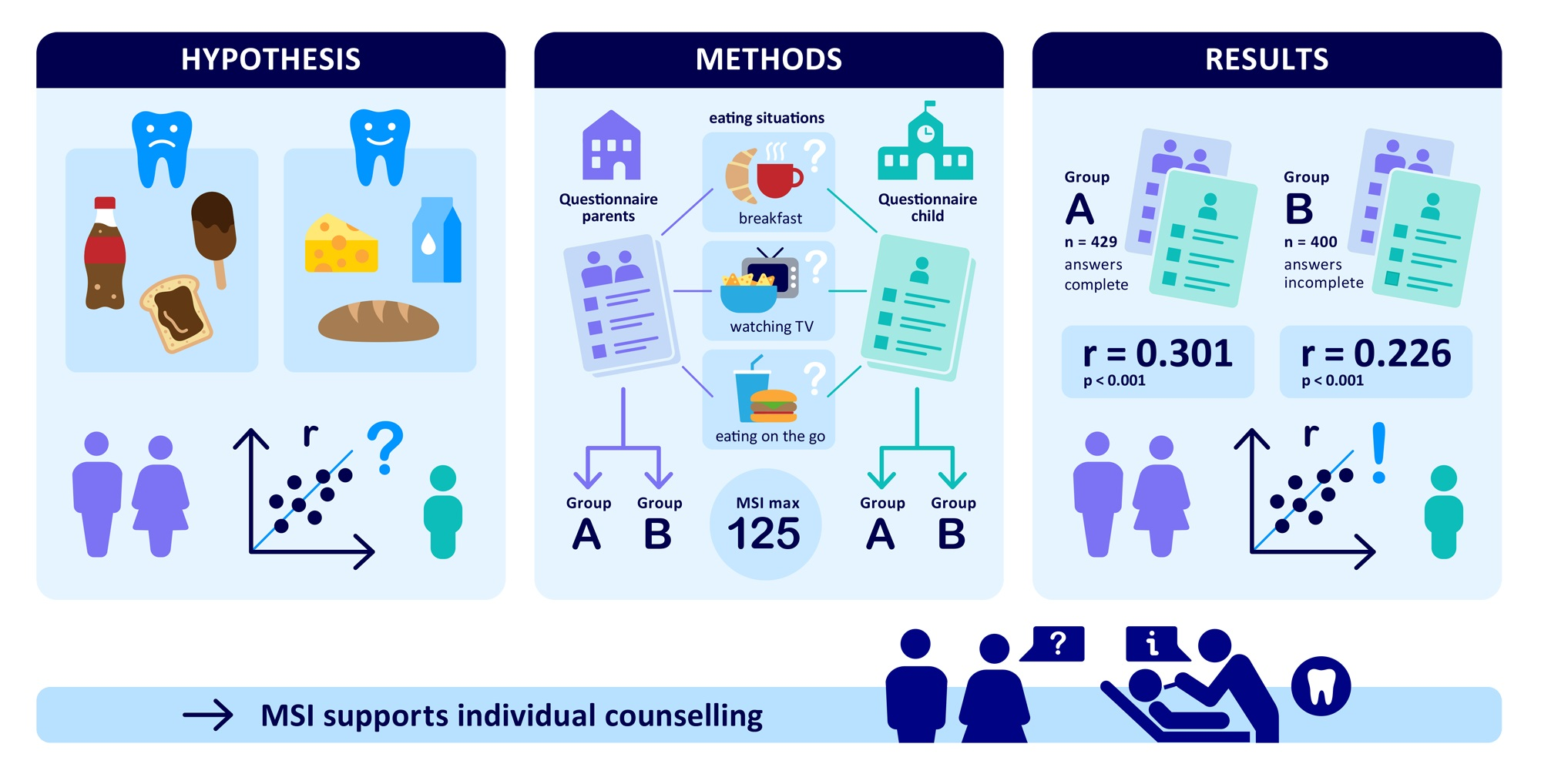
- Breakfast;
- Between-meal snacks;
- Watching television;
- Eating on the go.
- Schooling: ranging from no diploma up to high school diploma enabling university attendance (1–5 points);
- Occupational training: ranging from no degree up to a university degree (1–4 points);
- Occupational status: ranging from unemployed up to academic/self-employed (1–6 points).
- Low class (Low SES): 6–18 points;
- Middle and upper class (Higher SES): 19–30 points.
Statistical Analysis
3. Results
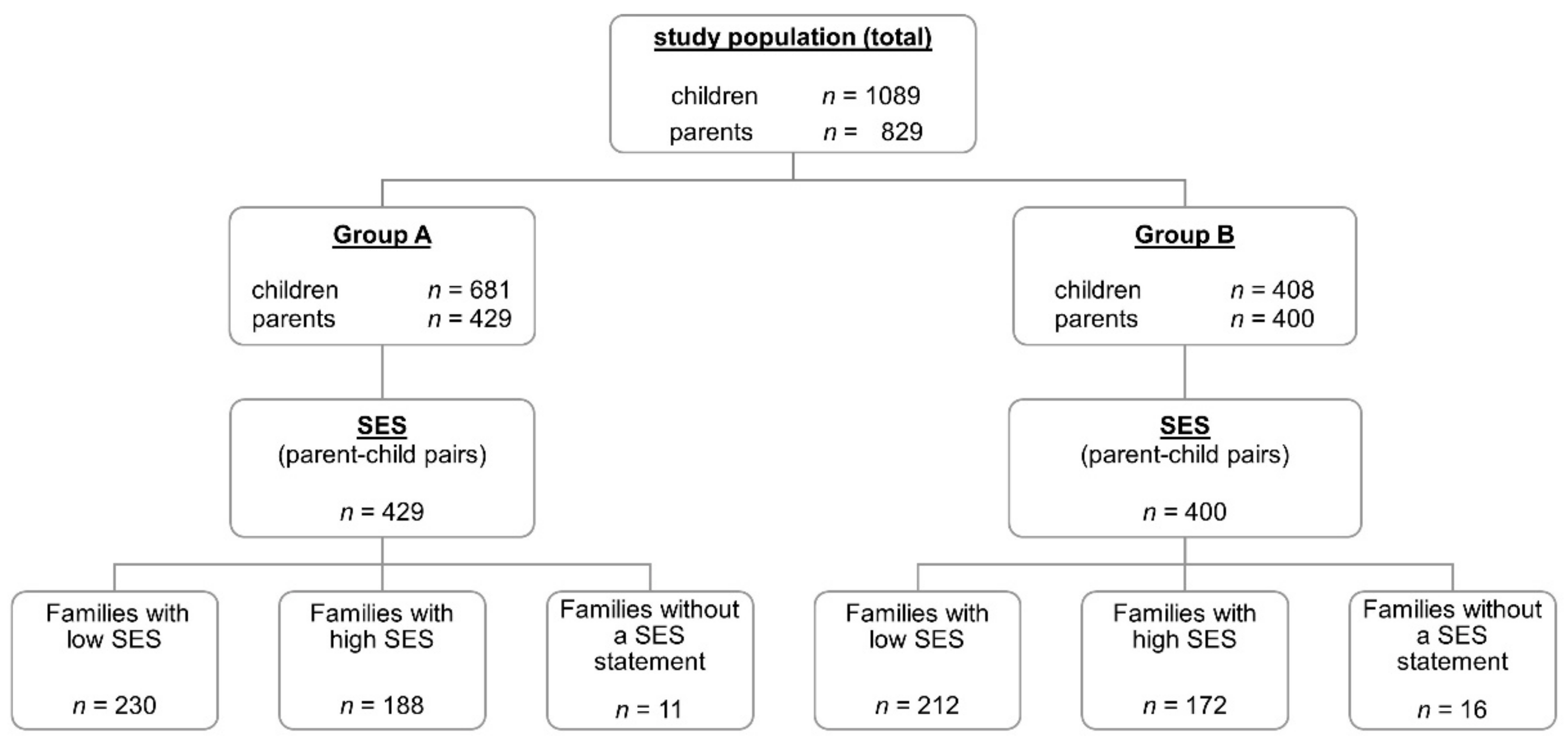
- Group A comprised matched parent–child pairs who had responded to all of the food items in the diet section of the questionnaire.
- Group B comprised matched parent–child pairs who did not respond to all of the food items in the diet section of the questionnaire.
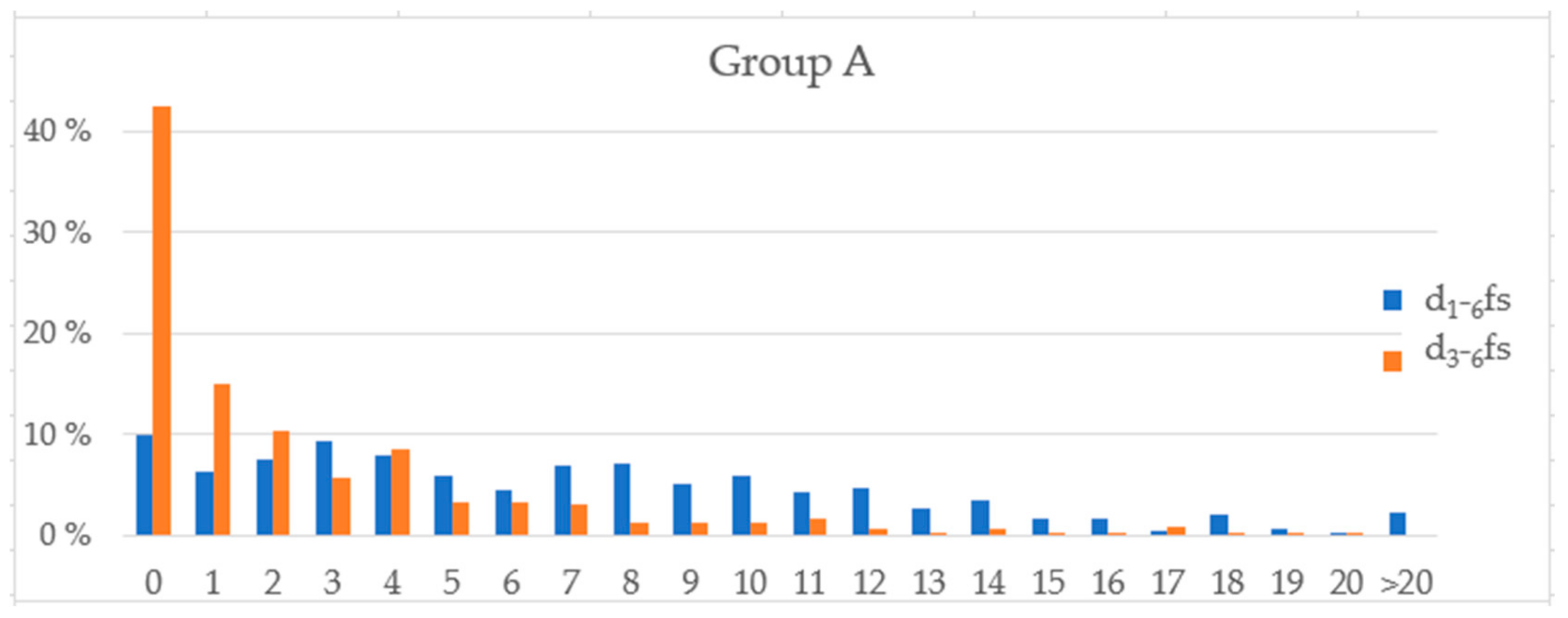
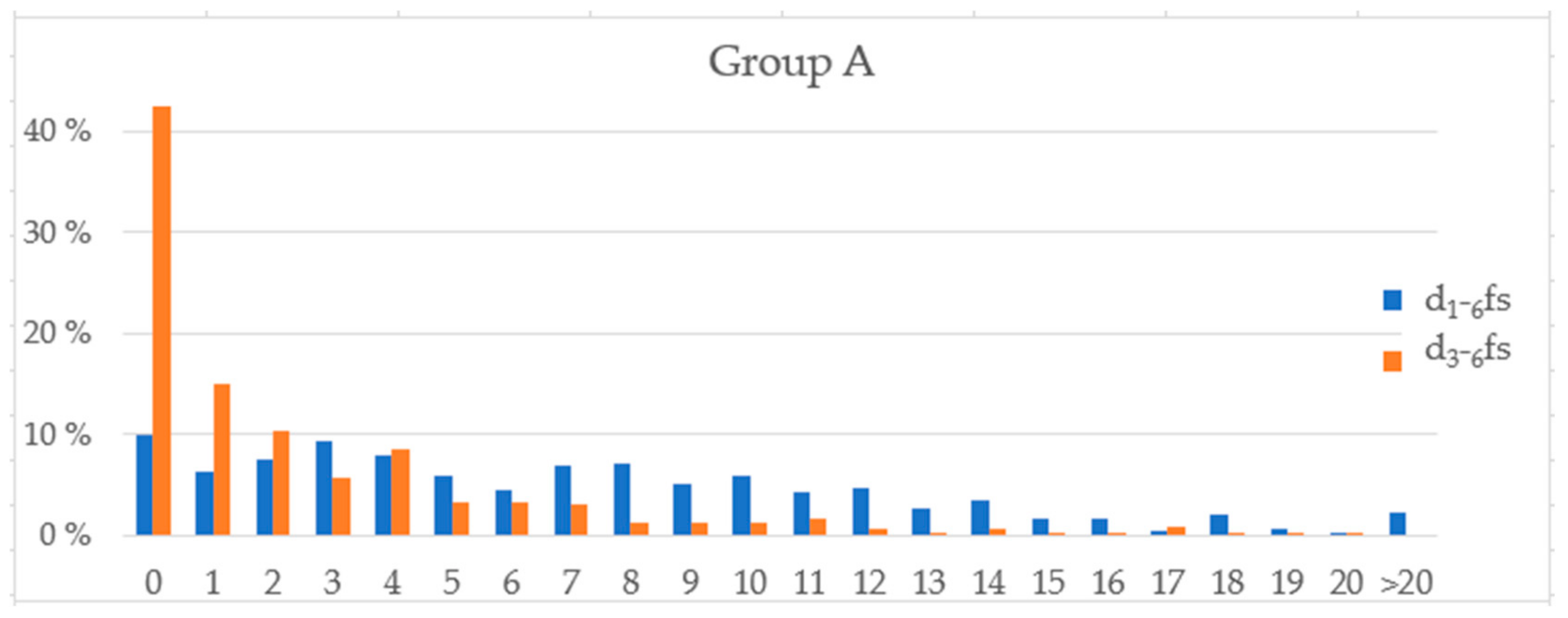
3.1. Correlation between the Children’s Caries Experience and the Sugar Indices of the Parent–Child Pairs
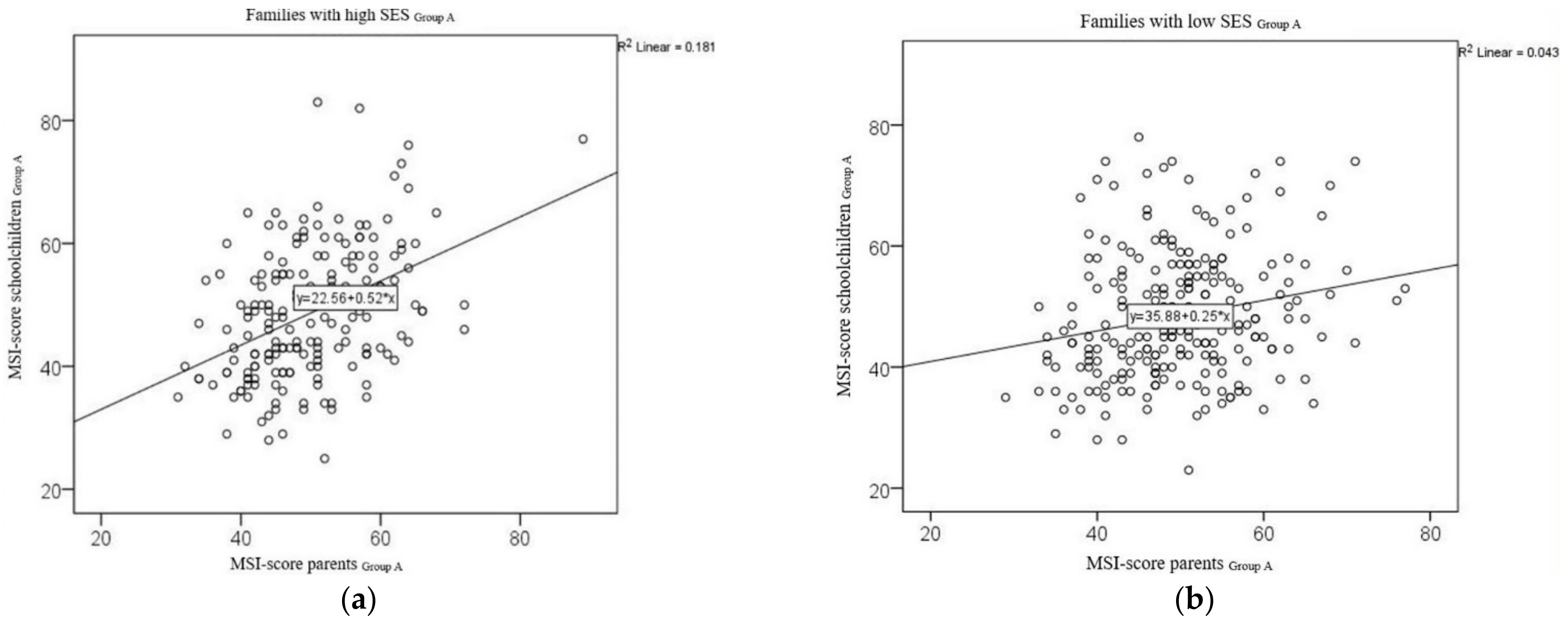
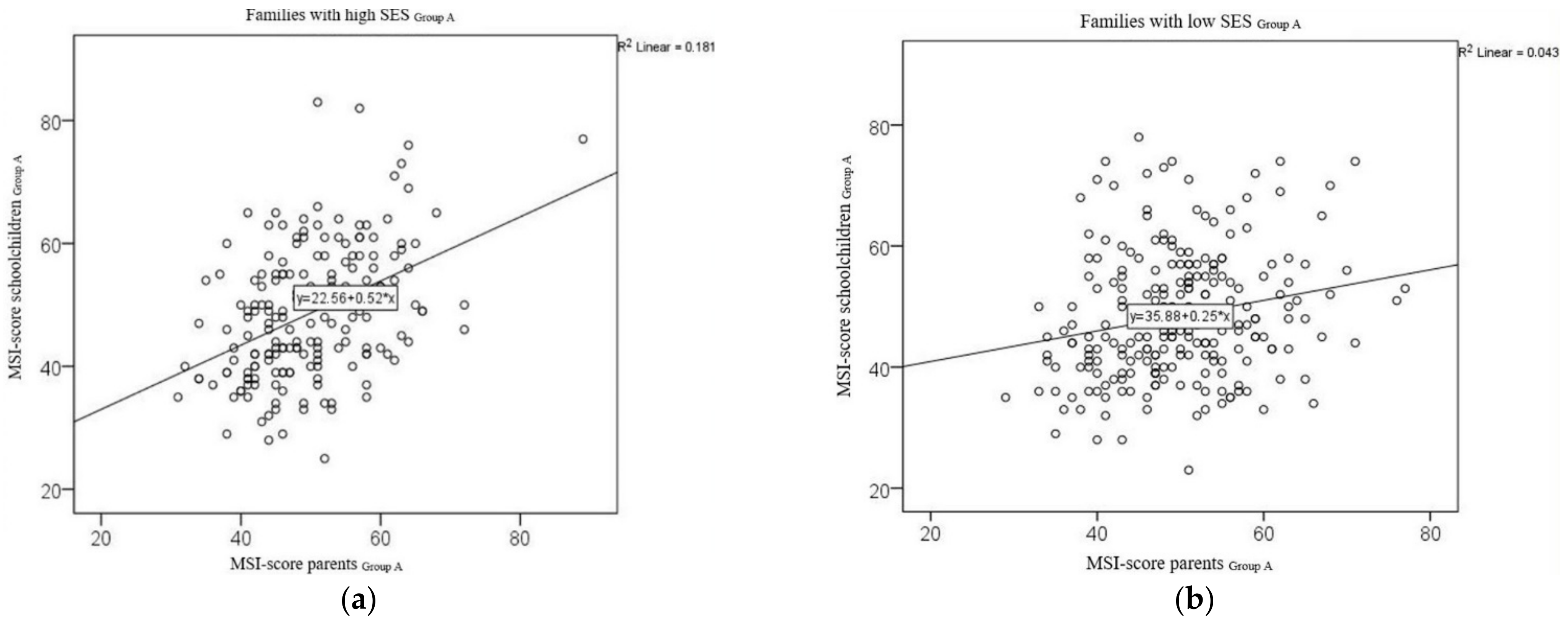
3.2. SES and Correlations between the MSI Values for Parent–Child Pairs
3.2.1. Group A
3.2.2. Group B
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia-Closas, R.; Garcia-Closas, M.; Serra-Majem, L. A cross-sectional study of dental caries, intake of confectionery and foods rich in starch and sugars, and salivary counts of Streptococcus mutans in children in Spain. Am. J. Clin. Nutr. 1997, 66, 1257–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, A.G.; Tsakos, G. The Joint ORCA-EADPH Symposium on Sugar: The Oral Health Perspective—A Commentary. Caries Res. 2019, 53, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Hancock, S.; Zinn, C.; Schofield, G. The consumption of processed sugar- and starch-containing foods, and dental caries: A systematic review. Eur. J. Oral Sci. 2020, 128, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; James, W.P. A new understanding of the relationship between sugars, dental caries and fluoride use: Implications for limits on sugars consumption. Public Health Nutr. 2014, 17, 2176–2184. [Google Scholar] [CrossRef] [Green Version]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Macigo, F.G.; James, R.M.; Ogunbodede, E.; Gathece, L.W. Sugar consumption and dental caries experience in Kenya. Int. Dent. J. 2016, 66, 158–162. [Google Scholar] [CrossRef]
- Ahovuo-Saloranta, A.; Forss, H.; Hiiri, A.; Nordblad, A.; Makela, M. Pit and fissure sealants versus fluoride varnishes for preventing dental decay in the permanent teeth of children and adolescents. Cochrane Database Syst. Rev. 2016, 1, CD003067. [Google Scholar] [CrossRef]
- Pieper, K.; Winter, J.; Heinzel-Gutenbrunner, M.; Margraf-Stiksrud, J. Association between a New Sugar Index and Caries Experience: Results of a Cross-Sectional Field Study. Caries Res. 2019, 53, 160–167. [Google Scholar] [CrossRef]
- König, K.G.; Navia, J.M. Nutritional role of sugars in oral health. Am. J. Clin. Nutr. 1995, 62, 275S–282S; discussion 282S–283S. [Google Scholar] [CrossRef] [Green Version]
- König, K.G. Diet and oral health. Int. Dent. J. 2000, 50, 162–174. [Google Scholar] [CrossRef]
- Kleemola-Kujala, E.; Rasanen, L. Relationship of oral hygiene and sugar consumption to risk of caries in children. Community Dent. Oral Epidemiol. 1982, 10, 224–233. [Google Scholar] [CrossRef]
- Ismail, A.I.; Tanzer, J.M.; Dingle, J.L. Current trends of sugar consumption in developing societies. Community Dent. Oral Epidemiol. 1997, 25, 438–443. [Google Scholar] [CrossRef]
- Llena, C.; Forner, L. Dietary habits in a child population in relation to caries experience. Caries Res. 2008, 42, 387–393. [Google Scholar] [CrossRef]
- Della Corte, K.; Fife, J.; Gardner, A.; Murphy, B.L.; Kleis, L.; Della Corte, D.; Schwingshackl, L.; LeCheminant, J.D.; Buyken, A.E. World trends in sugar-sweetened beverage and dietary sugar intakes in children and adolescents: A systematic review. Nutr. Rev. 2021, 79, 274–288. [Google Scholar] [CrossRef]
- Meier, T.; Deumelandt, P.; Christen, O.; Stangl, G.I.; Riedel, K.; Langer, M. Global Burden of Sugar-Related Dental Diseases in 168 Countries and Corresponding Health Care Costs. J. Dent. Res. 2017, 96, 845–854. [Google Scholar] [CrossRef]
- Al Rawahi, S.H.; Asimakopoulou, K.; Newton, J.T. Theory based interventions for caries related sugar intake in adults: Systematic review. BMC Psychol. 2017, 5, 25. [Google Scholar] [CrossRef] [Green Version]
- Chi, D.L.; Hopkins, S.; O’Brien, D.; Mancl, L.; Orr, E.; Lenaker, D. Association between added sugar intake and dental caries in Yup’ik children using a novel hair biomarker. BMC Oral Health 2015, 15, 121. [Google Scholar] [CrossRef]
- Hinnig Pde, F.; Mariath, A.B.; Freaza, S.R.; Gambardella, A.M.; Bergamaschi, D.P. Development of a food frequency questionnaire for children from 7 to 10 years old. Rev. Bras. Epidemiol. 2014, 17, 479–494. [Google Scholar] [CrossRef]
- Kobayashi, T.; Tanaka, S.; Toji, C.; Shinohara, H.; Kamimura, M.; Okamoto, N.; Imai, S.; Fukui, M.; Date, C. Development of a food frequency questionnaire to estimate habitual dietary intake in Japanese children. Nutr. J. 2010, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Neelakantan, N.; Whitton, C.; Seah, S.; Koh, H.; Rebello, S.A.; Lim, J.Y.; Chen, S.; Chan, M.F.; Chew, L.; van Dam, R.M. Development of a Semi-Quantitative Food Frequency Questionnaire to Assess the Dietary Intake of a Multi-Ethnic Urban Asian Population. Nutrients 2016, 8, 528. [Google Scholar] [CrossRef]
- Bertoli, S.; Petroni, M.L.; Pagliato, E.; Mora, S.; Weber, G.; Chiumello, G.; Testolin, G. Validation of food frequency questionnaire for assessing dietary macronutrients and calcium intake in Italian children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 555–560. [Google Scholar] [CrossRef]
- Winter, J.; Jablonski-Momeni, A.; Ladda, A.; Pieper, K. Long-term effect of intensive prevention on dental health of primary school children by socioeconomic status. Clin. Oral. Investig. 2018, 22, 2241–2249. [Google Scholar] [CrossRef]
- Pitts, N. “ICDAS”—An international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent. Health 2004, 21, 193–198. [Google Scholar]
- Pieper, K.; Dressler, S.; Heinzel-Gutenbrunner, M.; Neuhäuser, A.; Krecker, M.; Wunderlich, K.; Jablonski-Momeni, A. The influence of social status on pre-school children’s eating habits, caries experience and caries prevention behavior. Int. J. Public Health 2012, 57, 207–215. [Google Scholar] [CrossRef]
- Kiwanuka, S.N.; Astrom, A.N.; Trovik, T.A. Sugar snack consumption in Ugandan schoolchildren: Validity and reliability of a food frequency questionnaire. Community Dent. Oral Epidemiol. 2006, 34, 372–380. [Google Scholar] [CrossRef]
- Livingstone, M.B.; Robson, P.J. Measurement of dietary intake in children. Proc. Nutr. Soc. 2000, 59, 279–293. [Google Scholar] [CrossRef] [Green Version]
- Bundegesundheitsministerium. Mitglieder und Versicherte der Gesetzlichen Krankenversicherung (GKV). Available online: https://www.bundesgesundheitsministerium.de/themen/krankenversicherung/zahlen-und-fakten-zur-krankenversicherung/mitglieder-und-versicherte.html (accessed on 10 March 2022).
- Pieper, K.; Schulte, A.G. The decline in dental caries among 12-year-old children in Germany between 1994 and 2000. Community Dent. Health 2004, 21, 199–206. [Google Scholar] [PubMed]
- Bundesgesundheitsministerium. Bekanntmachung eines Beschlusses des Gemeinsamen Bundesausschusses über die Richtlinien des Bundesausschusses der Zahnärzte und Krankenkassen über die Früherkennungsuntersuchungen auf Zahn-, Mund- und Kieferkrankheiten (zahnärztliche Früherkennung gemäß § 26 Absatz 1 Satz 2 des Fünften Buches Sozialgesetzbuch–SGB V)–Neufassung–vom: 17.01.2019, BAnz AT 28.05.2019 B2. Available online: https://www.bundesanzeiger.de/pub/de/amtliche-veroeffentlichung?13 (accessed on 11 April 2022).
- Gemeinsamer Bundesausschuss. Richtlinien Individualprophylaxe—Richtlinien des Bundesausschusses der Zahnärzte und Krankenkassen über Maßnahmen zur Verhütung von Zahnerkrankungen (Individualprophylaxe). Available online: https://www.g-ba.de/downloads/62-492-10/2003-06-04_IP-RL.pdf (accessed on 11 March 2022).
- Hong, J.; Whelton, H.; Douglas, G.; Kang, J. Consumption frequency of added sugars and UK children’s dental caries. Community Dent. Oral Epidemiol. 2018, 46, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, M.; Patel, D.K.; Vyas, A.; Khan, A.J.; McGrady, M.G.; Boothman, N.; Pretty, I.A. Sugar before bed: A simple dietary risk factor for caries experience. Community Dent. Health 2017, 34, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Johansson, I.; Holgerson, P.L.; Kressin, N.R.; Nunn, M.E.; Tanner, A.C. Snacking habits and caries in young children. Caries Res. 2010, 44, 421–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramini, P.; Molinari, N.; Tentscher, M.; Demattei, C.; Schulte, A.G. Association between caries experience and body mass index in 12-year-old French children. Caries Res. 2009, 43, 468–473. [Google Scholar] [CrossRef]
- Maliderou, M.; Reeves, S.; Noble, C. The effect of social demographic factors, snack consumption and vending machine use on oral health of children living in London. Br. Dent. J. 2006, 201, 441–444; discussion 437; quiz 466. [Google Scholar] [CrossRef]
- Okullo, I.; Astrom, A.N.; Haugejorden, O.; Rwenyonyi, C.M. Variation in caries experience and sugar intake among secondary school students in urban and rural Uganda. Acta Odontol. Scand. 2003, 61, 197–202. [Google Scholar] [CrossRef]
- Gordon, Y.; Reddy, J. Prevalence of dental caries, patterns of sugar consumption and oral hygiene practices in infancy in S. Africa. Community Dent. Oral Epidemiol. 1985, 13, 310–314. [Google Scholar] [CrossRef]
- Eronat, N.; Koparal, E. Dental caries prevalence, dietary habits, tooth-brushing, and mother’s education in 500 urban Turkish children. J. Marmara Univ. Dent. Fac. 1997, 2, 599–604. [Google Scholar]
- Robert Koch Institut. Inanspruchnahme von Früherkennungsuntersuchungen. Faktenblatt zu KiGGS Welle 1: Studie zur Gesundheit von Kindern und Jugendlichen in Deutschland—Erste Folgebefragung 2009–2012; RKI: Berlin, Germany, 2015. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Age Distribution | Total | |||||
|---|---|---|---|---|---|---|---|
| Boys | Girls | 8 yrs | 9 yrs | 10 yrs | 11 yrs | ||
| Group A | |||||||
| n | 216 | 213 | 28 | 307 | 91 | 3 | 429 |
| 50.3% | 49.7% | 6.5% | 71.6% | 21.2% | 0.7% | 100% | |
| Group B | |||||||
| n | 187 | 213 | 26 | 281 | 85 | 8 | 400 |
| 46.8% | 53.2% | 6.6% | 70.3% | 21.3% | 2.0% | 100% | |
| Children | Parents | |
|---|---|---|
| n | 429 | 429 |
| MSI score (mean) | 48.6 | 49.8 |
| MSI score (min) | 23 | 29 |
| Median | 48 | 49 |
| MSI score (max) | 83.0 | 89.0 |
| ±SD | 10.4 | 8.6 |
| Number of Omitted Items | Children (%) | Parents (%) |
|---|---|---|
| 0–1 | 70.0 | 80.8 |
| 2 | 13.5 | 7.5 |
| 3 | 5.5 | 2.3 |
| 4–5 | 5.3 | 5.0 |
| 6 and more | 5.7 | 4.5 |
| d1–6fs | d3–6fs | |||
|---|---|---|---|---|
| MSI Score (Children) | MSI Score (Parents) | MSI Score (Children) | MSI Score (Parents) | |
| n | 429 | 429 | 429 | 429 |
| Spearman’s Rho | 0.107 | 0.111 | 0.053 | 0.111 |
| p-value | 0.026 * | 0.021 * | 0.275 | 0.022 * |
| Total | Low SES | High SES | |
|---|---|---|---|
| Group A | |||
| n | 429 | 230 | 188 |
| r-value | 0.301 | 0.206 | 0.425 |
| p-value | <0.001 * | 0.002 * | <0.001 * |
| Group B | |||
| n | 400 | 212 | 172 |
| r-value | 0.226 | 0.212 | 0.225 |
| p-value | <0.001 * | 0.002 * | 0.003 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmidt, P.; Schulte, A.G.; Margraf-Stiksrud, J.; Heinzel-Gutenbrunner, M.; Pieper, K. Children’s and Parents’ Marburg Sugar Index (MSI) Values: Are They Comparable? Nutrients 2022, 14, 1630. https://doi.org/10.3390/nu14081630
Schmidt P, Schulte AG, Margraf-Stiksrud J, Heinzel-Gutenbrunner M, Pieper K. Children’s and Parents’ Marburg Sugar Index (MSI) Values: Are They Comparable? Nutrients. 2022; 14(8):1630. https://doi.org/10.3390/nu14081630
Chicago/Turabian StyleSchmidt, Peter, Andreas G. Schulte, Jutta Margraf-Stiksrud, Monika Heinzel-Gutenbrunner, and Klaus Pieper. 2022. "Children’s and Parents’ Marburg Sugar Index (MSI) Values: Are They Comparable?" Nutrients 14, no. 8: 1630. https://doi.org/10.3390/nu14081630
APA StyleSchmidt, P., Schulte, A. G., Margraf-Stiksrud, J., Heinzel-Gutenbrunner, M., & Pieper, K. (2022). Children’s and Parents’ Marburg Sugar Index (MSI) Values: Are They Comparable? Nutrients, 14(8), 1630. https://doi.org/10.3390/nu14081630