
Nutrition Education Programs for Adults with Neurological Diseases Are Lacking: A Scoping Review




Abstract
:1. Introduction
2. Methods
2.1. Inclusion Criteria
2.1.1. Participants
2.1.2. Concept
2.1.3. Context
2.1.4. Types of Studies
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
3. Results
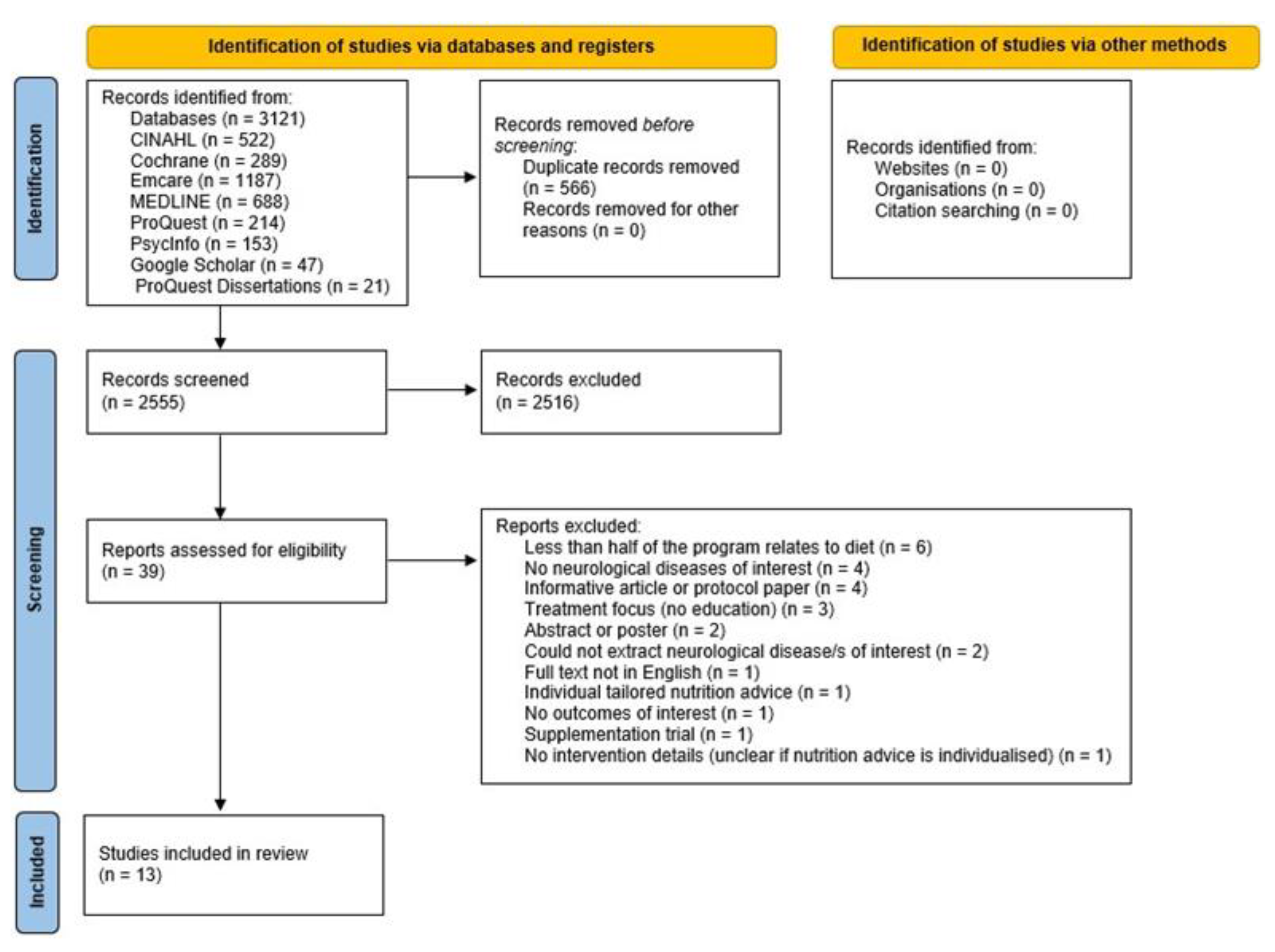
3.1. Search Results
3.2. Study Details
3.3. Target Populations
3.4. Characteristics of the Nutrition Education Programs
3.4.1. Nutrition Education Programs for People with Dementia
3.4.2. Nutrition Education Programs for People with Multiple Sclerosis
3.4.3. Nutrition Education Programs for Stroke Survivors
3.4.4. Nutrition Education Programs for People with Parkinson’s Disease
3.5. Theories and Behavior Change Techniques
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erkkinen, M.G.; Kim, M.-O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2018, 10, a033118. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Vos, T.; Nichols, E.; Owolabi, M.O.; Carroll, W.M.; Dichgans, M.; Deuschl, G.; Parmar, P.; Brainin, M.; Murray, C. The global burden of neurological disorders: Translating evidence into policy. Lancet Neurol. 2020, 19, 255–265. [Google Scholar] [CrossRef]
- Bertram, L.; Tanzi, R.E. The genetic epidemiology of neurodegenerative disease. J. Clin. Investig. 2005, 115, 1449–1457. [Google Scholar] [CrossRef] [Green Version]
- Selby, M. Neurological diseases. Pract. Nurse 2011, 41, 35–41. [Google Scholar]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. Dietary Guidelines for Americans, 2020–2025. Available online: https://www.dietaryguidelines.gov/resources/2020-2025-dietary-guidelines-online-materials (accessed on 3 February 2021).
- National Health and Medical Research Council. Australian Dietary Guidelines. Available online: https://www.nhmrc.gov.au/guidelines-publications/n55 (accessed on 3 February 2021).
- Huang, Y.-P.; Chen, L.-S.; Yen, M.-F.; Fann, C.-Y.; Chiu, Y.-H.; Chen, H.-H.; Pan, S.-L. Parkinson’s disease is related to an increased risk of ischemic stroke—A population-based propensity score-matched follow-up study. PLoS ONE 2013, 8, e68314. [Google Scholar] [CrossRef] [Green Version]
- Cragg, J.J.; Kramer, J.K.; Borisoff, J.F. Relationship between neurological disorders and heart disease: A national population health survey. Neuroepidemiology 2015, 44, 64–65. [Google Scholar] [CrossRef]
- Marrie, R.A.; Cohen, J.; Stuve, O.; Trojano, M.; Sørensen, P.S.; Reingold, S.; Cutter, G.; Reider, N. A systematic review of the incidence and prevalence of comorbidity in multiple sclerosis: Overview. Mult. Scler. J. 2015, 21, 263–281. [Google Scholar] [CrossRef]
- Marrie, R.A. Comorbidity in multiple sclerosis: Implications for patient care. Nat. Rev. Neurol. 2017, 13, 375–382. [Google Scholar] [CrossRef]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Australian Health Survey: Consumption of Food Groups from the Australian Dietary Guidelines, 2011–2012 (No. 4364.0.55.012). Available online: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4364.0.55.012main+features12011-12 (accessed on 17 July 2020).
- Yau, A.; Adams, J.; Monsivais, P. Time trends in adherence to UK dietary recommendations and associated sociodemographic inequalities, 1986-2012: A repeated cross-sectional analysis. Eur. J. Clin. Nutr. 2019, 73, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. NDNS: Results from Years 9 to 11 (Combined)—Statistical Summary. Available online: https://www.gov.uk/government/statistics/ndns-results-from-years-9-to-11-2016-to-2017-and-2018-to-2019/ndns-results-from-years-9-to-11-combined-statistical-summary (accessed on 9 June 2021).
- Rehm, C.D.; Peñalvo, J.L.; Afshin, A.; Mozaffarian, D. Dietary intake among US adults, 1999–2012. JAMA 2016, 315, 2542–2553. [Google Scholar] [CrossRef] [PubMed]
- Contento, I.; Balch, G.; Bronner, Y.; Maloney, S. The effectiveness of nutrition education and implications for nutrition education policy, programs, and research: A review of research. J. Nutr. Educ. 1995, 27, 275. [Google Scholar]
- World Health Organization. Global Action Plan for the Prevention and Control on Noncommunicable Diseases 2013–2020. Available online: https://www.who.int/nmh/events/ncd_action_plan/en/ (accessed on 20 May 2021).
- Atoloye, A.T.; Savoie-Roskos, M.R.; Guenther, P.M.; Durward, C.M. Effectiveness of Expanded Food and Nutrition Education Program in changing nutrition-related outcomes among adults with low income: A systematic review. J. Nutr. Educ. Behav. 2021, 53, 691–705. [Google Scholar] [CrossRef] [PubMed]
- Eyles, H.C.; Mhurchu, C.N. Does tailoring make a difference? A systematic review of the long-term effectiveness of tailored nutrition education for adults. Nutr. Rev. 2009, 67, 464–480. [Google Scholar] [CrossRef] [Green Version]
- Tay, B.S.J.; Cox, D.N.; Brinkworth, G.D.; Davis, A.; Edney, S.M.; Gwilt, I.; Ryan, J.C. Co-design practices in diet and nutrition research: An integrative review. Nutrients 2021, 13, 3593. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.; Auld, G.; Ammerman, A.; Lohse, B.; Serrano, E.; Wardlaw, M.K. Identification of a framework for best practices in nutrition education for low-income audiences. J. Nutr. Educ. Behav. 2020, 52, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Contento, I.R. Nutrition education: Linking research, theory, and practice. Asia Pac. J. Clin. Nutr. 2008, 17, 176–179. [Google Scholar] [PubMed]
- Murimi, M.W.; Kanyi, M.; Mupfudze, T.; Amin, M.R.; Mbogori, T.; Aldubayan, K. Factors influencing efficacy of nutrition education interventions: A systematic review. J. Nutr. Educ. Behav. 2017, 49, 142–165. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.; Cane, J.; Wood, C. The Behavior Change Technique Taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Sheals, K.; Godinho, C.A. Evaluating the effectiveness of behavior change techniques in health-related behavior: A scoping review of methods used. Transl. Behav. Med. 2018, 8, 212–224. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.D.; Black, L.J.; Begley, A. Dietary education programs for adults with neurological diseases: A scoping review protocol. JBI Evid. Synth. 2020, 19, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.; Godfrey, C.; McInerney, P.; Soares, C.B.; Khalil, H.; Parker, D. Chapter 11: Scoping Reviews. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and ExplanationThe PRISMA-ScR Statement. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.-S.; Kim, J.-Y. Effects of exercise and nutrition education programs on motor function and eating habit in mild dementia patients. J. Exerc. Rehabil. 2019, 15, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faxén-Irving, G.; Andrén-Olsson, B.; af Geijerstam, A.; Basun, H.; Cederholm, T. The effect of nutritional intervention in elderly subjects residing in group-living for the demented. Eur. J. Clin. Nutr. 2002, 56, 221–227. [Google Scholar] [CrossRef]
- Pivi, G.A.; da Silva, R.V.; Juliano, Y.; Novo, N.F.; Okamoto, I.H.; Brant, C.Q.; Bertolucci, P.H. A prospective study of nutrition education and oral nutritional supplementation in patients with Alzheimer’s disease. Nutr. J. 2011, 10, 98. [Google Scholar] [CrossRef] [Green Version]
- Rivière, S.; Gillette-Guyonnet, S.; Voisin, T.; Reynish, E.; Andrieu, S.; Lauque, S.; Salva, A.; Frisoni, G.; Nourhashemi, F.; Micas, M.; et al. A nutritional education program could prevent weight loss and slow cognitive decline in Alzheimer’s disease. J. Nutr. Health Aging 2001, 5, 295–299. [Google Scholar]
- Salva, A.; Andrieu, S.; Fernandez, E.; Schiffrin, E.J.; Moulin, J.; Decarli, B.; Rojano-i-Luque, X.; Guigoz, Y.; Vellas, B.; NutriAlz, G. Health and nutrition promotion program for patients with dementia (NutriAlz): Cluster randomized trial. J. Nutr. Health Aging 2011, 15, 822–830. [Google Scholar] [CrossRef]
- Hsiao, H.-T.; Chang, C.-C.; Chen, N.-C.; Chiu, H.-C.; Huang, C.-W.; Lee, F.-P.; Wang, J.-J. Effects of a dementia dietary educational program on nutritional knowledge and healthy eating behavior of family caregivers. Educ. Gerontol. 2020, 46, 270–283. [Google Scholar] [CrossRef]
- Doidge, M.J. Evaluation of a nutrition education programme for people with multiple sclerosis. J. Hum. Nutr. Diet. 1993, 6, 131–148. [Google Scholar] [CrossRef]
- Riemann-Lorenz, K.; Eilers, M.; von Geldern, G.; Schulz, K.-H.; Köpke, S.; Heesen, C. Dietary interventions in multiple sclerosis: Development and pilot-testing of an evidence based patient education program. PLoS ONE 2016, 11, e0165246. [Google Scholar] [CrossRef]
- Katz Sand, I.; Benn, E.K.T.; Fabian, M.; Fitzgerald, K.C.; Digga, E.; Deshpande, R.; Miller, A.; Gallo, S.; Arab, L. Randomized-controlled trial of a modified Mediterranean dietary program for multiple sclerosis: A pilot study. Mult. Scler. Relat. Disord. 2019, 36, 101403. [Google Scholar] [CrossRef] [PubMed]
- Wingo, B.C.; Rinker, J.R.; Goss, A.M.; Green, K.; Wicks, V.; Cutter, G.R.; Motl, R.W. Feasibility of improving dietary quality using a telehealth lifestyle intervention for adults with multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 46, 102504. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, J.H.; Braunschweig, C.; Silverman, K.; Riley, B.; Creviston, T.; Nicola, T. Effects of a short-term health promotion intervention for a predominantly African-American group of stroke survivors. Am. J. Prev. Med. 2000, 18, 332–338. [Google Scholar] [CrossRef]
- Towfighi, A.; Cheng, E.M.; Hill, V.A.; Barry, F.; Lee, M.; Valle, N.P.; Mittman, B.; Ayala-Rivera, M.; Moreno, L.; Espinosa, A.; et al. Results of a pilot trial of a lifestyle Intervention for stroke survivors: Healthy eating and lifestyle after stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105323. [Google Scholar] [CrossRef]
- Brenes, P. Virtual Nutrition Education for People Affected by Parkinson’s Disease. Ph.D. Thesis, Kansas State University, Manhattan, AP, USA, 2021. [Google Scholar]
- Roehl, K.; Sewak, S.L. Practice Paper of the Academy of Nutrition and Dietetics: Classic and modified ketogenic diets for treatment of epilepsy. J. Acad. Nutr. Diet. 2017, 117, 1279–1292. [Google Scholar] [CrossRef]
- Żukiewicz-Sobczak, W.; Król, R.; Wróblewska, P.; Piątek, J.; Gibas-Dorna, M. Huntington Disease—Principles and practice of nutritional management. Neurologia 2014, 48, 442–448. [Google Scholar] [CrossRef]
- Motor Neurone Disease Association. Eating and Drinking with Motor Neurone Disease (MND). Information, Tips, and Easy-Swallow Recipes. Available online: https://static.mndassociation.org/app/uploads/2017/05/19135151/Eating-and-drinking-with-MND-final-web-PDF-2017.pdf (accessed on 15 May 2020).
- Parkinson’s Foundation. Diet & Nutrition. Available online: https://www.parkinson.org/Living-with-Parkinsons/Managing-Parkinsons/Diet-and-Nutrition (accessed on 15 May 2020).
- Salvioni, C.C.S.; Stanich, P.; Almeida, C.S.; Oliveira, A.S.B. Nutritional care in motor neurone disease/ amyotrophic lateral sclerosis. Arq. Neuro-Psiquiatr. 2014, 72, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Sheard, J.M.; Ash, S.; Mellick, G.D.; Silburn, P.A.; Kerr, G.K. Improved nutritional status is related to improved quality of life in Parkinson’s disease. BMC Neurol. 2014, 14, 212. [Google Scholar] [CrossRef] [Green Version]
- Spahn, J.M.; Reeves, R.S.; Keim, K.S.; Laquatra, I.; Kellogg, M.; Jortberg, B.; Clark, N.A. State of the evidence regarding behavior change theories and strategies in nutrition counseling to facilitate health and food behavior change. J. Am. Diet. Assoc. 2010, 110, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Plow, M.A.; Moore, S.; Husni, M.E.; Kirwan, J.P. A systematic review of behavioural techniques used in nutrition and weight loss interventions among adults with mobility-impairing neurological and musculoskeletal conditions. Obes. Rev. 2014, 15, 945–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whatnall, M.C.; Patterson, A.J.; Ashton, L.M.; Hutchesson, M.J. Effectiveness of brief nutrition interventions on dietary behaviours in adults: A systematic review. Appetite 2018, 120, 335–347. [Google Scholar] [CrossRef]
- Evangelidis, N.; Craig, J.; Bauman, A.; Manera, K.; Saglimbene, V.; Tong, A. Lifestyle behaviour change for preventing the progression of chronic kidney disease: A systematic review. BMJ Open 2019, 9, e031625. [Google Scholar] [CrossRef] [PubMed]
- Dombrowski, S.U.; Sniehotta, F.F.; Avenell, A.; Johnston, M.; MacLennan, G.; Araújo-Soares, V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychol. Rev. 2012, 6, 7–32. [Google Scholar] [CrossRef] [Green Version]
- Russell, R.D.; Black, L.J.; Pham, N.M.; Begley, A. The effectiveness of emotional wellness programs on mental health outcomes for adults with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2020, 44, 102171. [Google Scholar] [CrossRef]

{kind=link}
| Year | Author | Study Design | Sample Size (n) | AgeMean (SD) (Years) | Intervention Description | Delivery Method | Intervention Duration and Frequency | Comparator | Behavior Change Theory Used | Number of BCTs Used | Diet/Nutrition Outcome (Tool) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dementia | |||||||||||
| 2019 | Cho and colleagues [31] | Pre-post | 23 | 83.5 (4.9) | Physical activity and nutrition education for people with mild dementia. Nutrition topics: the concept of health, proper eating habits, nutrition and nutrients, and the problems of hyper-nutrition and nutrient deficiency. | NR | 20 min; 16 sessions over 16 weeks | None | NR | 3 | Nutritional status (Mini Nutritional Assessment) |
| 2002 | Faxen-Irving and colleagues [32] | Quasi-controlled trial | 33 (IG 21; CG 12) | 84.0 (4.0) | Nutrition education for caregivers, plus nutritional supplements for people with dementia for 6 months. Education included practical exercises. Topics: malnutrition, food and nutritional requirements, dental care, detecting swallowing difficulties, altering food consistency. | Group, in-person | 12 h; 1 session | Nutritional supplement only | NR | 4 | Nutritional status (serum albumin, transferrin, B12, and hemoglobin) |
| 2020 | Hsaio and colleagues [36] | RCT | 57(IG 30; CG27) | 74.0 (10.2) | Nutrition education for people with dementia and their caregivers, including practical exercises and demonstrations. Topics: altered eating, nutritional imbalances, Mediterranean diet preparing food, healthy fast food., videos. | Group, in-person | 1 h plus 10–15 min phone calls; 6 sessions plus 3 phone calls over 3 months | Treatment as usual plus telephone counselling | Knowledge-attitude-behavior Model, Bandura’s Social Learning Theory, and the integrative model of mediators of health behavior change | 6 | Caregiver’s nutritional knowledge (Family Caregivers Nutritional Knowledge of Dementia); caregiver’s healthy eating behavior (Family Caregiver’s Healthy Eating Behavior for Dementia Checklist); and nutritional status (Mini Nutritional Assessment) |
| 2011 | Pivi and colleagues [33] | RCT | 78(IG 25; CG1 27; CG2 26) | 75.2 (76 *) | Nutrition education for people with dementia and their caregivers. Topics: nutrition in disease, behavioral changes during meals, attractive meals, constipation, hydration, administration of drugs, swallowing, food supplementation, lack of appetite. | Group, in-person | NR; 10 sessions over 6 months | CG1: treatment as usualCG2: nutritional supplement twice daily | NR | 1 | Nutritional status (total protein and serum albumin) |
| 2001 | Riviere and colleagues [34] | Non-randomized cluster trial | 225(IG 151; CG 74) | 76.3 (8.0) | Nutrition education for caregivers of people with dementia at a day hospital. Topics: weight loss consequences, eating behavior disorders, enriching food, nutritional recommendations, increasing protein and energy intake. | Group, in-person | 1 h; 9 sessions over 1 year | Treatment as usual (patients and caregivers from day hospitals in France and Spain) | NR | 9 | Nutritional status (Mini Nutritional Assessment); and caregiver’s nutritional knowledge (Family Caregivers Nutritional Knowledge of Dementia) |
| 2011 | Salva and colleagues [35] | Cluster randomized trial | 946(IG 448; CG 498) | 79 (7.3) | NutriAlz nutrition program for families and caregivers of people with dementia. Topics: weight loss, nutritional monitoring, the food pyramid, menu creation, cooking methods, food substitution, eating behavior problems. | Group, in-person | NR; 4 sessions over 1 year | Treatment as usual (five patient day care centers) | NR | 4 | Nutritional status (Mini Nutritional Assessment) |
| Multiple sclerosis | |||||||||||
| 1993 | Doidge and colleagues [37] | Pre-post | 48 | 46.9 (9.9) | Nutrition education for people with multiple sclerosis. Topics: The Action and Research for Multiple Sclerosis healthy eating plan, saturated and polyunsaturated fat, preparing food at home, understanding food labels, suitable convenience food, vitamins and minerals, weight maintenance, recipe tasting. | Group, in-person | 90 min; 8 sessions over 8 weeks | None | NR | 8 | Diet composition (daily energy intake and nutrient intakes) |
| 2019 | Katz Sand and colleagues [39] | Pilot RCT | 34(IG 18; CG 16) | 43 (NR) | Nutrition education for people with multiple sclerosis (groups of five); Mediterranean Diet. Topics: shopping tips, sample menu plan, reading food labels, eating at restaurants. Participants returned monthly (or dialed in) to discuss issues with following the diet. | Group, in-person and/or telehealth | NR; 6 sessions over 6 months | MS education seminars | NR | 6 | Dietary adherence and food group intake (food frequency questionnaire); and perceived benefits |
| 2016 | Riemann-Lorenz and colleagues [38] | Single aim, post | 11 | 38.5 (12.3) | Nutrition education for people with multiple sclerosis (1 session), including 2 short group discussions. Topics: epidemiology, research study designs, study endpoints and problems, experiences with multiple sclerosis diets, common multiple sclerosis diets, RCTs of diet and multiple sclerosis. | Group, in-person | 2 h; 1 session | None | NR | 3 | Novelty of information/knowledge; importance of information; and impact of information |
| 2020 | Wingo and colleagues [40] | Single arm, post | 18 | 46.0 (11.6) | Nutrition education and physical activity education for people with multiple sclerosis, for the low glycemic index diet, including online modules and calls from tele-coaches. Nutrition topics: meal planning, foods to eat and limit, cooking basics, healthy eating on a budget. Weeks 1–5 were standardized information. Weeks 6–12 were tailored to address barriers and goals. | Individual, telehealth | 12 online modules (time NR) and 12 20–45 min phone calls over 12 weeks | None | Health Action Process Approach | 10 | Diet quality (24-h food recall); and fat mass (dual-energy X-ray absorptiometry scan) |
| Stroke | |||||||||||
| 2000 | Rimmer and colleagues [41] | RCT | 35(IG 18; CG 17) | 53.2 (8.3) | Health Promotion program for stroke survivors (exercise, nutrition, and health behavior classes), including cooking demonstration and practice. Nutrition topics: low-fat and low-cholesterol foods, preparation of healthy meals, healthy food substitutes. | Group, in-person | 1 h; 36 sessions over 12 weeks | Waitlist controls | Transtheoretical (Stage of Change) Model | 11 | Dietary fat intake (Rate Your Plate Eating Pattern Assessment) and blood lipid profile (total cholesterol, high-density and low-density lipoprotein cholesterols, triglycerides) |
| 2020 | Towfighi and colleagues [42] | RCT | 100(IG 49; CG 51) | 58.0 (9.0) | Healthy Eating and Lifestyle After Stroke program for stroke survivors. Nutrition topics: healthy dietary patterns, monitoring food intake, food label reading, shopping, purchasing healthy foods, diet as a means of secondary stroke prevention. | Group, in-person | 2 h; 6 sessions over 6 weeks | Treatment as usual | Transtheoretical (Stage of Change) Model, Health Belief Model, and Social Cognitive Theory | 11 | Serves of fruits/vegetables per day; waist circumference; and blood lipid profile (total cholesterol, high-density and low-density lipoprotein cholesterols, triglycerides, hemoglobin A1c) |
| Parkinson’s disease | |||||||||||
| 2000 | Brenes [43] | Pre-post | 15 | 69.0 (NR) | Virtual nutrition education program for people with Parkinson’s disease and their caregivers. Included lesson videos, handouts and recipes (video and written). Topics: basic nutrition, healthy eating, Parkinson’s disease and the gut, inflammation and Parkinson’s disease, constipation and hydration, and ‘protein and Levodopa. | Individual, online | Self-paced; 6 sessions over 6 weeks | None | Self-Determination Theory | 11 | Nutritional status (Mini Nutritional Assessment); intake of macronutrients, micronutrients, and food groups (Diet History Questionnaire 3); nutrition knowledge (nutrition knowledge questionnaire); motivation about nutrition knowledge |
| Cho and Colleagues [31] | Doidge and Colleagues [37] | Faxen-Irving and Colleagues [32] | Hsiao and Colleagues [36] | Katz Sand and Colleagues [39] | Pivi and Colleagues [33] | Riemann-Lorenz and Colleagues [38] | Rimmer and Colleagues [41] | Riviere and Colleagues [34] | Salva and Colleagues [35] | Towfighi and Colleagues [42] | Wingo and Colleagues [40] | Brenes [43] | Total n | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Instruction how to perform a behavior | 11 | |||||||||||||
| Credible source | 9 | |||||||||||||
| Behavioral practice/rehearsal | 8 | |||||||||||||
| Information about health consequences | 7 | |||||||||||||
| Social comparison | 7 | |||||||||||||
| Self-monitoring behavior | 5 | |||||||||||||
| Demonstration of the behavior | 5 | |||||||||||||
| Problem solving | 4 | |||||||||||||
| Adding objects to the environment | 4 | |||||||||||||
| Social support (unspecified) | 3 | |||||||||||||
| Goal setting (outcome) | 3 | |||||||||||||
| Framing/reframing | 3 | |||||||||||||
| Feedback on behavior | 3 | |||||||||||||
| Action planning | 2 | |||||||||||||
| Reduce negative emotions | 2 | |||||||||||||
| Prompts/cues | 2 | |||||||||||||
| Review behavior goal(s) | 2 | |||||||||||||
| Monitoring behavior by others without feedback | 1 | |||||||||||||
| Monitoring outcome(s) by others without feedback | 1 | |||||||||||||
| Biofeedback | 1 | |||||||||||||
| Social support (practical) | 1 | |||||||||||||
| Goal setting (behavior) | 1 | |||||||||||||
| Total n | 3 | 8 | 4 | 6 | 6 | 1 | 3 | 11 | 9 | 4 | 11 | 10 | 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russell, R.D.; Black, L.J.; Begley, A. Nutrition Education Programs for Adults with Neurological Diseases Are Lacking: A Scoping Review. Nutrients 2022, 14, 1577. https://doi.org/10.3390/nu14081577
Russell RD, Black LJ, Begley A. Nutrition Education Programs for Adults with Neurological Diseases Are Lacking: A Scoping Review. Nutrients. 2022; 14(8):1577. https://doi.org/10.3390/nu14081577
Chicago/Turabian StyleRussell, Rebecca D., Lucinda J. Black, and Andrea Begley. 2022. "Nutrition Education Programs for Adults with Neurological Diseases Are Lacking: A Scoping Review" Nutrients 14, no. 8: 1577. https://doi.org/10.3390/nu14081577
APA StyleRussell, R. D., Black, L. J., & Begley, A. (2022). Nutrition Education Programs for Adults with Neurological Diseases Are Lacking: A Scoping Review. Nutrients, 14(8), 1577. https://doi.org/10.3390/nu14081577