
A Comparison of the Low-FODMAPs Diet and a Tritordeum-Based Diet on the Gastrointestinal Symptom Profile of Patients Suffering from Irritable Bowel Syndrome-Diarrhea Variant (IBS-D): A Randomized Controlled Trial

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
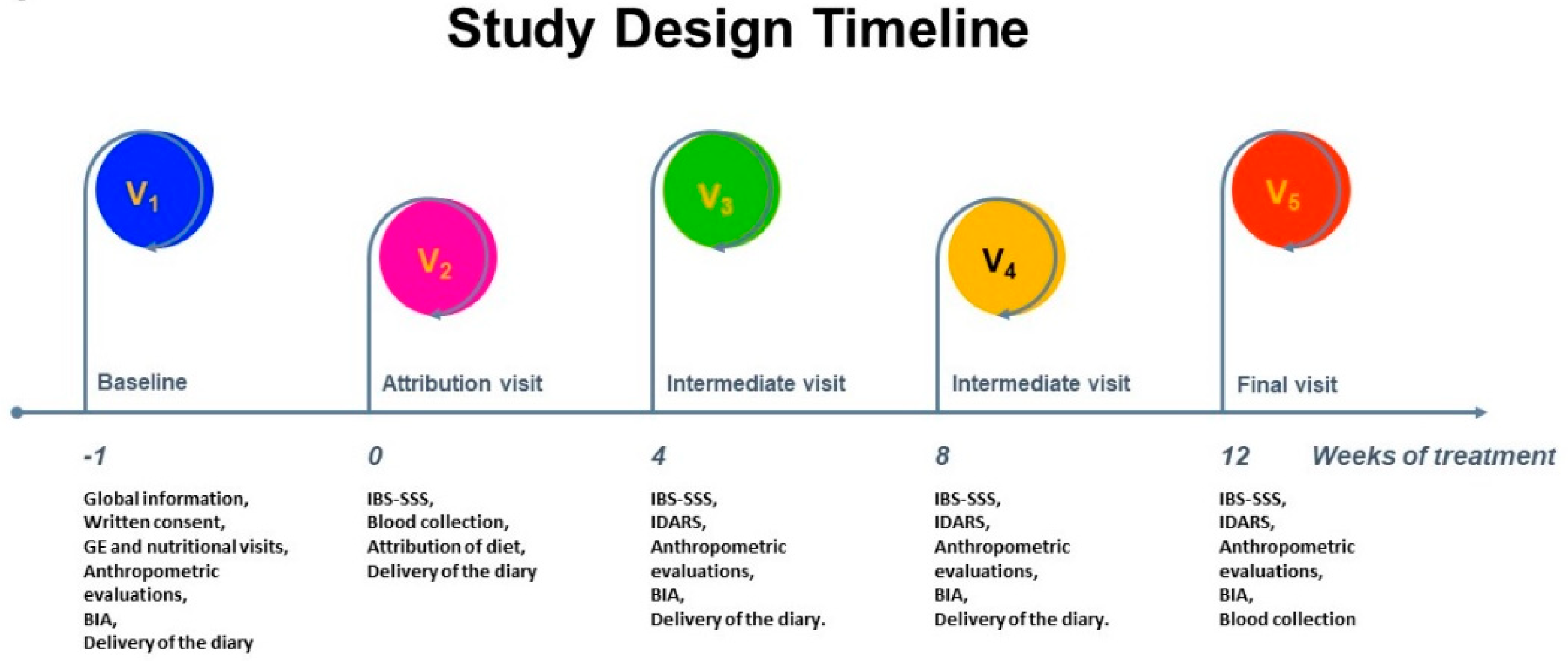
2.1. Study Design and Participants Enrollment
2.2. GI Symptom Scores
2.3. LowFODMAPs Characteristics and Diet
2.4. Tritordeum-Based Foods Characteristics and Diet
2.5. Assessment of Nutrient Intakes
2.6. Biochemical Analyses
2.7. Statistical Analysis
3. Results
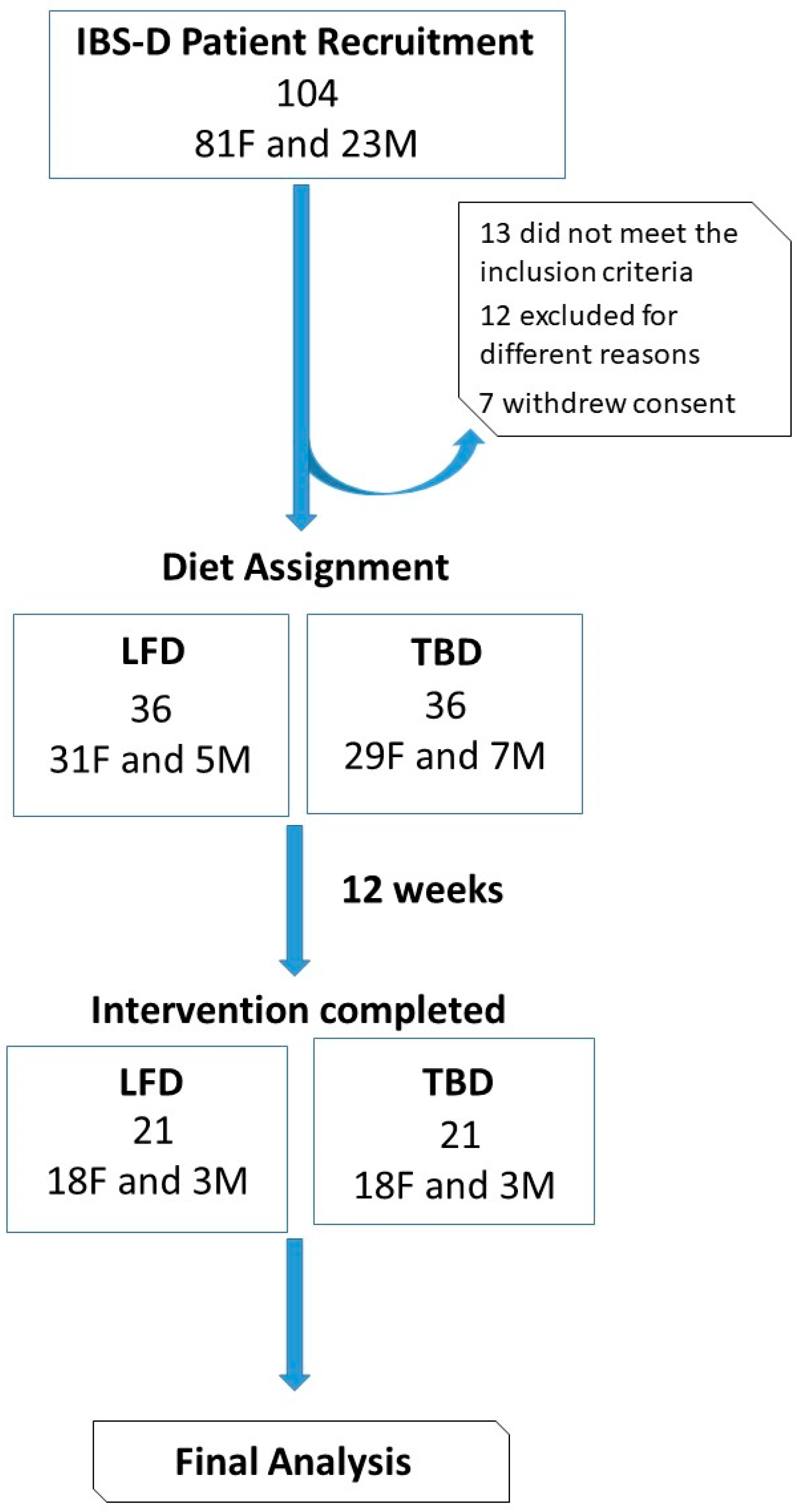
3.1. Number and Characteristics of the Patients
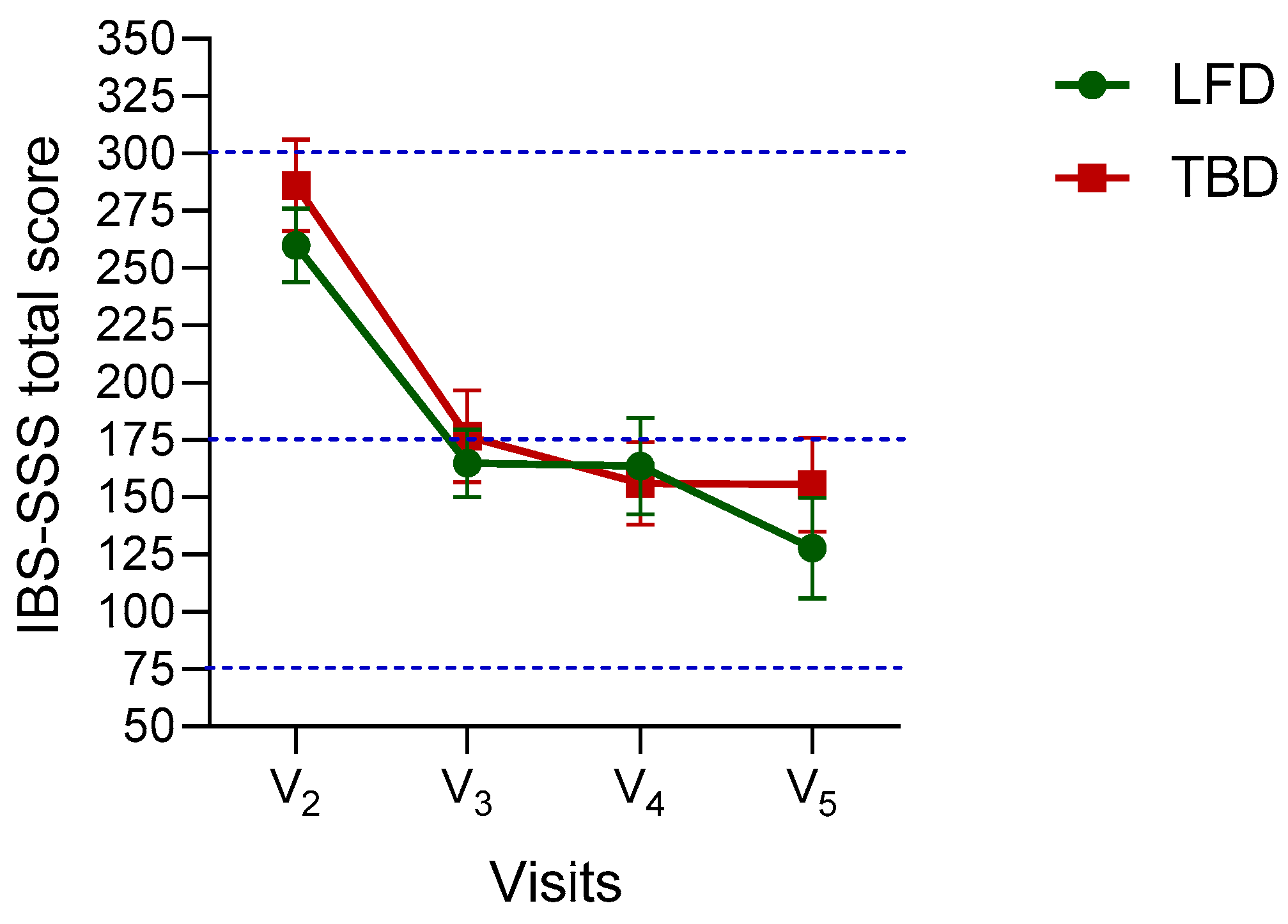
3.2. The Symptom Profile in IBS-D Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sperber, A.D.; Dumitrascu, D.; Fukudo, S.; Gerson, C.; Ghoshal, U.C.; Gwee, K.A.; Hungin, A.P.S.; Kang, J.Y.; Minhu, C.; Schmulson, M.; et al. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: A Rome Foundation working team literature review. Gut 2017, 66, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Lovell, R.M.; Ford, A.C. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721.e4. [Google Scholar] [CrossRef] [PubMed]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J. Neurogastroenterol. Motil. 2017, 23, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A.; Mearin, F.; Spiller, R.C. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Chey, W.D.; Olden, K.; Carter, E.; Boyle, J.; Drossman, D.; Chang, L. Utility of the Rome I and Rome II criteria for irritable bowel syndrome in U.S. women. Am. J. Gastroenterol. 2002, 97, 2803–2811. [Google Scholar] [CrossRef]
- Tuck, C.J.; Reed, D.E.; Muir, J.G.; Vanner, S.J. Implementation of the low FODMAP diet in functional gastrointestinal symptoms: A real-world experience. Neurogastroenterol. Motil. 2020, 32, e13730. [Google Scholar] [CrossRef]
- Linsalata, M.; Riezzo, G.; Orlando, A.; D’Attoma, B.; Prospero, L.; Tutino, V.; Notarnicola, M.; Russo, F. The Relationship between Low Serum Vitamin D Levels and Altered Intestinal Barrier Function in Patients with IBS Diarrhoea Undergoing a Long-Term Low-FODMAP Diet: Novel Observations from a Clinical Trial. Nutrients 2021, 13, 1011. [Google Scholar] [CrossRef]
- Orlando, A.; Tutino, V.; Notarnicola, M.; Riezzo, G.; Linsalata, M.; Clemente, C.; Prospero, L.; Martulli, M.; D’Attoma, B.; De Nunzio, V.; et al. Improved Symptom Profiles and Minimal Inflammation in IBS-D Patients Undergoing a Long-Term Low-FODMAP Diet: A Lipidomic Perspective. Nutrients 2020, 12, 1652. [Google Scholar] [CrossRef]
- Martín, A.; Alvarez, J.B.; Martín, L.M.; Barro, F.; Ballesteros, J. The development of tritordeum: A novel cereal for food processing. J. Cereal Sci. 1999, 30, 85–95. [Google Scholar] [CrossRef]
- Vaquero, L.; Comino, I.; Vivas, S.; Rodriguez-Martin, L.; Gimenez, M.J.; Pastor, J.; Sousa, C.; Barro, F. Tritordeum: A novel cereal for food processing with good acceptability and significant reduction in gluten immunogenic peptides in comparison with wheat. J. Sci. Food Agric. 2018, 98, 2201–2209. [Google Scholar] [CrossRef]
- Rotondi Aufiero, V.; Fasano, A.; Mazzarella, G. Non-Celiac Gluten Sensitivity: How Its Gut Immune Activation and Potential Dietary Management Differ from Celiac Disease. Mol. Nutr. Food Res. 2018, 62, e1700854. [Google Scholar] [CrossRef]
- Barmeyer, C.; Schumann, M.; Meyer, T.; Zielinski, C.; Zuberbier, T.; Siegmund, B.; Schulzke, J.D.; Daum, S.; Ullrich, R. Long-term response to gluten-free diet as evidence for non-celiac wheat sensitivity in one third of patients with diarrhea-dominant and mixed-type irritable bowel syndrome. Int. J. Colorectal Dis. 2017, 32, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Russo, F.; Riezzo, G.; Linsalata, M.; Orlando, A.; Tutino, V.; Prospero, L.; D’Attoma, B.; Giannelli, G. Managing symptom profile of IBS-D patients with Tritordeum-based foods: Results from a pilot study. Front. Nutr. 2022, 9, 797192. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.R., Jr. The International Conference on Harmonization Good Clinical Practice guideline. Qual. Assur. 1998, 6, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.A. The Consolidated Standards of Reporting Trials (CONSORT): Guidelines for reporting randomized trials. Nurs. Res. 2005, 54, 128–132. [Google Scholar] [CrossRef]
- Low FODMAPs Diet vs. Specific Dietary Advice in Patients with IBS Diarrheal Variant. Available online: https://ClinicalTrials.gov/NCT03423069 (accessed on 15 February 2020).
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef]
- Maagaard, L.; Ankersen, D.V.; Vegh, Z.; Burisch, J.; Jensen, L.; Pedersen, N.; Munkholm, P. Follow-up of patients with functional bowel symptoms treated with a low FODMAP diet. World J. Gastroenterol. 2016, 22, 4009–4019. [Google Scholar] [CrossRef]
- Varney, J.; Barrett, J.; Scarlata, K.; Catsos, P.; Gibson, P.R.; Muir, J.G. FODMAPs: Food composition, defining cutoff values and international application. J. Gastroenterol. Hepatol. 2017, 32 (Suppl. 1), 53–61. [Google Scholar] [CrossRef]
- Monash University. The Monash University Low FODMAP App. 2017. Available online: https://www.monashfodmap.com/ibs-central/i-have-ibs/get-the-app/ (accessed on 4 September 2021).
- Weaver, K.R.; Melkus, G.D.; Henderson, W.A. Irritable Bowel Syndrome. Am. J. Nurs. 2017, 117, 48–55. [Google Scholar] [CrossRef]
- Bellini, M.; Gambaccini, D.; Stasi, C.; Urbano, M.T.; Marchi, S.; Usai-Satta, P. Irritable bowel syndrome: A disease still searching for pathogenesis, diagnosis and therapy. World J. Gastroenterol. 2014, 20, 8807–8820. [Google Scholar] [CrossRef]
- Khan, M.A.; Nusrat, S.; Khan, M.I.; Nawras, A.; Bielefeldt, K. Low-FODMAP Diet for Irritable Bowel Syndrome: Is It Ready for Prime Time? Dig. Dis. Sci. 2015, 60, 1169–1177. [Google Scholar] [CrossRef] [PubMed]
- Bohn, L.; Storsrud, S.; Liljebo, T.; Collin, L.; Lindfors, P.; Tornblom, H.; Simren, M. Diet low in FODMAPs reduces symptoms of irritable bowel syndrome as well as traditional dietary advice: A randomized controlled trial. Gastroenterology 2015, 149, 1399–1407.e2. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.J.; Gibson, P.R. Fructose malabsorption and symptoms of irritable bowel syndrome: Guidelines for effective dietary management. J. Am. Diet. Assoc. 2006, 106, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.J.; Parker, F.C.; Muir, J.G.; Gibson, P.R. Dietary triggers of abdominal symptoms in patients with irritable bowel syndrome: Randomized placebo-controlled evidence. Clin. Gastroenterol. Hepatol. 2008, 6, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Ong, D.K.; Mitchell, S.B.; Barrett, J.S.; Shepherd, S.J.; Irving, P.M.; Biesiekierski, J.R.; Smith, S.; Gibson, P.R.; Muir, J.G. Manipulation of dietary short chain carbohydrates alters the pattern of gas production and genesis of symptoms in irritable bowel syndrome. J. Gastroenterol. Hepatol. 2010, 25, 1366–1373. [Google Scholar] [CrossRef]
- Shepherd, S.J.; Lomer, M.C.; Gibson, P.R. Short-chain carbohydrates and functional gastrointestinal disorders. Am. J. Gastroenterol. 2013, 108, 707–717. [Google Scholar] [CrossRef]
- Major, G.; Pritchard, S.; Murray, K.; Alappadan, J.P.; Hoad, C.L.; Marciani, L.; Gowland, P.; Spiller, R. Colon Hypersensitivity to Distension, Rather Than Excessive Gas Production, Produces Carbohydrate-Related Symptoms in Individuals with Irritable Bowel Syndrome. Gastroenterology 2017, 152, 124–133.e2. [Google Scholar] [CrossRef]
- Dorn, S.D.; Palsson, O.S.; Thiwan, S.I.; Kanazawa, M.; Clark, W.C.; van Tilburg, M.A.; Drossman, D.A.; Scarlett, Y.; Levy, R.L.; Ringel, Y.; et al. Increased colonic pain sensitivity in irritable bowel syndrome is the result of an increased tendency to report pain rather than increased neurosensory sensitivity. Gut 2007, 56, 1202–1209. [Google Scholar] [CrossRef]
- Nawawi, K.N.M.; Belov, M.; Goulding, C. Low FODMAP diet significantly improves IBS symptoms: An Irish retrospective cohort study. Eur. J. Nutr. 2020, 59, 2237–2248. [Google Scholar] [CrossRef]
- Ankersen, D.V.; Weimers, P.; Bennedsen, M.; Haaber, A.B.; Fjordside, E.L.; Beber, M.E.; Lieven, C.; Saboori, S.; Vad, N.; Rannem, T.; et al. Long-Term Effects of a Web-Based Low-FODMAP Diet Versus Probiotic Treatment for Irritable Bowel Syndrome, Including Shotgun Analyses of Microbiota: Randomized, Double-Crossover Clinical Trial. J. Med. Internet Res. 2021, 23, e30291. [Google Scholar] [CrossRef]
- Schwenk, A.; Eschner, W.; Kremer, G.; Ward, L.C. Assessment of intracellular water by whole body bioelectrical impedance and total body potassium in HIV-positive patients. Clin. Nutr. 2000, 19, 109–113. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Energy Per 100 g | Flour | Pasta |
|---|---|---|
| Kcal | 350 | 355.6 |
| Proteins (g) | 12.8 | 12 |
| Fats (g) | 1.7 | 0.1 |
| Saturated fats (g) | 0.4 | 0.0 |
| Dietary fiber (g) | 2.6 | 1.5 |
| Carbohydrates (g) | 69.6 | 75.9 |
| Simple sugars (g) | 0.8 | 4.3 |
| Salt (g) | 0.1 | 0.2 |
| Ingredients | Preparation | |
|---|---|---|
| Pasta | Water and Tritordeum semolina | Long pasta shapes (spaghetti, linguine, and fettuccine) and short pasta shapes (penne rigate and rigatoni) were produced in a pilot pasta-making plant (Intini Food, Putignano-Bari, Italy) |
| Bread | Tritordeum flour, water, salt, brewer’s yeast | The dough was prepared and risen sufficiently to reach double the volume. Then, it was baked for about 30 min at 240 °C. |
| Taralli | Tritordeum flour, olive oil, white wine, salt | These salty biscuits were prepared by baking the ready dough for about 40 min at 250 °C. |
| Breakfast biscuits | Tritordeum flour, lactose-free milk, olive oil, sugar, ammonium bicarbonate | The dough was prepared and then baked for about 20 min at 200 °C. |
| LFD | TBD | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameters | V2 | V3 | V4 | V5 | V2 | V3 | V4 | V5 | Time | Diet × Time |
| Severity of Abdominal Pain | 45.8 ± 23.1 | 27.9 ± 16.7 | 29.3 ± 25.1 | 20.1 ± 21.0 | 48.7 ± 24.8 | 27.9 ± 24.2 | 20.4 ± 19.2 | 24.4 ± 23.3 | <0.0001 | 0.25 |
| Frequency of Abdominal Pain | 45.7 ± 28.0 | 33.8 ± 28.4 | 37.1 ± 30.0 | 19.0 ± 25.5 | 48.6 ± 31.8 | 27.8 ± 31.2 | 26.7 ± 32.8 | 24.9 ± 26.3 | <0.0001 | 0.68 |
| Severity of Abdominal Distension | 51.1 ± 23.9 | 25.6 ± 17.6 | 28.2 ± 23.2 | 23.0 ± 21.3 | 61.8 ± 21.7 | 32.1 ± 22.8 | 29.7 ± 18.8 | 30.9 ± 24.4 | <0.0001 | 0.10 |
| Dissatisfaction with Bowel Habit | 60.2 ± 23.9 | 41.9 ± 25.7 | 37.3 ± 25.6 | 32.3 ± 24.5 | 69.4 ± 24.9 | 50.0 ± 26.0 | 38.6 ± 24.6 | 41.2 ± 24.3 | <0.0001 | 0.76 |
| Interference with Quality of Life | 57.1 ± 21.1 | 35.8 ± 21.9 | 33.9 ± 28.8 | 33.4 ± 27.3 | 57.5 ± 24.4 | 40.1 ± 28.7 | 31.9 ± 23.8 | 34.0 ± 25.0 | <0.0001 | 0.87 |
| LFD | TBD | p Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Parameters | V2 | V5 | Change | V2 | V5 | Change | Time | Diet × Time |
| Anthropometric and BIA measurements | ||||||||
| Weight (kg) | 64.7 ± 12.9 | 60.8 ± 12.1 | −3.9 ± 2.3 | 69.4 ± 12.9 | 66.1 ± 12.0 | −3.2 ± 3.1 | <0.0001 | 0.40 |
| BMI (kg/m2) | 24.3 ± 4.3 | 23.0 ± 4.2 | −1.4 ± 0.9 | 26.5 ± 4.7 | 25.2 ± 4.3 | −1.3 ± 1.2 | <0.001 | 0.70 |
| Abdominal circumference (cm) | 87.0 ± 10.5 | 84.1 ± 10.9 | −2.9 ± 2.5 | 93.2 ± 10.3 | 89.9 ± 10.0 | −3.2 ± 4.4 | <0.001 | 0.71 |
| Waist Circumference (cm) | 77.8 ± 11.7 | 74.8 ± 10.4 | −3.0 ± 2.8 | 82.8 ± 12.7 | 79.8 ± 11.7 | −2.9 ± 3.0 | <0.001 | 0.90 |
| PhA (degrees) | 5.7 ± 0.7 | 5.9 ± 0.71 | 0.2 ± 0.4 | 6.3 ± 1.8 | 6.5 ± 1.0 | 0.2 ± 1.2 | 0.22 | 0.93 |
| BCM (kg) | 24.4 ± 4.8 | 24.4 ± 5.0 | 0.0 ± 1.2 | 26.6 ± 7.7 | 26.4 ± 6.3 | −0.2 ± 2.8 | 0.73 | 0.75 |
| FM (kg) | 18.0 ± 7.5 | 15.2 ± 7.1 | −2.8 ± 2.0 | 20.9 ± 7.1 | 19.4 ± 6.4 | −1.5 ± 2.4 | <0.001 | 0.07 |
| FFM (kg) | 46.7 ± 8.1 | 45.7 ± 7.6 | −1.0 ± 1.3 | 48.6 ± 8.4 | 46.7 ± 8.1 | −1.9 ± 2.2 | 0.0001 | 0.08 |
| TBW (L) | 34.2 ± 6.1 | 33.3 ± 5.7 | 0.9 ± 1.1 | 35.3 ± 5.8 | 33.8 ± 5.6 | −1.5 ± 1.9 | 0.0002 | 0.15 |
| ECW (L) | 16.1 ± 3.0 | 15.4 ± 2.4 | 0.7 ± 1.0 | 15.9 ± 2.6 | 14.8 ± 2.1 | −1.1 ± 1.6 | 0.0003 | 0.43 |
| LFD | TBD | p Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Parameters | V2 | V5 | Change | V2 | V5 | Change | Time | Diet × Time |
| Biochemical profiles | ||||||||
| Total cholesterol (mg/dL) | 182.3 ± 34.1 | 181.6 ± 36.2 | −0.8 ± 22.5 | 195.0 ± 39.60 | 191.8 ± 33.2 | −3.2 ± 30.2 | 0.63 | 0.77 |
| HDL cholesterol (mg/dL) | 55.9 ± 10.3 | 55.9 ± 12.6 | 0.0 ± 7.2 | 58.0 ± 12.9 | 55.9 ± 13.2 | −3.1 ± 8.1 | 0.28 | 0.12 |
| LDL cholesterol (mg/dL) | 115.2 ± 41.3 | 108.4 ± 32.6 | −6.8 ± 33.4 | 117.1 ± 37.3 | 119.5 ± 31.4 | 2.4 ± 28.6 | 0.65 | 0.35 |
| Triglycerides (mg/dl) | 89.3 ± 34.2 | 86.2 ± 47.4 | −3.0 ± 35.1 | 88.5 ± 42.6 | 86.8 ± 43.1 | −1.7 ± 32.1 | 0.65 | 0.90 |
| Total cholesterol/HDL | 3.3 ± 0.7 | 3.3 ± 0.8 | 0.0 ± 0.6 | 3.5 ± 1.0 | 3.7 ± 1.1 | 0.2 ± 0.5 | 0.26 | 0.43 |
| Fasting glucose (mg/dL) | 86.0 ± 15.3 | 79.1 ± 9.2 | −6.9 ± 12.5 | 88.8 ± 12.2 | 83.8 ± 9.3 | −5.1 ± 9.8 | 0.003 | 0.62 |
| CRP (mg/dL) | 0.2 ± 0.2 | 0.1 ± 0.1 | −0.1 ± 0.2 | 0.3 ± 0.2 | 0.2 ± 0.1 | −0.1 ± 0 | 0.02 | 0.58 |
| Vitamin D (ng/mL) | 21.8 ± 8.0 | 30.8 ± 8.4 | 9.9 ± 8.8 | 25.9 ± 17.5 | 27.4 ± 8.6 | 1.6 ± 18.5 | 0.03 | 0.10 |
| Iron (µg/dL) | 104.5 ± 50.3 | 99.0 ± 36.1 | −5.4 ± 50.8 | 86.0 ± 40.6 | 113.8 ± 35.4 | 27 ± 46.3 | 0.154 | 0.04 |
| Urea (mg/dL) | 32.4 ± 7.1 | 33.2 ± 5.5 | 0.8 ± 7.4 | 30.4 ± 7.5 | 30.9 ± 6.1 | 0.5 ± 6.7 | 0.55 | 0.90 |
| Creatinine (mg/dL) | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.0 ± 0.1 | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.0 ± 0.3 | 0.80 | 0.24 |
| Urate (mg/dL) | 4.3 ± 1.0 | 4.6 ± 0.8 | 0.3 ± 1.0 | 4.9 ± 1.0 | 4.7 ± 1.0 | −0.1 ± 0.7 | 0.52 | 0.09 |
| Total protein (g/dL) | 7.0 ± 0.4 | 7.2 ± 0.4 | 0.1 ± 0.5 | 7.1 ± 0.4 | 7.1 ± 0.4 | 0.0 ± 0.4 | 0.46 | 0.24 |
| Cobalamin (pg/mL) | 314.1 ± 124.7 | 327.6 ± 125.9 | 13.5 ± 67 | 352.0 ± 187.7 | 346.4 ± 243.7 | −5.7 ± 110.8 | 0.79 | 0.51 |
| Folate (ng/mL) | 5.9 ± 2.5 | 6.3 ± 3.3 | 0.5 ± 1.9 | 7.5 ± 5.4 | 6.8 ± 5.7 | −0.7 ± 3.9 | 0.85 | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, F.; Riezzo, G.; Orlando, A.; Linsalata, M.; D’Attoma, B.; Prospero, L.; Ignazzi, A.; Giannelli, G. A Comparison of the Low-FODMAPs Diet and a Tritordeum-Based Diet on the Gastrointestinal Symptom Profile of Patients Suffering from Irritable Bowel Syndrome-Diarrhea Variant (IBS-D): A Randomized Controlled Trial. Nutrients 2022, 14, 1544. https://doi.org/10.3390/nu14081544
Russo F, Riezzo G, Orlando A, Linsalata M, D’Attoma B, Prospero L, Ignazzi A, Giannelli G. A Comparison of the Low-FODMAPs Diet and a Tritordeum-Based Diet on the Gastrointestinal Symptom Profile of Patients Suffering from Irritable Bowel Syndrome-Diarrhea Variant (IBS-D): A Randomized Controlled Trial. Nutrients. 2022; 14(8):1544. https://doi.org/10.3390/nu14081544
Chicago/Turabian StyleRusso, Francesco, Giuseppe Riezzo, Antonella Orlando, Michele Linsalata, Benedetta D’Attoma, Laura Prospero, Antonia Ignazzi, and Gianluigi Giannelli. 2022. "A Comparison of the Low-FODMAPs Diet and a Tritordeum-Based Diet on the Gastrointestinal Symptom Profile of Patients Suffering from Irritable Bowel Syndrome-Diarrhea Variant (IBS-D): A Randomized Controlled Trial" Nutrients 14, no. 8: 1544. https://doi.org/10.3390/nu14081544
APA StyleRusso, F., Riezzo, G., Orlando, A., Linsalata, M., D’Attoma, B., Prospero, L., Ignazzi, A., & Giannelli, G. (2022). A Comparison of the Low-FODMAPs Diet and a Tritordeum-Based Diet on the Gastrointestinal Symptom Profile of Patients Suffering from Irritable Bowel Syndrome-Diarrhea Variant (IBS-D): A Randomized Controlled Trial. Nutrients, 14(8), 1544. https://doi.org/10.3390/nu14081544