
Impact of Cafeteria Service Discontinuation at a Dialysis Facility on Medium-Term Nutritional Status of Elderly Patients Undergoing Hemodialysis

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
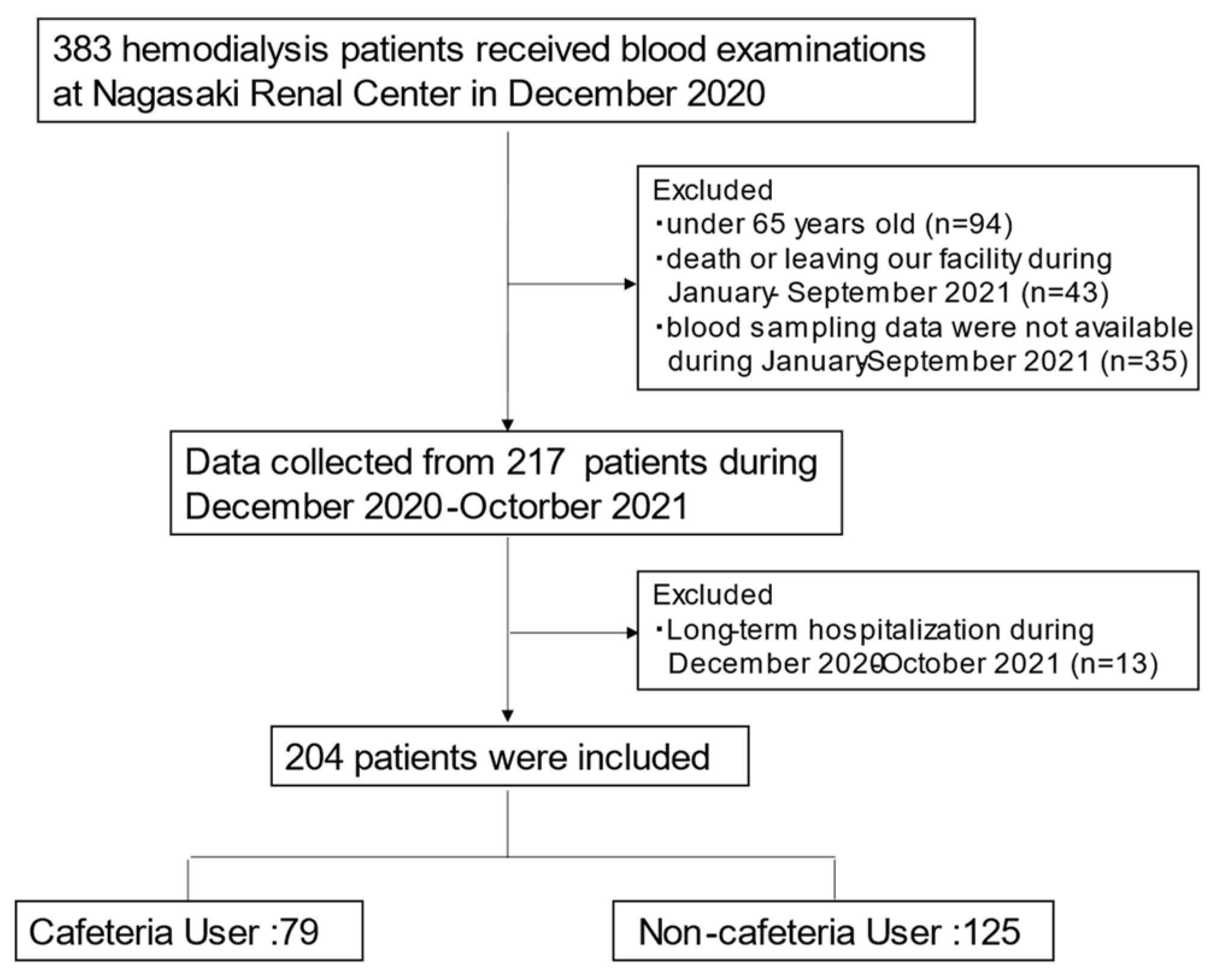
2.1. Patient Background
2.2. Data Collection
2.3. Statistical Analyses
3. Results
3.1. Patient Background
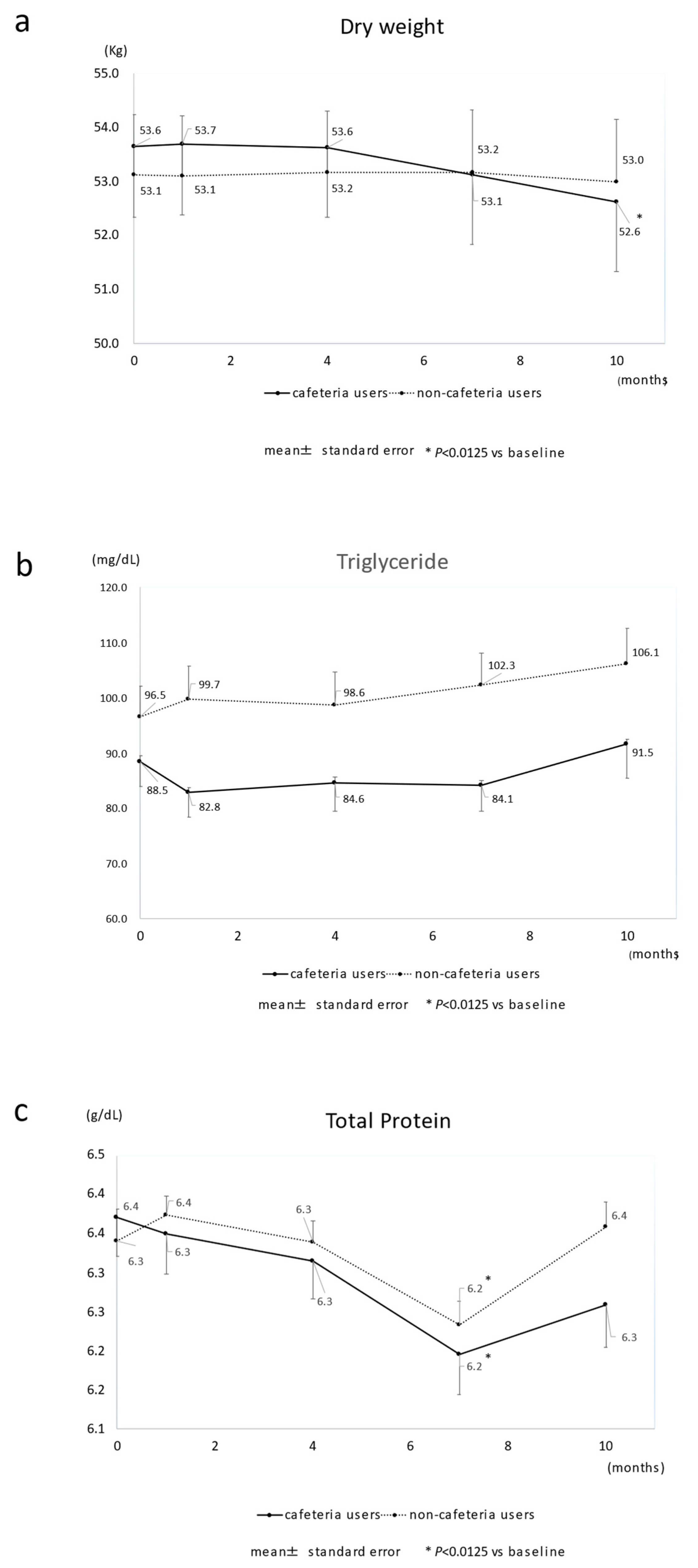
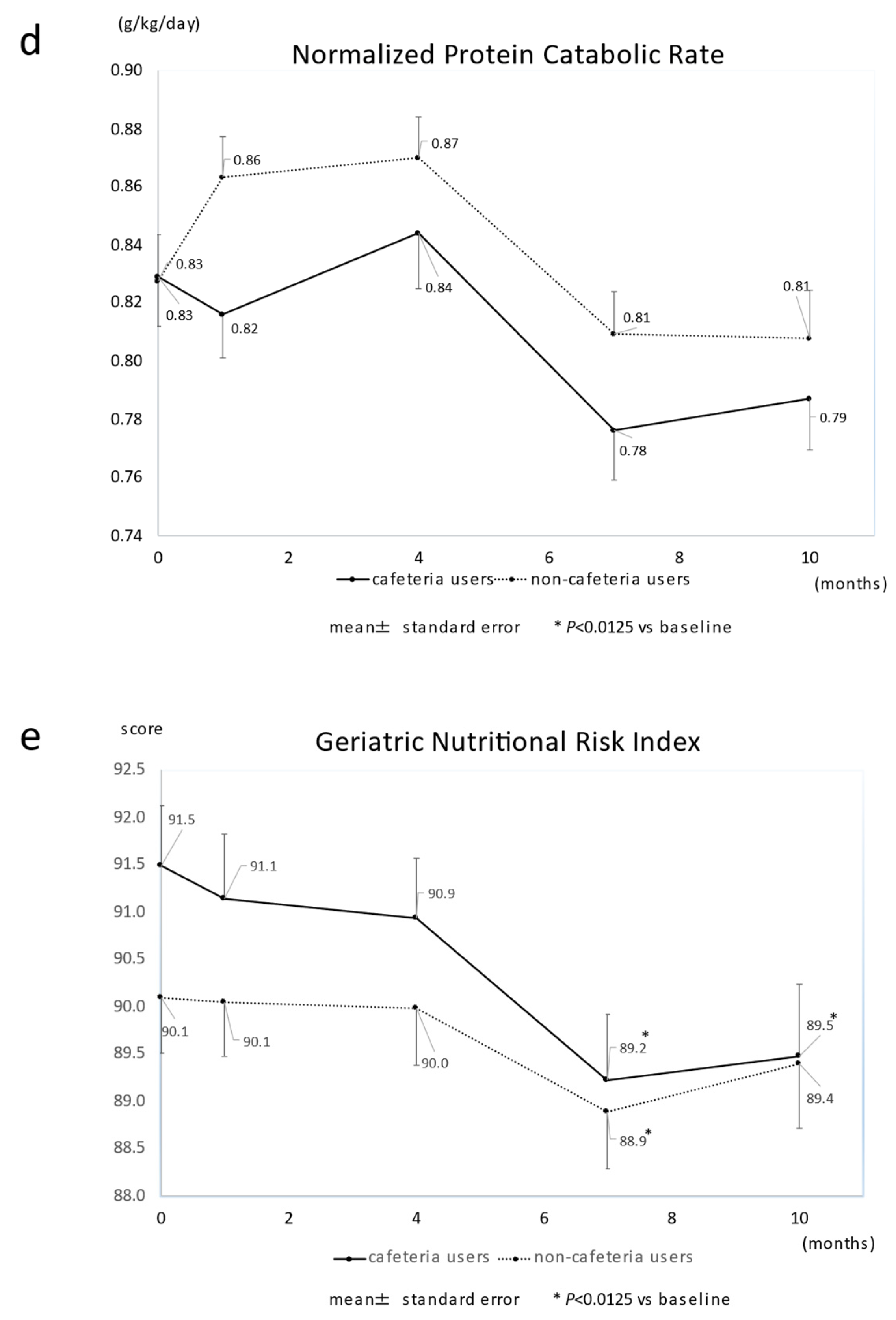
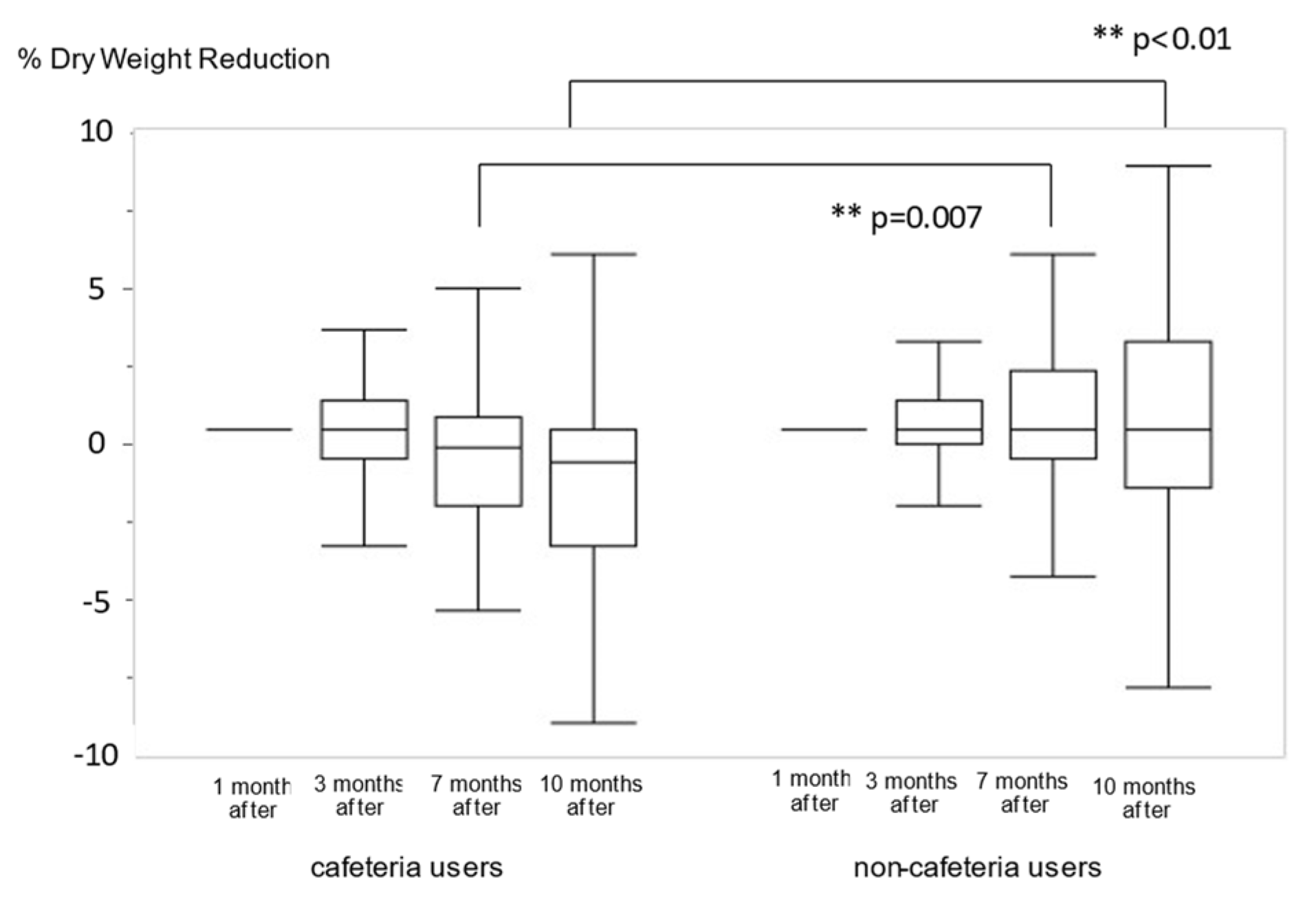
3.2. Dry-Weight Reduction and Changes in Parameters by Use of Cafeteria Services
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- López-Moreno, M.; López, M.T.I.; Miguel, M.; Garcés-Rimón, M. Physical and Psychological Effects Related to Food Habits and Lifestyle Changes Derived from COVID-19 Home Confinement in the Spanish Population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef] [PubMed]
- Cancello, R.; Soranna, D.; Zambra, G.; Zambon, A.; Invitti, C. Determinants of the Lifestyle Changes during COVID-19 Pandemic in the Residents of Northern Italy. Int. J. Environ. Res. Public Health 2020, 17, 6287. [Google Scholar] [CrossRef] [PubMed]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Schaap, L.A.; Wijnhoven, H.A.H. Self-Reported Impact of the COVID-19 Pandemic on Nutrition and Physical Activity Behaviour in Dutch Older Adults Living Independently. Nutrients 2020, 12, 3708. [Google Scholar] [CrossRef]
- Jayaweera, M.; Perera, H.; Gunawardana, B.; Manatunge, J. Transmission of COVID-19 Virus by Droplets and Aerosols: A Critical Review on the Unresolved Dichotomy. Environ. Res. 2020, 188, 109819. [Google Scholar] [CrossRef]
- Henry, B.M.; Lippi, G. Chronic Kidney Disease Is Associated with Severe Coronavirus disease 2019 (COVID-19) Infection. Int. Urol. Nephrol. 2020, 52, 1193–1194. [Google Scholar] [CrossRef] [Green Version]
- Kutner, N.G.; Zhang, R.; Allman, R.M.; Bowling, C.B. Correlates of ADL Difficulty in a Large Hemodialysis Cohort. Hemodial. Int. 2014, 18, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Charra, B.; Laurent, G.; Chazot, C.; Calemard, E.; Terrat, J.C.; Vanel, T.; Jean, G.; Ruffet, M. Clinical Assessment of Dry Weight. Nephrol. Dial. Transplant. 1996, 11, 16–19. [Google Scholar] [CrossRef] [Green Version]
- Villain, C.; Ecochard, R.; Genet, L.; Jean, G.; Kuentz, F.; Lataillade, D.; Legrand, E.; Moreau-Gaudry, X.; Fouque, D. Impact of BMI Variations on Survival in Older adult Hemodialysis Patients. J. Ren. Nutr. 2015, 25, 488–493. [Google Scholar] [CrossRef]
- Kuwahara, K.; Kuroda, A.; Fukuda, Y. COVID-19: Active Measures to Support Community-Dwelling Older Adults. Travel Med. Infect. Dis. 2020, 36, 101638. [Google Scholar] [CrossRef]
- Smith, M.L.; Steinman, L.E.; Casey, E.A. Combatting Social Isolation among Older Adults in a Time of Physical Distancing: The COVID-19 Social Connectivity Paradox. Front. Public Health 2020, 8, 403. [Google Scholar] [CrossRef] [PubMed]
- Azzolino, D.; Saporiti, E.; Proietti, M.; Cesari, M. Nutritional Considerations in Frail Older Patients with COVID-19. J. Nutr. Health Aging. 2020, 24, 696–698. [Google Scholar] [CrossRef] [PubMed]
- Steinman, M.A.; Perry, L.; Perissinotto, C.M. Meeting the Care Needs of Older Adults Isolated at Home during the COVID-19 Pandemic. JAMA Intern. Med. 2020, 180, 819–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danilovich, M.K.; Norrick, C.R.; Hill, K.C.; Conroy, D.E. Nursing Home Resident Weight Loss during Coronavirus Disease 2019 Restrictions. J. Am. Med. Dir. Assoc. 2020, 21, 1568–1569. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.; Cuppari, L.; Campbell, K.L.; Avesani, C.M. Nutritional Assessment of Older adult Patients on Dialysis: Pitfalls and Potentials for Practice. Nephrol. Dial. Transplant. 2017, 32, 1780–1789. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, K.; Kitamura, M.; Takazono, T.; Sato, S.; Yamamoto, K.; Notomi, S.; Sawase, K.; Harada, T.; Funakoshi, S.; Mukae, H.; et al. Association between the Psoas Muscle Index and Hospitalization for Pneumonia in Patients Undergoing Hemodialysis. BMC Nephrol. 2021, 22, 394. [Google Scholar] [CrossRef]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified Nutritional Screening Tools for Patients on Maintenance Hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Sahathevan, S.; Khor, B.H.; Ng, H.M.; Gafor, A.H.A.; Mat Daud, Z.A.; Mafra, D.; Karupaiah, T. Understanding Development of Malnutrition in Hemodialysis Patients: A Narrative Review. Nutrients 2020, 12, 3147. [Google Scholar] [CrossRef]
- Carrero, J.J.; Thomas, F.; Nagy, K.; Arogundade, F.; Avesani, C.M.; Chan, M.; Chmielewski, M.; Cordeiro, A.C.; Espinosa-Cuevas, A.; Fiaccadori, E.; et al. Global Prevalence of Protein-Energy Wasting in Kidney Disease: A Meta-Analysis of Contemporary Observational Studies from the International Society of Renal Nutrition and Metabolism. J. Ren. Nutr. 2018, 28, 380–392. [Google Scholar] [CrossRef]
- Takahashi, H.; Inoue, K.; Shimizu, K.; Hiraga, K.; Takahashi, E.; Otaki, K.; Yoshikawa, T.; Furuta, K.; Tokunaga, C.; Sakakibara, T.; et al. Comparison of Nutritional Risk Scores for Predicting Mortality in Japanese Chronic Hemodialysis Patients. J. Ren. Nutr. 2017, 27, 201–206. [Google Scholar] [CrossRef]
- Kitamura, M.; Takazono, T.; Yamaguchi, K.; Notomi, S.; Sawase, K.; Harada, T.; Funakoshi, S.; Mukae, H.; Nishino, T. The Impact of Muscle Mass Loss and Deteriorating Physical Function on Prognosis in Patients Receiving Hemodialysis. Sci. Rep. 2021, 11, 22290. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Enoki, Y.; Maruyama, T. Sarcopenia in Chronic Kidney Disease: Factors, Mechanisms, and Therapeutic Interventions. Biol. Pharm. Bull. 2019, 42, 1437–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hara, H.; Nakamura, Y.; Hatano, M.; Iwashita, T.; Shimizu, T.; Ogawa, T.; Kanozawa, K.; Hasegawa, H. Protein Energy Wasting and Sarcopenia in Dialysis Patients. Contrib. Nephrol. 2018, 196, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A Proposed Nomenclature and Diagnostic Criteria for Protein-Energy Wasting in Acute and Chronic Kidney Disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, K.; Mullan, J.; Mansfield, K. An Integrative Review of the Methodology and Findings regarding Dietary Adherence in End Stage Kidney Disease. BMC Nephrol. 2017, 18, 318. [Google Scholar] [CrossRef] [Green Version]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Sepúlveda-Loyola, W.S.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef]
- Xue, Q.L.; Bandeen-Roche, K.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial Manifestations of Frailty Criteria and the Development of Frailty Phenotype in the Women’s Health and Aging Study II. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 984–990. [Google Scholar] [CrossRef] [Green Version]
- Besora-Moreno, M.; Llauradó, E.; Tarro, L.; Solà, R. Social and Economic Factors and Malnutrition or the Risk of Malnutrition in the Older Adult: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2020, 12, 737. [Google Scholar] [CrossRef] [Green Version]
- Carrero, J.J.; Stenvinkel, P.; Cuppari, L.; Ikizler, T.A.; Kalantar-Zadeh, K.; Kaysen, G.; Mitch, W.E.; Price, S.R.; Wanner, C.; Wang, A.Y.; et al. Etiology of the Protein-Energy Wasting Syndrome in Chronic Kidney Disease: A Consensus Statement from the International Society of Renal Nutrition and Metabolism (ISRNM). J. Ren. Nutr. 2013, 23, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Stenvinkel, P.; Lindholm, B.; Heimbürger, O. Poor nutritional status and inflammation: Novel Approaches in an Integrated Therapy of Inflammatory-Associated Wasting in End-Stage Renal Disease. Semin. Dial. 2004, 17, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Block, G.; McAllister, C.J.; Humphreys, M.H.; Kopple, J.D. Appetite and Inflammation, Nutrition, Anemia, and Clinical Outcome in Hemodialysis Patients. Am. J. Clin. Nutr. 2004, 80, 299–307. [Google Scholar] [CrossRef]
- Stenvinkel, P. Inflammation in End-Stage Renal Disease--a Fire That Burns Within. Contrib. Nephrol. 2005, 149, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Bergström, J. Nutrition and Mortality in Hemodialysis. J. Am. Soc. Nephrol. 1995, 6, 1329–1341. [Google Scholar] [CrossRef] [PubMed]
- Ohnaka, S.; Yamada, S.; Tsujikawa, H.; Arase, H.; Taniguchi, M.; Tokumoto, M.; Tsuruya, K.; Nakano, T.; Kitazono, T. Association of Normalized Protein Catabolic Rate (nPCR) with the Risk of Bone Fracture in Patients Undergoing Maintenance Hemodialysis: The Q-Cohort Study. Clin. Nutr. 2021, 40, 997–1004. [Google Scholar] [CrossRef]
- Morley, J.E. Undernutrition in Older Adults. Fam. Pract. 2012, 29, i89–i93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, K. Maintenance of Skeletal Muscle to Counteract Sarcopenia in Patients with Advanced Chronic Kidney Disease and Especially Those Undergoing Hemodialysis. Nutrients 2021, 13, 1538. [Google Scholar] [CrossRef]
- Hendriks, F.K.; Smeets, J.S.J.; Broers, N.J.H.; van Kranenburg, J.M.X.; van der Sande, F.M.; Kooman, J.P.; van Loon, L.J.C. End-Stage Renal Disease Patients Lose a Substantial Amount of Amino Acids during Hemodialysis. J. Nutr. 2020, 150, 1160–1166. [Google Scholar] [CrossRef]
- Johansen, K.L.; Shubert, T.; Doyle, J.; Soher, B.; Sakkas, G.K.; Kent-Braun, J.A. Muscle Atrophy in Patients Receiving Hemodialysis: Effects on Muscle Strength, Muscle Quality, and Physical Function. Kidney Int. 2003, 63, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Walston, J.; Buta, B.; Xue, Q.L. Frailty Screening and Interventions: Considerations for Clinical Practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cafeteria Users (n = 79) | Non-Cafeteria Users (n = 125) | p Value | |
|---|---|---|---|
| Age (years) | 73.0 (68.0–80.0) | 72.0 (69.0–80.5) | 0.70 |
| Male (%) | 46 (58.2) | 65 (52.0) | 0.38 |
| Dialysis vintage (month) | 66 (28–102) | 51 (22–120) | 0.43 |
| Dialysis time (hour) | 4.0 (3.5–4.0) | 4.0 (3.5–4.0) | 0.35 |
| DM history (%) | 16 (20.3) | 36 (28.8) | 0.19 |
| Dementia (%) | 6 (7.6) | 18 (14.4) | 0.18 |
| Living alone (%) | 18 (22.8) | 20 (16.0) | 0.27 |
| Nursing-home residents (%) | 1 (1.3) | 18 (14.4) | 0.0018 |
| Dry weight (kg) | 53.0 (44.0–61.0) | 53.2 (42.8–61.0) | 0.76 |
| Body mass index (kg/m2) | 21.1 (18.1–23.8) | 20.7 (18.8–22.6) | 0.82 |
| ChE (U/L) | 192 (167–223) | 210 (165–239) | 0.23 |
| TP (g/dL) | 6.4 (6.1–6.7) | 6.4 (6.1–6.6) | 0.78 |
| AST (U/L) | 15 (11–18) | 14 (11–16) | 0.15 |
| ALT (U/L) | 10 (7–13) | 9 (6–12) | 0.29 |
| CK (U/L) | 71 (47–93) | 60 (39–85) | 0.07 |
| TC (mg/dL) | 149 (127–180) | 150 (126–176) | 0.93 |
| TG (mg/dL) | 84 (55–116) | 85 (56–111) | 0.89 |
| cCa (mg/dL) | 8.7 (8.3–9.0) | 8.5 (8.1–8.8) | 0.0075 |
| UA (mg/dL) | 6.6 (5.6–7.5) | 6.9 (6.1–7.9) | 0.07 |
| BUN (mg/dL) | 57.8 (48.8–67.4) | 60.5 (51.8–70.3) | 0.14 |
| Cr (mg/dL) | 9.26 (7.92–10.45) | 8.97 (7.26–10.57) | 0.28 |
| K (mEq/L) | 4.7 (4.2–5.1) | 4.7 (4.1–5.2) | 0.95 |
| P (mg/dL) | 5.1 (4.5–6.0) | 5.3 (4.5–6.1) | 0.46 |
| CRP (mg/dL) | 0.16 (0.08–0.61) | 0.2 (0.08–0.49) | 0.87 |
| Hb (g/dL) | 11.0 (10.2–11.8) | 10.7 (10.0–11.5) | 0.19 |
| Ht (%) | 34.5 (31.1–36.0) | 33.2 (31.1–35.4) | 0.16 |
| Alb (g/dL) | 3.6 (3.4–3.7) | 3.5 (3.3–3.8) | 0.10 |
| GNRI | 91.3 (88.2–95.7) | 90.8 (85.3–95.0) | 0.24 |
| nPCR (g/kg/day) | 0.80 (0.72–0.92) | 0.82 (0.69–0.94) | 0.77 |
| Intact PTH (pg/mL) | 93 (28–143) | 72 (37–134) | 0.83 |
| KT/V | 1.6 (1.3–1.9) | 1.5 (1.2–1.8) | 0.06 |
| Univariate | Multivariable | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age per 1 year old | 1.08 | 1.04–1.13 | <0.001 | 1.07 | 1.01–1.19 | 0.009 |
| Male vs. Female | 1.01 | 0.58–1.76 | 0.97 | |||
| Dialysis vintage per 1 month | 0.99 | 0.96–1.03 | 0.74 | |||
| Dialysis time per 1 hr | 0.50 | 0.28–0.86 | 0.01 | 0.69 | 0.37–1.29 | 0.23 |
| DM history | 1.64 | 0.86–3.10 | 0.15 | |||
| Dementia | 1.13 | 0.48–2.70 | 0.78 | |||
| Cafeteria users | 2.62 | 1.47–4.74 | 0.001 | 3.23 | 1.66–6.28 | <0.001 |
| Living Alone | 1.22 | 0.60–2.50 | 0.57 | |||
| Nursing-home residents | 0.50 | 0.17–1.34 | 0.17 | |||
| Dry weight per 1 kg (kg) | 0.98 | 0.95–1.00 | 0.06 | |||
| Body mass index per 1 kg/m2 | 0.92 | 0.85–0.99 | 0.037 | 0.96 | 0.88–1.06 | 0.44 |
| ChE per 1 unit U/L | 0.94 | 0.89–0.99 | 0.016 | 0.99 | 0.93–1.05 | 0.65 |
| TP per 1 g/dL | 1.23 | 0.66–2.48 | 0.47 | |||
| AST per 1 U/L | 1.00 | 0.97–1.04 | 0.88 | |||
| ALT per 1 U/L | 0.99 | 0.95–1.02 | 0.54 | |||
| TC per 1 mg dL | 1.00 | 0.99–1.01 | 0.60 | |||
| TG per 1 mg/dL | 0.95 | 0.90–1.00 | 0.08 | |||
| cCa per 1 mg/dL | 1.03 | 0.61–1.75 | 0.91 | |||
| UA per 1 mg/dL | 0.88 | 0.73–1.06 | 0.18 | |||
| BUN per 1 mg/dL | 0.72 | 0.56–0.89 | 0.002 | 0.77 | 0.60–0.98 | 0.028 |
| Cr per 1 mg/dL | 0.82 | 0.72–0.93 | 0.002 | 0.93 | 0.79–1.10 | 0.41 |
| CRP per 1 mg/dL | 1.56 | 1.09–2.53 | 0.011 | 1.79 | 1.08–2.98 | 0.005 |
| Hb per 1 g/dL | 0.92 | 0.71–1.20 | 0.55 | |||
| Alb per 1 g/dL | 0.49 | 0.18–1.24 | 0.13 | |||
| KT/V per 1 Unit | 0.54 | 0.57–1.00 | 0.053 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Notomi, S.; Kitamura, M.; Yamaguchi, K.; Harada, T.; Nishino, T.; Funakoshi, S.; Kuno, K. Impact of Cafeteria Service Discontinuation at a Dialysis Facility on Medium-Term Nutritional Status of Elderly Patients Undergoing Hemodialysis. Nutrients 2022, 14, 1628. https://doi.org/10.3390/nu14081628
Notomi S, Kitamura M, Yamaguchi K, Harada T, Nishino T, Funakoshi S, Kuno K. Impact of Cafeteria Service Discontinuation at a Dialysis Facility on Medium-Term Nutritional Status of Elderly Patients Undergoing Hemodialysis. Nutrients. 2022; 14(8):1628. https://doi.org/10.3390/nu14081628
Chicago/Turabian StyleNotomi, Satoko, Mineaki Kitamura, Kosei Yamaguchi, Takashi Harada, Tomoya Nishino, Satoshi Funakoshi, and Kazue Kuno. 2022. "Impact of Cafeteria Service Discontinuation at a Dialysis Facility on Medium-Term Nutritional Status of Elderly Patients Undergoing Hemodialysis" Nutrients 14, no. 8: 1628. https://doi.org/10.3390/nu14081628
APA StyleNotomi, S., Kitamura, M., Yamaguchi, K., Harada, T., Nishino, T., Funakoshi, S., & Kuno, K. (2022). Impact of Cafeteria Service Discontinuation at a Dialysis Facility on Medium-Term Nutritional Status of Elderly Patients Undergoing Hemodialysis. Nutrients, 14(8), 1628. https://doi.org/10.3390/nu14081628